OITE & ABOS Orthopedic Board Exam MCQs: Sports Medicine, Reconstruction, Trauma - Part 244

Key Takeaway
This page is Part 244 of an expert-authored MCQ bank for orthopedic surgeons. It offers 100 verified, high-yield questions for OITE/AAOS board exam prep. Covering Arthroscopy, Hip, Knee, Shoulder, this interactive quiz enhances clinical knowledge and readiness for certification success.
About This Board Review Set
This is Part 244 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 244
This module focuses heavily on: Arthroscopy, Cartilage, Fracture, Hip, Knee, Shoulder.
Sample Questions from This Set
Sample Question 1: What structure is the primary restraint to inferior translation of the shoulder?...
Sample Question 2: A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degr...
Sample Question 3: -The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is ...
Sample Question 4: -A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with internation...
Sample Question 5: A 26-year-old female twists her knee while playing soccer and sustains the injury shown in Figure A. She undergoes a reconstructive surgery and is started on an accelerated rehabilitation program. Which of the following is true regarding th...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive Exam
00:00
Start Quiz
Question 1
What structure is the primary restraint to inferior translation of the shoulder?
Explanation
REFERENCES: Harryman DTII, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53 -66.
Bigliani LU, Pollock RG, Soslowsky LJ, et al: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 2
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
REFERENCES: Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496.
Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 3
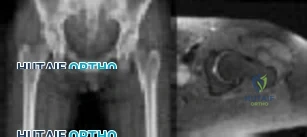
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
Explanation
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
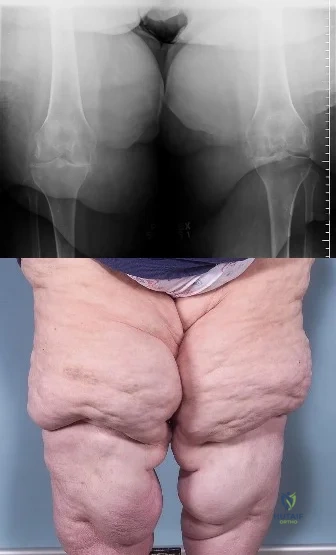
CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.


Question 4
-
A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Explanation
Question 5
A 26-year-old female twists her knee while playing soccer and sustains the injury shown in Figure A. She undergoes a reconstructive surgery and is started on an accelerated rehabilitation program. Which of the following is true regarding this type of rehabilitation protocol? Review Topic

Explanation
Rehabilitation after ACL reconstruction is necessary for a successful surgical outcome and remains an important topic of research interest. Accelerated programs allow for earlier weightbearing and certain strengthening exercises, rather than waiting several weeks before performing certain activities which put strain on the graft. Despite initial concerns that accelerated rehabilitation programs may lead to worse outcomes, many studies have demonstrated comparable outcomes between accelerated and nonaccelerated rehabilitation programs. No significant long-term differences have been reported regarding ACL laxity, range of motion, strength, or return to sports. Use of an accelerated program does not imply earlier return to sports. The optimal time to return to sports has not yet been elucidated.
Beynnon et al. performed a randomized controlled trial of patients who underwent ACL reconstruction with bone-patellar tendon-bone autograft comparing rehabilitiaton with either accelerated (19 week) or nonaccelerated (32 week) programs. At final evaluation, patients in both programs had the same increase in the envelope of knee laxity, clinical assessment, functional performance, proprioception,
and
thigh
muscle
strength.
Kruse et al. presented a systematic review evaluating studies on rehabilitation following ACL reconstruction. The authors found that accelerated rehabilitation does not appear to be harmful. It is likely safe for patients to begin immediate postoperative weight bearing, range of motion from 0-90 degrees of flexion, and perform closed-chain exercises. Bracing following ACL reconstruction is neither necessary nor beneficial and often adds to the cost of the procedure.
Figure A is a sagittal MRI demonstrating a complete ACL tear.
Incorrect
Question 6
belowdepicttheAPandlateralradiographsobtainedfromayear-oldmanwithlong-standing
rightkneeosteoarthritisandpainthatisunresponsivetononsurgicaltreatment.Thepatientundergoes navigatedcruciate-retainingrighttotalkneearthroplasty.Aftersurgery,thispatientcontinuesto experiencepainandswellingofthekneewithrecurrenteffusions.Hereturnstotheofficereporting continuedpain2yearsaftersurgery.Hedescribesinstability,particularlywhendescendingstairs.On examination,rangeofmotionof0°to120°isobserved,withnoextensorlag.Slopeofthetibialcomponent is7°.Thekneeisstabletovarusandvalgusstressinextension,butflexioninstabilityispresentinboth theanterior-posteriordirectionandthevarus-valgusdirection.Bracingleadstoaslightdecreasein symptomsbutisnotwelltolerated.Isokinetictestingdemonstratesdecreasedkneeextensionvelocityat
midpush.Radiographsdemonstratewell-alignedandfixedkneeimplants.Aninfectionwork-upis negative.Whatisthemostappropriatesurgicalinterventionatthistime?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 7
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 8
What is the main function of collagen found within articular cartilage?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 9
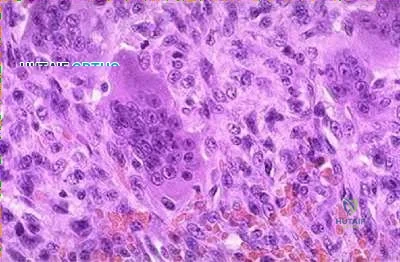
Giant cell tumors of bone can occur in many different areas throughout the body. All of the following are common locations for giant cell tumors of bone EXCEPT?
Explanation
Giant cell tumors are one of the more common tumors in young adults 22-40 years of age. There is much argument as to whether giant cell tumors arise in the metaphysis or the epiphysis, but most authors agree that giant cell tumors are very uncommon in the diaphysis. The most common sites of giant cell tumors in bone, which are the distal radius, sacrum, distal femur, proximal tibia and proximal humerus. Treatment typically involves intralesional curettage with adjuvant treatment (e.g., phenol, hydrogen peroxide, argon beam, etc).
Williams et al undertook a prospective study to evaulate the recurrence rate of giant cell tumors of the hand and they found that soft tissue extension of the tumor significantly increased the rate of local recurrence. This finding is significant because multiple previous studies have demonstrated similar higher recurrence rates for giant cell tumors with soft tissue extension in other areas like around the knee and the distal radius.
Illustration A are radiographs classic for a giant cell tumor showing a large lytic metaphseal-epiphyseal lesion in the distal femur. Illustration B is an axial CT of the distal femur showing the lytic giant cell tumor, abutting and fracturing the subchondral bone. Illustration C is histology classic for a giant cell tumor where the nuclei of the multi-nucleated giant cells look identical to the nuclei of the stromal cells.
Incorrect Answers:


