Orthopedic Board Review MCQs: Arthroplasty, Fracture & Knee | Part 91

Key Takeaway
This page offers Part 91 of a professional orthopedic surgery board review quiz. It provides 100 high-yield MCQs for orthopedic residents and surgeons preparing for their OITE, AAOS, and ABOS board certification exams. Questions are verified and formatted like the actual tests, covering topics like arthroplasty, fracture, and knee.
About This Board Review Set
This is Part 91 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 91
This module focuses heavily on: Arthroplasty, Fracture, Knee.
Sample Questions from This Set
Sample Question 1: A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharpanterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals ...
Sample Question 2: Which treatment of the current fracture will provide the best long-term outcome?...
Sample Question 3: During a posterior approach to the glenoid with retraction as shown in Figure 33, care should be taken during superior retraction to avoid injury to which of the following structures?...
Sample Question 4: -Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and curr...
Sample Question 5: A unilateral "piano key" sign, indicates...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 2
Which treatment of the current fracture will provide the best long-term outcome?
Explanation
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
Question 3
During a posterior approach to the glenoid with retraction as shown in Figure 33, care should be taken during superior retraction to avoid injury to which of the following structures?
Explanation
glenoid fracture, or posterior shoulder pathology, the interval between the teres minor and infraspinatus is split. Excessive superior retraction on the infraspinatus, or excessive dissection superomedially under the infraspinatus muscle and tendon can cause injury to the suprascapular nerve and/or artery. During dissection in this interval, the axillary artery and axillary nerve are well protected. A branch of the circumflex scapular artery ascends between the teres minor
and infraspinatus muscle, but it is at risk during dissection on the scapula in the mid portion of the interval and not during superior retraction. The profunda brachii artery is not present in
this interval.
REFERENCES: Jerosch JJ, Greig M, Peuker ET, et al: The posterior subdeltoid approach: A modified access to the posterior glenohumeral joint. J Shoulder Elbow Surg 2001;10:265-268.
Judet R: Surgical treatment of scapular fractures. Acta Orthop Belg 1964;30:673-678.
Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Question 4
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
Explanation
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
Question 5
A unilateral "piano key" sign, indicates
Explanation
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
Question 6
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Warner JP, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Sammarco VJ: Os acromiale: Frequency, anatomy, and clinical implications. J Bone Joint Surg Am 2000;82:394-400.
Question 7
You have been waiting to enroll a patient into your recent institutional review board (IRB)-approved clinical research protocol. A patient is admitted who, upon initial screening, meets all inclusion criteria. However, he has late-stage dementia, and you are told by your research coordinator that this condition is an exclusionary criterion. This scenario demonstrates the need for which aspect of proper informed consent?
Explanation
Question 8
Lipohemarthrosis of the knee is most likely secondary to which of the following?

Explanation
Question 9
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology? Review Topic

Explanation
Question 10
Acetabular reconstruction followed by external beam irradiation The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. The most likely diagnosis based upon the radiographs would be:
Question 11
Which modality has the broadest application for the reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as can TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 12
Figure 18 is the radiograph of a 52-year-old woman who has leg length inequality and chronic activity-related buttock discomfort. This has been a life-long problem, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step vs. oblique cut, or strut grafts.
Question 13
A surgeon performs a minimally invasive total knee arthroplasty through a quadriceps-sparing approach using medial-to-lateral cutting jigs. When beginning therapy that afternoon, the patient can passively but not actively extend her knee, although she has minimal knee pain. All regional blocks have been discontinued. What is the most likely reason for this finding?
Explanation
This patient lacks active knee extension. It is not attributable to the regional block because that block is no longer acting. The most likely cause is laceration of the patella tendon, which has been described during both large-incision surgery and minimally invasive surgery. However, this is reported with increased frequency during minimally invasive surgery. Quadriceps inhibition, avulsion of the quadriceps tendon, and femoral nerve palsy can cause lack of active extension, but these problems are less likely because the patient has minimal pain.
Question 14
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 306-309.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 15
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 16
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
REFERENCES: Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 17
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 18
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
REFERENCES: Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110.
Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571.
Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL: Muscle creatine loading in men. J Appl Physiol 1996;81:232-237.
Question 19
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
Explanation
REFERENCES: Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Azakie A, McElhinney DB, Thompson RW, et al: Surgical management of subclavian-vein effort thrombosis as a result of thoracic outlet compression. J Vasc Surg 1998;28:777-786.
Question 20
An adult patient has had low-grade fevers, malaise, and joint pain for the past several days. Examination reveals an erythematous "bulls eye" rash over the right thigh (erythema migrans). What is the organism associated with this infection? Review Topic
Explanation
Question 21
The posterior circumflex humeral artery and the axillary nerve usually lie in a space bordered superiorly by the
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III: The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, vol 1, pp 70-71.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 401-402, 407.
Question 22
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include
Explanation
REFERENCES: Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
Question 23
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10° of hip abduction on the left and 30° on the right with the hips and knees extended. The Thomas test shows 20° of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0° on the left and -10° on the right. The neck shaft angles are 170° bilaterally. Which of the following procedures would offer the best results?
Explanation
REFERENCES: Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Brunner R, Baumann JU: Long-term effects of intertrochanteric varus-derotation osteotomy on femur and acetabulum in spastic cerebral palsy: An 11- to 18-year follow-up study. J Pediatr Orthop 1997;17:585-591.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 24
A 16-year-old boy has a symptomatic flatfoot deformity that is causing pain, skin breakdown, and shoe wear problems. Shoe modification and an orthosis have failed to provide relief. Examination reveals hindfoot valgus, talonavicular sag, and forefoot abduction that are all passively correctable. Treatment should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Evans D: Calcaneo-valgus deformity. J Bone Joint Surg Br 1975;57:270-278.
Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot: Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995;77:500-512.
Question 25
-What is the most appropriate initial treatment for her condition?
Explanation
This patient has a history most consistent with multidirectional instability. A lax capsule causes subluxation of the shoulder and strain on the rotator cuff and may result in pain and instability. The capsule is most closely associated with the cause of her problem. Initial treatment for multidirectional instability is physical therapy focusing on restoring balance to the shoulder with rotator cuff and scapular stabilization exercises. Nonsurgical therapy should be protracted and is the mainstay of treatment in this scenario. This patient has exhausted all nonsurgical measures and is now a candidate for surgical reconstruction. Capsular plication will best address the lax capsule and provide the best option for reducing her symptoms. The rotator cuff and biceps tendon may be secondarily strained but are not the primary sources of the problem. The brachial plexus does not address the etiology, but rather the symptoms that may occur as a result of instability of the shoulder joint.
Complete rest will not alleviate the patient's underlying condition because the shoulder girdle may still be weak and symptoms likely will return. A corticosteroid injection and arthroscopic surgery are too invasive as initial treatment for this condition. Arthroscopic rotator cuff repair, a biceps tenodesis, and superior labral anterior-posterior repair are unlikely to result in symptomatic improvement for this patient and are not associated with pathologic findings in the setting of multidirectional instability.
Question 26
What process is often found associated with other neoplasms?
Explanation
REFERENCES: Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83.
Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Martinez V, Sissons HA: Aneurysmal bone cyst: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291-2304.
Question 27
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
Explanation
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
Question 28
Integrins function in which of the following ways?
Explanation
Integrins are a large family of heteromeric cell surface receptors composed of non-covalently bound alpha and beta subunits which interact with extracellular matrix molecules, serum constituents and various adhesion molecules. Specifically, aVß3 is a type of integrin found on osteoclasts that attaches to bone by coupling with vitronectin.
Bikle reviews the cause of bone loss during periods of unloading. They state the during periods of rest, integrin expression is decreased, leading to disuse osteoporosis. They argue that drugs that selectively regulate the integrin signaling pathway may
reverse bone loss during periods of disuse.
Illustration A shows an example of an osteoclast attaching to bone via the integrin aVß3.
Incorrect
1:
This
is
the
function
of osteocytes.
2:
This
is
the
function
of osteoblasts.
3:
This
is
the
function
of
osteoprogenitor cells.
Question 29
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a “red bull’s eye” rash. Management should consist of
Explanation
REFERENCES: Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Faller J, Thompson F, Hamilton W: Foot and ankle disorders resulting from Lyme disease. Foot Ankle 1991;11:236-238.
Question 30
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient? Review Topic

Explanation
Question 31
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
REFERENCES: Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Question 32
What is the most common fracture associated with a lateral subtalar dislocation?

Explanation
Post-reduction x-rays need to be scrutinized carefully for fractures of the tarsal bones as this is the most common injury associated with subtalar dislocations. Occult fractures of the lateral process of the talus are also associated with these injuries.
The referenced study by Wagner et al noted radiographic subtalar DJD in 2/3 of their patients, but noted no correlation between radiographic and clinical outcomes. The referenced study by Bibbo et al noted an 88% incidence of other concurrent injuries and an 89% rate of radiographic DJD at 5 year follow-up. The referenced article by Saltzman et al is a review of hindfoot dislocations.
Question 33
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T 1 - and T 2 -weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Kausch T, Rutt J: Subcutaneous rupture of the tibialis anterior tendon: Review of the literature and case report. Arch Orthop Traum Surg 1998;117:290-293.
Question 34
Examination of a hand with compartment syndrome is most likely to reveal which of the following?
Explanation
REFERENCES: Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
Dellaero DT, Levin LS: Compartment syndrome of the hand: Etiology, diagnosis, and treatment. Am J Orthop 1996;25:404-408.
Question 35
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 36
Which of the following rehabilitation methods has proven as effective as surgical treatment for the treatment of patellar tendinopathy (jumper’s knee)?
Explanation
REFERENCES: Bahr R, Fossan B, Loken S, et al: Surgical treatment compared with eccentric training for patellar tendinopathy (Jumper’s Knee): A randomized, controlled trial. J Bone Joint Surg Am 2006;88:1689- 1698.
Coleman BD, Khan KM, Maffulli N, et al: Studies of surgical outcome after patellar tendinopathy: Clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 2000;10:2-11.
Question 37
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Explanation
REFERENCES: Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Hove LM: Delayed rupture of the thumb extensor tendon: A 5-year study of 18 consecutive cases. Acta Orthop Scand 1994;65:199-203.
Question 38
A 19-year-old collegiate baseball player injures the ring finger on his dominant hand while sliding headfirst into second base. He reports that he is unable to actively flex or extend the distal interphalangeal joint of the finger. Radiographs are shown in Figures 19a and 19b. What is the anatomic lesion leading to this injury?
Explanation
REFERENCES: Leddy JP, Packer JW: Avulsion of the insertion of the profundus tendon insertion in athletes. J Hand Surg 1977;2:66-69.
