Orthopedic Board Exam MCQs: Trauma, Oncology & Joint Surgery Part 220

Key Takeaway
This page provides Part 220 of an OITE & ABOS Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs designed for orthopedic residents and surgeons. Ideal for certification exam preparation, it covers key topics like Ankle, Elbow, Fracture, Shoulder, and Tumor.
About This Board Review Set
This is Part 220 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 220
This module focuses heavily on: Ankle, Elbow, Fracture, Shoulder, Tumor.
Sample Questions from This Set
Sample Question 1: The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the...
Sample Question 2: What is the neoplastic cell of origin for this tumor?...
Sample Question 3: A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment sho...
Sample Question 4: During shoulder motion with the elbow controlled in a brace, electromyographic studies of the supraspinatus show significant activity with all range-of-motion testing. Concurrent electromyographic studies of the long head of the biceps will...
Sample Question 5: An 8-year-old boy weighing 70 lb sustains a displaced diaphyseal femur fracture and is treated with two flexible retrograde intramedullary rods. What is the most common complication following treatment with this technique? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Explanation
REFERENCES: Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 2
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 3
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of
Explanation
REFERENCES: Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibial physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Gruber HE, Phieffer LS, Wattenbarger JM: Physeal fractures: Part II. Fate of interposed periosteum in a physeal fracture. J Pediatr Orthop 2002;22:710-716.
Question 4
During shoulder motion with the elbow controlled in a brace, electromyographic studies of the supraspinatus show significant activity with all range-of-motion testing. Concurrent electromyographic studies of the long head of the biceps will most likely show
Explanation
REFERENCES: Yamaguchi K, Riew KD, Galutz LM, et al: Biceps activity during shoulder motion: An electromyographic analysis. Clin Orthop 1997;336:122-129.
Levy AS, Kelly BT, Lintner SA, et al: Function of the long head of the biceps at the shoulder: Electromyographic analysis. J Shoulder Elbow Surg 2001;10:250-255.
Question 5
An 8-year-old boy weighing 70 lb sustains a displaced diaphyseal femur fracture and is treated with two flexible retrograde intramedullary rods. What is the most common complication following treatment with this technique? Review Topic
Explanation
Question 6
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
REFERENCES: Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 7
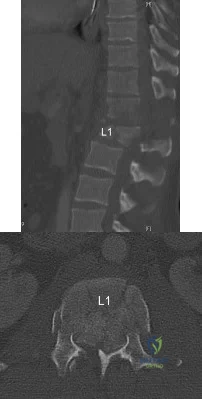
- A 31-year-old man who is a recent immigrant from Guatemala has had pain in his back and thighs for the past 12 months. History notes a recent diagnosis of gout, and the patient reports falling a distance of 3 feet on his buttocks immediately before the pain began. Examination reveals that he is neurologically intact. Plain radiographs are shown in Figures 44a and 44b, and T2-weighted MRI scans are shown in Figures 44c and 44d. The most likely cause of the pathologic fracture is
Explanation
The MR demonstrates involvement of L1 and adjacent disc spaces. With peri-vertebral edema and mass involving the posterior aspect of the vertebral body, placing pressure on the spinal cord. There is also involvement of the L2-3 disc with early signal changes.
The slow clinical course of the patients symptoms, being from a third world country and the findings on imaging studies, with an anterior wedge compression fracture. The level most commonly involved with TB is lower thoracic and upper lumbar. The anterior wedging results in the classic “Gibbus”.
Some of the MR findings are also consistent with metastatic disease, but with the localized mass, peri-vertebral abscess make this choice more unlikely.
The usual findings on MR found with TB are: Confluently decreased signal intensity of the vertebral bodies associated interspace with poor distinction between these on short TR/short TE images: Abnormal increased signal of the disk on long TR/long TE images with an abnormal configuration (i.e., absent intranuclear cleft): Increased signal of the vertebral endplates at the abnormal disk level on long TR/long TE images.
Question 8
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 9
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
REFERENCES: Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868.
Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 10
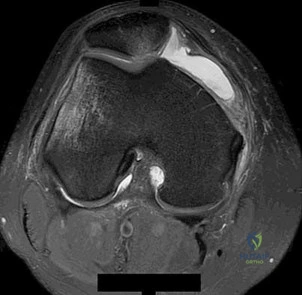
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
Explanation
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.

Question 11
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
Question 12
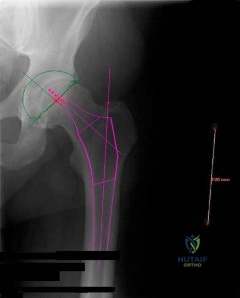
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
Explanation
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
Question 13
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.