What is the most appropriate treatment for a 65-year-old female with a 100-pack-year tobacco history who presents with a new painful lytic lesion in her femoral diaphysis?
Antegrade femoral nailing with reamings sent to pathology for analysis
Antegrade femoral nailing with adjuvant radiotherapy to the lesion 3
. Minimally invasive plating of the femur for stabilization and open cementation of the lesion
Referral to medical oncology for chemo-radiotherapy
Lesion biopsy with further treatment based on the results of the biopsy
New lesions which are not diagnosed by imaging and require surgical intervention need to have an appropriate biopsy with treatment dictated by the results of the biopsy. While this patient has a significant tobacco history, incorrect treatment of this lytic bone lesion could affect both her overall morbidity and mortality. As an example, a lytic high-grade chondrosarcoma may look exactly like a metastatic lesion but requires wide surgical excision, not just stabilization of an impending pathological fracture. Intramedullary nailing of a chondrosarcoma would spread the tumor the entire length of the bone and likely require a major amputation, not a limb salvage operation.
A 14-year-old child is referred to your office for evaluation of a tibia lesion found incidentally after a minor ankle injury. A radiograph of the child's ankle is shown in Figure A. What treatment do you suggest?

Endocrine consultation secondary to associated endocrine abnormalities
Surgical consultation secondary to associated gastrointestional cancers
Short leg cast and non-weight bearing for a minimum of 6 weeks
Open biopsy and tumor staging
Routine followup of tibial lesion
The radiograph is classic for a non-ossifying fibroma given the classic eccentric position, sclerotic margin, and benign appearance. Other than routine followup for the tibial lesion, this child requires no subsequent treatment. Marks and Bauer review the diagnosis, imaging, and treatment of many different fibrous tumors of bone and review the diagnostic imaging criteria specific to each subclass of bony fibrous tumors.
The chromosomal translocation t(X;18)is found in which of the following conditions?
Myxoid liposarcoma
Synovial Sarcoma
Osteosarcoma
Ewing's Sarcoma
Clear cell sarcoma
Synovial sarcoma is a rare soft tissue sarcoma with biphasic features of both spindle cell and epithelial differentiation. Synovial sarcoma is a rare high-grade tumor that spreads along fascial planes and, thus, can be much more widespread than apparent on initial evaluation. Males are more commonly affected than females with a ratio of 1.1:1. Synovial sarcoma is characterized by a specific chromosomal translocation t(X;18)(p11;q11) that is observed in more than 90% of cases. The t(X;18)(p11;q11) translocation fuses the SYT gene from chromosome 18 to either of 2 homologous genes at Xp11, either SSX1 or SSX2. The fusion proteins SYT-SSX1 and SYT-SSX2 function as aberrant transcriptional regulators, resulting in either activation of protooncogenes or inhibition of tumor suppressor genes.
Kawai et al found that SYT-SSX fusion transcripts are a defining diagnostic marker of synovial sarcomas. These fusion transcripts may yield important independent prognostic information and provide important information for different types of treatment.
Incorrect Answers
Question 10
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
REFERENCES: Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A
double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood.
J Bone Joint Surg Br 1984;66:770-771.
Question 11
Which of the following is considered the most common long-term effect on the spine of a professional race horse jockey?
Explanation
REFERENCES: Tsirikos A, Papagelopoulos PJ, Giannakopoulos PN, et al: Degenerative spondyloarthropathy of the cervical and lumbar spine in jockeys. Orthop 2001;24:561-564.
Hordegen KM: The spine and horseback riding. Schweiz Med Wochenschr 1975;105:668-675.
Question 12
What is the best way to determine whether a radial head implant is too thick intraoperatively?
Explanation
Question 13
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 14
A patient with rheumatoid arthritis has an unstable pseudarthrosis after undergoing C1-2 posterior fusion. No neurologic deficits are noted, and repair with posterior transarticular fixation screws and a posterior wiring technique at C1-2 is planned. Which of the following preoperative studies offers the best visualization?
Explanation
REFERENCES: Paramore CG, Dickman CA, Sonntag VK: The anatomic suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg 1996;85:221-224.
Dickman CA, Sonntag VK: Posterior C1-C2 transarticular screw fixation for atlantoaxial arthrodesis. Neurosurgery 1998;43:275-280.
Song GS, Theodore N, Dickman CA, Sonntag VK: Unilateral posterior atlantoaxial transarticular Screw fixation. J Neurosurg 1997;87:851-855.
Question 15
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
REFERENCES: Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38. 500.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 16
Which of the following is true regarding intimate partner violence (IPV)?

