Orthopedic Surgery Board Review MCQs: Trauma, Hand, Ligament | Part 163

Key Takeaway
This page offers Part 163 of a comprehensive Orthopedic Surgery Board Review, featuring 100 high-yield MCQs by Dr. Hutaif. Designed for orthopedic residents and surgeons, it mirrors AAOS/OITE exam formats. It focuses on Fracture, Ligament, and Wrist topics, serving as a critical tool for board certification preparation.
About This Board Review Set
This is Part 163 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 163
This module focuses heavily on: Fracture, Ligament, Wrist.
Sample Questions from This Set
Sample Question 1: The thumb metacarpophalangeal (MCP) joint should be flexed to what degree to properly assess ligamentous stability?...
Sample Question 2: Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate tre...
Sample Question 3: A 64-year-old female sustains a nondisplaced distal radius fracture and undergoes closed treatment using a cast. Three months after the fracture she reports an acute loss of her ability to extend her thumb. What is the most likely etiology ...
Sample Question 4: An acetabular fracture with all segments of the articular surface detached from the intact posterior ilium is defined as what fracture pattern?...
Sample Question 5: Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The thumb metacarpophalangeal (MCP) joint should be flexed to what degree to properly assess ligamentous stability?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 339-358.
Stener B: Displacement of the ruptured ulnar collateral ligament of the MP joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1962;44:869-879.
33 • American Academy of Orthopaedic Surgeons
Question 2
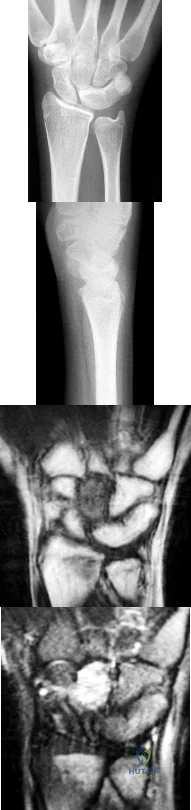
Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate treatment option?

Explanation
This patient sustained a lesser-arc perilunate dislocation. As a result of the injury, he also developed acute carpal tunnel syndrome. The closed reduction attempt was unsuccessful; therefore, this injury is best managed with emergent surgery, an open carpal tunnel release, an open reduction of the perilunate dislocation, scapholunate ligament repair, and intercarpal pinning. Outpatient surgery in a delayed fashion is not advised because of the acuity and severity of the carpal tunnel syndrome. Closed reduction and casting is not advised, because it commonly leads to continued carpal instability with subsequent dorsal
intercalated segment instability deformity and scaphoid lunate advanced collapse wrist arthritis.
Question 3
A 64-year-old female sustains a nondisplaced distal radius fracture and undergoes closed treatment using a cast. Three months after the fracture she reports an acute loss of her ability to extend her thumb. What is the most likely etiology of her new loss of function?

Explanation
Question 4
An acetabular fracture with all segments of the articular surface detached from the intact posterior ilium is defined as what fracture pattern?

Explanation
radiographic findings consistent with a both column acetabular fracture can be seen in Illustration A (AP), Illustration B (obturator oblique), and Illustration C (iliac oblique).
Question 5
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?
Explanation
REFERENCES: Levine AM, Edwards CC: Fractures of the atlas. J Bone Joint Surg Am 1991;73:680-691.
Kurz LT: Fractures of the first cervical vertebra, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 409-413.
Question 6
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 7
A 14-year-old gymnast presents after a fall from the balance beam with a hyperextension injury to her left knee. She could ambulate with pain but was unable to continue exercise due to pain. On examination she has a swollen knee with painful

Explanation
Tibial eminence fractures are rare but occur more often in pediatric populations, often in the setting of sports-related injuries. Debate continues over operative vs nonoperative treatment, as well as fixation type (screw vs suture) for openly treated fractures. Past evidence suggested closed treatment was adequate but there has been an increase in operative management. Closed treatment is suggested for minimally displaced fractures (Type I and reducible Type II) and open treatment for completely displaced fractures (non-reducible Type II and Type III).
Wilfinger et al provide the results of a closed reduction protocol at their institution including 38 patients with long term followup. All patients underwent aspiration and closed reduction in the OR under fluoroscopic guidance followed by long leg casting in hyperextension and graduated weight bearing over weeks. No patients complained of persistent pain, swelling, giving way, or disability at follow up.
However, Edmonds et al in a retrospective review compare open reduction internal fixation (ORIF), arthroscopic-assisted internal fixation (AAIF), and closed reduction with casting (CRC) for pediatric patients with displaced tibial spine fractures. They report improved reduction but also increased arthrofibrosis in ORIF and AAIF groups
compared to CRC, but of the 24% of patients with long term followup results, there was no difference in functional outcomes across all 3 groups. There was a 17% rate of later operation for the CRC group patients. They suggest closed treatment for fractures with <5mm displacement, otherwise ORIF or AAIF.
Gans et al conducted a systematic review focused on the questions of open vs closed reduction, and screw vs suture fixation. The 26-article review found insufficient evidence to have any clear recommendations. They did find reduced laxity and improved range of motion for minimally displaced fractures that had an open reduction, and that completely displaced fractures treated nonoperative had higher rates of nonunion.
Figures A and B are AP and lateral knee radiographs demonstrating a moderately displaced (Meyers and McKeever Type II) tibial spine fracture in a skeletally immature patient.
Incorrect Responses
Question 8
Figures 28a and 28b show the posteroanterior and lateral radiographs of a 38-year-old woman with adult idiopathic scoliosis. She reports symptoms of long-standing lower back pain, progressive loss of height, and the inability to stand upright at the end of the day. What radiographic finding has been found to most closely correlate with symptoms of lower back pain? Review Topic