Question 14
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
REFERENCES: Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89.
Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 15
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
White KK, Williams SK, Mubarack SJ: Definition of two types of anterior superior iliac spine avulsion fractures. J Pediatr Orthop 2002;22:578-582.
Question 16
A 42-year-old female with chronic discogenic back pain undergoes lumbar spine surgery via retroperitoneal approach. Figure A is the postoperative radiograph of her lumbar spine. Six weeks after the surgery the patient develops worsening low back pain. You obtain a radiograph of her lumbar spine, pictured in Figure B. What is the next best step in management? Review Topic

Explanation
Management of failed TDR is dictated by (1) patient symptoms and (2) radiographic implant position. Asymptomatic patients with implant subsidence without extrusion can be managed with close observation. Patients with persistent symptomatic back pain relating to facet joint or implant microinstability in the setting of an otherwise well-positioned TDR can be treated with posterior stabilization alone. Symptomatic patients with unacceptable implant position (i.e. complete dislodgement, fracture) require either revision arthroplasty or conversion to arthrodesis (anterior +/-
posterior).
Harrison et al. authored a report detailing a case of failed L5-S1 TDR with anterior dislocation of the polyethylene inlay and bilateral L5 pars fractures noted 2 weeks postoperatively. It is unclear whether the pars defect was missed following previous microdiscectomy, acquired during instrumentation, or acquired postoperatively due to abnormal endplate forces during rehabilitation. The patient underwent removal of TDR components and revision to anterior arthrodesis followed by percutaneous fixation of the bilateral L5 pars fractures.
Patel et al. published a review of the literature regarding revision lumbar TDR. Retroperitoneal revision procedures are complicated by higher risk of injury to vascular structures (16.7% versus 3.6% at primary surgery) and urogenital structures due to adhesions. Revision surgery should only be performed by surgeons familiar with the retroperitoneal approach to the spine. Alternative surgical approaches, such as the far lateral approach, should be considered to access the anterior spine at L4-L5 and above.
Madigan et al. reviewed the management of lumbar degenerative disc disease (DDD). They state that TDR is a motion-sparing surgical option designed to temper the problem of adjacent-segment disease. They report that long-term studies are limited, but point out that several short-term comparisons between TDR and ALIF show equivalent improvement in pain and function, equal complication rate, shorter hospitalization and lower rate of reoperation in the TDR group.
Figure A is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement. Figure B is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement with anterior dislocation of the polyethylene inlay.
Incorrect Responses:
Question 17
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
REFERENCES: Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Holtom PD: Antibiotic prophylaxis: Current recommendations. J Am Acad Orthop Surg 2006:14:S98-S100.
Question 18
A subtrochanteric femur fracture in which the lesser trochanter is intact is associated with what deformity?
Explanation
Question 19
In articular cartilage, Interleukin 1 (IL-1) increases
Explanation
Question 20
The mother of a healthy 8-month-old boy reports that her son refuses to use his left arm. Examination reveals that the arm hangs limp at his side in an adducted and internally rotated position, and the affected shoulder subluxates posteriorly. Passive external rotation measures 15 degrees. Management should consist of
Explanation
REFERENCES: Neer CS: Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990,
pp 452-454.
Pearl ML: Arthroscopy release of shoulder contracture secondary to birth palsy: An early report on findings and surgical technique. Arthroscopy 2003;19:577-582.
Pearl ML, Edgerton BW, Kon DS, et al: Comparison of arthroscopic findings with MRI and arthrography in children with GH deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 2003;85:890-898.
Question 21
When comparing arthroscopic and open rotator cuff repairs, which of the following tears shows a decreased recurrent tear rate in the open versus the arthroscopic group? Review Topic
Explanation
Question 22
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the
Explanation
REFERENCES: Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Nawab A, Hester PW, Caborn DN: Arthroscopic meniscus repair, in Miller MD, Cole BJ (eds): Textbook of Arthroscopy. Philadelphia, PA, WB Saunders, 2004, pp 517-537.
Question 23
A 44-year-old woman has had lower extremity dysesthesias, urinary incontinence, and has been unable to walk for the past 2 days. She reports no pain or history of trauma. She notes that 3 weeks ago she missed work for 2 days because of back pain, but it resolved with rest. Examination shows decreased or absent sensation below the knees, no motor function below the knees, and decreased rectal tone. Catheterization results in a postvoid residual of 2,000 mL. Plain radiographs and MRI scans without contrast are shown in Figures 1a through 1d. What is the next most appropriate step in management?