Explanation
Interdisciplinary collaboration among healthcare workers was a predictor of positive treatment outcomes. Included were more accurate assessments of past history, more descriptive emotional symptoms as displayed by victims and written documentation of recommendations concerning intervention and linkage to community resources.
Bhandari et al performed a cross-sectional study of 282 women who presented to fracture clinic at two Level-I trauma centers in Canada. The prevalence of abuse was found to be 32% while 8.5% were found to have a history of previous abuse in the past 12 months. Ethnicity, socioeconomic status, and injury patterns were not associated with abuse.
Shields et al reviewed 153 cases of domestic violence victims who presented to two Emergency departments. They determined that positive treatment outcomes were correlated to the degree of interdisciplinary collaboration among treating health care providers.
Question 17
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
as indicated by the arrow. This technique suppresses the signal of the surrounding fat
and causes the stationary surrounding tissues to become intermediate in signal intensity.
The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient’s symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue.
REFERENCES: Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Holder LE, Merine DS, Yang A: Nuclear medicine, contrast angiography, and magnetic resonance imaging for evaluating vascular problems in the Hand: Vasospastic disorders. Hand Clin 1993;9:95-113.
Question 18
When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure? Review Topic
Explanation
Question 19
Figures 51a and 51b show the radiographs of a 12-year-old boy obtained after an attempted closed reduction of an elbow injury in the emergency department. His motor examination is intact but he reports decreased sensation along the palmar aspect of his ring and little finger. What is the best treatment plan? Review Topic

Explanation
(SBQ13PE.97) A 3-year-old boy presents to your office for evaluation. On physical examination, the patient has large calves and uses his hands to assist in rising from the floor. Laboratory results from the pediatrician reports notably high creatinine kinase of 43000 IU/L. What is the most likely inheritance pattern? Review Topic
Autosomal recessive
Autosomal dominant
X-linked recessive
X-linked dominant
Mitochondrial inheritance
Duchenne's muscular dystrophy (DMD) has an X-linked recessive inheritance pattern.
Duchenne's muscular dystrophy is characterized by a lack of dystrophin on muscle biopsy. Gower's sign is a typical physical exam finding (child uses hands to assist in rising from sitting), along with pseudohypertrophy of the calves. Notable laboratory values include elevated creatinine kinase (CK), typically above 25,000 IU/L.
Sussman et al. provide a comprehensive review of DMD, highlighting characteristic findings, including pseudohypertrophy of the calves (due to replacement of skeletal muscle with adipose tissue), Gower's sign, as well as CK levels typically above 25,000 IU/L. CK levels can aid in distinguishing between Becker's dystrophy which has levels less than 25,000 IU/L.
Figure A exhibits a muscle biopsy (calf) at low power of DMD; note the replacement of muscle with adipose tissue.
Incorrect answers:
(SBQ13PE.47) Figure A shows an ultrasound of a 2 week old infant being evaluated for developmental dysplasia of the hip. Which of the labels depict the alpha angle, and what anatomic landmarks define this angle? Review Topic
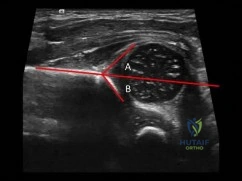
Angle A, ilium and cartilaginous acetabulum
Angle A, ilium and bony acetabulum
Angle B, ilium and cartilaginous acetabulum
Angle B, ilium and bony acetabulum
Angle B, bony acetabulum and acetabular labrum
The alpha angle is subtended by (1) a line drawn down the ilium to a point where it intersects with the bony and cartilaginous confluence of the acetabulum and (2) a line drawn along the roof of the bony acetabulum.
The coronal flexion view (as depicted in figure A) of the infant hip is perhaps more familiar if rotated 90 degrees to view as one would view an anterior posterior radiograph of the pelvis. Acetabular development is evaluated primarily by the alpha angle, indicating the morphology of the developing acetabulum, and the percentage of the femoral head that is covered by the bony acetabulum. These are each readily apparent on ultrasound. Normal hips should have an alpha angle of at least 60 degrees by 6-8 weeks of age.
Harcke et al. provide a current concepts review on the state of ultrasound in the diagnosis and management of developmental dysplasia of the hip (as of 1991). They report, since that time, ultrasound has become the mainstay for diagnostic confirmation and management of DDH.
LeBa et al. performed a study to look at whether ultrasound screening would increase in effectiveness if targeted toward infants with established risk factors for developmental dysplasia of the hip and normal findings on physical examination. They found dynamic ultrasound evaluation showed developmental dysplasia in 7.8% of patients who had normal physical exams and led to a change in treatment in 8%. They conclude selective ultrasound screening in infants with risk factors and normal
findings on physical examination is effective and leads to more effective treatment.
Figure A shows an ultrasound exam of a 2 week old infant. The alpha angle is labeled 'B'. The beta angle is lableled 'A'. Illustration A is a diagram from Tachdjian's illustrating diagrammatically the elements of these angles.
Incorrect answers.
Question 20
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
REFERENCES: Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Raaymakers EL: Complications of talar fractures, in Tscherne H, Schatzker J (eds): Major Fractures of the Pilon, the Talus, and Calcaneus: Current Concepts of Treatment. Berlin, Springer-Verlag, 1993, pp 137-142.
Question 21
A funnel plot is used in meta-analyses to perform which of the following functions:
Explanation
Publication bias occurs because studies with a non-significant result, so-called
negative studies, have a higher likelihood of being rejected than positive studies, and are oftentimes not even submitted for publication. Funnel plots, which plot the effect size of a study against a measure of the study’s size are used to detect this bias. This method is based on the fact that larger studies have smaller variability, whereas small studies, which are more numerous, have larger variability. Thus the plot of a sample of studies without publication bias will produce a symmetrical, inverted-funnel shaped scatter, whereas a biased sample will result in a skewed plot.
Vavken et al. reviewed orthopaedic meta-analyses in order to determine whether publication bias was assessed and to evaluate its effect on the outcomes of these meta-analyses. They found that only 35% of all orthopaedic meta-analyses published between 1992 and 2008 in English and German assessed publication bias. Adjustment for publication bias did not produce significantly different results, but the magnitude of the pooled estimates in the affected meta-analyses changed by 29% on average.
Illustration A depicts a symmetrical funnel plot with no evidence for publication bias. Illustration B shows a skewed funnel plot suggesting publication bias, as it is missing studies in the lower left corner, i.e. ‘‘negative studies’’. Illustration C depicts a forest plot comparing the incidence of squeaking between ceramic-on-ceramic (COC) and ceramic-on-polyethylene (COP). Illustration D is an example of a ROC curve examining the probability of DVT.
Incorrect Answers:
Question 22
Which of the following cohorts of patients is at highest risk of a future anterior cruciate ligament (ACL) tear? Review Topic
Explanation
Question 23
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?
Explanation
REFERENCE: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997.
Question 24
A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Question 25
-
What is the primary mechanism of wear of polyethylene acetabular components?
Explanation
Question 26
A 17-year-old girl develops chronic posterolateral rotatory instability (PLRI) of the elbow following closed treatment of an elbow dislocation. Advanced imaging reveals incompetence of the lateral collateral ligament complex, and ligament reconstruction is planned. Examination under anesthesia is performed with the forearm in maximal supination and valgus force applied to the elbow, demonstrated in Video 1. As the elbow is brought through a range of motion assessment, the radial head is
Explanation
Question 27
74 A
B
year-old with the injury seen in Figures 74a and 74b