Explanation
Question 9
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
Explanation
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
Question 10
A 22-year-old man sustained a cervical fracture-dislocation of the C5-6 level in a motor vehicle accident along with an associated spinal cord injury. Six months after his injury, he has 4 out of 5 biceps on the left, with 5 out of 5 biceps on the right. Deltoid is graded at 5 out of 5 bilaterally. There is 0 strength in the triceps, wrist flexors, wrist extensors, and digital extensors. He has neurogenic bowel and bladder with absent perianal sensation and no voluntary motor in the lower extremities. The patient's neurologic deficit is best categorized as which of the following? Review Topic
Explanation
Question 11
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
REFERENCES: Aiona MD: Guidelines for managing lower extremity problems in cerebral palsy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1534-1541.
Chambers H, Laure A, Kaufman K, Cardelia M, Sutherland D: Prediction of outcome after rectus femoris surgery in cerebral palsy: The role of cocontraction of the rectus femoris and vastus lateralis. J Pediatr Orthop 1998;18:703-711.
Ounpuu S, Muik E, Davis RB, Gage JR, Deluca PA: Rectus femoris surgery in children with cerebral palsy. J Pediatr Orthop 1993;13:331-335.
Question 12
On average, the radial nerve travels from the posterior compartment of the arm to the anterior compartment at which of the following sites?

Explanation
Question 13
Figures 28a and 28b are the MR images of a 30-year-old man who has right shoulder pain and difficulty throwing a football. His history includes a shoulder injury from a skiing accident 2 years ago. He has not had a recent shoulder injury. Which shoulder motion is most likely to demonstrate weakness?
Explanation
The MR images reveal a large paralabral cyst extending into the spinoglenoid notch. This cyst can be expected to compress the branch of the suprascapular nerve to the infraspinatus. Compression of this branch could lead to weakness in the infraspinatus, which would manifest as external rotation weakness. Shoulder abduction would be unaffected because the axillary and main suprascapular nerves would be intact. Shoulder internal rotation and adduction would be unaffected because the subscapularis and pectoralis would be unaffected.
Question 14
Figure 53 shows the MRI scan of a 53-year-old carnival worker who has pain and swelling in the left shoulder as a result of attempting to stop a roller coaster car with his arm. Examination reveals decreased ROM, apprehension, and inability to move the dorsum of his hand away from his back. Treatment should consist of
Explanation
Question 15
All of the following techniques can help to prevent valgus angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
A final technical trick is the usage of blocking (Poller) screws - the referenced article by Ricci et al had 100% correction and maintenance of reduction with usage of blocking screws without other adjunct techniques. These should be placed in the lateral aspect of the proximal and distal fragments when needed.
The referenced study by Krettek et al is a biomechanical evaluation of blocking screws in a tibial model that showed significantly increased strength when they were utilized.
Question 16
All of the following are advantages of supine over lateral positioning during intramedullary nailing of subtrochanteric femur fractures EXCEPT:

Explanation
Advantages of the supine position include: may help protect a potentially unstable spine, facilitates access to sites other than the injured femur, shorter setup time, rotational and angulatory deformities may be more easily appreciated. Disadvantages of the supine position include: starting point localization may be more difficult.
Question 17
-A 42-year-old woman has had right wrist pain for 2 years. She tried splint wear and naproxen and has had 3 steroid injections, each time experiencing less relief.
Explanation

