Orthopedic Surgery MCQ Mock Exam: Fracture, Hip & Nerve Review | Part 191

Key Takeaway
This page offers Part 191 of Dr. Mohammed Hutaif's comprehensive Orthopedic Surgery board review. Featuring 100 verified, high-yield MCQs mimicking OITE/AAOS exams, it helps orthopedic residents and surgeons prepare for certification. Utilize study or exam mode to master Fracture, Hip, and Nerve topics for optimal exam readiness.
About This Board Review Set
This is Part 191 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 191
This module focuses heavily on: Fracture, Hip, Nerve.
Sample Questions from This Set
Sample Question 1: Which nerve is not included in a standard popliteal nerve block?...
Sample Question 2: Figure 99 is the radiograph of an 18-year-old National Collegiate Athletic Association Division I basketball player who jumped for a basket. Afterlanding, he was unable to put weight on his left great toe. He developed pain, swelling, and e...
Sample Question 3: Which of the following structures may help maintain radial length after a radial head fracture?...
Sample Question 4: Of all the pelvic ring injury types, anteroposterior compression type III pelvic ring injuries have the highest rate of which of the following?...
Sample Question 5: A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which nerve is not included in a standard popliteal nerve block?
Explanation
A standard popliteal nerve block is performed with the patient prone. The injection aims for the area at, or close to, the peroneal and tibial nerves. The sural nerve branches distal to the injection site, so this nerve and the superficial peroneal, deep peroneal, and tibial nerves are covered with the injection. The saphenous nerve is in an anteromedial location at knee level and is not close enough to the area covered by the posterior injection to be included in the analgesic effect.
RECOMMENDED READINGS
Varitimidis SE, Venouziou AI, Dailiana ZH, Christou D, Dimitroulias A, Malizos KN. Triple nerve block at the knee for foot and ankle surgery performed by the surgeon: difficulties and efficiency. Foot Ankle Int. 2009 Sep;30(9):854-9. PubMed PMID: 19755069. View Abstract at PubMed
Hromádka R, Barták V, Popelka S, Jahoda D, Pokorný D, Sosna A. [Regional anaesthesia of the foot achieved from two cutaneous points of injection: an anatomical study]. Acta Chir Orthop Traumatol Cech. 2009 Apr;76(2):104-9. Czech. PubMed PMID: 19439129. View Abstract at PubMed
Tran D, Clemente A, Finlayson RJ. A review of approaches and techniques for lower extremity nerve blocks. Can J Anaesth. 2007 Nov;54(11):922-34. Review. PubMed PMID: 17975239. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 44

42A

B
Figures 42a and 42b are the radiographs of a 32-year-old man with an accessory navicular, pes planovalgus deformity, and an associated gastrocnemius contracture. He has been treated with custom orthotics and a physical therapy program for several years and has progressed to stage II posterior tibial tendon dysfunction (PTTD). This patient is now interested in surgery. Tendon reconstruction with bony procedure to correct alignment, medializing calcaneal osteotomy with lateral column lengthening, and a subtalar arthroereisis implant are discussed with the patient.
Question 2
Figure 99 is the radiograph of an 18-year-old National Collegiate Athletic Association Division I basketball player who jumped for a basket. After landing, he was unable to put weight on his left great toe. He developed pain, swelling, and ecchymosis maximally around the sesamoids. When assessing stability of the first metatarsophalangeal joint, he appears to have more laxity on the left. What is the best next step?

Explanation
This patient jumped on his forefoot and landed with pain in his great toe. His radiograph shows possible increased space between the sesamoids and the base of the phalanx. A comparison radiograph on the other side will reveal if this position is normal for this patient. If findings are asymmetric, turf toe injury is a possibility based on this patient's symptoms and mechanism of injury.
RECOMMENDED READINGS
Waldrop NE 3rd, Zirker CA, Wijdicks CA, Laprade RF, Clanton TO. Radiographic evaluation of plantar plate injury: an in vitro biomechanical study. Foot Ankle Int. 2013 Mar;34(3):403-8. doi: 10.1177/1071100712464953. Epub 2013 Jan 14. PubMed PMID: 23520299. View
Abstract at PubMed
McCormick JJ, Anderson RB. The great toe: failed turf toe, chronic turf toe, and complicated sesamoid injuries. Foot Ankle Clin. 2009 Jun;14(2):135-50. doi: 10.1016/j.fcl.2009.01.001. Review. PubMed PMID: 19501799. View Abstract at PubMed
Question 3
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
REFERENCES: Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 4
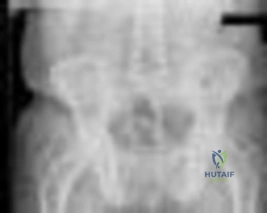
Of all the pelvic ring injury types, anteroposterior compression type III pelvic ring injuries have the highest rate of which of the following?

