OITE & ABOS Orthopedic Board Exam MCQs: Shoulder, Elbow, Trauma & Fractures - Part 2

Key Takeaway
This interactive quiz offers 100 verified, high-yield MCQs for orthopedic surgeons and residents preparing for OITE/AAOS/ABOS board certification. Mimicking exam format, it provides detailed explanations. Practice in Study or Exam Mode to master essential topics, ensuring comprehensive board exam preparation.
About This Board Review Set
This is Part 2 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 2
This module focuses heavily on: Elbow, Fracture, Shoulder, Trauma.
Sample Questions from This Set
Sample Question 1: Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the...
Sample Question 2: A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform...
Sample Question 3: A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?...
Sample Question 4: Figure 23 is the radiograph of a 22-year-old woman who was involved in a motor vehicle collision. She reports isolated pain in her left shoulder. She is hemodynamically stable, respiring comfortably, and neurovascularly intact. Based on the...
Sample Question 5: A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Steinmann SP, King GJ, Savoie FH III, et al: Arthroscopic treatment of the arthritic elbow.
J Bone Joint Surg Am 2005;87:2114-2121.
Question 2
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 3
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.
Question 4
Figure 23 is the radiograph of a 22-year-old woman who was involved in a motor vehicle collision. She reports isolated pain in her left shoulder. She is hemodynamically stable, respiring comfortably, and neurovascularly intact. Based on these findings, which of the following statements regarding treatment is most appropriate?

Explanation
Question 5
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches
Explanation
REFERENCES: Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000.
Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Gilliland MD, Ward RE, Barton RM, et al: Factors affecting mortality in pelvic fractures.
J Trauma 1982;22:691-693.
Question 6
What vessel is marked with an asterisk in Figure 44?
Explanation
REFERENCES: Agur AM, Dalley AF (eds): Grant’s Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Uflacker R: Atlas of Vascular Anatomy: An Angiographic Approach, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006.
Question 7
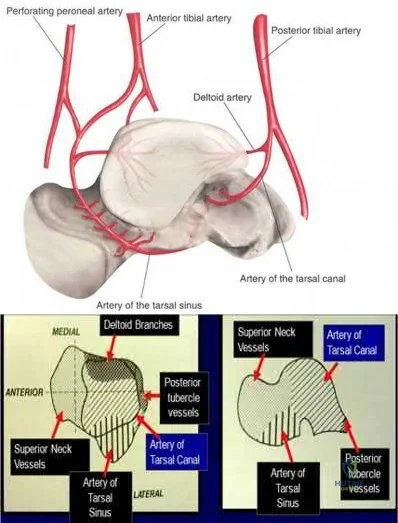
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?

Explanation
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
OrthoCash 2020
Question 8
Which treatment of the current fracture will provide the best long-term outcome?
Explanation
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
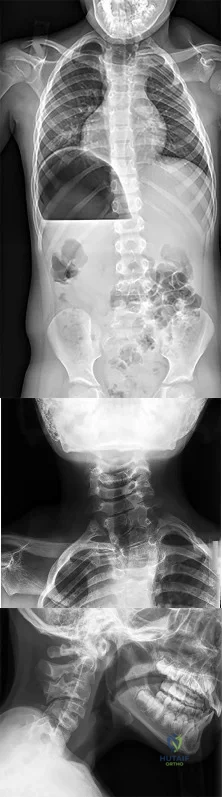
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
Question 9
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Loebenberg MI, Cuomo F: The treatment of chronic anterior and posterior dislocations of the glenohumeral joint and associated articular surface defects. Orthop Clin North Am 2000;31:23-24.
Question 10
Which of the following growth factors binds and activates the lipoprotein receptor-related protein 5/6 (LRP5/6) during bone development? Review Topic
Explanation
Question 11
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 12
What is the primary mechanism by which anabolic steroids increase muscle tissue? Review Topic
Explanation
Question 13
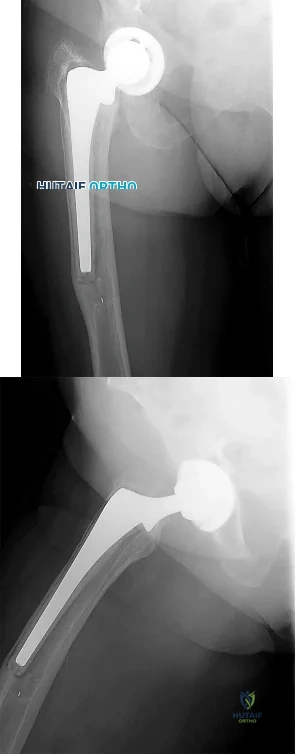
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 14
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of
Explanation
(greater than 50%) for treating MDI.