Explanation
REFERENCES: Eichler ME, Dacey RG: Intramedullary spinal cord tumors, in Bridwell KH, Dewald RL (eds): The Textbook of Spine Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, vol 2, pp 2089-2116.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 81-87.
Question 24
Which of the following substances is least likely to affect the success of bone union after lumbar arthrodesis?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
Dimar JR II, Ante WA, Zhang YP, Glassman SD: The effect of nonsteroidal anti-inflammatory drugs on posterior spinal fusions in the rat. Spine 1996;21:1870-1876.
Question 25
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
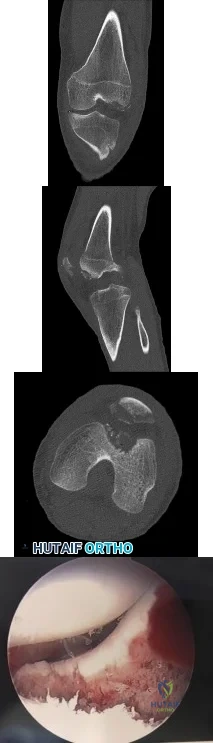
Explanation
Question 26
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
REFERENCES: Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
Heydarian K, Akbarnia BA, Jabalameli M, Tabador K: Posterior capsulotomy for the treatment of severe flexion contractures of the knee. J Pediatr Orthop 1984;4:700-704.
Question 27
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time? Review Topic
Explanation
Question 28
Type II collagen in nondiseased adult human articular cartilage has a half-life that is generally
Explanation
REFERENCES: Maroudas A, Palla G, Gilav E: Racemization of aspartic acid in human articular cartilage. Connect Tissue Res 1992;28:161-169.
Verzijl N, DeGroot J, Thorpe SR, et al: Effect of collagen turnover on the accumulation of advanced glycation end products. J Biol Chem 2000;275:39027-39031.
Question 29
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30° of flexion, which decreases as the knee is flexed to 90°. What is the most likely diagnosis?
Explanation
REFERENCES: Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 30
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
Explanation
REFERENCES: Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.
Young CF, Nanu AM, Checketts RG: Seven-year outcome following Colles’ type distal radial fracture: A comparison of two treatment methods. J Hand Surg Br 2003;28:422-426.
Question 31
Figures 45a and 45b show the CT scans of a 41-year-old man who was ejected from a vehicle after a high-speed collision. Examination reveals weak (2/5) toe flexion on the right side, but otherwise he has no voluntary motor function in his lower extremities and no sensation. He has some perianal sensation. He has no other associated injuries and his upper extremities are neurologically intact. Which of the following represents the best treatment option? Review Topic
Explanation
(SBQ12SP.25) A 63-year-old female undergoes lumbar decompression and instrumented fusion for the condition shown in Figure A and B. Which of the following factors are associated with increased risk of early post-operative complications? Review Topic

Increasing Age
Intraoperative blood loss
Number of levels fused
All of the above
Age, intraoperative blood loss, and number of spinal levels fused are associated with increased rates of inpatient complication following lumbar decompression and fusion for degenerative spondylolisthesis. Older age correlates with the highest risk for complications.
Lumbar decompression and fusion is well supported in the literature to be effective in the treatment of degenerative spondylolithesis when nonoperative modalities fail. Common complications associated with lumbar decompression and fusion include asymptomatic or symptomatic pseudarthroses (estimated 5-30%), surgical site infection (0.10-2%),and adjacent level degeneration (2-3%). Age, intraoperative blood loss, longer operative times, number of levels fused are associated with increased risk of complication. Smoking is associated with worse outcome after surgery.
Kalanithi et al. reviewed the Nationwide Inpatient Sample adminstrative data on sixty six thousand patients undergoing lumbar laminectomy and fusion. They found the increased age and having 3 or more medical comorbidities was associated with increased risk of complication.
Carreon et al. reviewed cases of ninety eight patients who underwent laminectomy and fusion for lumbar degenerative disease. They found that rates of major and minor complication increased with older age, increased blood loss, longer operative time, number of levels fused.
Figure A is a AP lumbar spine radiograph. Figure B is a lateral lumbar spine radiograph showing degenerative spondylolisthesis at L4-L5. Illustration A shows the postoperative images of the patient treated with an L4-5 fusion with an interbody device.
Incorrect
Question 32
An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?
Explanation
REFERENCES: Hornicek FJ, Zych GA, Hutson JJ, Malinin TI: Salvage of humeral nonunions with onlay bone plate allograft augmentation. Clin Orthop 2001;386:203-209.