Explanation
Figures 71a through 71d reveal a severe intra-articular distal femur fracture that is best treated with ORIF with a locking condylar plate. A retrograde IM nail is not an ideal option for this application. Lateral and medial nonlocking plates have gone by the wayside in favor of locked plating and fixed-angle devices. External fixation will not allow for articular reconstruction and is best reserved for temporary stabilization of these fractures. Screws alone will not address this injury
Figures 72a and 72b reveal an extra-articular distal femur fracture that is best treated with an IM nail, which would also allow for earlier weight bearing. Screw fixation alone is inappropriate, and this does not necessitate medial and lateral plate fixation. Although a locking condylar plate could be used, blood loss in a polytrauma patient may be problematic. ?
Figures 73a and 73b show a comminuted supracondylar femur fracture with complex intra-articular involvement. This would be treated using the same application as seen in Figures 71a through 71d.
Figures 74a and 74b reveal a coronal plane fracture of the medial femoral condyle, which can be treated with screws alone.
RECOMMENDED READINGS
Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. J Am Acad Orthop Surg. 2010 Oct;18(10):597-607. Review. PubMed PMID: 20889949.View Abstract at PubMed
Markmiller M, Konrad G, Südkamp N. Femur-LISS and distal femoral nail for fixation of distal femoral fractures: are there differences in outcome and complications? Clin Orthop Relat Res. 2004 Sep;(426):252-7. PubMed PMID: 15346082. View Abstract at PubMed
Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S, Benirschke SK. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005 Mar;87(3):564-9. PubMed PMID: 15741623. View Abstract at PubMed
Question 28
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 29
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic

Explanation
Question 30
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement? Review Topic

Explanation
Question 31
Following insertion of a cementless femoral component into the total hip arthroplasty construct, the amount of femoral stress shielding is most associated with
Explanation
Although material modulus, characteristics of surface, and extent of coating all contribute to stress shielding, poor bone quality is the most important factor associated with stress shielding.
Question 32
Figures below show the radiograph and the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
Question 33
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic
Explanation
Question 34
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?
Explanation
REFERENCES: Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 35
All of the following indicators of resuscitation may be within normal limits for a trauma patient that is in "compensated" shock EXCEPT:

Explanation
Question 36
-Where is the physis with the highest growth rate (in mm per year) located?
|
| Location | Growth Rate (mm/year) |
|---|---|
| Distal femur | 9 to 11 |
| Proximal humerus | 7 |
| Distal tibia | 4 to 5 |
| Distal radius | 5 to 6 |
Explanation

