OITE & ABOS Orthopedic Board Exam MCQs: Fracture, Infection, Trauma | Part 236

Key Takeaway
This page presents Part 236 of a comprehensive orthopedic board review. Featuring 100 high-yield MCQs, it's designed for OITE and AAOS exam prep. Orthopedic surgeons and residents can enhance knowledge on topics like Fracture, Infection, and Trauma through interactive study and exam modes.
About This Board Review Set
This is Part 236 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 236
This module focuses heavily on: Fracture, Infection, Trauma.
Sample Questions from This Set
Sample Question 1: A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of...
Sample Question 2: Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?...
Sample Question 3: All of the following are factors associated with transfer of patients to Level 1 trauma centers EXCEPT:...
Sample Question 4: A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Fi...
Sample Question 5: A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynami...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 2
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
REFERENCES: Sady SP, Wortman M, Blanke D: Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil 1982;63:261-263.
Tanigawa MC: Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys Ther 1972;52:725-735.
Wallin D, Ekblom B, Grahn R, Nordenberg T: Improvement of muscle flexibility: A comparison between two techniques. Am J Sports Med 1985;13:263-268.
Question 3
All of the following are factors associated with transfer of patients to Level 1 trauma centers EXCEPT:

Explanation
Question 4
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
REFERENCES: McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 5
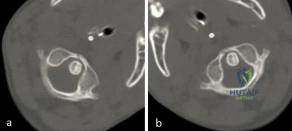
A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynamic computed tomographic (CT) was obtained and shown in Figure A. Panel (a) shows an axial image with maximal rotation to the left. Panel (b) shows an axial image with maximal rotation to the right. What is the most appropriate next step in management? Review Topic
Explanation
Common causes of Atlantoaxial rotatory displacement (AARD) include infection, trauma, and recent neck surgery. Diagnosis is challenging and is best confirmed with dynamic CT (CT with the head turned maximally to either side and at neutral). If the symptoms are acute (less than 7 days) then initial treatment with a soft collar and anti-inflammatory medications is indicated. If the condition has been present for more than a week, more aggressive treatment with halter traction (present 1 week to 1 month) or halo traction (present for 1-3 months) is indicated. If nonoperative modalities fail, the condition has been present for > 3 months, or the patient has neurologic deficits, then posterior C1-C2 fusion is indicated.
Copley et al discuss the evaluation and treatment of various congenital and traumatic conditions of the pediatric cervical spine. They report that the underlying mechanism of Atlantoaxial rotatory displacement (AARD) is inflammation and spasm which can be caused by infection, prior surgery, trauma, and rheumatoid arthritis.
Subach et al reviewed at 20 children with atlantoaxial rotatory subluxation. They found that of the 20 patients treated overall, conservative management failed in 6 (30%), and they required posterior fusion because of recurrence of the atlantoaxial rotatory subluxation or unsuccessful reduction. The major factor predicting the failure of conservative management was the duration of subluxation before initial reduction. Patients with long-standing subluxation were more likely to experience recurrence and require surgery.
Figure A shows an asymmetric placed odontoid within the ring of C1. There is an increased distance from the odontoid to the right arch of C1 which is fixed and minimally changes with maximal rotation to the left. This radiographic finding is indicative of fixed subluxation. Illustration A further demonstrates this.
Incorrect
(SBQ12SP.1) A 65-year-old female with a history of breast cancer presents with bilateral buttock and leg pain that is worse with walking and improves with sitting. In addition, she reports that she feels unsteady on her feet and requires holding the railing when going up and down stairs. On physical exam she is unable to complete a tandem gait and has hip flexion weakness, ankle dorsiflexion weakness, and ankle plantar flexion weakness. Her reflex exam shows 3+ bilateral patellar reflexes. Radiographs and an MRI are shown in Figure A and B. What is the next most appropriate step in management. Review Topic

Lumbar epidural injection
Physical therapy with core strengthening and anti-inflammatory medications as needed
Lumbar decompression
Lumbar decompression and fusion
MRI of the cervical and thoracic spine
The clinical scenario is consistent with a patient with symptoms of degenerative spondylolisthesis AND symptoms of myelopathy. Myelopathy must be ruled out by performing an MRI of the cervical and thoracic spine.
Tandem stenosis occurs in approximately 5 to 25% of patients. Because of the stepwise progressive nature of myelopathy, treatment of myelopathy often takes precedence over lumbar spinal stenosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies. Both the upward babinski reflex and the presence of clonus were found to be very non-sensitive (13%). The most sensitive provacative test was found to be the Hoffman sign (59%).
Salvi et al. reviewed the classic presentations for cervical myelopathy including demographics, history, and physical exam findings (the inability to preform a tandem gait, hyperreflexia, an abnormal babinksi and hoffman reflex, the inability to preform rapid movements and bilateral muscle weakness). Additionally they identify other potential causes for myelopathy, including multiple sclerosis, amyotrophic lateral sclerosis, multifocal motor neuropathy, and Guillain-Barre´syndrome.
Maezawa et al. showed that gait analysis can identify a pattern in patients with myelopathy. Patients with severe myelopathy have a characteristic gait with hyperextension of the knee in the stance phase without plantar flexion of the ankle in the swing phase. They also have decreased walking speed and stride length with a prolonged stance phase.
Figure A and B show a classic degenerative spondylolisthesis.
Incorrect Answers:
Question 6
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
REFERENCES: Chance PF: Molecular genetics of hereditary neuropathies. J Child Neurol 1999;14:43-52.
Bell C, Haites N: Genetic aspects of Charcot-Marie-Tooth disease. Arch Dis Child 1998;78:296-300.
Question 7
Figure 242 is the anteroposterior radiograph of a 28-year-old man who underwent resection and reconstruction for an Ewing sarcoma. What is the most common functional deficit encountered during rehabilitation?
Explanation

Question 8
What complication is most likely to occur following proximal humeral fixation with a locked plate-and-screw construct?
Explanation
reduction which can result in failure. However, penetration of the screws remains the most commonly reported complication.
Question 9
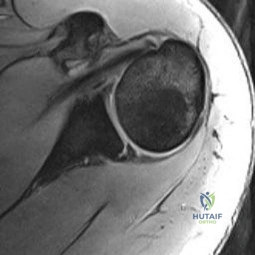
If the structure marked by the tip of the probe in Figure 94 is repaired to the bony glenoid with suture anchors during an arthroscopic stabilization procedure, what is the most likely result? Review Topic

Explanation
Question 10
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
Explanation
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.