Explanation
Question 5
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
REFERENCES: Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Morrissy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 579-624.
Question 6
03 A 26-year-old woman has chronic toe pain after hitting a bedpost 3 months ago. A radiograph is shown in Figure 27. Her injury represents an avulsion of the

Explanation
The EDB originates on the distal lateral and superior surface of the calcaneus and inserts on the
lateral aspect of the flexor digitorum longus tendon and also on to the base of the proximal phalanx of the first through fourth toes. There is no EDB tendon to the fifth toe. If an EDB laceration is easily identified at the time of an EDL repair, than it may be repaired as well, otherwise repair of the EDL alone is sufficient.
Heckman JD: Fractures and dislocation of the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds):Rockwood and Green’s Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 2166-2169.
Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 787-788.
back to this question next question
Question 7
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 8
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Ogden JA, Ganey TM, Hill JD, et al: Sever’s injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 9
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Larsen E, Lauridsen F: Conservative treatment of patellar dislocations: Influence of evident factors on the tendency to redislocation and the theraputic result. Clin Orthop
1982;171:131-136.
Question 10
Which of the following cohorts of patients is at highest risk of a future anterior cruciate ligament (ACL) tear? Review Topic
Explanation
Question 11
During the ilioinguinal approach to the pelvis, the corona mortis artery must be identified and ligated if present. The corona mortis artery joins the external illiac artery with which other major artery?

Explanation
Question 12
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
REFERENCE: Leffert RD: Anatomy of the Brachial Plexus in Brachial Plexus Injuries. Churchill Livingstone, New York, NY, 1985.
Question 13
Which laboratory findings would most support a diagnosis of prosthetic joint infection (PJI) in a hip or knee arthroplasty performed 3 weeks ago?
Explanation
The diagnosis of acute PJI is associated with different criteria than the diagnosis of a chronic PJI. There is no agreed-upon threshold for ESR during the acute period (6 weeks) following total joint arthroplasty. The CRP threshold is higher during the acute period (100 mg/L vs 10 mg/L for a chronic infection). The threshold for synovial fluid analysis for an acute PJI is 10000 cells/µL and more than 90% PMN neutrophils vs 3000 cells/µL and more than 80% PMN neutrophils for a chronic infection.

Question 14
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
Explanation
REFERENCES: Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264.
Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 15
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice.
REFERENCES: Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 16
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with Review Topic
Explanation
Question 17
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty? Review Topic
Explanation
Question 18
- A healed fracture of the tibia that demonstrates 25 degrees apex posterior angulation and 28 degrees varus angulation on AP and lateral radiographs is most accurately described as a
Explanation
Question 19
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?
Explanation
REFERENCES: Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Pierz KA, Stieber JR, Kusumi K, Dormans JP: Hereditary multiple exostoses: One center’s experience and review of etiology. Clin Orthop 2002;402:49-59.
Question 20
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
Explanation
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, www.aaos.org/research/guidelines/ PEguide.asp
Question 21
Which structure is shown in Video 27? 27

Explanation
Video 27 shows the medial patellofemoral ligament running from the medial epicondyle of the femur to the medial portion of the patella. The posterior oblique ligament and the superficial medial collateral ligament run from medial epicondyle to the tibia.
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Aatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 22
Intramedullary nailing of proximal tibial shaft fractures are technically demanding, and use of an extended medial parapatellar incision with a semiextended technique can prevent what common deformity at the fracture site?

Explanation
Lang et al. reported in their study of 32 proximal third tibia fractures that 56% of the fractures had 5 degrees or more valgus angulation and 28% had 10 degrees or more valgus angulation. Angulation in the AP plane ranged from 0 degrees to 20 degrees, all of which was apex anterior. Nineteen (59%) fractures demonstrated 5 degrees or more angulation, and 7 (22%) fractures demonstrated 10 degrees of more angulation.
Tornetta advocates use of extended medial parapatellar incision with the leg in a semiextended position to allow for a more proximal and lateral starting point. This modified starting point forces the nail to overcome the tendency of the fracture to flex (apex anterior) and go into valgus.
Question 23
During revision total knee arthroplasty (TKA), there is significant laxity in 90° of flexion and 10° short of full extension. Correcting the gap imbalance is best achieved by
Explanation
A. Nonoperative treatment with close radiographic follow-up
B. Revision THA with ceramic- on-polyethylene with abductor reconstruction
C. Removal of components and placement of spacer as stage 1 of 2-stage revision
D. Revision THA with metal-on- polyethylene and trochanteric slide
Question 24
A 30-year-old patient underwent open reduction internal fixation of a talar neck fracture 8 weeks ago. His current radiographs demonstrate a subchondral radiolucency of the dome of the talus. What is the next most appropriate course of action?