Question 37
A 29-year-old man sustained an injury when he was playing basketball, landing on his left knee while jumping for a rebound. He had vague pain in the anterior aspect of the knee for several weeks. The initial radiographs were negative with the exception of a large traumatic effusion. Examination reveals no apparent ligament instability but a significant extension lag of 30 degrees. There was a palpable defect above the superior pole of the patella. What is the most appropriate management? Review Topic
Explanation
Question 38
A 60-year-old man reports increasing pain in his right foot with limited ankle dorsiflexion and anterior ankle pain after sustaining a fracture of the calcaneus in a fall several years ago. Bracing, nonsteroidal anti-inflammatory drugs, and cortisone injections have failed to provide significant relief. Radiographs are shown in Figures 19a and 19b. What is the next most appropriate step in management?
Explanation
REFERENCE: Robinson TF, Murphy GA: Arthrodesis as salvage for calcaneal avulsions. Foot Ankle Clin 2002;7:107-120.
Question 39
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Explanation
REFERENCES: Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Lee D, Ferlic R, Neviaser R: Hand infections, in Berger R, Weiss AP (eds): Hand Surgery. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 1784-1785.
Question 40
Which of the following medications inhibits release of neurotransmitters by binding to presynaptic calcium channels?
Explanation
Gabapentin (also known as Neurontin) is a medication that is commonly used to treat neuropathic pain. It acts by binding the alpha2delta subunit of voltage-dependent calcium channels on the presynaptic membrane. This serves to increase GABA synthesis, as well as inhibit the release of excitatory neurotransmitters. These neurotransmitters are believed to be part of the pathway leading to neuropathic pain.
Bennett et al. provide a review of the pharmacology of gabapentin for the use of neuropathic pain. They note effective antihyperalgesic and antiallodynic properties of gabapentin but not significant anti-nociceptive action. Among patients with neuropathic pain they found an average pain score reduction of 2.05 points on an 11 point Likert scale, which compared favorably to placebo.
Mehta et al. explored outcomes of gabapentin and pregabalin (Lyrica) for use in patients with spinal cord injury. Both agents were found to decrease pain and secondary conditions such as sleep disturbance. They did not directly compare these agents to other analgesic medications.
Guy et al. present a meta-analysis of the use of anticonvulsants (such as gabapentin) to treat pain in patients with spinal cord injury. Large effect size was seen in 4 of 6 studies looking at the effectiveness of gabapentin.
Illustration A show the mechanism of currently available antiepileptic drugs (AEDs) that target several molecules at the excitatory synapse. Gabapentin and pregabalin bind to the a2d subunit of voltage-gated Ca2+ channels, which is thought to be associated with a decrease in neurotransmitter release.
Incorrect Answers
Question 41
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 42
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm 3 . Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of
Explanation
REFERENCES: Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Marmor L: Stress fracture of the pubic ramus simulating a loose total hip replacement. Clin Orthop 1976;121:103-104.
Question 43
Following operative repair of lower extremity long bone and periarticular fractures, what is the time frame for patients to return to normal automobile braking time?

Explanation
The second reference by Egol studied only operatively treated ankle fractures and found that time to appropriate braking returns at 9 weeks postoperatively. Interestingly, no significant association was found between the functional scores and normalization of total braking time.
Question 44
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
REFERENCES: Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Weber TG, Manoli A II: Compartment syndromes of the foot. Foot Ankle Clin 1999;4:473-486.
Question 45
Which lower extremity muscle is first weakened in Charcot-Marie-Tooth (CMT) disease?
Explanation
Although many of the lower extremity muscles may be affected in CMT, those innervated by the longest axons have been shown to be affected first. In the lower extremity the muscles innervated by the longest axons are the intrinsic foot muscles. The tibialis anterior and the peroneus brevis may be severely affected but not before the foot intrinsics. The peroneus longus typically is spared, resulting in the cavus.
RECOMMENDED READINGS
Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009 Jul;8(7):654-67. Review. PubMed PMID: 19539237. View Abstract at PubMed
Wenz W, Dreher T. Charcot-Marie-Tooth disease and the cavovarus foot. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:291-306.
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
Figure 60 is the standing radiograph of a 27-year-old man who played football throughout his teen years. During those years, he noted that he had less mobility of his left foot and ankle. He twisted his left foot and ankle 8 months ago and has tried over-the-counter nonsteroidal anti-inflammatory drugs and a brace. He now has pain and edema in the left sinus tarsi area.
|
| Motion | Right (degrees) | Left (degrees) |
|---|---|---|
| Ankle dorsiflexion | 5 | 5 |
| Ankle plantar flexion | 30 | 30 |
| Foot inversion | 10 | 5 |
| Foot eversion | 10 | 5 |

Question 46
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
REFERENCES: AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. http://www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf
The Orthopaedic Surgeon’s Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. http://www.aaos.org/about/papers/ethics/1204eth.asp
AdvaMed Code of Ethics on Interactions with Health Care Professionals 2005. http://www.advamed.org/MemberPortal/searchresults.htm?query=Advamed%20Code%20of%20Ethics%20on%20Interactions%20with%20Health%20Care%20Professionals%202005
Question 47
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of
Explanation
REFERENCES: Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
Lotke PA, Abend JA, Ecker ML: The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop 1982;171:109-116.
Question 48
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?

Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of childbearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 49
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes? Review Topic
Explanation
Question 50
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness. Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities. Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following? Review Topic

Explanation
Question 51
Figure A shows immediate post-operative radiographs of a 75-year-old patient with primary osteoarthritis. She presents 3 years later with increasing pain and weakness in the shoulder despite home physical therapy. Examination reveals limited active range of motion, with forward elevation of 80 degrees and external rotation of 50 degrees. Her deltoid function is intact. Repeat radiographs are seen in Figure B.