Question 18
Radiographs shown in Figures 1 through 3 show two different prosthetic design variations of the same knee implant. When compared with the design of right knee prosthesis, the left can be expected to have a
Explanation
Question 19
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?
Explanation
REFERENCES: Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 255-264.
Question 20
Which of the following conditions precludes performing a tendon transfer?
Explanation
REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. St Louis, MO, Mosby, 2003, pp 1283-1287.
Coughlin MJ, Mann RA: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 786-861.
Question 21
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 22
A 64-year-old man with a history of metastatic lung cancer reports increasing right hip pain over the period of several months. Radiographs are shown in Figures 3a and 3b. Initial management should consist of
Explanation
REFERENCE: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 23
- Radiographs of the cervical spine of a 73-year-old man who fell down stairs reveal cervical spondylosis without evidence of fracture or dislocation. MRI and CT scans are consistent with the plain radiographs. After 72 hours, neurologic evaluation reveals intact sensation; however, weakness of the upper extremities is greater than that of the lower extremities. What is the most likely diagnosis?
Explanation
extremity deep pressure and proprioceptive preserved. 3-Posterior cord syndrome is rare with loss of deep pressure, deep pain, and proprioception. 4-Brown-Sequard syndrome-Uncommon-Ipsilateral motor deficit, contralateral pain and temperature deficit. 5-Cervical nerve root injury- functional impairment of the cervical spine. Symptoms are often acute and severe, dependent on the level of the lesion. An infraforaminal protrusion may compress only the spinal root ganglion resulting in severe brachialgia with paresthesia and numbness but with little or no motor involvement.
Question 24
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 25
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
Explanation
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
Question 26
Figures 12a and 12b show the radiographs of a 50-year-old patient who reports acute knee pain after sustaining a twisting injury while playing tennis. Examination is unremarkable. The next most appropriate step in management should consist of
Explanation
REFERENCES: Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby Inc, 1998, pp 1105-1107.
Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Hove E, Sury B: Melorheostosis: Report on 5 cases with follow-up. Acta Orthop Scand 1971;42:315-319.
Question 27
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 28
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 29
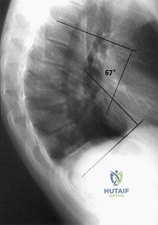
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of Review Topic
Explanation
Question 30
MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
Explanation
A. Pain with elbow extension in forearm pronation
B. Mechanical symptoms when rising from a chair
C. Valgus instability
D. Tenderness over the medial collateral ligament (MCL)
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
56- A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and 2. What is the most appropriate next step to restore this patient’s function?
Question 31
An 82-year-old man has had episodic right thigh pain after undergoing a total hip arthroplasty 10 years ago. Initial postoperative radiographs are shown in Figures 26a and 26b, and current radiographs are shown in Figures 26c and 26d. What is the most likely cause of his pain?
Explanation
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of biologic fixation of porous-surface femoral components. Clin Orthop Relat Res 1990;257:107-128.
Engh CA, Hooten JP, Zettl-Schaffer KF, et al: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Question 32
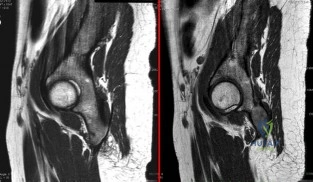
A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal images shown in Figure A (left, pre-operative; right, post-operative). Which of the following pre-operative physical examination findings may have been positive? Review Topic
Explanation
Snapping hip exists in 3 forms: (1) external snapping hip, which is caused by the iliotibial band (ITB) sliding over the greater trochanter, (2) internal snapping hip, and
(3) intraarticular snapping hip, which is caused by loose bodies (traumatic, or from synovial chondromatoses) or labral tears. While painless snapping hip requires no treatment, painful snapping hip may be addressed with activity modification, physical therapy, steroid injections. Surgical release (ITB z-plasty or psoas tenotomy) is indicated if nonoperative management is unsuccessful.
Ilizaliturri et al. evaluated the results of endoscopic iliopsoas tendon release at the lesser trochanter (10 patients) vs endoscopic transcapsular psoas release from the peripheral compartment (9 patients). There were improvements in WOMAC scores in both groups, and no difference between groups. They conclude that both techniques are equally effective.
Marquez Arabia et al. evaluated if the psoas tendon regenerates after tenotomy in 27 patients. At 23 months, they found that tendon regeneration occurred in all patients, to
a mean circumference of 84% of the original. One patient had persistent pain, but all had 5/5 hip flexion strength. They hypothesize that the bulk of iliopsoas muscle fibers attaches directly to the proximal femoral shaft without a tendon, preventing retraction and allowing regeneration to occur easily.