Explanation
Question 25
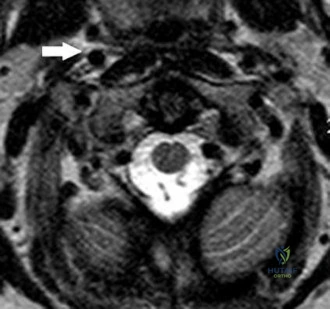
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
Explanation
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity
= 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Question 26
A 57-year-old man with type II diabetes mellitus was successfully treated for a first occurrence forefoot full-thickness (Wagner II) diabetic foot ulcer underlying the third metatarsal head with associated hammertoe with a series of weight-bearing total contact casts. There was no evidence of osteomyelitis. The ulcer is now fully healed. He is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. What is the next most appropriate step in management?
Explanation
REFERENCES: Pinzur MS, Slovenkai MP, Trepman E, et al: Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int 2005;26:113-119.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 27
Because of the ongoing pain and instability and the demonstration of radiographic instability when the ankle is stressed, what surgical procedure should be performed to restore stability to the ankle joint based on the CT findings?
Explanation
The fracture at the insertion of the AITFL into the fibula represents a syndesmosis injury. In some cases, a direct repair of the fracture will stabilize the syndesmosis, but in most cases this injury should most likely be reinforced by placing a screw or suture tensioning device across the syndesmosis for additional support.A Brostrom or allograft reconstruction is indicated for an ankle sprain involving the ATFL or CFL.Simply excising the fragment will leave the patient with an incompetent syndesmosis. Repairing the SPR with or without a groove deepening procedure is indicated if there is evidence of subluxated or dislocated peroneal tendons, which is not demonstrated on the CT scans. The bone has been avulsed off the fibula by the portion of the AITFL that attaches to the fibula, therefore indicating that there is a syndesmosis injury. Allograft lateral ligament reconstruction and excision of loose body/fracture fragment are incorrect procedures based on location. The deltoid is a medial structure and this fracture is lateral. The ATFL and CFL attach at the inferior margin of the fibula near the lateral process of the talus and calcaneus. A SPR avulsion would present as an avulsion off the lateral wall of the fibula, not superior and not into the syndesmotic space as shown on the CT scans.
Question 28
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?

Explanation
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 29
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30° of flexion, which decreases as the knee is flexed to 90°. What is the most likely diagnosis?
Explanation
REFERENCES: Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 30
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann’s sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
REFERENCES: Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745.
Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 31
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Question 32
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
Explanation
REFERENCE: Glassman SD, Anagnost SC, Parker A, et al: The effect of cigarette smoking and smoking cessation on spinal fusion. Spine 2000;25:2608-2615.
Question 33
Figures 54a and 54b are the radiographs of a 23-year-old man who fell from a height and sustained an isolated injury to his right leg. Which of the following is a useful surgical technique to optimize alignment during intramedullary nailing?

Explanation
(SBQ12TR.65) A patient falls and sustains the isolated injury seen in Figures A and
B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?

Full pronation
25 degrees pronation
Neutral
25 degrees supination
Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial
head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with < 3 fragments. Radial head replacement is considered for comminuted fractures (Mason Type III) with 3 or more fragments.
Cheung et al. reviewed the surgical approaches to the elbow. The lateral approach (Kocher or Kaplan) is most commonly used with these injuries. The Kocher approach utilizes the intramuscular plane between anconeus and extensor carpi ulnaris. Kaplan utilizes the plane between extensor digitorum commons and extensor carpi radialis brevis.
Figure A and B show AP and lateral radiographs of the left elbow. There is a displaced radial head fracture. Illustration A shows a schematic diagram of the radial head "safe zone" between the radial styloid to Lister's tubercle.
Incorrect Answers:
Question 34
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
REFERENCES: Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.
Question 35
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
Explanation
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
Question 36
MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
Explanation
A. Pain with elbow extension in forearm pronation
B. Mechanical symptoms when rising from a chair
C. Valgus instability
D. Tenderness over the medial collateral ligament (MCL)
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
56- A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and 2. What is the most appropriate next step to restore this patient’s function?
Question 37
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
REFERENCES: Peters CL, Kull L, Jacobs JJ, Rosenberg AG, Galante JO: The fate of well fixed cemented femoral components left in place at the time of revision of the acetabular component. J Bone Joint Surg Am 1997;79:701-706.
Poon ED, Lachiewicz PF: Results of isolated acetabular revisions: The fate of the unrevised femoral component. J Arthroplasty 1998;13:42-49.
Moskal JT, Shen FH, Brown TE: The fate of stable femoral components retained during isolated acetabular revision: A six- to twelve-year follow-up study. J Bone Joint Surg Am
2002;84:250-255.
Templeton JE, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC: Revision of a cemented acetabular component to a cementless acetabular component. A ten- to fourteen-year follow-up study. J Bone Joint Surg Am 2001;83:1706-1711.
Question 38
Which of the following knee ligament injury patterns is most associated with an increase in external tibial rotation with the knee at 90 degrees of flexion?
Explanation
REFERENCES: Gollehon DL, Torzilli PA, Warren RF: The role of the posterolateral and cruciate ligaments in the stability of the human knee: A biomechanical study. J Bone Joint Surg Am 1987;69:233-242.
Cooper DE: Tests for posterolateral instability of the knee in normal subjects: Results of examination under anesthesia. J Bone Joint Surg Am 1991;73:30-36.
Veltri DM, Xeng XH, Torzilli PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 39
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
Explanation
Question 40
A 12-year-old girl who is 3 months postmenarchal undergoes full-time brace treatment for scoliosis. The posteroanterior radiograph (Figure A ) taken at that time reveals a right thoracic curve measures 28 degrees, and the left lumbar curve measures 23 degrees. At age 15, after 3 years of bracing, a repeat posteroanterior radiograph is obtained, now revealing a right thoracic curve measuring 11 degrees and the left lumbar curve measuring 19 degree, and Risser 4. Which statement best represents the indicated course of action in this patient? Review Topic