Explanation
RTSA is considered a viable treatment option for patients with failed shoulder arthroplasty. It allows for improved arm elevation and abduction in the setting of nonfunctional rotator cuff muscles, as seen in this example. Despite the expanding indications for rTSA, there are high complication rates in the revision setting. Complication rates for rTSA after failed shoulder arthroplasty have been reported to be between 11-36%. This procedure should, therefore, be performed by surgeons with extensive training in reconstructive shoulder arthroplasty.
Patel et al. retrospectively reviewed 31 patients (mean age, 68.7 years) who underwent rTSA for treatment of a failed shoulder arthroplasty. They found the greatest improvement with active forward elevation from 44° preoperatively to 108° postoperatively (P < .001). Complications occurred in 3 patients with periprosthetic fracture.
Hattrup et al. reviewed a series of 19 patients that underwent open rotator cuff repair after shoulder arthroplasty. Out of the 19 patients only 4 shoulders were successfully repaired. They concluded that successful rotator cuff repair after shoulder arthroplasty is possible but failure is more common.
Figure A shows a left total shoulder arthroplasty that is well reduced in the glenoid. Figure B shows antero-superior escape of the prosthesis, indicative of a massive rotator cuff tear.
Incorrect Answers:
Question 52
Figure 1 is the clinical photograph of a 22-year-old college pitcher who complains of posterior shoulder pain and feelings of shoulder weakness. He denies shoulder trauma. Evaluation should include
Explanation
Question 53
A 56-year-old man has upper thoracic pain after undergoing stereotactic radiosurgery for a blastic metastatic lesion in the vertebral body of T5. He has normal alignment without collapse, but the tumor involves the entire vertebral body. Which factor increases this patient's risk for a pathologic fracture?
Explanation
Criteria for spinal instability have been outlined by the Spine Oncology Study Group, which developed the Spinal Instability Neoplastic Score (SINS) criteria. Factors associated with lower risk for instability/fracture are location outside of a junctional level (the SINS criteria use C7-T2 as the junctional level),
blastic metastases, and no evidence of vertebral collapse (even with more than 50% involvement). Radiation has been associated with risk for pathologic fracture, and stereotactic radiation has been associated with risk for a spinal fracture.
RECOMMENDED READINGS
Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fourney DR. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010 Oct 15;35(22):E1221-9. doi: 10.1097/BRS.0b013e3181e16ae2. Review. PubMed
PMID:20562730. View Abstract at PubMed
Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH, Bilsky MH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fisher CG. Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol. 2011 Aug 1;29(22):3072-7. doi:10.1200/JCO.2010.34.3897. Epub 2011 Jun 27. PubMed PMID: 21709187. View Abstract at PubMed
Rose PS, Laufer I, Boland PJ, Hanover A, Bilsky MH, Yamada J, Lis E. Risk of fracture after single fraction image-guided intensity-modulated radiation therapy to spinal metastases. J Clin Oncol. 2009 Oct 20;27(30):5075-9. doi: 10.1200/JCO.2008.19.3508. Epub 2009 Sep 8.
PubMed PMID: 19738130 View Abstract at PubMed
Question 54
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?
Explanation
kyphosis and stenosis. Because he is healthy, has responded well to previous surgery,
|and has a potentially correctable lesion, he is not a good candidate for an end-stage failed
back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient’s relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
REFERENCE: Eck JC, Humphreys SC, Hodges SD: Adjacent-segment degeneration after lumbar fusion: A review of clinical, biomechanical, and radiographic studies. Am J Orthop 1999;28:336-340.
Question 55
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of
Explanation
REFERENCE: Sunderland SS: Nerves and Nerve Injuries, ed 2. New York, NY, Churchill Livingstone, 1978, pp 343-347.
Question 56
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
REFERENCES: Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am 1999;81:649-659.
Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report on the incidence and prognosis. J Pediatr Orthop 1984;4:689-692.
Question 57
The attachments of the transverse carpal ligament include which of the following structures?
Explanation
REFERENCES: Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 471-472.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 168-170.
Question 58
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
Question 59
A healthy, active collegiate soccer player returns to your office approximately 10 months after returning to full play and 18 months after undergoing ACL reconstruction with bone-patellar tendon-bone (BTB) autograft. The patient reports landing awkwardly after a jumping for a ball and felt his knee give way. He presents with pain, worse with weight bearing. On physical exam, there is a mild effusion and a grade 2B Lachman. Radiographs are shown in Figure A. What is the likely underlying cause of his current diagnosis? Review Topic

Explanation
Ideal tunnel placement on the femoral side should be at the approximately 2 o'clock (for a left knee) or 10 o'clock (for a right knee) position on the lateral wall, which facilitates a more horizontal, anatomic graft. On the tibial side, the tunnel trajectory in the coronal plane should be about 60-75 degrees from the horizontal and the tunnel entrance should be approximately 10-11mm from the anterior border of the PCL.
Noyes et al. emphasize the importance of anatomic reconstruction. They recommended against using a transtibial tunnel to make the femoral tunnel because it will result in a vertical orientation. The authors summarized and recommended the use of individual drilling of each tunnel, and using a anteromedial portal to obtain the ideal femoral tunnel.
Driscoll et al. compared the rotational properties of a BTB graft placed centrally in the tibial footprint in both groups, but on the femoral side, placed in the anteromedial aspect versus central portion of the ACL femoral origin. They noted a significantly stronger resistance to rotational failure when placed centrally. Thus, noting the importance of placing the graft anatomically, within the central areas of both the tibial footprint and femoral origin.
Figure A exhibits malpositioned tunnels, both of which are too vertical. Illustration A exhibits well-placed tunnels, with the horizontality exhibited on the femoral side and approximately 75 degrees from the horizontal on the tibial side.
Incorrect answers:
Question 60
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?
Explanation
REFERENCES: Hsu LC, Leong JC: Tuberculosis of the lower cervical spine (C2 to C7): A report on 40 cases. J Bone Joint Surg Br 1984;66:1-5.
Loder RT: The cervical spine, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 739-789.
Question 61
A 16-year-old boy has had left knee pain and swelling after sustaining a minor twisting injury while playing basketball 2 weeks ago. Figures 5a through 5e show the radiograph, MRI scans, and biopsy specimens. What is the most likely diagnosis?
Explanation
REFERENCES: Sissons HA, Murray RO, Kemp HBS: Orthopaedic Diagnosis. Berlin, Springer-Verlag, 1984, pp 254-256.
Wafa H, Grimer RJ: Surgical options and outcomes in bone sarcoma. Expert Rev Anticancer Ther 2006;6:239-248.
Question 62
Figure 1 is the T2 coronal MRI scan of a 52-year-old woman with a 6- month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
Question 63
Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?
Explanation
REFERENCES: Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.
Myerson MS, Schon LC, McGuigan FX, et al: Results of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int
2000;21:297-306.
Question 64
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 65
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of
Explanation
REFERENCES: Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
Hyman J, Breazeale NM, Altchek DW: Valgus instability of the elbow in athletes. Clin Sports Med 2001;20:11-24.
Question 66
A 45-year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has
had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to
85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well- fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
Question 67
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
Explanation
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.