Figure A shows pre- and post-operative arthroscopic psoas tenotomy magnetic resonance sagittal images. Illustration A shows the psoas tendon (white arrows) prior to transection. Illustration B shows the psoas tendon after transection (green arrows, proximal tendon segment; yellow arrows, distal segment). Illustration C and D are diagrams showing release at the level of the lesser trochanter and hip joint respectively.
Incorrect
90 degrees, but full external rotation. Answer 2: Decreased internal rotation and a positive impingement test (forced
flexion, adduction, femoroacetabular Answer 4: These
and internal
rotation) are classic findings
findings may
be found with intra-articular
for cam-type impingement loose bodies.
Question 33
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 34
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?
Explanation
REFERENCES: Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Richards BS: Delayed infections following posterior spinal instrumentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995;77:524-529.
Question 35
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
Explanation
REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.
Question 36
A 47-year-old, healthy, active patient presents with a sub-acute, full-thickness supraspinatus tear. His physical examination reveals significant weakness and pain with abduction. There was no glenohumeral instability. Radiographs demonstrate a type 1 acromion. An MRI scan shows a crescent shaped tear with 2-cm of tendinous retraction and no tendinous fatty changes. A subacromial corticosteroid injection 6 weeks ago provided him with 24 hours of pain relief but no improvement in strength. What would be the most appropriate treatment option? Review Topic QID:4501
Explanation
The primary purpose of rotator cuff repair is to restore muscle function. Secondary outcomes include reduction of pain and prevention of irreversible cuff changes, specifically muscular atrophy. Non-operative treatment (exercise, therapy and pain medications) are recommended for partial thickness tears. The indication of surgical repair includes, isolated supraspinatus weakness +/- pain that correlates with MRI imaging of a respective full thickness tear. Routine acrominoplasty is not recommended in conjunction with rotator cuff repair, especially with no previous symptoms of impingement.
Pedowitz et al. developed clinical practice guidelines for the treatment of rotator cuff pathology. The strongest supporting evidence in current literature was given a grade of 'moderate' with four treatment recommendations. These were,
Exercise and non-steroidal anti-inflammatory drugs can be used to manage partial thickness tears,
Routine acromioplasty is not required the time of cuff repair,
Non-cross-linked, porcine small intestine submucosal xenograft patches should not be used to manage cuff tears, and
Surgeons can advise patients that workers' compensation status correlates with a less favorable outcome after rotator cuff surgery.
Illustration A shows the different shapes of rotator cuff tears. Incorrect Answers:
Question 37
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of Review Topic
Explanation
or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated.
Question 38
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a
Explanation
flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb.
REFERENCES: Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Lister GD: Skin flaps, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1741.
Question 39
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
REFERENCES: Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 40
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 41
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
REFERENCES: Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am 1999;81:649-659.
Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report on the incidence and prognosis. J Pediatr Orthop 1984;4:689-692.
Question 42
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 43
Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
Explanation
REFERENCES: Tile M: Assessment and management of acetabular fractures, in Tile M (ed): Pelvic and Acetabular Fractures, ed 2. Baltimore, MD, Williams and Wilkins, 1995, pp 305-354.
Letournel E: Acetabular fractures: Classification and management. Clin Orthop 1980;151:81-106.
Letournel E, Judet R: Fractures of the Acetabular, ed 2. Berlin, Springer-Verlag, 1993, pp 29-49.
Question 44
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286, 339-365.
Question 45
Biomechanical in vitro studies of double-row anchor fixation of rotator cuff tears show what initial advantage over single-row anchor fixation? Review Topic
Explanation
Question 46
A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?
Explanation
flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant.
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Fehring TK, Odum S, Griffin WL, et al: Early failures in total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 47
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?
Explanation
REFERENCES: Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398.
McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Schock HJ, Pinzur M, Manion L, et al: The use of the gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg Br 2007;89:1055-1059.
Question 48
The nerve to the abductor digiti quinti, implicated in some patients who have chronic heel pain, is most commonly a branch of what larger nerve?
Explanation
REFERENCES: Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
Schon LC, Glennon TP, Baxter DE: Heel pain syndrome: Electrodiagnostic support for nerve entrapment. Foot Ankle 1993;14:129-135.
Question 49
A B Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?