Explanation
Curves <25° can be treated with observation, while flexible curves from 25° to 45° in skeletally immature patients (Risser 0, 1, 2) should be treated with bracing. Bracing success is most commonly defined as <5° curve progression and failure is 6° or more curve progression at orthotic discontinuation (skeletal maturity), absolute progression to >45° either before or at skeletal maturity, or discontinuation in favor of surgery. Skeletal maturity is defined Risser sign 4, <1cm change in height over 2 visits 6 months apart, 2 years postmenarchal.
Richards et al. attempted to define parameters for future AIS bracing studies. Outcome measures should include patients with (1) <5° curve progression vs >6° progression at maturity, (2) curves exceeding 45° at maturity, or those who have had surgery recommendation/undergone.
Negrini et al. performed a Cochrane systematic review. Basing conclusions on 2
studies, they found that (1) a brace treated curve progression (74% success) better than observation (34% success) and electrical stimulation (33% success), and (2) a rigid brace is more successful than an elastic one (SpineCor) at curbing curve progression.
A
is
a
standing
PA
radiograph
showing.
Incorrect
Question 41
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
Question 42
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
Question 43
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Beaty JH: Fractures and dislocations about the elbow in children. Instr Course Lect 1992;41:373-384.
Question 44
Figure 24 shows the sitting AP and lateral spinal radiographs of a nonambulatory 12½-year-old boy with Duchenne muscular dystrophy who is being evaluated for scoliosis. The lumbar curve from T12 to L5 measures 36 degrees, and the thoracic curve from T3 to T12 measures 24 degrees on the AP radiograph. He has 5 degrees of pelvic obliquity. His forced vital capacity is 45% of predicted for height and weight. What is the most appropriate treatment for the spinal deformity?
Explanation
REFERENCES: Hahn GV, Mubarak SJ: Muscular dystrophy, in Weinstein SL (ed): The Pediatric Spine, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 819-832.
Mubarak SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 45
What is the primary mechanism by which anabolic steroids increase muscle tissue? Review Topic
Explanation
Question 46
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
Explanation
REFERENCES: Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Rettig ME, Dassa GL, Raskin KB, Melone CP Jr: Wrist fractures in the athlete: Distal radius and carpal fractures. Clin Sports Med 1988;17:469-489.
Question 47
Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 48
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
Explanation
compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO but does not influence technique.
Question 49
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?

Explanation

These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.

Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.

Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.

Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.

The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 50
-A 30-year-old man sustained the injury seen in Figure 261. According to the Lauge-Hansen Classification System, the fracture should be classified as
Explanation