Jupiter JB: The treatment of complex non-unions of the humeral shaft with a combination of surgical techniques. J Bone Joint Surg Am 1990;72:701-707.
Question 33
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
Explanation
REFERENCES: Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.
Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Question 34
A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
Explanation
Question 35
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
REFERENCES: Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
p 52.
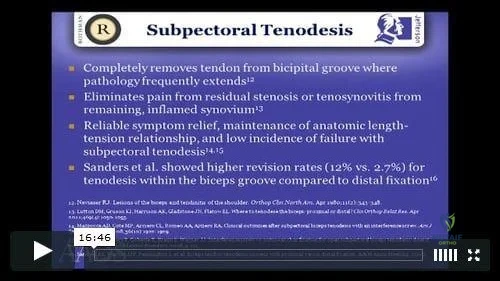
Question 36
Figure 7 is the MR image of a 43-year-old man who has left shoulder pain with a traumatic rotator cuff tear after a fall. An examination reveals active forward elevation at 120 degrees and positive Yergason and lift-off test results. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time?
Explanation
Video 7 for reference
The MR image shows medial subluxation of the biceps tendon, which can be confused with an articular loose body. In the clinical scenario of biceps instability/subluxation, the rationale regarding tenodesis is to address the painful dislocation and subluxation of the biceps tendon from the bicipital groove.
The MR image does not show a loose body or Bankart lesion. Patients with irreparable rotator cuff tears with a severe external rotation deficit and a deficient teres minor may experience a better functional result with latissimus dorsi transfer.
Question 37
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 38
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intraoperatively, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation
Question 39
A 45-year-old IV drug abuser has sternoclavicular (SC) joint pain for the past 2 weeks. He is afebrile and physical exam findings include point tenderness and swelling. He most likely has septic arthritis of the sternoclavicular joint. If so, what is the most likely infecting organism?

Explanation
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
Question 40
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?
Explanation
The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images.
REFERENCES: Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Mink JH, Deutsch AL: The knee, in MRI of the Musculoskeletal System, ed 1. New York, NY, Raven Press, 1990, pp 251-387.
Question 41
Which of the following cohorts of patients is at highest risk of a future anterior cruciate ligament (ACL) tear? Review Topic
Explanation
Question 42
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.

Question 43
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
REFERENCES: Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 44
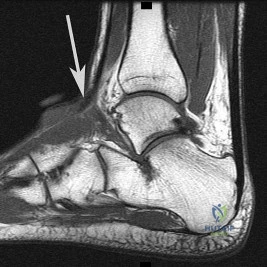
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 45
Figures 37a and 37b show radiographs of a 24-year-old man who has a humeral bone lesion that was found during a screening chest radiograph. He denies any symptoms despite leading a very active lifestyle. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 46
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 47
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured?
Explanation
REFERENCES: O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
O’Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
Question 48
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
www.watchtower.org. Official Web Site of Jehovah’s Witnesses. Link verified as active as of August 8, 2008.
Question 49
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include
Explanation
The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome.
REFERENCES: Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250.
Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 339-365.
Question 50
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies?
Explanation
REFERENCES: Unkila-Kallio L. Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Herring JA(ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia. PA. WB Saunders, 2008, pp 2090-2100.
AL-Madena Copy
Question 51
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92?
Explanation
REFERENCES: Vellet AP, Marks PH, Fowler PJ, et al: Occult posttraumatic osteochondral lesions of the knee: Prevalence, classification, and short-term sequelae evaluated with MR imaging. Radiology 1991;178:271-276.
Cone R: Imaging sports-related injuries of the knee, in DeLee J, Drez D, Miller M (eds): DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 2, pp 1595-1652.
Question 52
When the data are normally distributed, what statistical test is best used to compare means of three or more independent groups?
Explanation
Question 53
A new composite material is being evaluated for potential use as a prosthetic ligament. In measuring the tensile strength of this material, why is it important to consider and accurately control the loading rate?
Explanation
Question 54
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy. D. improved long-term survivorship profile.
Question 55
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis?
Explanation
REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
Emami A, Deviren V, Berven S, et al: Outcome and complications of long fusions to the sacrum in adult spine deformity: Luque-Galveston, combined iliac and sacral screws, and sacral fixation. Spine 2002;27:776-786.
Question 56
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Easley ME, Trnka HJ, Schon LC, Myerson MS: Isolated subtalar arthrodesis. J Bone Joint Surg Am 2000;82:613-624.
Question 57
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
REFERENCES: McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654.
Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study.