Explanation
The indications for surgery in a Charcot joint are an unbraceable deformity or recurrent ulceration despite use of adequate bracing. Any significant varus/valgus deformity of the ankle or hindfoot (as in this patient) is unbraceable, whereas midfoot Charcot deformities usually can be treated nonsurgically. The goal of surgery is to provide a stable aligned foot and ankle to permit activities and reduce risk for recurrent ulceration. This does not mean that there has to be a radiographic fusion because many patients with diabetes achieve a stable nonunion without pain. The only surgical construct that will provide long-term inherent stability and alignment in this situation is use of a hindfoot fusion rod. It provides better stability and purchase than screw fixation and can be left in indefinitely (unlike an external fixator).
RECOMMENDED READINGS
Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. View Abstract at PubMed
Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. View Abstract at PubMed Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87

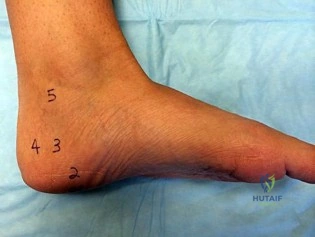
Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
Question 50
A 38-year-old man sustains a terrible triad injury consisting of an elbow dislocation, comminuted and displaced radial head fracture, and a type I coronoid fracture. Intraoperative findings after radial head replacement and lateral collateral ligament complex repair reveal persistent instability consisting of medial opening on valgus stress and posteromedial subluxation of the ulnohumeral and radiocapitellar joints. What is the best next step?
Explanation
normally correct the medial instability. Articulated versus static external fixation can be considered if
restoration of the ligamentous constraint of the medial side of the elbow cannot be accomplished surgically.
Question 51
A 27-year-old man has recurrent right shoulder instability. He first dislocated his shoulder in college while playing rugby and was treated nonsurgically. Since then, he has sustained nearly 1 dozen dislocations and says that his shoulder always feels “loose.” The shoulder recently dislocated in his sleep and while he was putting on clothes. Which factor is a contraindication to an arthroscopic soft-tissue repair?
Explanation
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Although some studies suggest that open stabilization may result in lower recurrence rates in contact athletes, this approach is now under scrutiny. Extensive labral involvement (posterior labral involvement in this scenario) is likely more accessible via arthroscopic methods. Although HAGL lesions may be more easily accessible via an open approach (particularly for inexperienced arthroscopists), numerous authors describe successful repair via arthroscopic techniques. Among these responses, the strongest indication for an open approach, including possible bony transfer, is high-grade glenoid bone loss. Although the critical amount of bone loss is a topic of debate, most surgeons and authors suggest a cutoff of 20% to 25%.

CLINICAL SITUATION FOR QUESTIONS 90 THROUGH 92
Figure 90 is the radiograph of a 14-year-old pitcher who plays in a year-round baseball program and has vague pain in his dominant shoulder. The pain occurs with throwing, and it has been worsening for 2 months. Pain typically occurs during the late cocking phase of throwing. He has no tenderness of the rotator cuff and 5/5 rotator cuff strength. His arc of motion is symmetric between his dominant and nondominant arms. The sulcus sign is negative.
Question 52
Figure 45 shows the current radiograph of an 11-year-old girl who sustained a simple nondisplaced fracture of the distal radius 4 weeks ago. Management at the time of injury consisted of application of a short arm cast but no manipulation. What is the major concern at this time?
Explanation
REFERENCES: Peterson HA: Physeal fractures: Part 2. Two previously unclassified types. J Pediatr Orthop 1994;14:431-438.
Peterson HA: Physeal and apophyseal injuries, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 108-109.
Question 53
A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports groin pain. What is the next most appropriate step in management?
Explanation
obtaining a dedicated AP radiograph of the hip with the leg internally rotated 15 to 20 degrees. Because the femoral neck is anteverted, 15 to 20 degrees of internal rotation of the hip offers the best view of the femoral neck. Whereas associated lumbar spine pathology may cause groin pain, the presence of a missed femoral neck fracture must first be ruled out prior to investigating other sources of pain.
Question 54
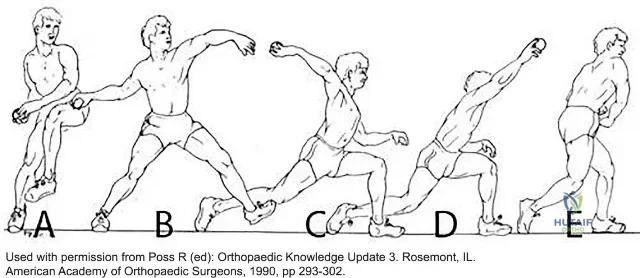
A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Question 55
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Davis AM, O’Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 56
5 degrees medial and 10 degrees cephalad
Explanation
Question 57
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
Explanation
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
Question 58
A 32-year-old woman with systemic lupus erythematosus treated with methotrexate and oral corticosteroids reports right groin pain with ambulation and night pain. Examination reveals pain with internal and external rotation and flexion that is limited to 105 degrees because of discomfort. Laboratory studies show a serum WBC of 9.0/mm 3 and an erythrocyte sedimentation rate of 35 mm/h. Figures 5a and 5b show AP and lateral radiographs of the right hip. Further evaluation should include
Explanation
REFERENCES: Mont MA, Jones LC, Sotereanos DG, Amstutz HC, Hungerford DS: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect
2000;49:169-185.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont , IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 59
What anatomic site is considered at highest risk for pathologic fracture?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1055.
Question 60
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
Explanation
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
distal femoral varus osteotomy.
osteoarticular transplant to the lateral femoral condyle.
unicondylar arthroplasty.
high tibial osteotomy.
Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
Question 61
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Easley ME, Trnka HJ, Schon LC, Myerson MS: Isolated subtalar arthrodesis. J Bone Joint Surg Am 2000;82:613-624.
Question 62
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
REFERENCES: Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Garfin SR, Botte MJ, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1987;69:954.
Question 63
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 64
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
Explanation
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
Question 65
A 35-year-old man reports a 2-year history of right groin pain. The pain is made worse with hip flexion, prolonged sitting, and cycling. A radiograph and MRI scan are shown in Figures 16a and 16b. Nonsurgical management has failed to provide relief. What is the best surgical option?
Explanation
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Question 66
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 67
Figure 71 is the MRI scan of a 2-year-old girl who has been febrile for 1 week and has refused to bear weight on her left lower extremity for 3 days. Her entire left lower extremity is markedly swollen. Doppler ultrasound shows a deep venous thrombosis of the internal iliac vein. Her white blood cell count is 19000/ µL (reference range, 4500-11000/ µL) and her C-reactive protein level is higher than 20 mg/L (reference range, 0.08-3.1 mg/L). If blood cultures yield positive results, what is the most likely organism? Review Topic