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896.
Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am
2000;82:919-928.
Miniaci A, Birnie J: Thermal capsular shrinkage for treatment of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003;85:2283-2287.
Question 15
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment? Review Topic

Explanation
option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform.
Question 16
This reporting avoids a ceiling and floor effect, where most of the respondents score either at the top or the bottom of the assessment scale.
Explanation
The only accurate statement is that, at 1 month, patients in group 3 are more likely to live longer than patients in group 1 and 2.
The Kaplan-Meier curve is a statistical method used in survivorship analysis to estimate survival rates at different time points. The horizontal axis depicts the time points and the vertical axis depicts the probability of survival. At a given time point, greater survivorship is demonstrated by higher values on the vertical axis.
Kocher et al. reviewed clinical epidemiology and biostatistics relevant in orthopaedic
surgery. They reported that survivorship data are typically analyzed with use of the Kaplan-Meier method. This analysis is used when the actual date of the end point is known. A survivorship curve can be plotted to illustrate the percentage of patients still alive after the intervention.
Petrie et al. reviewed statistics, terminology and the principles involved in simple data analysis, and outlines areas of medical statistics that have gained
prominence in recent years in orthopaedic papers. The authors provide an insight into some of the more common errors that occur in published orthopaedic journals and which are frequently encountered at the review stage in papers submitted to the Journal of Bone and Joint Surgery.
Figure A depicts a Kaplan-Meier curve for 3 groups of patients undergoing 3 different interventions.
Incorrect Answers:
When evaluating patient-reported outcomes in spine surgery, the Patient- Reported Outcomes Measurement Information System (PROMIS) has been found to have what differences compared to other assessment tools?
Communication failures have been associated with increased treatment costs, increased complications, and delays in patient care.
The leading cause of medical errors, wrong-site surgeries, diagnostic delays and loss to follow-up is attributed to communication errors. Studies have shown that this directly leads to increased complications, increased treatment costs, and delays in patient care. In the surgical setting, the performance of the pre-surgical time-out affords clarification of the treatment plan, confirmation of the procedure and site, and an opportunity for the team to address any concerns.
Weller et al. reviewed barriers to effective teamwork in healthcare delivery. They found that effective communication across all team members, inclusive training, and the creation of democratic teams can reduce treatment delays and minimize complications. They concluded that all team members should have a shared understanding of the situation when involved in patients care.
Lingard et al. performed a prospective study determining the feasibility of a preoperative 10-item checklist discussion including nurses, surgeons, and anesthesiologists. They reported that the discussion usually took place prior to bringing the patient to the OR and took on average 3.5 minuted. Overall, the guided discussion was very well received by participants and provided an opportunity to inform providers of the patient's information to address potential problems. The authors cited that variations in workflow patterns as a potential barrier to widescale implementation of the checklist discussion.
Incorrect answers:
The outcomes of three novel interventions are investigated and the preliminary results are depicted in Figure A. Which of the following statements is most accurate?
Linezolid acts to inhibit protein synthesis by preventing the formation of the initiation complex between the 30S and 50S subunits of the ribosome.
Linezolid is a type of oxazolidinone, a relatively newer class of antibiotics that are active against multidrug-resistant staphylococci, streptococci, and enterococci. Although many antimicrobial agents affect or disrupt protein synthesis in bacteria, linezolid is unique in that it disrupts protein synthesis at its origin rather than later in the cascade. It achieves this by binding to the
50S subunit of the bacterial ribosome, preventing the formation of the initiation complex.
Swaney et al. performed a study to investigate the mechanism of action of linezolid. They found that linezolid inhibits the formation of the initiation complex in bacterial translation systems by preventing the formation of the N- formylmethionyl-tRNA-ribosome-mRNA ternary complex.
Thompson et al. performed a study on the efficacy of various antibiotics in treating periprosthetic joint infections (PJI). They administered oral linezolid with or without oral rifampin, intravenous vancomycin with oral rifampin, intravenous daptomycin or ceftaroline with or without oral rifampin, oral doxycycline, or sham treatment at human- exposure doses for 6 weeks in a mouse model of PJI. They found that oral-only linezolid-rifampin and all intravenous antibiotic-rifampin combinations resulted in no recoverable bacteria and minimized reactive bone changes. Additionally, although oral linezolid was found to be the most effective monotherapy, all oral and intravenous antibiotic monotherapies failed to clear infection or prevent reactive bone changes.
They concluded that the oral-only linezolid-rifampin option might reduce venous access complications and health-care costs.