Question 51
What is the most common complication following surgical treatment of a displaced talar neck fracture?
Explanation
(SBQ12TR.14) Elevated interleukin 6 (IL-6) is most closely associated to which of the following clinical outcomes in orthopedic trauma patients?
Decreased mortality rates
Increased mortality rates
Decreased osteomyelitis infection rates
Increased rhabdomyolysis rates
Increased compartmental syndrome rates
Elevated levels of Interleukin 6 (IL-6) is most closely associated with higher injury severity scores and increased mortality rates in polytrauma orthopaedic patients.
Hyperstimulation of the inflammatory system by major trauma is considered to be the key element in the pathogenesis of severe inflammatory response syndrome and multi-organ dysfunction syndrome. IL-6 is a complex acute-reactant cytokinase that is expressed by cells in response to tissue injury. IL-6 levels are associated with injury severity, complications, and mortality. Patients with the most severe injuries have the highest IL-6 serum levels.
Sears et al. reviewed the markers of inflammation in major trauma. They suggest that interleukin-6 and human leukocyte antigen-DR class II molecules appear to have the greatest potential for use in predicting the clinical course and outcome in trauma patients. Early identification of traumatic patients, based on inflammatory markers and genomic predisposition, could help to guide intervention and treatment.
Pape et al measured the perioperative concentrations of interleukin-6 in sixty-eight blunt trauma patients with non-life threatening pelvic fractures. Release of proinflammatory cytokines were higher in patients undergoing surgical procedures that cause increased blood loss. The release of markers seems to be related to the type and magnitude of surgery, rather than to the duration of the procedure.
Illustration A shows a diagram of the acute inflammatory response after major trauma Incorrect Answers:
Question 52
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation? Review Topic

Explanation
Question 53
Up to what time frame are the risks minimized in anterior revision disk replacement surgery? Review Topic
Explanation
Question 54
The examination finding shown in Video 1 is consistent with which defect?
Explanation
The video shows the lack of tenodesis caused by the incompetence of the FDP tendon to the ring finger, which can be attributable to a laceration, tendon rupture, or avulsion. Note how the ring finger stays extended (compared to the other digits) when the extensor tendons are tightened during wrist extension. The other fingers are pulled into flexion by the FDP tendons when the extensor tendons are relaxed during wrist extension. With the wrist flexed, the extensor mechanism to all fingers appears to be functioning normally. Findings indicating a trigger finger would be locking in flexion of the proximal interphalangeal joint. FDS incompetence can only be detected by blocking FDP function of the other fingers and actively flexing the examined finger.
Question 55
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time? Review Topic
Explanation
sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter.
Question 56
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 57
- A 20-year-old college football player sustains a forceful hyperextension injury to his shoulder 4 months after undergoing an anterior capsular shift. Examination 2 weeks later reveals anterior tenderness. He is unable to lift the dorsum of his hand away from his back. What is the most likely diagnosis?
Explanation
Question 58
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 59
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 60
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 61
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
REFERENCES: Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Wolf EM, Cheng JC, Dickson K: Humeral avulsion of the inferior glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Question 62
Risk of fat embolism is greatest during what step of total hip arthroplasty?
Explanation
REFERENCES: Pitto RP, Koessler M, Kuehle JW: Comparison of fixation of the femoral component without cement and fixation with use of a bone-vacuum cementing technique for the prevention of fat embolism during total hip arthroplasty. J Bone Joint Surg Am
1999;81:831-843.
Christie J, Burnett R, Potts HR, Pell AC: Echocardiography of transatrial embolism during cemented and uncemented hemiarthroplasty of the hip. J Bone Joint Surg Br 1994;76:409-412.
Question 63
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of
Explanation
REFERENCES: Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
Question 64
Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?

Explanation
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. View Abstract at PubMed
Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. View Abstract at PubMed
Question 65
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
REFERENCES: Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Cantu RC: Criteria for return to competition after closed head injury, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby, 1991.
Question 66
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 67
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
REFERENCES: Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 165-201.
Question 68
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
REFERENCES: Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 961-990.
Question 69
A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of difficulty with running. Examination reveals developing swelling in the anterior mid-thigh area. The thigh compartments are soft, and he is able to extend his knee against gravity. Knee flexion at 90° gives him discomfort in the thigh but no knee pain. The knee and hip examinations are otherwise unremarkable. Plain films of the femur are negative. What is the best next step?
Explanation
A. only type 1 collagen.
B. only type 2 collagen.
C. type 1 and type 2 collagen.
D. neither type 1 or type 2 collagen.
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
15- Figures 1 and 2 are the radiographs of a 58-year-old retired laborer who has had many years of right shoulder pain. He initially experienced relief with anti-inflammatory medication over the past year, but this no longer provides him pain relief. He has pain with overhead activities and is dissatisfied with his shoulder function. Examination indicates active and passive forward elevation to 130°, full strength with external rotation, and a negative belly press test. MRI demonstrates an intact rotator cuff. What is the best next step in treatment?
A. Anatomic total shoulder arthroplasty (TSA)
B. Hemiarthroplasty
C. Reverse shoulder arthroplasty
D. Arthroscopy with debridement and biceps tenodesis
The patient has glenohumeral osteoarthritis based on the radiograph. His examination demonstrates limited motion and no significant rotator cuff pathology – full strength with external rotation, negative belly press, and no pseudoparalysis. Of all the answer choices, an anatomic TSA would be the most appropriate treatment option. Hemiarthroplasty does not address glenoid pathology and provides inferior pain relief and function, compared with TSA. A reverse shoulder arthroplasty is utilized for patients with degenerative shoulder changes in conjunction with irreparable rotator cuff pathology. Shoulder arthroscopy with debridement and biceps tenodesis is not appropriate for those with severe degenerative changes of the shoulder.
16- According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
A. Figure 2
B. Figure 3
C. Figure 4
D. Figure 5
The sagittal MRI scan is a clear example of a double posterior cruciate ligament (PCL) sign. This sign has a high specificity for a displaced bucket handle tear of the medial meniscus as seen in Figure 4. The other arthroscopic
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments. Correct answer : C 13
17- Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
A. Incorrect graft choice
B. Improper tunnel position
C. Tibial graft-tunnel mismatch
D. Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
Question 70
Examination of a 34-year-old man who has had left leg pain for the past 6 weeks reveals minimal weakness of the left extensor hallucis longus and normal ankle jerk and patellar reflexes. Figure 33 shows an axial MRI scan of the L4-5 disk. Based on these findings, the MRI scan results are consistent with compression of the
Explanation
REFERENCE: McCulloch JA, Young PH: Essentials of Spinal Microsurgery. Philadelphia, PA, Lippincott-Raven, 1998.
Question 71
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
Explanation
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.