Explanation
Question 68
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 69
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
REFERENCES: Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop 2001;390:17-30.
Question 70
03 5.
Explanation
The radiograph here shows the typical Paget’s lesion in the right iliac wing with mixed lytic and sclerotic areas.
Question 71
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 72
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.
Question 73
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Explanation
Question 74
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 75
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 76
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.
Munshi M, Pretterklieber ML, Chung CB, et al: Anterior bundle of ulnar collateral ligament: Evaluation of anatomic relationships by using MR imaging, MR arthrography, and gross anatomic and histologic analysis. Radiology 2004;231:797-803.
Question 77
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?
Explanation
REFERENCE: Mink JH: Tendons, in Deutsch AL, Mink JH, Kerr R (eds): MRI of the Foot and Ankle. New York, NY, Raven Press, 1992, pp 135-172.
Question 78
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 79
Which of the following is most important to acheive a good outcome following a Syme amputation?

Explanation
Question 80
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?
Explanation
REFERENCES: Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby Year Book, 1995, p 688.
Question 81
Surgical treatment of an adult cavovarus foot with fixed forefoot valgus that does not correct on Coleman block testing should consist of Review Topic
Explanation
Question 82
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 83
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet. You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have?

Explanation
Question 84
Intradiskal electrothermal therapy (IDET) uses an intradiskal catheter to deliver controlled thermal energy to the inner periphery of the annulus fibrosis of a chronically painful intervertebral disk. Lumbar diskography is used diagnostically to identify the presumed pain generator to be targeted with IDET. Based on the medical literature, what can be said about the current status of IDET?
Explanation
REFERENCES: Freeman BJ, Fraser RD, Cain CM, et al: A randomized, double-blind, controlled trial: Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 2005;30:2369-2377.
Pauza KJ, Howell S, Dreyfuss P, et al: A randomized, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 2004;4:27-35.
Wetzel FT, McNally TA: Treatment of chronic discogenic low back pain with intradiskal electrothermal therapy. J Am Acad Orthop Surg 2003;11:6-11.
Question 85
Massive cortical structural allografts are commonly used in oncologic and arthroplasty surgery. What percent of cortical structural allografts fracture due to insufficiency?
Explanation
Question 86
An awake and alert patient with neck pain arrives at the emergency department after an automobile crash. Upon examination he is weak in the left deltoid and biceps muscles (3/5 strength). CT scans performed 2 hours after admission are shown in Figures 70a and 70b. His weakness deteriorates to 1/5 strength in the upper and lower extremities. What is the most appropriate treatment? A B