J Bone Joint Surg Am 2003;85:773-781.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 58
Which of the following antibiotics is contraindicated in children?
Explanation
REFERENCE: Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 59
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?

Explanation
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter. Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
Question 60
The use of nonsteroidal anti-inflammatory drugs following femoral nailing has been associated with which of the following?

Explanation
Giannoudis et al assessed factors which could affect union in 32 patients with nonunion of a fracture of the diaphysis of the femur and 67 matched patients whose fracture had united. They found that there was no relationship between the rate of union and the type of implant, mode of locking, reaming, distraction or smoking. They also concluded that there was a marked association between nonunion and the use of NSAIDs after injury and delayed healing was noted in patients who took NSAIDs and whose fractures had united.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Question 61
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Unni KK, Dahlin DC, Beabout JW, Ivins JC: Parosteal osteogenic sarcoma. Cancer 1976;37:2466-2475.
Question 62
Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
Explanation
Question 63
Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic
Explanation
Question 64
A 16-year-old boy who is a competitive basketball player (Figure 43)
Explanation
Question 65
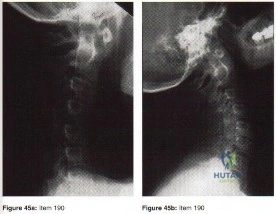
Explanation
In the context of viewing a lateral cervical spine to evaluate cranial setting, multiple lines can be used to assess anatomic relationships (i.e. McRae’s Chamberlin’s, or McGregor’s) McRae’s and Chamberlin’s use the foramen magnum as one land mark. Commonly, however, the margins of the foramen magnum are difficult to precisely identify. McGregor’s line connects the posterior margin of the hard palate to the most caudal point of the occiput and is easier to use. The tip of the odontoid should not project more than 4.5 mm above this line.
Anterior subluxation of more than 10-12 mm implies destruction of the entire ligamentous complex.
An atlantoaxial distance greater than 3.5mm is considered abnormal in an adult. The subaxial cervical spine is affected through involvement of the facets, interspinous ligaments, and intervertebral discs (spondylodiscitis). The initial site of destruction has been postulated to be through synovitis of the neurocentral joints with erosion of the adjacent disc and bone causing subluxation, or through primary facetal arthritis and ligamentous laxity causing secondary chronic discovertebraltrauma and destructive hypermobile segmentsis associated with disc destruction and toward the C2-C3 and C3-C4 segments, typically lack osteophytes, and often are at multiple levels, giving a stepladder appearance.
Question 66
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.
Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.
Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 67
-Which gene correlates with severity of disease in spinal muscular atrophy (SMA)?
Explanation
The other choices are not associated with spinal muscular atrophy.Defects in PMP22 are the cause of 70% to 80% of cases of Charcot-Marie-Tooth disease. Mutations in the dystrophin gene cause Duchenne muscular dystrophy.
Question 68
A 61-year-old right-hand-dominant woman falls down the stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
Explanation
<3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range
of motion is important to avoid stiffness.
Question 69
This condition is most prevalent in people of which ancestry?
Explanation
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.

Question 70
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient’s left knee. Abnormal findings include
Explanation
REFERENCES: Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Andrish JT: Meniscal injuries in children and adolescents: Diagnosis and management.
J Am Acad Orthop Surg 1996;4:231-237.
Question 71
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient? Review Topic
Explanation
Question 72
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 73
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the
inability to gain purchase for extraction.
Question 74
- Figure 67 shows the AP radiograph of both knees of a 26-year-old woman. A review of the patient’s medical record will most likely reveal a history of
Explanation
Question 75
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 76
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 77
Figure 31 is the sagittal MR image of a 30-year-old man with a clear-cell sarcoma of the foot. There is no evidence of disease elsewhere after standard staging of a soft-tissue sarcoma.
Explanation
For patients with rapidly enlarging painless masses, particularly those that are either large or deep, the diagnosis of a soft-tissue sarcoma should be entertained. Masses exceeding 5 cm in largest dimension that are subfascial and heterogenous on MRI are concerning. MRI with and without contrast is the preferred imaging modality for evaluation of soft-tissue sarcomas because it can delineate location of the lesion, involvement of neurovascular structures, intra-articular involvement, and underlying signal alteration in the osseous structures. Most patients can relate the onset of their symptoms to a traumatic event, and the interpretation of an MRI may include a hematoma. Ultrasound is more commonly used to confirm the clinical impression of a cyst and to distinguish cystic from solid masses.