Illustration A is a diagram depicting the mechanism of action of various antibiotics.
Incorrect Answers:
50S subunit of the bacterial ribosome, preventing protein chain elongation by inhibiting peptidyl transferase activity of the ribosome.
elongation by blocking aminoacyl translocation.
Failure of effective communication in the surgical setting has been associated with what?
Unfractionated heparin works in the coagulation cascade by promoting the ability of antithrombin III to inhibit factors IIa, III, Xa.
Heparin works by binding to and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. It is metabolized by the liver. The risks associated with the use of unfractionated heparin include bleeding and heparin induced thrombocytopenia (HIT). The reversal agent is protamine sulfate.
Agnelli et al. reviewed direct thrombin inhibitors for the prevention of VTE after major orthopaedic surgery. They reported widespread use, however, limitations in the use of unfractionated heparin and low-molecular-weight heparins. They highlighted that direct thrombin inhibitors (Ximelagatran) inactivate thrombin without requiring any plasma cofactor, inhibit both free
and fibrin-bound thrombin, and do not appreciably bind to plasma proteins. They concluded that the features of rapid absorption, conversion, bioavailability, low variability, dose-time, food independency, and the predictable anticoagulant activity make direct thrombin inhibitors an attractive antithrombotic agent especially for prolonged out-of hospital prophylaxis.
Kwong et al. reviewed the efficacy and safety of fondaparinux, a selective factor Xa inhibitor and reported its efficacy and safety in 4 phase III clinical trials. They reported fondaparinux usage resulted in an overall 55% decrease in the risk of venous thromboembolism (VTE) relative to the low-molecular- weight heparin enoxaparin without increasing the incidence of clinically relevant bleeding, which was similarly low for both agents. They concluded
that the superior efficacy of fondaparinux relative to enoxaparin is the result of its unique mechanism of action, clinical pharmacology.
McLynn et al. investigated the risk factors and chemoprophylaxis for VTE in elective spine surgery. They reported that independent risk factors for VTE included greater age, male gender, increasing body mass index, dependent functional status, lumbar spine surgery, longer operative time, perioperative blood transfusion, longer length of stay, and other postoperative
complications. The majority of patients received unfractioned heparin and they observed this did not significantly influence the rate of VTE, but was associated with a significant increase in hematoma requiring a return to the operating room. They concluded that there is insufficient evidence to support the routine use of chemoprophylaxis in low-risk patients, and recommended full consideration of risks and benefits after elective spine surgery.
Figure A depicts the coagulation cascade, with the factor circled in red (IIa) being the target of unfractionated heparin, through its effect on antithrombin III.
Incorrect Answers:
Which of the following antibiotics acts to inhibit protein synthesis by preventing the formation of the initiation complex between the 30S and 50S subunits of the ribosome?
Acetaminophen inhibits prostaglandin E2 production through its effect on interleukin-1 beta. It exerts its effects on the central nervous system.
Multimodal pain management has become an increasingly important consideration in total joint arthroplasty recovery, namely in regard to minimizing opioid requirements while optimizing pain control and patient satisfaction. Given the negative side effects and increasing scrutiny on narcotic use, modalities that help to decrease post-operative narcotic requirements have become a major focus and include nonsteroidal anti- inflammatories, selective COX-2 inhibitors, gabapentinoids, local anesthetic blocks, and acetaminophen. Acetaminophen acts directly the central nervous system, providing both pain relief and antipyretic effects. It does so by inhibiting prostaglandin E2 production through the blockade of interleukin-1 beta.
Jinnah et al. performed a comparison of two multimodal pain regimens used for postoperative pain control in total joint arthroplasty patients. They hypothesized that using a multimodal pain protocol focusing on periarticular injections including liposomal bupivacaine would have improved results when compared with a parenteral opioid- based regimen. They found a decrease in length of stay and rate of discharge to skilled nursing facilities with the implementation of a novel multimodal protocol. They concluded that a multimodal approach inclusive of periarticular injection can lead to a reduced
length of stay.
Politi et al. performed a prospective randomized trial comparing the use of intravenous versus oral acetaminophen in total joint arthroplasty. They found that IV acetaminophen did not provide a significant difference in pain relief except within the first 0-4 hours. They concluded that IV acetaminophen does not provide a significant benefit when compared to the oral form, which is also less expensive.
Incorrect Answers:
Which of the following agents results in blood anticoagulation by exerting inhibitory effects on the factor circled in the color red in Figure A?
Based on the stress-strain curve in Figure A, ceramic has the highest modulus of elasticity.