Explanation
Facet subluxation reduction may be performed in awake patients. Posterior spinal laminectomy and fusion can result in worsening neurologic status and is not recommended in this setting. Generally, corpectomy in the setting of facet subluxation is not recommended because it does not facilitate reduction or fully alleviate spinal cord compression. High-dose steroid use is not supported by current literature.
RECOMMENDED READINGS
Fehlings MG, Perrin RG. The timing of surgical intervention in the treatment of spinal cord injury: a systematic review of recent clinical evidence. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S28-35; discussion S36. Review. PubMed PMID: 16685233. View Abstract at PubMed
Lee AS, MacLean JC, Newton DA. Rapid traction for reduction of cervical spine dislocations. J Bone Joint Surg Br. 1994 May;76(3):352-6. PubMed PMID: 8175833.View Abstract at PubMed
Question 87
A 42-year-old woman who observes traditional Muslim practices is seen in your office accompanied by her physician husband to discuss possible elective bunion correction. In considering the treatment of this patient, what is one of the most important considerations?
Explanation
REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 88
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?
Explanation
REFERENCE: Gerber C, Myer DC, Schneeberger AG, et al: Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J Bone Joint Surg Am 2004;86:1973-1982.
Question 89
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 90
A 63-year-old woman who sustained a distal radial fracture 2 months ago now reports that she is unable to achieve active extension of the thumb at the interphalangeal joint. What type of trauma may lead to this clinical finding?
Explanation
REFERENCES: Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles’ type of fracture. Hand 1982;14:41-47.
Hirasawa Y, Katsumi Y, Akiyoshi T, et al: Clinical and microangiographic studies on the rupture of the EPL tendon after distal radial fractures. J Hand Surg Br 1990;15:51-57.
Question 91
A 7-year-old boy sustained a 2-cm laceration to the anterior aspect of his left knee after falling on a rock. Examination reveals that the joint surface is not visible through the wound. Radiographs show no evidence of a foreign body or free air in the joint. Management should consist of
Explanation
REFERENCES: Voit GA, Irvine G, Beals RK: Saline load test for penetration of periarticular lacerations. J Bone Joint Surg Br 1996;78:732-733.
Leffers D: Dislocations and soft tissue injuries of the knee, in Browner BD (ed): Skeletal Trauma, ed 1. Philadelphia, PA, WB Saunders, 1992, pp 1717-1743.
Question 92
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Explanation
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. View Abstract at PubMed
Question 93
A B Figures 60a and 60b are the postmyelography CT images of a 62-year-old man who has had low-back and bilateral lower-extremity pain. His pain began approximately 1 year ago and there was no precipitating event. The location of the pain is in the lower lumbar region in the midline and it radiates into the buttocks and thighs bilaterally. The pain is exacerbated by standing and walking and relieved by forward spine flexion. He reports no pain while sitting or lying supine. Upright radiographs demonstrate 4 mm of anterolisthesis of L4 on L5. What is the most appropriate surgical procedure?