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
Question 39
Figure 194 is the radiograph of a 71-year-old woman who had a right total hip arthroplasty 4 months ago; now she has tripped and fallen. She is unable to continue weight-bearing activity on her right leg, but denies pain or ambulation issues prior to her fall. She is seen in the emergency department. What is best treatment for this patient?
Explanation
This patient has sustained a periprosthetic hip fracture consistent with a Vancouver B2 pattern. The femoral stem must be revised by bypassing the fracture and simultaneously providing stability through fixation. Method of fixation is dependent upon fracture pattern, and, in this case, the medial fracture fragment is better suited for cerclage fixation. Loosening of the stem precludes simply fixing the fracture with cables, plates, or allograft struts, and there is no need to allow the fracture to heal prior to placing a new stem if the fracture is adequately stabilized with fixation.
CLINICAL SITUATION FOR QUESTIONS 195 THROUGH 197
A 67-year-old woman with osteoarthritis is scheduled for total hip arthroplasty (THA). She has a history of hypertension and stenting for coronary artery disease. She has no surgical history. Her presurgical hemoglobin level is 11.5 g/dL (reference range, 14.0-17.5 g/dL).
Question 40
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10°. Initial management should consist of
Explanation
REFERENCES: Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 41
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 42
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Explanation
Question 43
-What is the recommended treatment for this injury?
Explanation
The hypertrophic zone of the growth plate has been implicated as the weak link in the physis in acute injuries. Epiphysiolysis of the proximal humerus in throwing athletes occurs as the result of tension and shear on the physis. More than 90% of affected patients who are treated with rest for an average of 3 months become asymptomatic. Prevention is the best option. Set limitations of the number of pitches and types of pitches depending on the age of the player. Also recommend use of proper pitching mechanics.
Question 44
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 45
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 46
A 51-year-old woman with shoulder pain responds transiently to a subacromial injection and physical therapy exercise program. When her symptoms recur, an arthroscopic subacromial decompression is recommended. During the surgery, a partial-thickness articular-sided supraspinatus tear is noted. The supraspinatus footprint is exposed for 3 mm from the articular margin. The remaining intra-articular structures are normal. Inspection from the bursal surface reveals the tendon to be intact. What is the most appropriate course of management? Review Topic
Explanation
Question 47
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 48
A year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging
stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 49
A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
Explanation
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
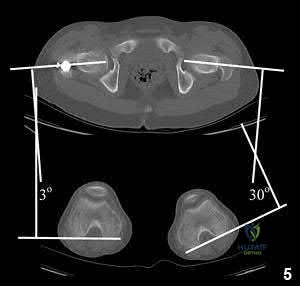
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
OrthoCash 2020
Question 50
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of Review Topic

Explanation
Question 51
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 52
Figure 1 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks?

Explanation
Question 53
What is the minimum hours per day of wear that has been correlated with the effectiveness of bracing on curve progression in idiopathic scoliosis? Review Topic
Explanation
Question 54
The parents of a 3-year-old girl who has had pain and swelling in the right ankle for the past 3 months now report that she has a limp and that the right knee and both ankles are painful and swollen. The limp and difficulty walking are most severe in the morning when the child first gets out of bed and are also more severe after extended walking. The parents deny fever, chills, weight loss, or night pain. Examination shows mild swelling and slightly restricted motion of the right knee and both ankles but is otherwise normal. In addition to initiation of treatment, the child should be referred to which of the following specialists?
Explanation
REFERENCES: Carey TP: Inflammatory arthritides: Juvenile rheumatoid arthritis, seronegative spondyloarthropathies, transient synovitis, hemophilic arthropathy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1315-1321.
Wright D: Juvenile idiopathic arthritis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 427-458.
Question 55
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
Question 56
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?
Explanation
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
McCarty EC, Tsairis P, Warren RF: Brachial neuritis. Clin Orthop Relat Res 1999;368:37-43.
Question 57
Which of the following statements is true regarding the posterior oblique portion of the medial collateral ligament of the elbow? Review Topic
Explanation
The medial ulnar collateral ligament is one of the primary static stabilizers of the elbow and is composed of three parts: anterior, posterior and transverse. The MCL provides resistance to valgus and distractive stresses. The anterior oblique fibers (of the anterior bundle) are the most important against valgus stresses. The posterior bundle is involved elbow contractures and releasing it can yield significant flexion gains, without creating valgus instability.
Morrey et al. performed a pilot study on 4 specimens and found the valgus stability is equally divided among the medial collateral ligament complex, anterior capsule, and bony articulation in full extension; whereas, at 90 degrees of flexion the contribution of the anterior capsule is assumed by the medial collateral ligament which provides approximately 55% of the stabilizing contribution to valgus stress.
Regan et al. was a subsequent study by the same group that found the posterior medial collateral ligament (PMCL) was taut only when the elbow was in a flexed position. Among the collateral ligaments, the anterior (AMCL) was the strongest and stiffest. (Of note, using present terminology these would be referred to as posterior oblique and anterior oblique portions of the medial ulnar collateral complex).
Wada et al. reported a series of open medial releases for post-traumatic elbow contracture and found scarring on the posterior oblique bundle in all cases. Large increases in flexion were achieved by releasing this structure and the capsule without the need for a lateral incision in most cases.
Illustrations A and B show the posterior oblique portion of the medial collateral ligament. Illustration C shows the most recent terminology and identifies the area to be resected for stiffness.