Question 11
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?
Explanation
REFERENCES: Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.
Vienne P, Schoniger R, Helmy N, et al: Hindfoot instability in cavovarus deformity: Static and dynamic balancing. Foot Ankle Int 2007;28:96-102.
Question 12
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 13
A normal functioning posterior tibialis tendon is best confirmed by which of the following physical findings?
Explanation
Question 14
A 58-year-old woman has had a slowly progressing mass over the distal interphalangeal (DIP) joint of her dominant hand with a worsening deformity of her nail. She has no significant medical history but underwent bilateral knee arthroplasties 1 year ago. Radiographs reveal a small osteophyte at the DIP joint dorsally. A clinical photograph and a biopsy specimen are shown in Figures 76a and 76b. What is the most likely diagnosis?
Explanation
REFERENCES: Fritz GR, Stern PJ, Dickey M: Complications following mucous cyst excision. J Hand Surg Br 1997;22:222-225.
Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
Question 15
Local administration of recombinant bone morphogenetic protein-2 (rhBMP-2) to patients with type III-A and III-B open tibial shaft fractures at the time of initial surgery has shown all of the following when compared to standard treatment EXCEPT:

Explanation
Question 16
This medication, a factor Xa inhibitor, currently is not approved for venous thromboembolism (VTE) prophylaxis.
Explanation
Warfarin has a long clinical track record and is well known among most physicians. It is a vitamin K antagonist that can be monitored with prothrombin time (INR) testing and reversed with vitamin K and fresh frozen plasma if needed. Newer oral anticoagulants are becoming more common and offer the advantage of being rapidly active without a need for monitoring. These oral anticoagulants are not reversible, which can complicate the treatment of patients who present with bleeding or require surgery. Dabigatran (Pradaxa) is a direct thrombin inhibitor that is approved for stroke prevention in atrial fibrillation. It is not reversible, and a surgical delay of 24 to 48 hours is recommended for all but emergent surgeries. A longer delay is recommended with renal insufficiency. Rivaroxaban (Xarelto) is an oral factor Xa inhibitor that is approved for atrial fibrillation and the treatment of VTE and deep vein thrombosis prophylaxis. It offers the advantage of daily dosing. It
is not reversible and a surgical delay of 36 to 48 hours is recommended. Apixaban (Eliquis) is another factor Xa inhibitor for which twice-daily dosing is required. It is currently approved for stroke prevention in atrial fibrillation, and a surgical delay of 36 to 48 hours is recommended.
RECOMMENDED READINGS
Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013 May;88(5):495-511. doi: 10.1016/j.mayocp.2013.03.006. Review. Erratum in: Mayo Clin Proc. 2013 Jul;88(7):777. PubMed PMID: 23639500. View Abstract at PubMed Alquwaizani M, Buckley L, Adams C, Fanikos J. Anticoagulants: A Review of the Pharmacology, Dosing, and Complications. Curr Emerg Hosp Med Rep. 2013 Apr 21;1(2):83-97. Print 2013 Jun. PubMed PMID: 23687625. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 100 AND 101
A 55-year-old woman slipped on ice while getting out of her car and sustained the injury shown in Figure 100.

Question 17
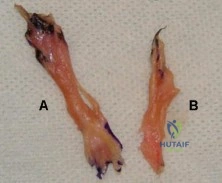
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true? Review Topic
Explanation
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle.
Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion
>30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect
Question 18
A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?
Explanation
REFERENCES: Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Clark CR, White AA III: Fractures of the dens: A multicenter study. J Bone Joint Surg Am 1985;67:1340-1348.
Question 19
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
Explanation
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non-vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age >60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Question 20
A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Freeland AE, Geissler WB: Plate fixation of metacarpal shaft fractures, in Blair WF (ed): Techniques in Hand Surgery. Baltimore, MD, Williams and Wilkins, 1996, pp 255-264.
Question 21
-What gene is implicated in spinal muscular atrophy?
Explanation

Question 22
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
Question 23
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 24
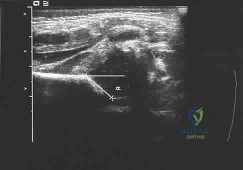
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? Review Topic
Explanation
not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
Question 25
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , include
Explanation
Question 26
A 23-year-old male is involved in a motor vehicle accident and sustains a left open femur fracture, right open humeral shaft fracture, and an LC-II pelvic ring injury. Which of the following best describes the radiographic findings associated with this pelvic injury pattern using the Young-Burgess Classification system?

Explanation
Burgess et al discuss the effectiveness of a treatment protocol as determined by their pelvic injury classification and hemodynamic status. The injury classification system was based on lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury types. They found that their classification-based treatment protocols reduce the morbidity and mortality related to pelvic ring disruption.
Tile discusses acute pelvic trauma and his classification system for pelvic injuries (ie. Types A, B, and C). He states that any classification system must be seen only as a general guide to treatment, and that the management of each patient requires careful, individualized decision making.
Incorrect
2:
This
describes
an
APC-II
injury
3:
This
describes
an
APC-III
injury
4:
This
describes
and
LC-I
injury
Question 27
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?
Explanation
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 28
A 44-year-old woman has bilateral knee pain, and history reveals bilateral hip replacements. Radiographs are seen in Figure 28a, and histopathologic specimens from the total hip replacement are shown in Figures 28b and 28c. Laboratory studies reveal anemia. What is the most likely diagnosis?
Explanation
REFERENCE: Dutkowsky J: Miscellaneous non traumatic disorders, in Crenshaw A (ed): Campbell’s Operative Orthopaedics. St Louis, MO, Mosby, 1992, pp 2007-2012.
Question 29
Figures 1 and 2 are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 9 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem?

Explanation
Plating of the proximal radius from a dorsal or Thompson approach (between the extensor carpi radialis brevis and extensor digitorum communis) allows complete visualization of the PIN through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 1 and 2.Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the extensor indicis proprius and the EDC of the ring finger to the extensor digiti quinti proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the mobile wad and the digital extensors will be more easily found.
Question 30
The term anorexia athletica refers to a problem whose criteria include all of the following, EXCEPT Review Topic
Explanation
Question 31
Figures 2a and 2b are this patient’s proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include
Explanation
This patient’s examination and history indicate recurrent patellar dislocations. Radiographs show an osseous or osteochondral loose fragment. There is no evidence of an obvious nondisplaced fracture or physeal changes. In the setting of suspected patella dislocation or subluxation with loose fragment seen on radiograph, an MRI is indicated. Lateral release alone is seldom indicated in a knee that is normal before injury. The examination and MRI do not indicate a need for medial collateral ligament repair. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence and the need for reconstruction.
Question 32
Figure 1 shows the radiograph obtained from a 67-year-old man recently diagnosed with osteoarthritis, 8 years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure 2. What is the most appropriate management at this time?

Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 33
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
REFERENCES: Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:1038-1047.
Question 34
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
Explanation
Question 35
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?