Explanation
This patient radiographically has L4-5 degenerative stenosis and a low-grade spondylolisthesis. The axial images demonstrate a gap in the facet joint, more on the left than the right, which is highly suggestive of dynamic instability. Thus, this patient would most benefit from a laminectomy and fusion of L4-5. A microdiskectomy would not be helpful as this patient does not have a disk herniation. Patients undergoing posterior decompression alone experience an unacceptably high rate of recurrent stenosis and/or progression of spondylolisthesis. Early studies demonstrated that adding an intertransverse process fusion to posterior decompression significantly improved clinical outcomes. Anterior interbody fusion likely will not decompress the spinal canal sufficiently, though there is some thought that indirect decompression can be effective in some cases.
RECOMMENDED READINGS
Frymoyer JW. Degenerative Spondylolisthesis: Diagnosis and Treatment. J Am Acad Orthop Surg. 1994 Jan;2(1):9-15. PubMed PMID: 10708989. Majid K, Fischgrund JS. Degenerative lumbar spondylolisthesis: trends in management. J Am Acad Orthop Surg. 2008 Apr;16(4):208-15. Review. PubMed PMID: 18390483. View Abstract at PubMed
Carlisle E, Fischgrund JS. Lumbar spinal stenosis and degenerative spondylolisthesis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006: 299-317.
Puschak TJ, Sasso RC. Spondylolysis-spondylolisthesis. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:553-563.
Question 94
During shoulder motion with the elbow controlled in a brace, electromyographic studies of the supraspinatus show significant activity with all range-of-motion testing. Concurrent electromyographic studies of the long head of the biceps will most likely show
Explanation
REFERENCES: Yamaguchi K, Riew KD, Galutz LM, et al: Biceps activity during shoulder motion: An electromyographic analysis. Clin Orthop 1997;336:122-129.
Levy AS, Kelly BT, Lintner SA, et al: Function of the long head of the biceps at the shoulder: Electromyographic analysis. J Shoulder Elbow Surg 2001;10:250-255.
Question 95
A 17-year-old male lacrosse player sustains an ACL tear. Imaging reveals closed physes and you recommend a transphyseal ACL reconstruction. His mother asks whether a “cadaver tendon” can be used to reconstruct his ACL instead of using his own tendon. What is the most appropriate response regarding the use of allograft compared to autograft for ACL reconstruction in an active adolescent? Review Topic
Explanation
The incidence of anterior cruciate ligament (ACL) injuries in adolescent athletes has significantly increased over the recent years, now comprising 24.5% of all ligamentous knee injuries in high school athletes. In skeletally mature adolescents, transphyseal ACLR is often performed, similar to adult patients. Proposed advantages of allograft reconstruction in patients of all ages include lack of donor-site morbidity, absence of size limitation, preservation of knee flexor/extensor mechanism, less risk of postoperative knee stiffness/pain and cosmetic appearance. Benefits of autografts include strong structural and fixation properties as well as optimal biologic incorporation.
Kraeutler et al. performed a meta-analysis comparing bone-patellar tendon-bone (BPTB) autograft to allograft for ACLR. Patients who underwent ACLR with BPTB autograft demonstrated lower rates of graft rupture, lower levels of knee laxity, improved single-legged hop test results and were more satisfied postoperatively compared to ACLR with BPTB allograft. The authors therefore recommended BPTB
autograft
ACLR,
particularly
in
young
active
patients.
Engelman et al. performed a case-control study comparing ACLR in an adolescent cohort using autograft or allograft. Postoperative knee laxity and use of allograft were significantly related to graft failure and need for revision surgery. There was no difference in functional outcome scores, knee range of motion, infection or growth disturbance. There was no difference in graft survival between low-dose (<2 Mrad) gamma-irradiated allografts and nonirradiated allografts.
Pallis et al reported a prospective cohort study of 122 ACLR performed in cadets prior to matriculation at the United States Military Academy (USMA). Cadets who entered the USMA with an allograft ACLR were 7.7 times more likely to experience graft failure compared to BPTB and hamstring (HS) autograft groups. There was no significant difference in failure between the BPTB and HS autograft groups. The authors recommend autograft ACLR for young, active individuals.
Incorrect
Responses:
Question 96
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Ackland HM, Cooper DJ, Malham GM, et al: Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine 2007;32:423-428.
Hewitt S: Skin necrosis caused by semi-rigid cervical collar in a ventilated patient with multiple injuries. Injury 1994;25:323-324.
Question 97
The mother of a healthy 8-month-old boy reports that her son refuses to use his left arm. Examination reveals that the arm hangs limp at his side in an adducted and internally rotated position, and the affected shoulder subluxates posteriorly. Passive external rotation measures 15 degrees. Management should consist of
Explanation
REFERENCES: Neer CS: Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990,
pp 452-454.
Pearl ML: Arthroscopy release of shoulder contracture secondary to birth palsy: An early report on findings and surgical technique. Arthroscopy 2003;19:577-582.
Pearl ML, Edgerton BW, Kon DS, et al: Comparison of arthroscopic findings with MRI and arthrography in children with GH deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 2003;85:890-898.
Question 98
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
at risk.
REFERENCES: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 281-289.
Question 99
A 78-year-old man is seen in the emergency room 3 hours after a fall from a standing position. The patient sustained a mild scalp laceration and the injury shown in Figure 90. He reports severe neck pain and is unable to move his hands and legs. Examination reveals absent motor function in the wrist flexors, triceps, and fingers. He cannot move his lower extremities during motor testing. The patient has some sensation in the lower extremities. Bulbocavernosus reflex is absent. Based on examination findings and the imaging findings, what is the most definitive treatment option? Review Topic
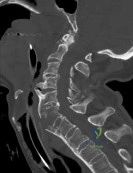
Explanation
(SBQ13PE.22) A 11-year-old male is referred for evaluation of scoliosis by his primary care physician. He has a normal birth and development history and denies any neurologic deficits or pain. On physical examination, he is neurologically intact with normal reflexes and tone. A PA radiograph is shown in Figure A. What is the next best step? Review Topic

Custom orthosis prescription to initiate bracing
Physical therapy referral and observation
Bending and lumbar oblique radiographs
Total spine CT
Total spine MRI
A left thoracic curve is an abnormal finding and warrants further work-up with a total axis MRI in order to rule out concomitant neurologic abnormalities such as a spinal cord cyst and/or syrinx.
In adolescent idiopathic scoliosis (AIS), the most commonly occurring curve is a right thoracic curve. Left thoracic curves are not as common, and warrants total axis MRI in order to rule out concomitant central axis abnormalities. This is imperative not only during initial work-up, but most importantly for operative planning.
Spiegel et al. performed a a retrospective radiographic review on 41 patients with scoliosis associated with a Chiari I malformation and/or syringomyelia. Approximately 50% of patients had an "atypical" pattern (left thoracic, double thoracic, triple, long right thoracic). The authors recommend that MRI should be considered in these patients.
Gillingham et al. provides a thorough review of early onset scoliosis and notes the relatively high incidence of concurrent central axis abnormalities, even in patients with normal neurologic exams. Rates have been reported upwards of 21.7%, with malformations including Chiari Type 1, dural ectasias, syrinx, and spinal cord cysts.
Figure A exhibits a left thoracic curve. Further imaging in this patient revealed a syrinx which required decompression.
Incorrect answers:
thoracic
curve.
Question 100
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