Question 68
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
REFERENCES: Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 961-990.
Question 69
What portion of the pitching phase creates forces approaching the tensile limit of the medial ulnar collateral ligament of the elbow? Review Topic
Explanation
Fleisig et al. were among the first to elucidate the elbow and shoulder kinetics in healthy adult pitchers using high-speed motion capture analysis. Inability to generate sufficient elbow varus torque may result in medial tension, lateral compression, or posteromedial impingement injury.
According to Lynch et al. the late cocking phase of the overhand throw places a marked valgus moment across the medial elbow. This repetitive force reaches the tensile limits of the medial collateral ligament, subjecting it to microtraumatic injury and attenuation. The anterior bundle of the medial collateral ligament has been identified as the primary restraint to valgus load and is the focus of reconstruction.
Incorrect Responses:
1,4,5: The medial elbow forces are less during these phases. 4: Ball release is not one of the 5 phases of throwing and marks the end of the acceleration and beginning of deceleration phase.
Question 70
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
|
| Muscle Recovery Order |
|---|
| Brachioradialis |
| Extensor carpi radialis longus |
| Supinator |
| Extensor carpi radialis brevis |
| Extensor carpi ulnaris |
| Extensor digitorum comminus |
| Extensor digiti minimi |
| Extensor indicis proprious |
| Extensor pollicis longus |
| Abductor pollicis longus |
| Extensor pollicis brevis |
| Extensor pollicis brevis |
|
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ,
Ciba-Geigy, 1991, vol 8, p 53.
Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA,
Harper and Row, 1982, vol 3, pp 428-429.
Question 71
What is the most common malignant tumor of the foot?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 11-26.
Bos GD, Ester RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 72
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Kitaoka HB, Wikenheiser MA, Schaughnessy WJ, et al: Gait abnormalities following resection of talocalcaneal coalition. J Bone Joint Surg Am 1997;79:369-374.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 73
An osteoconductive bone graft material has which of the following properties?
Explanation
substitution, which allows for graft incorporation. An osteoinductive graft will stimulate the recruitment of progenitor cells that can differentiate into osteoblastic cells. Specific BMPs are osteoinductive. Osteogenic material contains viable cells with the ability to form bone. The ability to provide osteoprogenitor cells is only seen in fresh autograft. Other grafts rely on the recruitment of host progenitor cells to differentiate.
Question 74
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
REFERENCES: Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
Kibler WB (ed): ACSM’s Handbook for Team Physician. Philadelphia, PA,
Williams & Wilkins, 1996, p 151.
Question 75
Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
Explanation
Question 76
A patient has a painful metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis if this patient is having a reaction to metal debris?
Explanation
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Question 77
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 78
A coach of three football teams—the B team, junior varsity team, and varsity team—wants to study the
average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on one team are different from those on the other teams?
Explanation
Question 79
Which of the following radiographic parameters is most predictive of a poor result following multilevel fusion surgery for adult degenerative scoliosis? Review Topic
Explanation
Question 80
A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
Explanation
used for elbow arthroplasty.
Question 81
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include
Explanation
REFERENCES: Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Velmahoos GC, Demetriades D: Gunshot wounds of the spine: Should retained bullets be removed to prevent infection? Ann R Coll Surg Engl 1976;94:85-87.
Question 82
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
REFERENCES: Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Arnoczky SP, Rubin RM, Marshall JL: Microvasculature of the cruciate ligaments and its response to injury. J Bone Joint Surg Am 1979;61:1221-1229.
Question 83
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
REFERENCES: Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Pemberton PA: Pericapsular osteotomy of the ilium for the treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am 1965;47:65-86.
Question 84
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, chapter 2.
Flynn TB: Neurologic complication of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 85
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of
Explanation
REFERENCES: Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Muller EB, Nordwall A: Brace treatment of scoliosis in children with myelomeningocele. Spine 1994;19:151-155.
Question 86
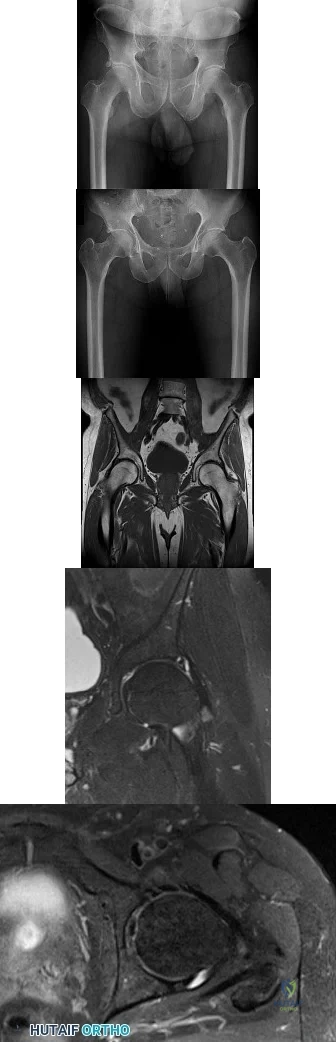
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. Images from an MRI scan of this patient's left hip are shown in Figures 3 through 5. What is the most likely cause of his acute pain?
Explanation
standing groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a
periacetabular osteotomy can develop a more retroverted acetabulum as well.
Question 87
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?
Explanation
REFERENCE: Anglen JO: Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds: A prospective, randomized study. J Bone Joint Surg Am 2005;87:1415-1422.
Question 88
What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o’clock position? Review Topic
Explanation
Question 89
Which of the following benign bone lesions can develop lung metastases?
Explanation
REFERENCES: Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Bloem JL, Mulder JD: Chondroblastoma: A clinical and radiological study of 104 cases. Skeletal Radiol 1985;14:1-9.
Question 90
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings.Figures 3 and 4 are this patient's proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include

Explanation
Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence and the need for reconstruction.
Question 91
Figures 1a through 1c are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury, she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?