Question 72
Which of the following statements best describes the instantaneous axis of rotation (IAR) for the functional spinal unit? Review Topic
Explanation
Question 73
A 55-year-old man is about to undergo right total hip arthroplasty. A preoperative AP pelvis radiograph is shown in Figure below. The final acetabular component and polyethylene liner are implanted. With the broach in place, the surgeon trials a standard offset neck and neutral length femoral head. The leg lengths are approximately equal, but the hip is unstable. What is the best next step?
Explanation
The radiograph shows that this patient has a high offset varus femoral morphology of both hips. Preoperative templating would identify this, and the surgeon should choose an implant system that has extended offset options to help match the native anatomy and biomechanics and minimize the risk of instability. Trialing a high offset neck, rather than a standard offset neck, is the next most appropriate step. Depending on the design of the implant system, this step can be accomplished by direct medialization of the femoral head, which would not affect leg length, or by lowering the neck angle, which would affect the leg length and would require a longer femoral head, because the leg lengths had previously been equal. Placement of a longer femoral head would likely improve hip stability but would also make the leg length uneven, which is a common cause of dissatisfaction after total hip arthroplasty. An offset acetabular liner also increases the leg length and does not correct the issue, which is on the femoral side. Trochanteric
advancement is sometimes used as a treatment for instability but would be inappropriate as the next step in this setting.
Question 74
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
REFERENCES: Chelly JE: Indications for upper extremity blocks, in Chelly JE (ed): Peripheral Nerve Blocks, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 19-27.
Misamore GW, Sallay PI: A prospective analysis of the safety and efficacy of interscalene brachial plexus block anesthesia for shoulder surgery. J Shoulder Elbow Surg 2007;16:e39.
Question 75
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure 62. Based on these findings, what is the most appropriate treatment?
Explanation
REFERENCES: Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Bellabarba C, Ricci WM, Bolhofner BR: Results of indirect reduction and plating of femoral shaft nonunions after intramedullary nailing. J Orthop Trauma 2001;15:254-263.
Question 76
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
Explanation
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma but would not lead to the clinical condition this patient has.
Question 77
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?
Explanation
REFERENCES: Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Gonzalez MH, Mekhail AO: The failed total knee arthroplasty: Evaluation and etiology. J Am Acad Orthop Surg 2004;12:436-446.
Question 78
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
REFERENCES: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 79
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?
Explanation
REFERENCES: Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000,
pp 598-601.
Question 80
A 42-year-old female undergoes a subtalar bone block distraction arthrodesis as sequelae of a nonoperatively treated calcaneus fracture ten years prior. This procedure addresses which of the following issues?