Incorrect Answers:
Question 58
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
REFERENCES: Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Eilber FC, Rosen G, Nelson SE, et al: High-grade extremity soft tissue sarcomas: Factors predictive of local recurrence and its effect on morbidity and mortality.
Ann Surg 2003;237:218-226.
Question 59
Which of the following pieces of equipment currently offers the greatest opportunity for lowering the number of equestrian injuries?
Explanation
REFERENCES: Ball CG, Ball JE, Kirkpatrick AW, et al: Equestrian injuries: Incidence, injury patterns, and risks factors for 10 years of major traumatic injuries. Am J Surg 2007;193:636-640.
Frankel HL, Haskell R, Digiacomo JC, et al: Recidivism in equestrian trauma. Am Surg 1998;64:151-154.
A 38-year-old man is three quarters of the way through the Hawaiian Ironman events run in a temperature of 60°F. He is sweating profusely and suddenly collapses. Prior to this he had been drinking large amounts of bottled water at every water stop. What is the most likely diagnosis?
Hypernatremia
Hypothermia
Hyponatremia
Subendocardial myocardial infarction
Ruptured berry aneurysm
DISCUSSION: Hyponatremia is often seen in endurance athletes such as triathloners, ultramarathoners, and marathoners after prolonged exertion. It is commonly attributed to excess free water intake that fails to replete massive sodium losses that result from sweating as reported by O’Connor. Exercise-induced hyponatremia is generally asymptomatic, particularly in patients in whom the sodium is only mildy reduced. Up to 10% of ultradistance athletes have a sodium level of 135 mEq/L or less, but those who are symptomatic usually have a sodium level of 125 mEq/L as reported by Noakes and O’Connor. The best way to prevent hyponatremia is to maintain the proper volume and types of fluid intake to ensure fluid balance during exercise. Beverages containing carbohydrates in concentrations of 4% to 8% (ie, “sports drinks”) are recommended for athletes participating in exercise lasting more than an hour (eg, marathon runners, etc.) To avert brainstem herniation and death, severe, acute hyponatremia requires rapid correction. Oral rehydration with salty solutions is safe and effective in patients with mild symptoms.
Too rapid correction has been reported to cause central pontine myelinolysis; therefore, correction ought to be performed slowly. Hypernatremia, hypothermia, subendocardial myocardial infarction, or ruptured berry aneurysm are unlikely in this scenario.
REFERENCES: O’Connor RE: Exercise-induced hyponatremia: Causes, risks, prevention, and management. Cleve Clin J Med 2006;73:S13-S18.
Noakes T: Hyponatremia in distance runners: Fluid and sodium balance during exercise. Curr Sports Med Rep
2002;1:197-207.
Laureno R, Karp BI: Myelinolysis after correction of hyponatremia. Ann Int Med 1997;126:57-62. Question 50
A 20-year-old male tennis player reports the acute onset of ulnar-sided wrist pain after hitting a forehand shot. Examination reveals dorsoulnar tenderness and minimal swelling. The pain is recreated with supination, wrist flexion, and ulnar deviation. Radiographs are normal. What structure is most likely involved?
Ulnar styloid
Flexor carpi radialis tendon
Extensor carpi ulnaris tendon
Scapholunate ligament
Transverse carpal ligament PREFERRED RESPONSE: 3
DISCUSSION: Extensor carpi ulnaris (ECU) lesions produce pain at the dorsoulnar aspect of the wrist, particularly during wrist supination, wrist flexion, and ulnar deviation. It has been frequently described in tennis players. Most ECU tenosynovitis can be successfully treated nonsurgically with immobilization techniques. Surgical treatment is generally indicated for ECU tenosynovitis or tendinopathy that does not respond to rest. Anatomically, the ECU retinaculum can rupture and the tendon can leave its sheath. With supination, the tendon can leave the sheath and then return to its position during pronation.
REFERENCES: Montalvan B, Parier J, Brasseur JL, et al: Extensor carpi ulnaris injuries in tennis players: A study of 28 cases. Br J Sports Med 2006;40:424-429.
Allende C, Le Viet D: Extensor carpi ulnaris problems at the wrist: Classification, surgical treatment and results. J Hand Surg Br 2005;30:265-272.
Question 60
The quadrilateral space in the shoulder contains which of the following structures?
Explanation
REFERENCES: Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 61-62.
Question 61
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 62
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
REFERENCE: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 32-33.
Question 63
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of
Explanation
REFERENCES: Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 64
In a postganglionic brachial plexus lesion at Erb’s point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29.
Zimmerman NB, Weiland AJ: Assessment and monitoring of brachial plexus injury in the adult, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA,
JB Lippincott, 1991, vol 2, pp 1273-1283.
Question 65
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
REFERENCES: Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 66
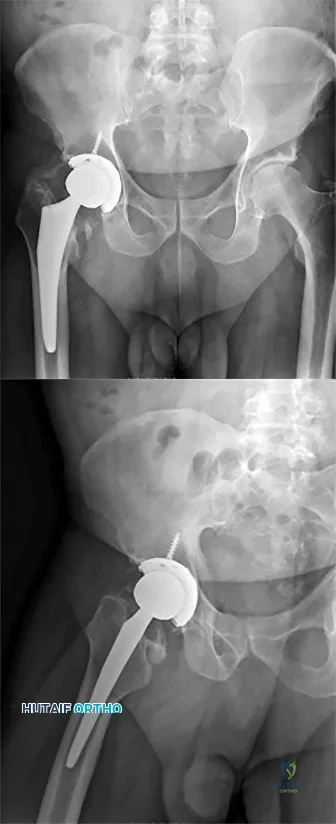
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 67
A 62-year-old runner injured his right ankle 8 weeks ago. He has ongoing lateral ankle pain and swelling that did not improve with 4 weeks of immobilization and 4 weeks of physical therapy. MR images demonstrate a longitudinal tear of the peroneus brevis tendon. Treatment should involve
Explanation
Additional nonsurgical treatment is not beneficial for peroneal tendon tears. Early repair of longitudinal tears reduces risk for progression to a full-thickness tear that would necessitate peroneus brevis to peroneus longus tenodesis. Platelet-rich plasma has no role in peroneal tendon tears.