A core needle biopsy can easily be performed in an outpatient setting or with image guidance to aid in the diagnosis. Core needle biopsies preserve the architectural relationship of cells, which is important in the diagnosis of mesenchymal lesions. A core needle biopsy is appropriate for soft-tissue lesions and osseous lesions and should be performed in a multidisciplinary setting with a surgeon performing the resection so unnecessary compartmental contamination is not introduced into the needle tract.
A fine-needle aspiration allows cytologic but not histologic analysis and generally is not favored for the diagnosis of a sarcoma. If an open biopsy is performed, the incision must be oriented in line with the long axis of the extremity to minimize contamination of surrounding structures. Meticulous hemostasis and closure of the tumor pseudocapsule must be achieved to minimize local tissue contamination. An open biopsy is commonly used if an initial needle biopsy is nondiagnostic. Transverse biopsy incisions should not be used.
Presurgical radiation for sarcomas is advantageous to decrease the field of radiation and overall radiation dose, but a significant postsurgical wound-healing complication rate (up to 35%) is associated with presurgical radiation therapy.
Staging of sarcomas is important to help predict prognosis. Not all sarcomas are reliably positive on a PET scan, so the preferred staging studies are CT scan of the chest and whole-body bone scan. Hematogenous spread of sarcomas is the most common route of metastatic disease, which speaks to the value of chest CT scans. Clear-cell sarcomas (in addition to synovial sarcoma, angiosarcoma, epithelioid sarcoma, and rhabdomyosarcoma) tend to involve lymphatic nodal metastatic disease, so sentinel node biopsy is considered when assessing these tumors. Evidence supports efficacy of sentinel node biopsy for clear-cell sarcomas in particular.
RECOMMENDED READINGS
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer; 2010.
Arbeit JM, Hilaris BS, Brennan MF. Wound complications in the multimodality treatment of extremity and superficial truncal sarcomas. J Clin Oncol. 1987 Mar;5(3):480-8.View Abstract at PubMed
Luce EA. The irradiated wound. Surg Clin North Am. 1984 Aug;64(4):821-9. PubMed PMID: 6591499. View Abstract at PubMed
Cheng EY, Dusenbery KE, Winters MR, Thompson RC. Soft tissue sarcomas: preoperative versus postoperative radiotherapy. J Surg Oncol. 1996 Feb;61(2):90-9.View Abstract at PubMed
Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg Am. 1982 Oct;64(8):1121-7. View Abstract at PubMed
Singer S, Nielsen T, Antonescu CR. Molecular biology of soft tissue sarcoma. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1522-1532.
Singer S, Maki RG, O'Sullivan B. Soft tissue sarcoma. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1533-1577.
Malawer MM, Helman LJ, O'Sullivan B. Sarcomas of bone. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1578-1609.
O'Sullivan B, Davis AM, Turcotte R, Bell R, Catton C, Chabot P, Wunder J, Kandel R, Goddard K, Sadura A, Pater J, Zee B. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet. 2002 Jun 29;359(9325):2235-41. View Abstract at PubMed
Andreou D, Boldt H, Werner M, Hamann C, Pink D, Tunn PU. Sentinel node biopsy in soft tissue sarcoma subtypes with a high propensity for regional lymphatic spread--results of a large prospective trial. Ann Oncol. 2013 May;24(5):1400-5. doi: 10.1093/annonc/mds650. Epub 2013 Jan 31. PubMed PMID: 23372051. View Abstract at PubMed
Question 78
Total hip arthroplasty in a patient with a long-standing hip fusion on the contralateral side is most likely to result in
Explanation
REFERENCES: Garvin KL, Pellicci PM, Windsor RE, et al: Contralateral total hip arthroplasty or ipsilateral total hip arthroplasty in patients who have long-standing fusion of the hip. J Bone Joint Surg Am 1989;71:1355-1362.
Gore DR, Murray MP, et al: Walking patterns of men with unilateral surgical hip fusion. J Bone Joint Surg Am 1975;57:759-765.
Romness DW, Morrey BF: Total knee arthroplasty in patients with prior ipsilateral hip fusion. J Arthroplasty 1992;7:63-70.
Question 79
A patient with Pott's disease, tuberculosis of the spine, is more likely to have which of the following early findings? Review Topic
Explanation
Question 80
Lumbar disk replacement has been shown to offer which of the following results?
Explanation
REFERENCES: Geisler FH, Blumenthal SL, Guyer RD, et al: Neurological complications of lumbar artificial disc replacement and comparison of clinical results with those related to lumbar arthrodesis in the literature. J Neurosurg Spine 2004;1:143-154.
Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 81
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
REFERENCES: Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Roy S, Caine D, Singer KM: Stress changes of the distal radial epiphysis in young gymnasts: A report of twenty-one cases and a review of the literature. Am J Sports Med 1985;13:301-308.
Question 82
An 83-year-old right-hand-dominant woman sustains a displaced right extra-articular distal radius fracture and is treated with closed reduction and casting. At her 4-week follow-up visit, radiographs demonstrate a volar tilt of -5 degrees and 4 mm of positive ulnar variance. Which treatment is recommended?
Explanation
Studies demonstrate that surgical treatment of distal radius fractures in elderly people does not result in improved outcomes. Although nonsurgical treatment resulted in worse radiographic findings for this patient, these findings did not translate into worse functional outcomes.
RECOMMENDED READINGS
Diaz-Garcia RJ, Oda T, Shauver MJ, Chung KC. A systematic review of outcomes and complications of treating unstable distal radius fractures in the elderly. J Hand Surg Am. 2011 May;36(5):824-35.e2. doi: 10.1016/j.jhsa.2011.02.005. Review. PubMed PMID: 21527140.
View Abstract at PubMed
Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. View Abstract
at PubMed
American Academy of Orthopaedic Surgeons: Treatment of Distal Radius Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons, March 2013. Available at http://www.aaos.org/research/Appropriate_Use/drfauc.asp Accessed {10/8/14}. Last Accessed on 10/8/14
Question 83
The addition of which of the following food supplements may lead to a decrease in neural tube defects?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 111-122.
Lemke L, Dias L: Spina bifida, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 203-210.
Question 84
A 7-year-old boy with spastic diplegia is a limited community ambulator. He has a moderately severe crouched gait. The parents request a treatment that will result in a permanent decrease in lower extremity muscle tone. This is best accomplished with Review Topic
Explanation
Question 85
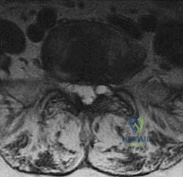
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time? Review Topic
Explanation
point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.
(SBQ12SP.20) Amphotericin B is most appropriate for the treatment of which type of spine infection? Review Topic
Fungal osteomyelitis
Bacterial osteomyelitis with a gram-positive organism
Bacterial osteomyelitis with a gram-negative organism
Tuberculous osteomyelitis
Viral meningomyelitis
Amphotericin B would be most appropriate for the treatment of fungal infections of the spine.
Amphotericin B is a broad-spectrum anti-fungal medication. It is commonly used as the first-line agent for treatment of fungal infections of the spine. The most common fungi involving the spine include cryptococcus, candida, and aspergillus. The indications for débridement and stabilization with spinal fusion, includes resistance to antibiotic therapy, spinal instability, and/or neurologic deficits.
Kim et al. reviewed fungal infections of the spine. They comment that fungus infections are most commonly spread by hematogenous or direct spread. Access to the vascular system may include intravenous lines, during implantation of prosthetic devices, or during surgery.
Frazier et al. retrospectively reviewed 11 patients with fungal osteomyelitis of the spine. Nine of the patients were immunocompromised secondary to diabetes mellitus, corticosteroid use, chemotherapy for a tumor, or malnutrition. All were treated with anti-fungal medication. 10 of 11 patients were also treated with surgical debridement. Paralysis secondary to the spine infection developed in eight patients. After an average of 6.3 years of follow-up, the infection had resolved in all nine surviving patients.
Illustration A shows the mechanism of action of Amphotericin. Illustration B shows T1- (Image A and B) and T2-weighted (Image C) images of the lower thoracic and lumbar spine. There are hypointense signals within the T12 and L1 vertebral bodies (Images A and B) indicative of fungal osteomyelitis.
IncorrectAnswers:
Question 86
Figure 45 shows the lateral radiograph of a 19-year-old swimmer who has had back pain for the past 2 months. What is the most likely diagnosis?
Explanation
REFERENCES: Papanicolaou N, Wilkinson RH, Emmans JB, Treves S, Micheli LJ: Bone scintigraphy and radiography in young athletes with low back pain. Am J Roentgenol 1985;145:1039-1044.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 291-302.
Question 87
A 58-year-old woman underwent a left total knee arthroplasty 6 years ago. She initially did well after surgery but sustained a fall 2 months ago while at work. She now describes left knee pain and instability and an inability to straighten her knee since the fall. She has been using a hinged knee brace, which provides partial support. On examination, she has passive range of motion of 0° to 115° and active range of motion of 80° to -115°. Her radiographs are shown in Figures below. What is the best option for the restoration of her function?