Explanation
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
Question 36
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 37
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and

Explanation
Question 38
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
REFERENCES: Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598.
Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Shereff MJ, Cullivan WT, Johnson KA: Osteoid-osteoma of the foot. J Bone Joint Surg Am 1983;65:638-641.
Question 39
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 40
The thickest bone in the occiput is located
Explanation
REFERENCES: Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
Ebraheim N, Lu J, Biyani A, et al: An anatomic study of the thickness of the occipital bone: Implications for occipitocervical instrumentation. Spine 1996;21:1725-1729.
Question 41
The best indication for a knee fusion after a failed total knee replacement is
Explanation
Question 42
A 17-year-old quarterback reports shoulder pain localized over the anterior aspect of the shoulder that occurs during the follow through phase of throwing. The pain worsens toward the end of the game, but becomes asymptomatic the next day. He denies any pain during the cocking phase of throwing or during normal daily activities. Examination reveals a negative relocation test and a negative posterior load and shift test. Motion of the shoulder is normal. An MRI arthrogram is shown in Figure 75. Based on the history, examination, and MRI findings, what initial treatment should be recommended? Review Topic
Explanation
Question 43
Bacitracin is a topical antibiotic agent that may be added to solutions and used for intraoperative lavage. What is this agent effective against?
Explanation
REFERENCES: Rosenstein BD, Wilson FC, Funderburk CH: The use of bacitracin irrigation to prevent infection in postoperative skeletal wounds: An experimental study. J Bone Joint Surg Am 1989;71:427-430.
Brooks GF, Butel JS, Morse SA (eds): Jawetz, Melnick, and Adelberg’ s Medical Microbiology: Antimicrobial Chemotherapy. New York, NY, McGraw-Hill, 1995, pp 187-188.
Question 44
A researcher is working on Medication A, a drug FDA-approved for the treatment of osteoporosis in men and women. It is an anti-resorptive agent that inhibits the formation, function and survival of osteoclasts. It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non-detectable. It can be used in the presence of cancer metastases to bone. What is Medication A? Review Topic
Explanation
Denosumab is a human monoclonal antibody against RANKL. By binding RANKL, it prevents interaction of RANKL with RANK (on OC and osteoclast precursors, OCP), and inhibits OC-mediated bone resorption, and the formation, function and survival of OC. In contrast, bisphosphonates bind to calcium hydroxyapatite in bone, and decrease resorption by decreasing function and survival (but not formation) of OC.
Vaananen et al. reviewed the cell biology of OC. During bone resorption, 3 membrane domains appear: ruffled border, sealing zone and functional secretory domain. The resorption cycle starts with migration, bone attachment, polarization (formation of membrane domains), dissolution of hydroxyapatite, degradation of organic matrix, removal of degradation products from resorption lacuna, and apoptosis of the OC or return to the non-resorbing stage.
Boyce et al. reviewed the regulation of osteoclasts and their functions. OCPs are held in bone marrow by chemokines e.g. stroma-derived factor-1 (SDF1) and attracted to blood by sphingosine-1 phosphate (S1P) (increased in synovial fluid of patients with RA). All aspects of osteoclast formation and functions are regulated by M-CSF and RANKL. More recent studies indicate that osteoclasts and their precursors regulate immune responses and osteoblast formation and functions by means of direct cell-cell contact through ligands and receptors, such as ephrins and Ephs, and semaphorins and plexins, and through expression of clastokines.
Warriner and Saag reviewed the diagnosis and treatment of osteoporosis. They defined osteoporosis as T-score of = -2.5 or a history of fragility fracture. Incident hip and vertebral fractures increase future risk of these fractures (hazard ratio 7.3 and 3.5, respectively).
Cummings et al. compared subcutaneous denosumab (60mg every 6mths) vs placebo in prevention of fractures in 7868 osteoporotic (T-score -2.5 to -4.0) postmenopausal women. They found that denosumab reduced risk of vertebral fracture by 68% (risk ratio, 0.32), hip fracture by 40% (hazard ratio 0.6), nonvertebral fracture by 20% (hazard ratio 0.8). There was no increased risk of cancer, infection, delayed fracture healing, cardiovascular disease, osteonecrosis of the jaw or adverse reactions. They concluded that it was useful for reduction of fractures in osteoporotic women.
The video shows the action of denosumab (prolia). Illustration A shows the different osteoclast zones.
Incorrect Answers:
Question 45
- A right-handed, 53 year old man reports pain in the left shoulder following a fall on an abducted externally rotated shoulder 3 months ago. Examination reveals pain on elevation and tenderness localized to the anterior aspect of the shoulder. Results of the lift-off test are inconclusive due to limited internal rotation. Figure 2 shows the T1-weighted axial image from an MRI-arthrogram. Treatment should include
Explanation
Question 46
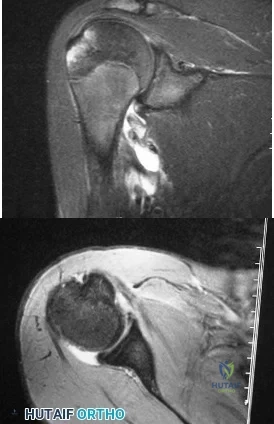
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon: Results of operative treatment. J Bone Joint Surg Am 1996;78:1015-1023.
Question 47
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Explanation
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
Question 48
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis? Review Topic

Explanation
Question 49
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Warner JJ, Johnson D, Miller M, Caborn DN: Technique for selecting capsular tightness in repair of anterior-inferior shoulder instability. J Shoulder Elbow Surg 1995;4:352-364.
Question 50
Figures below show the radiographs, and the MRIs obtained from a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?

Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
Question 51
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 52
Percutaneous placement of a lateral proximal tibial locking plate that extends down to the distal third of the leg is associated with postoperative decreased sensation of which of the following distributions?

Explanation
Question 53
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
Question 54
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of
Explanation
the fracture.
REFERENCES: Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Banks AS, Cain TD, Ruch JA: Physeal fractures of the distal phalanx of the hallux. J Am Podiatr Med Assoc 1988;78:310-313.
Question 55
The authors found that all 9 patients went on to both clinical and radiographic union. They concluded that the Masquelet technique was successful in effectively reconstructing traumatic and posttraumatic bony defects in the forearm with a low incidence of complications.
Explanation
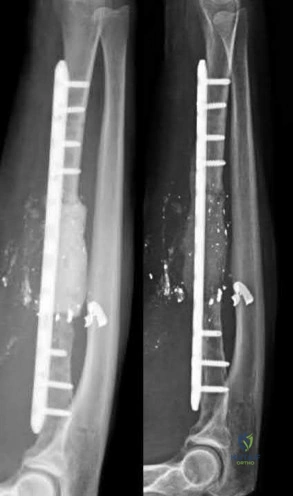
A 25-year-old male runs into a tree while going 45 mph on his motorcycle. He presents to your level 1 trauma hospital with the injuries shown in figures A through C. After closed reduction, which of the following is true with respect to treatment for this patient?