RECOMMENDED READINGS
Arbab D, Tingart M, Frank D, Abbara-Czardybon M, Waizy H, Wingenfeld C. Treatment of isolated peroneus longus tears and a review of the literature. Foot Ankle Spec. 2014 Apr;7(2):113-8. doi: 10.1177/1938640013514273. Epub 2013 Dec 30. Review. PubMed
PMID: 24381076.View Abstract at PubMed
Coughlin MJ, Schon LC. Disorders of tendons. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014: 1188-1291.
RESPONSES FOR QUESTIONS 71 THROUGH 75
Lapidus procedure
First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
Proximal first metatarsal osteotomy
Distal first metatarsal chevron osteotomy
Biplanar distal first metatarsal osteotomy
Match the appropriate surgical procedure listed above with the clinical scenario described below.
Question 68
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 69
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
REFERENCES: Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int
2001;22:47-50.
Trnka HJ, Muhlbauer M, Zettl R, et al: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 70
A 41-year-old male truck driver fell off his truck and tried to break his fall by holding on to the side of the door with his left arm. His MRI is depicted in Figures A. Which of the following special tests would most likely be positive on physical examination? Review Topic
Explanation
While the subscapularis is the largest of the rotator cuff muscles, the relative
prevalence of injuries to the subscapularis tendon has only recently been recognized. The primary function of the subscapularis is to internally rotate the humerus. Patients with such injury often present with anterior shoulder pain, and increased external rotation compared to the contralateral limb. It is often associated with medial subluxation of the long head of biceps. A number of special tests have been developed to help aid in the clinical diagnosis of this injury including the belly press, lift off and bear hug tests.
Gerber et al. demonstrated the efficacy of a simple clinical maneuver called the ‘lift-off test’ to reliably diagnose or exclude clinically relevant rupture of the subscapularis tendon in 16 patients.
Barth et al. evaluated the diagnostic value of three clinical tests commonly used to diagnose subscapularis tendon tears; the lift-off test, belly-press test, and bear-hug test. They found that the lift-off test was the most difficult for patients to perform. However, when it was performed and found to be positive, it was 74% sensitive of very severe tears. They also found that the bear hug test was the most sensitive of all tests (82%).
Figures A shows an axial MRI arthrogram showing a subscapularis tear with dislocation of the biceps tendon. Illustration A demonstrates how to perform the bear hug test.
Incorrect Answers:
Question 71
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
REFERENCES: Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362.
Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307.
Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 72
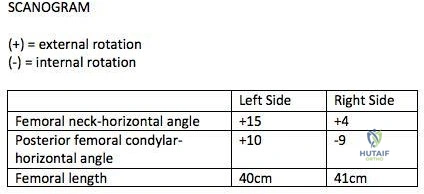
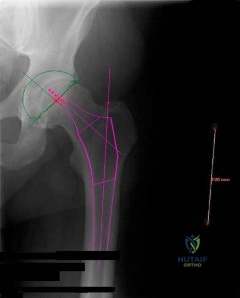
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
Explanation
>15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles. This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH -PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs. Therefore <15 degrees of rotational difference after fixation is considered acceptable.
Gugala et al. examined the long-term functional implications for patients with iatrogenic femoral malrotation following femoral intramedullary nail fixation. They
showed that patients can compensate for even significant femoral malrotation (up to 30 degrees) and tolerate it well. However, external femoral malrotation (more common) appears to be better compensated/tolerated than internal malrotation.
Figure A shows that the left femoral neck is externally rotated (ER) by 15° to the horizontal (ER15). The right femoral neck is externally rotated (ER) by 4° to the horizontal (ER4). The left distal fragment is ER10. The right distal fragment is internally rotated (IR) by 9°. Thus, left femur has a total (ER15)-(ER10)= (+15)-(+10)=(+5), and right femur has (ER4)-(IR9)= (+4)-(-9)=(+13) to the horizontal. Therefore, the difference is 8 degrees.
Incorrect Answers:
>15 degrees and symptomatic.
Question 73
A healthy, active year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in A radiograph taken after the fall is shown in He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 74
You perform an ACL reconstruction with bone-patella tendon-bone (BTB) autograft and are explaining the postoperative rehabilitation protocol to your patient. Which of the following is associated with increased quadriceps volume and improved quadriceps strength at 1 year without a higher risk of knee instability? Review Topic
Explanation
Proper rehabilitation following ACL reconstruction is vital to a successful outcome. The cornerstone of ACL rehabilitation is range of motion, strengthening and functional exercises without risk of destabilizing the knee. There are a variety of rehabilitation protocols and recently an effort has been made to standardize the approach to postoperative ACL care. An accelerated protocol starting at 3 weeks postoperatively has been deemed safe and may enhance the speed and safety with which an athlete returns to play.