Young's modulus is a measure of the stiffness (ability to resist deformation) of a material in the elastic zone that is calculated by measuring the slope of the stress-strain curve in the elastic zone. A higher modulus of elasticity indicates a stiffer material. Relative values of Young's modulus include: (1) ceramic, (2) alloy, (3) stainless steel, (4) titanium, (5)
cortical bone, (6) matrix polymers, (7) PMMA, (8) polyethylene, (9) cancellous bone, (10) tendon/ligaments, and (11) cartilage.
Lang et al. published a review on the use of ceramics in total hip replacement. They report that properties of ceramic which make it particularly attractive for this application include its hardness, high compression strength, and excellent wettability. However, its low fracture toughness and linear elastic behavior make it prone to breakage under stress.
Figure A is a stress-strain curve, the slope of which is used to determine Young's modulus.
Incorrect Answers:
Which of the following medications work by inhibiting prostaglandin E2 production through interleukin-1 beta?
A power analysis determines the minimum number of patients needed in a study to show a clinically significant difference. It should be performed before starting the study.
Power is the probability of finding a significant association if one truly exists. It is defined as 1 minus the probability of a type 2 error (beta) and is generally set to 80% meaning that we are willing to accept a 20% chance of a type 2 error. A power analysis will determine the minimum number of patients that shows a clinically significant difference. The minimum number of patients should be determined prior to initiating a study. Calculation of power after a study has been completed is controversial and discouraged.
Vavken et al. performed a review on the management of confounding in controlled orthopaedic trials. They report that confounding occurs when the effect of exposure of an outcome is distorted by a confounding factor and will lead to spurious effect estimates in clinical studies. They performed a cross- sectional study of a sample of controlled trials reported in the orthopaedic literature in 2006. They conclude that only 30 studies reported that the had a power analysis performed.
Kocher et al. performed a review of clinical epidemiology and biostatistics as a primer for orthopedic surgeons. They report that a power analysis should be performed prior to initiating the study. This will ensure the study is appropriately powered and decrease the effects of chance. They conclude that when a study determines no significant effect the power of the study should be reported.
Incorrect Answers:
Based on the stress-strain curve in Figure A, which of the following materials has the highest modulus of elasticity?
The World Health Organization (WHO) defines osteopenia as a bone mineral density (BMD) that is between 1 and 2.5 standard deviations below young normal (T-score of - 1 to -2.5).
The WHO defines osteopenia as decreased BMD without fracture risk. Osteopenia is defined as a T-score of 1 to 2.5 standard deviations below young normals (-1 to -2.5), while osteoporosis is defined as a T-score of more than
Question 17
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?
Explanation
REFERENCES: Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000,
pp 598-601.
Question 18
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 19
A 58-year-old African-American female who sustained an injury to her upper arm six months ago presents with persistent arm pain. She was initially treated with splinting, with conversion to fracture bracing. She is neurovascularly intact. An injury radiograph and a current radiograph are shown in Figures A and B respectively. What nutritional or metabolic disturbance is the most likely associated with this patient's diagnosis? Review Topic

Explanation
The incidence of nonunion with non-operative management of humeral shaft injuries ranges from 2-10%. Risk factors include vitamin D deficiency (most common), open fractures, segmental injuries, smoking and obesity. The optimal treatment is compression plating with bone grafting, which has been shown to be superior to intramedullary nailing with bone grafting or compression plating alone.
Ring et al. reviewed factors that contributed to humeral diaphyseal nonunion after fracture bracing. Fractures in the proximal to middle one-third of the shaft or fractures with a spiral/oblique pattern were more likely to go on to nonunion.
Brinker et al. reviewed 37 low-energy fractures that went onto nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having Vitamin D deficiency.
Figure A demonstrates a humeral shaft fracture. Figure B demonstrates an atrophic nonunion of the humeral shaft fracture.
Incorrect Answers:
Question 20
Which of the following alternatives to autogenous bone grafting functions through osteoinduction?
Explanation
Question 21
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman’s test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
REFERENCES: Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 22
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
Question 23
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
REFERENCES: Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Question 24
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Explanation
REFERENCES: Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394.
Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Weil WM, Trumble TE: Treatment of distal radius fractures with intrafocal (Kapandji) pinning and supplemental skeletal stabilization. Hand Clin 2005;21:317-328.
Question 25
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 26
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is
Explanation
REFERENCES: Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146.
Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 27
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?
Explanation
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 28
-The use of a soft cervical orthosis is most supported for which injury?
Explanation

Question 29
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Henry R, Goletz B, Williamson C: Lateral release in patello-femoral subluxation. Am J Sports Med 1986;14:121.
Question 30
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?