Heterotopic ossification is uncommon
Minifragment screws are sufficient for fracture fixation
Kocher-Langenbeck is the optimal surgical approach for this injury
Fragment excision leads to improved outcomes compared to open reduction and internal fixation
A 2 mm fragment step-off is considered the cut-off for non-surgical management
This patient has sustained a Pipkin II femoral head fracture with associated anterior hip dislocation. An open reduction with internal fixation of the femoral head fragments with direct visualization is indicated to restore stability and congruity of the hip joint. These fractures can be treated with mini-fragment screws with excellent reduction and purchase without risks of extensive chondral injury or screw prominence.
Femoral head fractures are uncommon injuries usually associated with hip dislocations. They are classified using the Pipkin Classification (Illustration B). While resection of small femoral head fracture fragments can be considered (Pipkin I) as sufficient and satisfactory treatment, this fragment is large and displaced and thus should be treated with ORIF for optimal results. Regarding the surgical approach, advocates for the direct anterior approach state direct access to the anterior portion of the femoral head with decreased overall complication rates. Other approaches, including surgical hip dislocation and Kocher-Langenbeck, are also useful depending on associated injuries (acetabulum fractures, etc.) and location of the head fragment. ORIF of these fractures can be performed with the use of countersunk mini-fragment screws, headless screws and even bioabsorbable pins to avoid prominence or extensive chondral injury.
Marecek et al. authored a review article on femoral head fractures. They described these injuries as being generally associated with hip dislocations and require prompt reduction. They noted that the surgical fixation of the femoral head is generally done through the direct anterior approach or via a surgical hip dislocation depending on associated injuries. The authors also discussed the importance of using mini-frag screws to avoid hardware prominence. They also noted that while heterotopic ossification is a common finding after the anterior approach for these injuries, it is rarely proven to be symptomatic.
Giannoudis et al. reviewed femoral head fractures focusing on management, complications and clinical results. They reported on 453 femoral head fractures in 450 patients. Regarding Pipkin Is, they noted that fragment excision gave better results compared to ORIF (p=0.07), while Pipkin IIs showed improved outcomes with ORIF. Regarding complications, they noted the following rates: wound infection (3%), sciatic nerve palsy (4%), AVN (11.9%), post-traumatic OA (20%) and HO (16.8%). They also noted the anterior approach was associated with promising long-term functional results and a lower incidence of major complication rates.
Figure A is an AP pelvis radiograph revealing a left hip dislocation with a large femoral head fracture extending into the weight-bearing zone of hip joint
(Pipkin II). Figures B and C are CT scan images revealing an anteriorly dislocated hip with a large femoral head fracture without associated acetabulum fractures. Illustration A is the post-op fluoroscopy showing ORIF of femoral head with multiple 2.7 cortical screws. Illustration B demonstrates the Pipkin classification for femoral head fractures.
Incorrect Answers:

Which of the following describes the most common organism cultured from septic olecranon bursitis?
Gram positive cocci in chains
Gram positive bacilli in branches
Gram positive cocci in pairs and clusters
Gram negative diplococci
Gram negative bacilli with thin rods Correct answer: 3
The most common cultured organism in the setting of septic olecranon bursitis is Staphylococcus aureus (S. aureus), appearing as gram positive cocci in pairs and clusters.
S. aureus is responsible organism in approximately 80% of cases of septic olecranon and prepatellar bursitis. Mixed flora is also common. Patient demographics in both conditions are similar, more commonly involving middle-aged males. Direct inoculation is presumed to be the primary culprit as opposed to hematogenous seeding, as blood supply to the bursal tissue is poor. Differentiating infectious from non-infectious bursitis can be challenging.
Aaron et al. provide a review article on the four most common types of bursitis: olecranon, prepatellar, trochanteric, and retrocalcaneal. They note that olecranon bursitis is the most common superficial bursitis, and that a careful history and physical exam can help differentiate infectious from noninfectious olecranon bursitis. The authors discuss one series of 46 patients demonstrating that a skin temperature overlying the affected bursa ≥2.2°C than the contralateral, unaffected bursa had a 100% sensitivity and 94% specificity in diagnosing a septic process.
Illustration A shows a patient with olecranon bursitis. Illustration B shows the classic gram stain for S. aureus (gram positive cocci in pairs and clusters).
Incorrect Answers:

During a trauma conference, a hand surgeon presents a case of a 25-year-old male who injured his elbow while roller skating. While describing the patient's radiographs, he reports that this injury is associated with valgus posterolateral rotatory instability. Which of the following images is most likely the patient's radiograph?

Posterolateral rotatory instability (PLRI) can result from a "terrible triad" fracture-dislocation pattern (seen in Figure E), classically involving a radial head fracture, coronoid tip or base fracture, and an elbow dislocation.
Terrible triad injuries typically occur with axial loading, supination, and a valgus directed force through the elbow. In comparison to PLRI which results from a terrible triad injury, posteromedial rotatory instability (PMRI) commonly results from an anteromedial coronoid facet fracture following a varus-directed force. These injuries also very frequently also have a lateral collateral ligament complex injury but often have no radial head fracture. PLRI is far more common than PMRI. Generally with a PLRI pattern, the lateral collateral ligament complex fails first, followed by injury to the anterior capsule or coronoid, and lastly the medial collateral ligament complex is affected. Nonoperative management is possible, but only indicated in small, non-displaced radial head fractures with small coronoid tip fractures. Typically, terrible triad injuries are addressed surgically with radial head fixation or arthroplasty, lateral collateral ligament repair, and, less commonly, coronoid fracture fixation or anterior capsule repair.
Ring et al. reviewed 56 patients who had been treated with an ORIF of the radial head at 48 months after injury. They found unsatisfactory outcomes for patients who had an ORIF of radial head fractures with greater than 3 articular fragments. The authors recommended ORIF of radial head fractures with 3 or few fragments.
Steinmann performed a review of coronoid process fractures. The author reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. Dr. Steinmann concludes that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL), and that medial instability is likely with involvement of the sublime tubercle.
Mathew et al. review the anatomic, biomechanical, and operative principles of terrible triad injuries. The authors discuss that the primary goal of fixation is to stabilize the elbow and allow early range of motion. They underscore technical improvements and implant developments which have improved outcomes.
Figure A demonstrates a capitellum fracture. Figure B demonstrates an olecranon fracture.
Figure C demonstrates a displaced radial head fracture.
Figure D demonstrates an anteromedial facet coronoid fracture.
Figure E demonstrates a terrible triad injury with a radial head fracture,
coronoid tip fracture, and elbow subluxation.
Incorrect Answers:
A 32-year-old soccer player presents with severe right ankle pain and inability to bear weight after sustaining a slide-tackle injury during a game. Radiographs are shown in Figures A and B. Given the nature of his injury, he is taken for surgical reduction and fixation. Following medial malleolar fixation, the syndesmosis is addressed. All of the following are true regarding the most appropriate intraoperative technique for anatomic syndesmotic reduction EXCEPT:

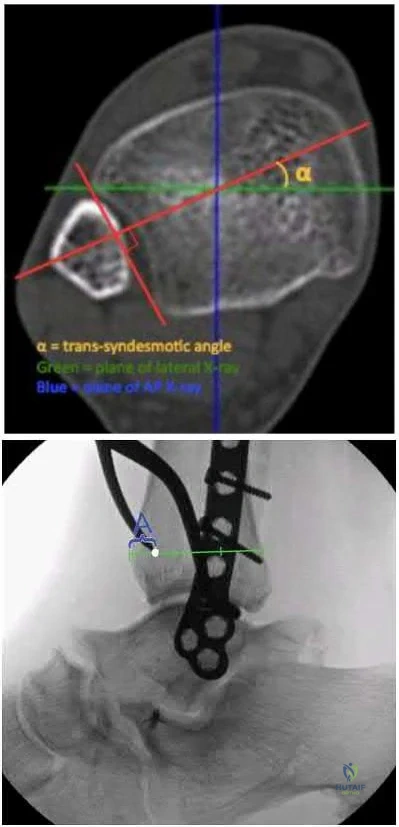
The axis of the reduction clamp should parallel the anatomic trans-syndesmotic angle
The lateral tine of the clamp should be seated just posterior to the lateral malleolar ridge
The medial tine should be placed on the anterior third of the tibia on a true lateral fluoroscopic view of the ankle
The reduction clamp should be placed 1-2cm proximal to the tibial plafond
The surgeon should apply judicious compression under fluoroscopic visualization to avoid over-compression of the syndesmosis
When placing a clamp across the syndesmosis to facilitate reduction, the lateral tine should be placed directly on the lateral malleolar ridge. Placing the lateral tine either more anteriorly or posteriorly has been shown to result in sagittal malreduction from fibular translation.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
A 45-year-old male injures his wrist during Live Action Role Play in Chicago two weeks ago. He underwent operative fixation by and presents to your clinic for his 2 week follow-up visit. You review his operative note in which the surgeon reports having to apply a volar
locking plate in a distal position to secure the difficult intra-articular fracture. The patient shows you the lateral film in Figure A. You remove his splint, he has no difficulty moving any fingers, very minimal pain, and is not taking any narcotic medication. How do you counsel him about his post-operative period?

The plate may need to removed once the fracture is healed to reduce the chance of flexor pollicis longus injury
The plate may need to removed once the fracture is healed to reduce the chance of flexor carpi radialis injury
The plate may need to removed once the fracture is healed to reduce the chance of flexor digitorum superficialis – index finger injury
The patient should undergo revision fixation as soon as possible
The plate is in appropriate position and will likely never need to be removed Correct answer: 1
This patient’s volar locking plate (VLP) is distal to the "watershed line", extending volarly beyond the most volar aspect of the distal radius. He is at greatest risk for an attritional rupture of the FPL.
A VLP placed this distal and volar is more likely to cause flexor tendon injury.
Up to 12% of all patients undergoing volar plate fixation will experience flexor tendon injury, and the FPL is the most common tendon associated with the VLP (57% of total flexor tendon ruptures). The average time from fixation to flexor tendon rupture has been cited at 9 months. To judge if a plate is volar to the watershed line, a plum line can be made in the proximal direction from the most volar edge of the distal radius. If a plate is volar to this (Soong) line, the patient is thought to be at a higher risk for flexor tendon injury. As a result, this patient should be followed closely and if pain with thumb flexion is present after 3 months, the surgeon should consider plate removal so long as the fracture is healed to reduce the chance of FPL rupture. Ruptured tendons require repair, grafting, or transfer with hardware removal.
Griffin and Chhabra comprehensively reviewed the risk factors and adverse events following VLP fixation of distal radius fractures, including flexor tendonitis and rupture. They found that risk factors for flexor tendon rupture following VLP fixation included plate placement distal to the watershed line and that PQ repair does not seem to affect flexor tendonitis.
Agnew et al. analyzed wrist MRIs to determine the relationship between the flexor tendons and the watershed line. They found that at 3mm proximal to the watershed line, the FPL and FDP to the index finger were 2.6 and 2.2mm anterior to the volar rim of the distal radius. The authors suggested that distally placed plates are incredibly close to the flexor tendons.
Chilelli et al. described 24 of 48 wrists which had VLP following distal radius fracture and went on to experiences loss of FPL flexion post-operatively. They found that FPL ROM generally returned after 52 days, however with an associated average loss of 11° in thumb IPJ ROM. The authors attribute this to stripping of FPL from the bone during the volar approach.
Soong et al. divided patients who underwent VLP fixation for distal radius fractures into three groups according to position of plate relative to a plum line extending proximally from the most volar and distal aspect of the distal radius: those with a VLP dorsal to the Soong line (grade 0), those with the VLP volar to the Soong line but proximal to the rim (grade 1), and those with a VLP volar to the Soong line and at or distal to rim (grade 2). Of the 73 cases reviewed, the authors reported three flexor tendon ruptures, two of which were grade 2 position. The authors concluded that both position of plate and type of plate were contributors to flexor tendon injury following VLP fixation.
Figure A is a lateral radiograph of the wrist demonstrating appropriate reduction and fixation but with the VLP volar to the "watershed" or Soong line.
Illustration A is a lateral radiograph with Soong's line drawn to show that this plate is too volar.
Incorrect Answers:

A 42-year-old construction worker sustains a crush injury to the hand at a job site. He has immediate pain and significant swelling, and is taken to the local emergency department for evaluation. Radiographs do not demonstrate any fracture or dislocation. On exam,
he experiences severe pain with passive motion at the metacarpal phalangeal joints and when the wrist is flexed and extended.
Otherwise he has intact sensation and appropriate capillary refill. What is the next best step in diagnosis or treatment?
Advanced imaging
Arterial Doppler
Admission for overnight observation
Surgical intervention
Pain control
This patient presents with compartment syndrome of the hand. A history and clinical exam are the best tools to identify the diagnosis, and the treatment consists of emergent fasciotomies.
Compartment syndrome of the hand may be secondary to trauma, burn, IV drug use, extravasation of IV fluids, or major limb revascularization. The diagnosis is usually made with pain out of proportion to exam, particularly with passive stretch of the digits. It is possible to have compartment syndrome without neurovascular changes (paresthesia, pallor, pulselessness), particularly earlier in the presentation. Compartment measurements may be obtained and are considered diagnostic with an absolute value greater than 30mmHg or when the compartment pressure is within 30mmHg of the patient's diastolic blood pressure. However pressure testing is not necessary in most cases, but may be particularly important in the patient who is obtunded, intubated, or who had a block, as the physical exam will be confounded. There are ten hand compartments: hypothenar, thenar, adductor pollicis, four dorsal interosseous, and three palmar interosseous; and emergent surgical release of all ten compartments is indicated.
Codding et al. comprehensively reviewed hand compartment syndrome. The authors identify the history and physical exam as the most critical aspect of the diagnosis. More specifically, they noted that pain with passive stretch of the MCPJ is the most sensitive clinical sign on physical exam. The authors conclude the short comings of the research on hand compartment syndrome, but note the potential morbidity of a missed diagnosis is so great that the threshold for surgical intervention should be very low.
Lipschitz et al. reviewed the measurement of compartment pressures in the hand. The authors discussed technical pearls including leveling the monitor at the level of the heart, using local analgesia on the skin only, inserting the needle perpendicular to the skin, and measuring all 10 hand compartments.
They noted that any measurement greater than 30mmHg or within 30mmHg of the diastolic blood pressure may be considered diagnostic.
Illustration A shows the standard incisions utilized to release all ten hand compartments. Incisions are generally placed directly overlaying the thenar musculature, hypothenar musculature, the carpal tunnel, and dorsally over the metacarpals. The radial and ulnar border of each metacarpal are incised through the dorsal incisions to release the interossei compartments.
Incorrect Answers:

A 60-year-old woman with a history of well-controlled diabetes and hypertension sustained a fall into a ditch yesterday and presents with persistent left ankle pain and deformity. The injury is closed, and the patient is neurovascularly intact. Injury films are shown in Figures A and B. An unsuccessful attempt at reduction in the emergency department with sedation was made. What is the cause of failure of closed reduction?