Explanation
The patient has an extensor mechanism disruption with patellar tendon rupture. This injury is treated with extensor mechanism reconstruction in the setting of previous total knee arthroplasty. There is a reported high failure rate with attempted repair. Revision to hinge knee arthroplasty would provide implant stability but would not restore the extensor mechanism. The patient is relatively young and is working, so reconstruction would offer better long-term function than a drop lock brace, which can be better used in low-functioning patients with this type of injury. Extensor mechanism reconstruction historically has been accomplished with allograft material, but a novel technique using synthetic mesh also has proved successful in treating this difficult problem.
Question 88
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively? Review Topic

Explanation
Question 89
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 90
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
Question 91
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
REFERENCES: Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Weber TG, Manoli A II: Compartment syndromes of the foot. Foot Ankle Clin 1999;4:473-486.
Question 92
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals? Review Topic
Explanation
Question 93
-The center of rotation of the knee can be best described as
Explanation
Question 94
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
Explanation
6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia.
REFERENCES: Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Bazaz R, Lee MJ, Yoo JU: Incidence of dysphagia after anterior cervical spine surgery:
A prospective study. Spine 2002;27:2453-2458.
Question 95
All of the following are characteristic of synovium affected by rheumatoid arthritis (RA) EXCEPT:
Explanation
Normal synovium consists of two layers, the intimal and the sublining, and two types of cells, type A and B. In RA, the following changes to the synovium are seen: 1) hyperplasia, with the intimal lining increasing from two cell layers to 10-20 layers 2) decreased apoptosis of the lining 3) increased angiogenesis and 4) abundant lymphocytes around vessels, forming lymphoid follicles.
The synovial pannus is invasive granulation tissue that contains fibroblast-like synoviocytes, but few inflammatory cells. The synovial cells in the pannus have anchorage-independent growth and invasive capabilities, allowing them to directly attack and destroy articular cartilage.
Koch et al. note that the possible contributions of angiogenesis to the proliferation of the inflammatory synovial pannus and the ingress of inflammatory leukocytes into the synovial tissue in RA have been extensively studied. Relevant angiogenesis inducers seen in RA include FGF-2, VEGF, TGFß, TNFa, IL-1, IL-8, VCAM-1, among others. Modulation of angiogenesis may be a viable therapeutic option for RA in the future.
Incorrect Answers:
Question 96
-A 32-year-old man who is a smoker sustained an open tibial fracture and underwent a staged treatment with placement of an intramedullary nail. Four weeks after surgery, he developed a pseudomonas deepwound infection. What is the strongest predictor of persistent infection if implants are retained until fracture union?
Explanation

Question 97
A 33-year-old female sustains the injury shown in Figure A as the result of a fall off a chair, and subsequently undergoes operative stabilization of her injury. Which of the following is most correlated with positive outcomes when treating this injury?

Explanation
While the importance of anatomic reduction of a syndesmotic injury is clear, controversy exists regarding the ideal method of fixation. No significant differences are reproducibly reported in regards to number of syndesmotic screws, size, or number of cortices. There is emerging data supporting the use of suture button fixation.
Wikeroy et al. reviewed 48 patients at a mean of 8.4 years, and they found that patients with a difference in the syndesmotic width between the operated and the nonoperated ankle of 1.5 mm or more showed inferior results. Posterior malleolar fragments and obese patients also had worse outcomes.
Schepers et al. published a review on the suture button device comparisons to traditional screw fixation, reviewing 6 biomechanical studies and 34 clinical studies. They found that the suture button systems have similar outcomes to screw fixation, but insufficient long-term and high-quality evidence prevented a strong conclusion. Implant removal in the suture button groups averaged 10%, while screw removal averaged 52%.
Sagi et al. reviewed 107 patients with ankle fractures and associated syndesmotic
injuries requiring surgery. They found that 39% were malreduced, but open reduction of the syndesmotic injury cut the malreduction rate by 2/3. They also reported that at a minimum of 2 years follow-up, patients with malreduced syndesmotic injuries demonstrated worse functional outcome scores.
Figure A shows an ankle fracture with obvious syndesmotic injury/widening. Incorrect answers:
1-4: These choices are not correlated with excellent outcomes with treatment of a
syndesmotic injury.
Question 98
The brachialis muscle is innervated by what two nerves?
Explanation
REFERENCES: Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
King A, Johnston GH: A modification of Henry’s anterior approach to the humerus. J Shoulder Elbow Surg 1998;7:210-212.
Question 99
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What is the most appropriate course of action for this patient’s condition?
Explanation
diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 100
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
REFERENCE: Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU: Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg 1995;4:41-50.