Kruse et al completed a meta-analysis of 29 Level I and II studies focused on the ACL rehabilitation process. The authors concluded that immediate postoperative weightbearing and knee range of motion 0-90 is safe. Early eccentric strengthening appears to accelerate and improve strength gains at 1 year as compared to delayed eccentric strengthening. Home-based rehabilitation programs can be as effective as formal physical therapy. Postoperative bracing and CPM use is neither necessary nor beneficial.
Van Grinsven et al conducted a systematic review of ACL rehabilitation programs and physical therapy modalities to develop an evidence-based rehabilitation protocol. The authors demonstrated that an accelerated protocol without postoperative bracing focused on reduction of pain, swelling and inflammation and regaining range of motion, strength and neuromuscular control has significant advantages and does not lead to stability problems.
Gerber et al performed a randomized trial comparing two accelerated postoperative rehabilitation protocols – early eccentric (ECC) rehabilitation versus traditional (TRAD) rehabilitation starting at 3 weeks. There were no significant differences in knee pain, effusion or stability. However, quadriceps strength, hopping distance and activity level improved by a significantly greater amount in the ECC group versus the TRAD group at 26 weeks postoperatively. In a separate analysis of these patients, quadriceps and gluteus muscle cross-sectional area and volume in ECC patients were more than twice those in the TRAD group.
Illustration A depicts two eccentric ergometers that can be used in postoperative ACL rehabilitation.
Incorrect Responses:
another Answer
type of brace,
2:
There
duration is
of
bracing or no bracing at all.
no
advantage
to
CPM
use.
Question 75
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
REFERENCES: DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 76
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T 1 -weighted, T 2 -weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?
Explanation
T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present.
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 77
-The center of rotation of the knee can be best described as
Explanation
Question 78
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
Explanation
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. View Abstract at PubMed
Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.View Abstract at PubMed
Question 79
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament.
REFERENCES: Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 80
- The radiographs shown in Figures 71a through 71c, and the CT scan shown in Figure 71d reveal an acetabular fracture that should be classified as
Explanation
Note the classic “Spur Sign” seen in these radiographs. This is pathognomonic of a both-column fracture of the acetabulum.
The other defining feature of the both column fx (as evident by these films) is that there is no intact acetabulum connected to the bone fragment which is connected to the ipsilateral SI joint.
Question 81
Figure 32 shows the T2-weighted MR image through the L4-5 level of a 60-year-old man who has new-onset acute right lower-extremity pain and numbness and weakness in his right quadriceps muscle. The arrow in Figure 32 is pointing to which structure?
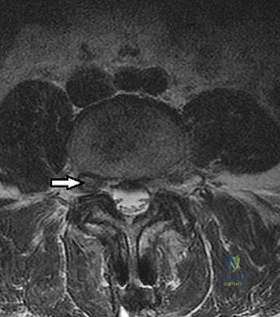
Explanation
The arrow is pointing to a structure of medium signal intensity that is equivalent to the nucleus pulposus on T2-weighted sequencing. This represents a foraminal disk herniation. A lumbar synovial cyst would display high-signal intensity on T2-weighted sequencing. Lumbar synovial cysts arise from the facet joints as a result of facet joint degeneration and may be a source of nerve root compression. The dorsal root ganglion is a collection of sensory nerve cell bodies and can be seen just dorsal and lateral to the disk herniation in Figure 32. The ligamentum flavum is located on the ventral
surface of the laminae and attaches between the laminae of adjacent vertebrae.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
Carrino JA, Morrison WB. Musculoskeletal imaging. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:119-136.
Question 82
- Which of the following shoulder girdle muscles is most active during forward flexion?
Explanation
Question 83
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)? Review Topic
Explanation
Question 84
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 85
03 Fig 51c. What laboratory finding is most likely associated with this disease entity?
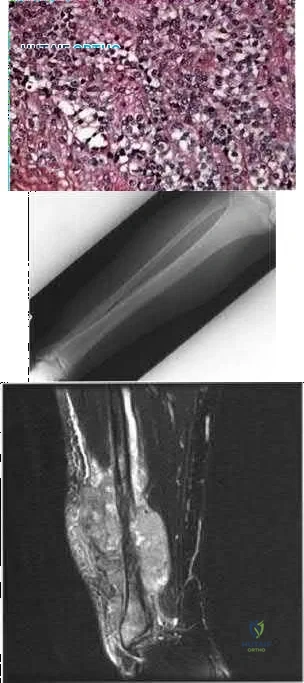
Explanation
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Inst Course Lect 2002;51:413-428
back to this question next question
Question 86
1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
Question 87
The main blood supply to the lateral two thirds of the talar body is provided by the
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1465-1518.
Haliburton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115-1120.
Question 88
Figure 46 shows the AP radiograph of an active 80-year-old patient with an acetabular fracture. The fracture was initially managed nonsurgically; however, the patient is now scheduled to undergo total hip arthroplasty. What is the treatment of choice for the contained acetabular bone defect?
Explanation
REFERENCES: Mears DC: Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128-141.
Bellabarba C, Berger RA, Bentley CD, et al: Cementless acetabular reconstruction after acetabular fracture. J Bone Joint Surg Am 2001;83:868-876.
Question 89
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Explanation
REFERENCES: Tencer AF, Johnson KD: Biomechanics in Orthopaedic Trauma: Bone Fracture and Fixation. Philadelphia, PA, JB Lippincott, 1994.