Subacute nature of fracture
Incarceration of the deltoid ligament
Incarceration of the fibula behind the posterolateral ridge of tibia
Entrapment of the flexor hallucis longus (FHL) tendon
Entrapment of the extensor digitorum brevis (EDB) Correct answer: 3
The patient has sustained a Bosworth fracture-dislocation, which is a fixed dislocation of the fractured fibula behind the posterolateral tibial ridge. These fractures are generally irreducible via a closed means and require open reduction.
The initial radiographs in this vignette reveal posterior subluxation of the talus and fibula without significant coronal plane deformity. This deformity should raise the suspicion of a Bosworth fracture-dislocation, especially if closed reduction is unsuccessful. Bosworth fracture-dislocations can often be associated with posterior malleolar fractures, specifically of the posterolateral rim of the distal tibia. These injuries often fail closed reduction, given the engagement of the fibula behind the posterolateral tibial ridge, and frequently require open reduction. In this situation, the most effective method to reduce the fracture is through a posterolateral approach. This is the same approach that can then be utilized for the fixation of the posterolateral fragment and fibula.
Delasotta et al. discussed a case presentation of a 24-year-old male with a Bosworth fracture-dislocation in which the anterior compartment musculature was interposed within the fracture site, impairing both closed and eventual open reduction of the injury. The authors go on to discuss how 3D CT reconstruction of the bone and soft tissues can aid in both the diagnosis and preoperative planning of such injuries. They also note that these injuries should be admitted for compartment and neurovascular checks and undergo urgent surgical treatment.
Gardner et al. performed a cadaveric study directly comparing fixation of posterior malleolar fractures to syndesmotic stabilization in a simulated stage IV pronation-external rotation injury. Compared with the intact specimens, the authors found that fixation of the posterior malleolus restored 70% of the native stiffness, but syndesmosis stabilization only restored 40%. The authors concluded that given the likely integrity of the posterior inferior tibiofibular ligament in the setting of posterior malleolar fractures, anatomic reduction and fixation may be more appropriate than syndesmotic stabilization and better suited to restore stability.
Switaj et al. retrospectively evaluated the incidence of posterior malleolar fractures and posterior pilon variants in a 270 patients with operatively treated ankle fractures. The authors noted a relative frequency of posterior malleolar fractures of 50% and that of the posterior pilon variants of 20% within the entire cohort. While they found no significant difference in frequency of posterior malleolar or posterior pilon variants with regard to either AO/OTA or Lauge-Hansen classification, patients with posterior pilon variants were significantly older.
Figure A and B show the AP and lateral views of an ankle revealing a lateral malleolar fracture with tibiotalar subluxation and posterior dislocation of the fibula with respect to the posterolateral ridge of the tibia, consistent with a
Bosworth fracture-dislocation.
Incorrect answers:
A 42-year-old male who works as a professional clown presents with severe ankle pain and gross deformity after tripping and falling over his props at a children’s birthday party. His radiograph is shown in Figure A. Following fixation of the medial and lateral malleolar fractures, the syndesmosis is assessed and is found to be persistently unstable. All of the following are true regarding posterior malleolar fixation EXCEPT:

Fixation of the posterior malleolus obviates the need for syndesmotic fixation in most cases
Fixation of the posterior malleolus remains biomechanically inferior to trans-articular syndesmotic fixation
Functional and radiographic outcomes following posterior malleolar fixation are at least equivalent if not superior to those following syndesmotic fixation
Non-anatomic fixation of the posterior malleolus will compromise syndesmotic fixation
The syndesmosis is often incompletely injured in the setting of a posterior malleolar fracture
Fixation of the posterior malleolus has been shown to be biomechanically superior to single-screw trans-articular syndesmotic fixation. Anatomic reduction and fixation will most often obviate the need for syndesmotic fixation, as the posterior inferior tibiofibular ligament (PITFL) is typically intact and attached to the fragment.
Posterior malleolar integrity is essential to ankle function and stability. The posterior malleolus not only contains the talus posteriorly but adds to articular congruity for tibiotalar load transfer and contributes to rotatory ankle stability through the PITFL. As a result, posterior malleolar fractures compromise these critical functions. Operative management is therefore aimed at containment of
the talus, restoration of articular congruity, reduction of the incisura, and restoring integrity to the syndesmosis. Functional and radiographic outcomes following posterior malleolar fixation have been shown to be at least equivalent to those following syndesmotic fixation.
Miller et al. compared the need for syndesmotic fixation in bi- and tri-malleolar ankle fractures following anatomic reduction and fixation in the prone position versus initial conservative management in the supine position. The authors found that fixation of the posterior malleolus obviated the need for syndesmotic fixation in 97.9% of cases, while nearly 25% of patients with no initial fixation required stabilization. They concluded that prone positioning and anatomic fixation of the posterior malleolus should be performed as this adequately restored syndesmotic stability in almost all cases.
Gardner et al. performed a radiographic evaluation of syndesmotic integrity in the setting of pronation-external rotation stage 4 ankle fractures with associated posterior malleolar fractures. Based on radiographs and MRI, no complete tears of the posterior-inferior tibiofibular ligament were evident. The fracture pattern was then simulated in cadavers, and posterior malleolar fixation restored 70% of the native stability while syndesmotic fixation alone restored only 40% of the native stability. The authors advocated for posterior malleolar fixation over syndesmotic stabilization.
Miller et al. prospectively compared the outcomes following posterior malleolar and syndesmotic fixation for unstable ankle fractures with partial syndesmotic injury. At a minimum one-year follow-up, the authors found that patients who had undergone open reduction with fixation of posterior malleolar fractures had no difference in outcomes as compared to those who underwent syndesmotic fixation. They concluded that not only was syndesmotic reduction maintained at final follow-up following posterior malleolar fixation, but that functional outcomes were at least equivalent to syndesmotic fixation.
Fitzpatrick et al. evaluated the impact of posterior malleolar fixation toward restoring syndesmotic stability in a cadaveric supination-external rotation stage 4 fracture model. The authors found that failure to fix or anatomically reduce posterior malleolar fragments resulted in non-anatomic translation of the fibula and ultimately in syndesmotic malreduction. They advocated for anatomic reduction and fixation of larger posterior malleolar fractures.
Figure A is an AP radiograph of the right ankle demonstrating a displaced trimalleolar ankle fracture with maintained relationship between the distal fibula and posterior malleolar fragment.
Incorrect Answers:
A 35-year-old morbidly obese female presents with global right ankle pain and significant swelling after a misstep over one of her cats on the stairs. She is unable to bear weight, but the skin is intact. Injury films are shown in Figures A through D. What is the internervous plane through which direct anatomic reduction and fixation of both fractures could best be achieved?