Explanation
This patient has a fracture of the middle phalanx attributable to the presence of an enchondroma. Enchondromas are the most common benign bone tumor affecting the hand. This particular enchondroma has thinned the cortices extensively so that even minor trauma can cause a pathologic fracture. Observation is not the best treatment because a fracture is present, and, at a minimum, the digit should be immobilized. Intralesional steroid injections have a role in the treatment of simple bone cysts; however, this treatment is not recommended for enchondromas. Immediate curettage alone is not the best treatment because it does not include bone graft (either autograft or allograft) or bone graft substitute. Also, it would be best to allow the fracture to heal prior to curettage to prevent fracture displacement. An enchondroma this size necessitates a graft because of high risk for refracture if curettage alone is performed. Many surgeons believe it is best if a fracture heals prior to curettage and grafting because this allows better graft containment and eliminates concern about fracture displacement. Recent data suggest early surgery using injectable calcium sulfate cement in the fracture setting can achieve satisfactory results. Splint
immobilization would allow fracture healing, and then curettage with bone graft can be performed after healing occurs.
RECOMMENDED READINGS
Jacobson ME, Ruff ME. Solitary enchondroma of the phalanx. J Hand Surg Am. 2011 Nov;36(11):1845-7. doi: 10.1016/j.jhsa.2011.05.002. Epub 2011 Jun 11. Review. PubMed PMID: 21658859.
Sassoon AA, Fitz-Gibbon PD, Harmsen WS, Moran SL. Enchondromas of the hand: factors affecting recurrence, healing, motion, and malignant transformation. J Hand Surg Am. 2012 Jun;37(6):1229-34. doi: 10.1016/j.jhsa.2012.03.019. Epub 2012 Apr 27. PubMed PMID: 22542061.
CLINICAL SITUATION FOR QUESTIONS 2 THROUGH 5
A 45-year-old man injured his arm when it was forcibly extended while he was flexing his elbow. He notes swelling in the antecubital fossa and arm weakness. The physician suspects a distal biceps rupture.
Question 92
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
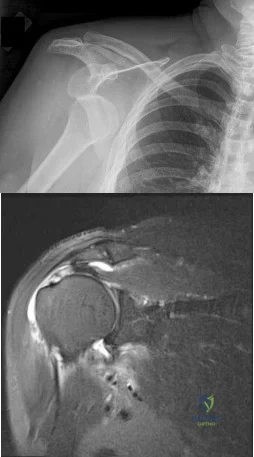
Explanation
Question 93
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intraoperatively, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation
Question 94
The newborn foot deformity seen in Figures 64a and 64b should initially treated with
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American AcademAyL-oMfadOenrathCooppayedic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
Arthroscopy
Antinuclear antibody
MRI
Bone scan
HLA-B27
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love l and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa ling. Prenatal and birth history are otherwise unremarkable. The child’s growth and
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
No treatment because internal tibial torsion slowly resolves on its own
Immediate treatment with a Denis-Browne bar
Distal tibial osteotomies
Proximal femoral derotational osteotomies
Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.

Question 95
Which of the following patients is considered the most appropriate candidate for an isolated split posterior tendon transfer?
Explanation
REFERENCES: Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 291-294.
Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Kling TF Jr, Kaufer H, Hensinger RN: Split posterior tibial-tendon transfers in children with cerebral spastic paralysis and equinovarus deformity. J Bone Joint Surg Am 1985;67:186-194.
Question 96
-
Gamma ray irradiation for sterilization of ultra-high molecular weight polyethylene in an oxygen environment can have what effect on the material?
Explanation
Question 97
Serum parathyroid hormone level
The plain radiograph of the shoulder shows lytic lesions in the scapular spine, distal clavicle, and the proximal third of the clavicle. There is an elliptical erosion in the proximal clavicle. These three lesions suggest a diagnosis of metastatic bone disease or multiple myeloma. The biopsy specimen shows plasma cells. The plasma cells have these characteristic features:
Eccentrically placed nucleus
Peripheral clumping of the nuclear chromatin A perinuclear halo
The diagnosis is multiple myeloma. Staging is important and is performed with a skeletal survey, bone marrow biopsy, hemoglobin level, and chemistry studies including kidney function and serum calcium determination.
Serum protein electrophoresis is performed to assess the amount of abnormal gammaglobulin in the serum. There are three major criteria in the diagnosis of multiple myeloma:
Explanation
A 55-year old man presents with a 4-month history of shoulder discomfort. The plain radiographs are shown in Slide 1 and a biopsy in Slide 2. Which of the following tests will probably be abnormal:
Question 98
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 379-426.
Gilbert MS, Radomisli TE: Therapeutic options in the management of hemophilic synovitis. Clin Orthop 1997;343:88-92.
Question 99
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Explanation
REFERENCES: Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
Mann RA: Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 167-296.
Question 100
The patient is given a blood transfusion. After starting the transfusion, nurses note that her temperature is 38.8°C and she has shaking and chills. What is the most likely cause of this problem?
Explanation
Blood management and venous thromboembolism prevention are important considerations in the perioperative management of THA. Recommendations now focus on presurgical optimization of hemoglobin, use of antifibrinolytics intrasurgically, and minimized use of transfusions. Current recommendations do not favor autologous blood donation for patients with hemoglobin levels higher than 13 g/dL. There is a move toward increased use of aspirin for venous thromboembolism prophylaxis, but this modality can cause GI bleeding that may necessitate blood transfusion. Transfusion reactions are rare, and the most common cause is administration of an incompatible unit because of clerical error.