Gonza ER: Biomechanical long bone injuries, in Gonza ER, Harrington IJ (eds): Biomechanics of Musculoskeletal Injury. Baltimore, MD, Williams & Wilkins, 1982, pp 1-30.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, p 297.
Question 90
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?
Explanation
REFERENCES: Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 91
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 92
A 14-year-old male sustains the injuries shown in Figures A and B after a fall off the roof of his house. What is the most appropriate management? Review Topic

Explanation
Pediatric femoral neck fractures are classified into transphyseal, transcervical, cervicotrochanteric and intertrochanteric (Delbets I-IV) respectively. Fixation type varies by author, but generally speaking, Types I-III can be treated with smooth wires for patients 0-3yrs of age, 4.5-6.5 mm cannulated screws 4-10yrs of age, or l 6.5-
Question 93
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 94
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 95
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? Review Topic
Explanation
not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
Question 96
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of
Explanation
REFERENCES: Black GB, Grogan DP, Bobechko WP: Butler arthroplasty for correction of adducted fifth toe: A retrospective study of 36 operations between 1968 and 1982. J Pediatr Orthop 1985;5:439-441.
Paton RW: V-Y plasty for correction of varus fifth toe. J Pediatr Orthop 1990;10:248-249.
Coughlin MJ, Mann RA: Lesser toe deformities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 5. St Louis, MO, Mosby, 1986, pp 132-157.
Question 97
Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral antibiotic therapy resolved the sepsis, and blood glucose levels are now well controlled. The patient has no palpable pulses. The ankle-brachial index is 0.70. Laboratory studies show a WBC count of 8,500/mm 3 , a serum albumin of 1.9 g/dL, and a total lymphocyte count of 1,500/mm 3 . What treatment has the best potential to optimize his survival and independence?
Explanation
REFERENCES: Pinzur MS, Stuck RR, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Pinzur MS, Smith D, Osterman H: Syme ankle disarticulation in peripheral vascular disease and diabetic foot infection: The one-stage versus two-stage procedure. Foot Ankle Int 1995;16:124-127.
Question 98
A newborn with bilateral talipes equinovarus undergoes serial manipulation and casting. What is the primary goal of manipulation?
Explanation
REFERENCES: Ponseti IV: Common errors in the treatment of congenital clubfoot. Int Orthop 1997;21:137-141.
Ponseti IV, Smoley EU: Congenital club foot: The results of treatment. J Bone Joint Surg Am 1963;46:261-275.
Question 99
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
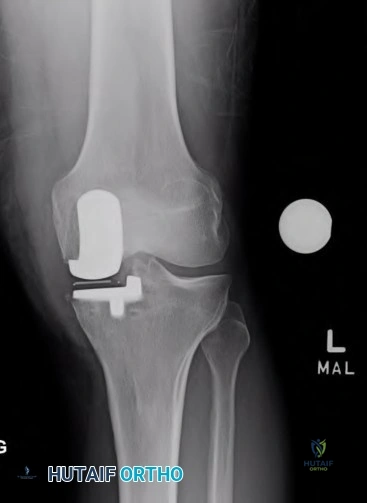
Explanation

OrthoCash 2020
Which of the following is the most common cause of early revision surgery (<20 weeks) following a hip resurfacing arthroplasty?
Periprosthetic fracture
Rupture of abductors
Dislocation
Heterotopic ossification
Post-operative stiffness
Periprosthetic fracture, specifically femoral neck fracture, is the most common cause of early revision less than 20 weeks following surgery.
The rate of femoral neck fractures following hip resurfacing varies, but most literature reports a rate of 1%. A majority of these fractures happen in the early post-operative period and are the most frequent cause of revision surgery within several months following surgery. The cause is usually multifactorial, but placing the femoral implant in varus, osteonecrosis, and notching have been proven risk factors for fracture.
Little el al. report on 377 patients undergoing hip resurfacing. 13 required revision including 8 for fracture of the femoral neck and 3 for loosening of a component. Evidence of osteonecrosis was seen in two of these cases, leading the authors to believe it may contributed to fracture.
Illustration A shows a comparison of a typical total hip replacement and a hip resurfacing arthroplasty. Illustration B shows notching of the femoral neck, a known cause of femoral neck fracture following hip resurfacing. Illustration C shows a femoral neck fracture in a patient with a hip resurfacing.
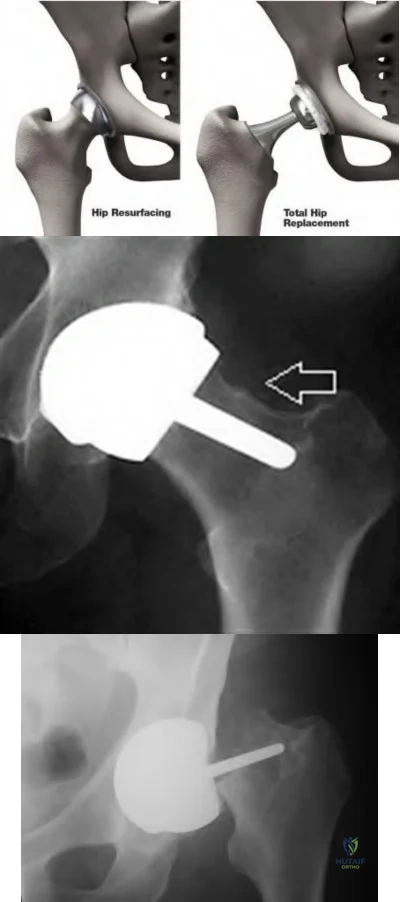
OrthoCash 2020
A 55-year-old male undergoes a revision total knee arthroplasty of an implant that is only 3 years old. At the time of surgery, the tibial polyethylene liner shows catastrophic delamination and cracking. What is the most likely cause of this extensive, accelerated wear of the polyethylene liner?