Question 56
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren’s contracture?
Explanation
REFERENCES: McGrouther D: Dupuytren’s contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone,
1999, vol 1, pp 565-569.
McFarlane R: Patterns of diseased fascia in the fingers in Dupuytren’s contracture.
Plast Reconstr Surg 1974;54:31-44.
Question 57
The quadrilateral space in the shoulder contains which of the following structures?
Explanation
REFERENCES: Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 61-62.
Question 58
A 32-year-old man has intense right hand and wrist pain, a deformed wrist, and numbness in his fingers after falling off his motorcycle. This is an isolated injury. Examination reveals a swollen wrist, normal capillary refill to all fingers, and limited flexion of all fingers. Radiographs are shown in Figures 21a and 21b. Neurologic examination of the hand will most likely reveal
Explanation
REFERENCES: Ruby LK, Cassidy C: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1297-1300.
Habernek H, Weinstabl R, Kdolsky R, et al: Volar lunate fracture-dislocations of the wrist: Case report for two patients treated with external frame and internal open reduction. J Trauma 1998;45:975-978.
Question 59
A 14-year-old boy is lifting weights and feels a sudden pain in his back, associated with sciatica bilaterally. The sciatica persists for several weeks. The radiograph shown in Figure 7a is negative, and the CT scan shown in Figure 7b is available for evaluation. An MRI scan is read as a disk bulge. Management should consist of
Explanation
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 694.
2010 Pediatric Orthopaedic Examination Answer Book • 13
Question 60
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Explanation
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 61
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
REFERENCES: Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Sammarco GJ: How I manage turf toe. Phys Sports Med 1988;16:113-118.
Question 62
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Bono JV, McCarthy JC, Thornhill TS, Bierbaum BE, Turner RH (eds): Revision Total Hip Arthroplasty. New York, NY, Springer Verlag, 1999, pp 530-592.
Question 63
Figures 4a and 4b are the radiographs of an isolated injury. What is the next most appropriate step in management?

Explanation
Question 64
In addition to lengthening the achilles, transfer of which tendon is important for functional ambulation after performing a Chopart amputation of the foot?

Explanation
Question 65
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. Which type of contraction of the involved muscle most likely resulted in this lineman's injury?
Explanation
followed by the ECU, EDQ, and, finally, the EIP.
Question 66
The structure that runs just beneath the peroneal tubercle of the calcaneus is the
Explanation
The peroneal tubercle is often a good landmark at which to identify the peroneus longus tendon surgically, and a hypertrophic tubercle has been associated with peroneus longus tendinopathy. Both peroneal tendons curve anteriorly around the tip of the fibula, with the peroneal tubercle separating the 2 tendons at the level of the calcaneus. The peroneus brevis runs in front of the tubercle and the longus behind. The flexor hallucis longus runs through a fibro-osseus tunnel posterior to the hindfoot formed by the posterolateral (os trigonum) and posteromedial tubercle of the talus. The calcaneal fibular ligament attaches to the calcaneus below the posterior facet of the subtalar joint and deep to the peroneal tendons.
RECOMMENDED READINGS
Hyer CF, Dawson JM, Philbin TM, Berlet GC, Lee TH. The peroneal tubercle: description, classification, and relevance to peroneus longus tendon pathology. Foot Ankle Int. 2005 Nov;26(11):947-50. Pub PMID: 16309609.View Abstract at PubMed
Bruce WD, Christofersen MR, Phillips DL. Stenosing tenosynovitis and impingement
of the peroneal tendons associated with hypertrophy of the peroneal tubercle. Foot Ankle Int. 1999 Jul;20(7):464-7. PubMed PMID: 10437932.View Abstract at PubMed
Question 67
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
REFERENCES: Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Petilon J, Carr DR, Sekiya JK, et al: Pectoralis major muscle injuries: Evaluation and management. J Am Acad Orthop Surg 2005;13:59-68.
Question 68
- A healed fracture of the tibia that demonstrates 25 degrees apex posterior angulation and 28 degrees varus angulation on AP and lateral radiographs is most accurately described as a
Explanation
Question 69
-What is the mechanism of action of tranexamic acid in controlling traumatic hemorrhage?
Explanation

Question 70
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 71
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use? Review Topic
Explanation
Question 72
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 73
A 4-year-old girl who is undergoing chemotherapy for acute lymphocytic leukemia sustains a displaced fracture through an osteolytic lesion in the metaphysis of the distal femur as a result of a fall. Treatment should include
Explanation
Question 74
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 75
A 45-year-old man reports that he awoke 2 weeks ago with severe pain in his right arm. Examination reveals weakness in the biceps, brachialis, and wrist extensors. There is decreased sensation in the thumb and index finger and a diminished brachioradialis reflex. Assuming this patient has a posterolateral herniated nucleus pulposus, what level is involved?
Explanation
REFERENCES: Standaert CJ: The patient history and physical examination: Cervical, thoracic and lumbar, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, vol 1, pp 171-186.
Bates B: A Guide to Physical Examination and History Taking, ed 5. Philadelphia, PA,
JB Lippincott, 1991.
Question 76
Which of the following methods of treating a vertically oriented (eg, Pauwels III) femoral neck fracture is mechanically optimal?
Explanation
(SBQ12TR.68) Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated non-operatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?

Hand dominance
Angulation of fracture
Smoking
Early physical therapy
Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with nonoperative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than nonsmokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Question 77
A 16-year-old female gymnast reports a 2-month history of back pain since falling off the parallel bars, and she has been unable to return to gymnastics. She has no numbness or tingling. Examination reveals lower back tenderness, some paravertebral muscle spasm, range of motion of the lumbosacral spine is 20 degrees of flexion and 20 degrees of extension, and an equivocal straight leg raise. Lumbosacral spine radiographs demonstrate Schomorl’s nodes but no evidence of spondylolisthesis. What is the next best step in management?
Explanation
REFERENCES: Katz DA, Scerpella TA: Anterior and middle column thoracolumbar spine injuries in young female gymnasts: Report of seven cases and review of the literature. Am J Sports Med 2003;31:611-616.
Tertti M, Paajanen H, Kujala UM, et al: Disc degeneration in young gymnasts: A magnetic resonance imaging study. Am J Sports Med 1990;18:206-208.
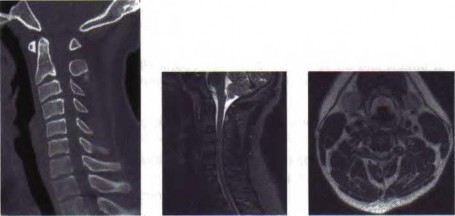
Question 78
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had
Explanation
Question 79
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 80
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?