Explanation
Question 81
- Which of the following nerves supply the muscles on each side of internervous plane identified when performing the anterior (Smith-Petersen) approach to the hip?
Explanation
Question 82
A 48-year-old man undergoes arthroscopy to repair a rotator cuff tear. During the arthroscopy, the tear is characterized and found to involve the entire supraspinatus and a majority of the infraspinatus tendons. After mobilization, the posterior rotator cuff can reach the greater tuberosity. However, the supraspinatus tendon cannot reach its insertion point at the greater tuberosity. What is the most appropriate treatment? Review Topic
Explanation
release, reverse acromioplasty, and tenotomy of the biceps tendon may improve shoulder pain. If these procedures fail, then a muscle transfer procedure can also be considered in select patients. If, however, a portion of the rotator cuff can be repaired, even partial repair can balance the coronal and axial forces about the shoulder to restore the kinematics of the joint. Reverse total shoulder arthroplasty is not appropriate for this relatively young patient.
Question 83
What are the most likely symptoms and examination findings related to the mass in zone 2 of Guyon’s canal seen in Figure 17?
Explanation
REFERENCES: Kuschner SH, Gelberman RH, Jennings C: Ulnar nerve compression at the wrist. J Hand Surg Am 1988;13:577-580.
Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Question 84
A 72-year-old man with diabetic neuropathy and 5 degrees of valgus talar tilt; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
Arthritis of the ankle and hindfoot can pose challenges. Depending upon patient age, comorbidities, and alignment, a variety of surgical interventions may be offered. A total ankle replacement may be considered for patients older than 60 years of age who have minimal misalignment and low-demand lifestyles. In all other cases, ankle fusion must be considered. The nonsurgical care of ankle arthritis includes anti-inflammatory medication, intra-articular steroid injections, bracing with customized products such as the Arizona brace, or a molded foot and ankle orthosis.
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
Queen RM, Adams SB Jr, Viens NA, Friend JK, Easley ME, Deorio JK, Nunley JA. Differences in outcomes following total ankle replacement in patients with neutral alignment compared with tibiotalar joint malalignment. J Bone Joint Surg Am. 2013 Nov 6;95(21):1927-34. doi: 10.2106/JBJS.L.00404. PubMed PMID: 24196462. View Abstract at PubMed
Nunley JA, Caputo AM, Easley ME, Cook C. Intermediate to long-term outcomes of the STAR Total Ankle Replacement: the patient perspective. J Bone Joint Surg Am. 2012 Jan 4;94(1):43-8. doi: 10.2106/JBJS.J.01613. PubMed PMID: 22218381. View Abstract t PubMed
Saltzman CL, Mann RA, Ahrens JE, Amendola A, Anderson RB, Berlet GC, Brodsky JW, Chou LB, Clanton TO, Deland JT, Deorio JK, Horton GA, Lee TH, Mann JA, Nunley JA, Thordarson DB, Walling AK, Wapner KL, Coughlin MJ. Prospective controlled trial of STAR total ankle replacement versus ankle fusion: initial results. Foot Ankle Int. 2009 Jul;30(7):579-96. doi: 10.3113/FAI.2009.0579. PubMed PMID: 19589303. View Abstract at PubMed
Faraj AA, Loveday DT. Functional outcome following an ankle or subtalar arthrodesis in adults. Acta Orthop Belg. 2014 Jun;80(2):276-9. PubMed PMID: 25090803. View Abstract at PubMed Grear BJ, Rabinovich A, Brodsky JW. Charcot arthropathy of the foot and ankle associated with rheumatoid arthritis. Foot Ankle Int. 2013 Nov;34(11):1541-7. doi: 10.1177/1071100713500490. Epub 2013 Jul 30. PubMed PMID: 23900228. View Abstract at PubMed
Question 85
The MRI scan shown in Figure 33 reveals the sequelae of an acute traumatic anteroinferior shoulder dislocation. The image reveals the typical separation of what two commonly injured structures? Review Topic

Explanation
Question 86
All of the following techniques can help to prevent apex-anterior angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
Question 87
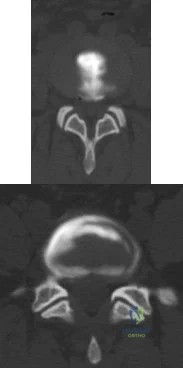
A 48-year-old man is brought in by emergency services after falling down a flight of stairs. He complains of weakness in both hands. Examination reveals weak grip bilaterally. Injury CT scans are shown in Figure A. What is the most appropriate treatment option? Review Topic
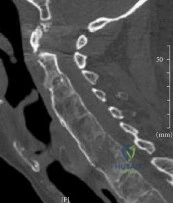
Explanation
The C-spine is the most common site of fracture in AS and is most susceptible to hyperextension injuries. When surgical intervention is required, multiple points of fixation both above and below the fracture are necessary. This is due to co-existing osteoporosis and abnormally increased forces from long lever arms of the ankylosed spine, both of which make the construct susceptible to failure and screw pullout.
Kubiak et al. reviewed the orthopaedic management of AS. They report bone scan, MRI or fine-cut CT is necessary because fractures are often missed on plain x-rays because of distortion of anatomy or difficulty with positioning.
Whang et al. reviewed spinal injuries in 12 patients with AS and 18 patients with DISH. Most injuries involved C5-C7. Patients with AS were more likley to have severe neurologic injury (41% ASIA A) than DISH (44% ASIA E). There was 81% good-excellent outcome and 4 deaths related to halo vest use.
Figure A is a sagittal CT reconstructed image showing a nondisplaced shear fracture through the C6 vertebral body and C5 posterior elements. Illustrations A and B are postop AP and lateral radiographs showing posterior decompression and C3-T2 fusion with lateral mass fixation in the cervical spine and pedicle screw fixation in the upper thoracic spine.
Incorrect Answers:
performed through a posterior approach. If there is significant osteoporosis and the risk of construct failure is high, a 360-approach may be necessary.
Question 88
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
REFERENCES: Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Durr HR, Krodel A, Trouillier H, Lienemann A, Refior HJ: Fibromatosis of the plantar fascia: Diagnosis and indications for surgical treatment. Foot Ankle Int 1999;20:13-17.
Question 89
What factor highly correlates with poor outcomes after surgery for femoroacetabular impingement? Review Topic
Explanation
Question 90
Figure 19 is the clinical photograph of a 54-year-old man who underwent a total ankle replacement (TAR). Three weeks after surgery he has increasing pain and a deep wound as seen in the photograph. What is the best next step?