Sterilization in ethylene oxide
Gamma irradiation of the polyethylene liner in the presence of air
Gamma irradiation of the polyethylene liner with vacuum packaging
Gamma irradiation of the polyethylene liner in nitrogen
Gamma irradiation of the polyethylene liner in argon Corrent answer: 2
Irradiation of polyethylene in air (i.e. oxygen present) has been shown to be a risk factor for catastrophic failure after total knee replacement.
Free radicals are generated when polyethylene is irradiated in the presence of air. Initially, these free radicals result in cross-linking. However, if the polyethylene is exposed to these free radicals for an extended period of time, delamination, cracking, and catastrophic failure may ensue. The industry has completely abandoned this method of sterilization as a result. Currently, the standard of care is irradiation of polyethylene in an inert gas (e.g. argon, nitrogen or vacuum packaging). The amount of oxidative products when polyethylene is sterilized in the absence of oxygen is much less and does not lead to catastrophic failure.
Sterilization without irradiation is another option (ethylene oxide). When this occurs, there is no cross-linking and thus the increased wear properties are lost. However, since there is no oxidization, you do not have the risk of catastrophic failure as seen in those liners irradiated in the presence of oxygen.
The cited reference by McNulty et al. from Orthopedics discusses the influence of sterilization methods on wear performance. They found that gamma irradiation and storage of the polyethylene components in an essentially oxygen-free environment imparted by gamma irradiation in a vacuum foil pouch (GVF) protects the components from oxidization.
Illustration A shows a polyethylene liner that has undergone catastrophic wear as a result of irradiation in the presence of oxygen.
Incorrect Answers:
catastrophic wear, although wear properties are less than gamma irradiation in the absence of air.

OrthoCash 2020
Which of the following interventions reduces osteolysis around distal portion of the femoral stem when performing a total hip arthroplasty?
Use of an extended offset femoral neck component
Use of a proximal circumferentially coated ingrowth stem
Use of a collared stem
Use of a long femoral stem
Ensuring that the stem fills the diaphysis of the femur Corrent answer: 2
Osteolysis of the femur is caused by activation of macrophages by microscopic polyethylene particles within the "effective joint space", defined as any area where joint fluid can come into contact with bone. This can occur above the acetabular cup, through screw holes, and down the femoral shaft around the prosthetic stem. Ideally, with a cementless stem, both the proximal and metaphyseal femur are well filled by the prosthesis. Collared stems are used to augment poor calcar bone quality or bone loss.
Sinha et al showed in a retrospective review of 101 hips with cementless circumferentially coated femoral stems no distal femur osteolysis occurred, but 82% showed “evidence of proximal femur stress shielding”, though only 38% showed proximal femoral osteolysis.
OrthoCash 2020
During a minimally invasive approach to total hip arthroplasty a femoral periprosthetic fracture occurs. Which of the following steps is crucial to properly treat this complication?
Transitioning to an extensile approach to adequately visualize and reduce the fracture
Limiting post-operative weight bearing
Switching to a cemented femoral stem to avoid the stresses created during press-fit fixation
Delaying the arthroplasty until the fracture has healed
Supplementing the fracture with autograft Corrent answer: 1
Proper treatment of an intraoperative femoral fracture during total hip arthroplasty involves adequate exposure, anatomic reduction, and bypassing the fracture site by 2 cortical diameters of the femur with a long stem. This may involve repositioning the patient on the table if the arthroplasty is performed in the supine position. Minimally invasive surgical techniques have been developed to insert the components through smaller exposures and less soft tissue dissection. The purported advantages include faster rehabilitation, less blood loss, shorter hospital stays, and better cosmesis. However, complications an arise if the surgeon sacrifices surgical exposure and visualization.
Fehring et al review 3 cases of total hip arthroplasty performed through minimally invasive techniques with catastrophic outcomes. Intra-operative fracture, chronic instability, and death were all identified.
OrthoCash 2020
A 70-year-old man underwent total hip arthroplasty 4 months ago and has experienced 3 dislocations. Radiographs reveal no failure of the hardware and an acetabular component that has an abduction
angle of 40 degrees and a version of 10 degrees retroverted. What is the most appropriate treatment for the recurrent dislocations?
hip abduction brace
revision of the acetabular liner to a constrained type
revision of the entire acetabular component
revision of the femoral head to a larger size
revision to an extended offset prosthesis Corrent answer: 3
Per Dorr et al: post-operative hip instability can be caused by several factors: soft tissue imbalance, component malposition, or position. Component malposition, as in this case, should be treated with revision of the offending component. In this case the acetabulum was placed in retroversion when it should have been 15-20 degrees anteverted. None of the other options addresses the cause of the instability. According to Morrey, the most signficant risk factors to instability are prior hip surgery, trochanteric nonunion, and posterior surgical approach. He wrote that the most reliable way to correct instability is to reorient a retroverted acetabular cup.
OrthoCash 2020
In patients with sickle cell disease and asymptomatic osteonecrosis of the femoral head identified with magnetic resonance imaging, what percentage will eventually go on to femoral head collapse?
Question 100
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