Explanation
Question 81
A 67-year-old woman has persistent anterior thigh and knee pain after undergoing total knee arthroplasty 1 year ago. Examination and radiographs reveal no problems in the knee, mild hip flexor weakness (grade 4+), and decreased sensation over the anterior thigh including and proximal to the incision. MRI of the lumbar spine will most likely reveal which of the following findings?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 250.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 82
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
Explanation
REFERENCE: Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.
Question 83
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10° of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of
Explanation
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med
1998;26:520-530.
Jackson DW, Silvino N, Reiman P: Osteochondritis in the female gymnast’s elbow. Arthroscopy 1989;5:129-136.
Ruch DS, Cory JW, Poehling GG: The arthroscopic management of osteochondritis dissecans of the adolescent elbow. Arthroscopy 1998;14:797-803.
Question 84
below show the radiographs, and the CT obtained from a year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 85
-Radiographs are shown in Figures 89a through 89c. What is the most likely diagnosis?
Explanation
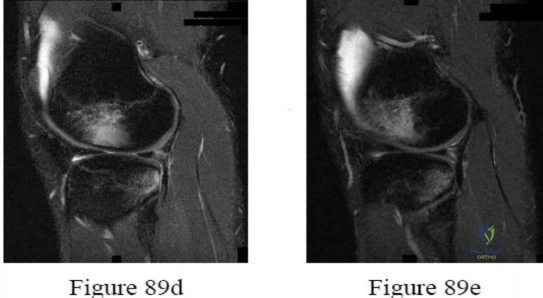
Question 86
Figure 35 is the MR image of an 18-year-old man who has had knee pain with running for 5 months. What is the most appropriate treatment?
Explanation
The MR image shows an osteochondritis dissecans (OCD), which is an acquired lesion of the subchondral bone. Patients with OCD initially report nonspecific pain and variable amounts of swelling. Initial radiographs help to identify the lesion and establish the physes status. MRI is useful for assessing potential for the lesion to heal with nonsurgical treatment. This lesion is unstable, considering the fluid line between the OCD and the underlying normal bone. Nonsurgical treatment is appropriate for small, stable lesions in patients with open physes and focuses on activity restriction for 3 to 9 months. Surgical treatment is necessary to address unstable or detached lesions. Stable lesions with intact articular cartilage can be treated with subchondral drilling to stimulate vascular ingrowth, with radiographic healing at an average of 4.4 months. Fixation is indicated for unstable or hinged lesions, and stabilization of the fragment can be achieved using a variety of implants through an arthroscopic or open approach. The fragment should be salvaged and the normal articular surface restored whenever possible.
Question 87
A 55-year-old man who runs on the weekends reports a 1-year history of continued pain directly posteriorly in the heel. Management consisting of anti-inflammatory drugs, icing techniques, a heel-counter in his shoe split, and physical therapy consisting of stretching, contrast baths, custom orthotics, and iontophoresis has failed to provide relief. Not only is his lifestyle disrupted with respect to running, but he now has pain with normal ambulation with all forms of shoe wear. He is not necessarily concerned with returning to running; he is primarily seeking pain relief. A lateral radiograph and clinical photograph are shown in Figures 32a and 32b. Treatment should now consist of
Explanation
REFERENCES: Clain M, Baxter D: Achilles tendinitis. Foot Ankle 1992;13:482-487.
Schepsis A, Wagner C, Leach R: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619.
Schepsis A, Leach R: Surgical management of Achilles tendinitis. Am J Sports Med 1987;15:308-315.
Keck S, Kelly P: Bursitis of the posterior part of the heel: Evaluation of surgical treatment of eighteen patients. J Bone Joint Surg Am 1965;47:267-273.
Question 88
03 A 26-year-old woman has chronic toe pain after hitting a bedpost 3 months ago. A radiograph is shown in Figure 27. Her injury represents an avulsion of the

Explanation
The EDB originates on the distal lateral and superior surface of the calcaneus and inserts on the
lateral aspect of the flexor digitorum longus tendon and also on to the base of the proximal phalanx of the first through fourth toes. There is no EDB tendon to the fifth toe. If an EDB laceration is easily identified at the time of an EDL repair, than it may be repaired as well, otherwise repair of the EDL alone is sufficient.
Heckman JD: Fractures and dislocation of the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds):Rockwood and Green’s Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 2166-2169.
Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 787-788.
back to this question next question
Question 89
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
REFERENCE: Ebraheim NA, Haman SP, Xu R, Stanescu S, Yeasting RA: The lumbosacral nerves in relation to dorsal SI screw placement and their locations on plain radiographs. Orthopedics 2000;23:245-247.
Question 90
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 91
In a pilon fracture, the Chaput fragment typically maintains soft tissue attachment via which of the following structures?

Explanation
Question 92
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
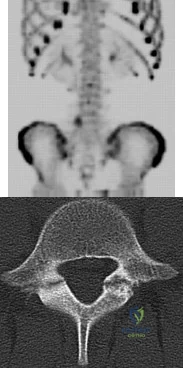
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 93
Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
Explanation
Question 94
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.
Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.
Question 95
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis?

Explanation
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 96
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. Assuming her workup is negative for any other causes, what is the best treatment option?

Explanation
Question 97
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?
Explanation
kyphosis and stenosis. Because he is healthy, has responded well to previous surgery,
|and has a potentially correctable lesion, he is not a good candidate for an end-stage failed
back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient’s relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
REFERENCE: Eck JC, Humphreys SC, Hodges SD: Adjacent-segment degeneration after lumbar fusion: A review of clinical, biomechanical, and radiographic studies. Am J Orthop 1999;28:336-340.
Question 98
A B Figures 60a and 60b are the postmyelography CT images of a 62-year-old man who has had low-back and bilateral lower-extremity pain. His pain began approximately 1 year ago and there was no precipitating event. The location of the pain is in the lower lumbar region in the midline and it radiates into the buttocks and thighs bilaterally. The pain is exacerbated by standing and walking and relieved by forward spine flexion. He reports no pain while sitting or lying supine. Upright radiographs demonstrate 4 mm of anterolisthesis of L4 on L5. What is the most appropriate surgical procedure?

Explanation
This patient radiographically has L4-5 degenerative stenosis and a low-grade spondylolisthesis. The axial images demonstrate a gap in the facet joint, more on the left than the right, which is highly suggestive of dynamic instability. Thus, this patient would most benefit from a laminectomy and fusion of L4-5. A microdiskectomy would not be helpful as this patient does not have a disk herniation. Patients undergoing posterior decompression alone experience an unacceptably high rate of recurrent stenosis and/or progression of spondylolisthesis. Early studies demonstrated that adding an intertransverse process fusion to posterior decompression significantly improved clinical outcomes. Anterior interbody fusion likely will not decompress the spinal canal sufficiently, though there is some thought that indirect decompression can be effective in some cases.
RECOMMENDED READINGS
Frymoyer JW. Degenerative Spondylolisthesis: Diagnosis and Treatment. J Am Acad Orthop Surg. 1994 Jan;2(1):9-15. PubMed PMID: 10708989. Majid K, Fischgrund JS. Degenerative lumbar spondylolisthesis: trends in management. J Am Acad Orthop Surg. 2008 Apr;16(4):208-15. Review. PubMed PMID: 18390483. View Abstract at PubMed
Carlisle E, Fischgrund JS. Lumbar spinal stenosis and degenerative spondylolisthesis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006: 299-317.
Puschak TJ, Sasso RC. Spondylolysis-spondylolisthesis. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:553-563.
Question 99
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 100
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis (musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii (musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis (musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis (musculocutaneous nerve)