Explanation
The patient is 3 weeks out from TAR. The wound is erythematous, and the tendon is visible. At 3 weeks this is an acute wound breakdown. The preferred treatment is a return to the operating room, an exchange of the polyethylene because the wound appears deep enough to go down to the joint, and a flap for coverage. Removal of the total ankle and placement of an antibiotic spacer should be considered in the settings of subacute (6 weeks postop) or chronic infection following TAR. A below-the-knee amputation may be considered with a failed salvage or a chronically infected TAR. Conversion to a fusion may be considered in situations in which the wound bed is not infected. In this case, there is concern for ongoing active infection, and an intercalary allograft is not appropriate.
RECOMMENDED READINGS
Cho EH, Garcia R, Pien I, Thomas S, Levin LS, Hollenbeck ST. An algorithmic approach for managing orthopaedic surgical wounds of the foot and ankle. Clin Orthop Relat Res. 2014 Jun;472(6):1921-9. doi: 10.1007/s11999-014-3536-7. Epub 2014 Feb 28. PubMed PMID:
Question 91
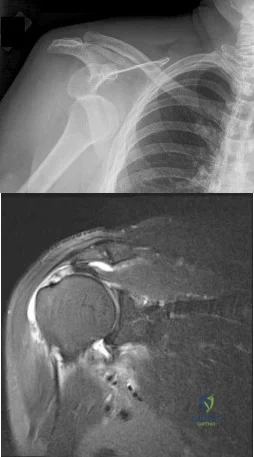
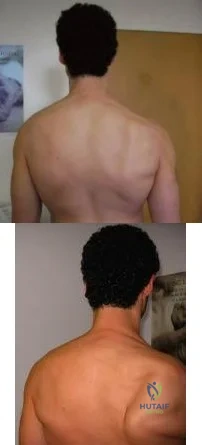
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B. What nerve is most likely injured? Review Topic
Explanation
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.
An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
An injury to the axillary nerve would result in deltoid muscle weakness.
An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging
Question 92
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a “pop” in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries.
Magn Reson Imaging Clin N Am 1999;7:39-49.
Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
Question 93
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 94
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 95
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include
Explanation
REFERENCES: Kempe CH, Silverman FN, Steele BF, et al: The battered-child syndrome. JAMA 1962;181:17-24.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 3, pp 2079-2082.
Question 96
A 52-year-old woman has right hip pain and obvious swelling 3 years after undergoing a resurfacing arthroplasty. Her implant consists of a 42-mm femoral component and 48-mm socket. Her components are well positioned, and her metal ion levels are slightly elevated (less than 4 ppm) with a normal erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level. What is the most likely cause of her discomfort?
Explanation
This patient likely has a soft-tissue reaction (pseudotumor) related to metal-on-metal articulation. Although the components are well positioned, patient gender and small head size are both known risk factors for failure of hip resurfacing arthroplasties. Metal ion levels are elevated but are not always markedly increased in the setting of a problematic metal-on-metal articulation. The patient should have a metal artifact reduction sequence MR imaging study to confirm the presence of a pseudotumor. Chronic infection is very unlikely in the setting of normal ESR and CRP findings. Impingement and lumbar disk disease would not explain the swelling around the hip.
Question 97
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule? Review Topic
Explanation
Question 98
A 45-year-old diabetic woman with a gangrenous foot undegoes a Chopart amputation without tendon transfer or lengthening. Which type of deformity is the most likely complication of this procedure?

Explanation
Advantages of the Chopart amputation include increased limb length and maintenance of heel proprioception that cannot be preserved with more proximal amputations.
Lieberman et al argue in patients with peripheral vascular disease, it is important to preserve as much tissue as possible to preserve maximum function. They recommend that with appropriate care, an amputation at the Chopart (calcaneocuboid-talonavicular) level can give a good functional result.
Question 99
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 100
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
REFERENCES: Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603.
Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med
1992;152:1985-1994.