Explanation
REFERENCES: Carter TR: Meniscal allograft transplantation. Sports Med Arthroscopy Rev 1999;7:51-63.
Garrett JC: Meniscal transplantation: A review of 43 cases with two- to seven-year follow-up. Sports Med Arthroscopy Rev 1993;2:164-167.
van Arkel ER, de Boer HH: Human meniscal transplantation: Preliminary results at 2- to 5-year follow-up. J Bone Joint Surg Br 1995;77:589-595.
Question 31
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
REFERENCE: Murphy S, Deshmukh R: Periacetabular osteotomy: Preoperative radiographic predictors of outcome. Clin Orthop 2002;405:168-174.
Question 32
Because the patient shown in Figure 27 can no longer fit in shoes, treatment of the deformity should consist of
Explanation
REFERENCES: Turra S, Santini S, Cagnoni G, Jacopetti T: Gigantism of the foot: Our experience in seven cases. J Pediatr Orthop 1998;18:337-345.
Guidera KJ, Brinker MR, Kousseff BG, et al: Overgrowth management in Klippel-Trenaunay-Weber and Proteus syndromes. J Pediatr Orthop 1993;13:459-466.
Question 33
-What is the most likely area of injury?
Explanation
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
Question 34
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 35
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 36
A 28-year-old construction worker sustains the closed injury shown in Figures A and B after a fall from a height. He is taken to the operating room. What is the next best step?

Explanation
In the distal tibial metaphysis, there is no snug endosteal fit for an IM nail. Center-center nail placement in both proximal and distal fragments is necessary to maintain alignment. There is also increased stress on distal locking bolts to maintain fracture alignment. Assuming static medial-lateral distal locking screws, accurate coronal plane and rotational alignment is achieved by fibular plating as a first step. This also
prevents late loss of alignment because of distal locking screw toggle. Reamed nailing allows a stiffer, larger nail to be placed, and allows redistribution of endosteal osteogenic material to the fracture site. Although there is endosteal vascular compromise, this does not affect fracture healing because of intact periosteal supply.
Bhandari et al. conducted a prospective, randomized, blinded comparison of 622 patients who had reamed nailing, and 604 who had unreamed nailing. For closed fractures, a significantly greater number in the unreamed group required bone grafting, implant exchange and dynamization. There was no difference in groups for open fracture nailing.
Egol et al. retrospectively reviewed distal metaphyseal tibia-fibula fractures treated with IM nailing with (25 cases) and without (47 cases) adjunctive plating. They found that plating was associated with maintenance of reduction (significant) as was the use of 2 medial-lateral distal locking bolts (not significant). They recommend fibular plating when IM nailing for distal tibia fractures.
Figures A and B show an extraarticular distal tibia fracture with distal fibula fracture. Incorrect Answers
Question 37
What adaptations occur in the dominant shoulder of throwers compared to their nondominant shoulder? Review Topic
Explanation
Question 38
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment? Review Topic
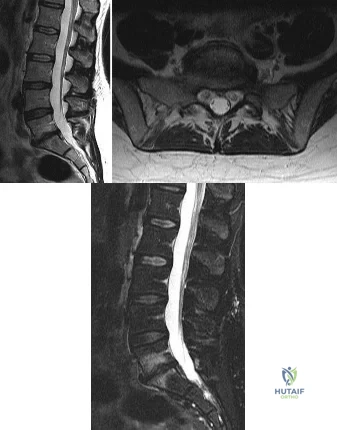
Explanation
In a recent updated Cochrane Review of surgery for degenerative lumbar spondylosis, it was noted that while Fritzell and associates appeared to provide strong evidence in favor of fusion, a more recent trial by Brox and associates demonstrated no difference between those patients undergoing lumbar fusion compared to those receiving cognitive intervention and exercise. The Cochrane Review suggests that this may reflect a difference between the control groups. Fritzell and associates compared lumbar fusion to standard 1990s “usual care,” whereas Brox and associates compared lumbar fusion to a “modern rehabilitation program.” Bear in mind that this patient is a certified athletic trainer and runs a hospital health fitness department; therefore, at least for purposes of this question, it can be assumed that she has participated in a “modern rehabilitation program.” The Cochrane Review goes on to state that preliminary results of three small trials of intradiskal electrotherapy suggest that it is ineffective and that preliminary data from three trials of disk arthroplasty do not permit firm conclusions.
Question 39
- For which of the following conditions will a rehabilitation program for shoulder instability most likely result in a satisfactory response?
Explanation
glenohumeral joint. In this classification Type I is a traumatic subluxation without previous dislocation, Type II is a traumatic subluxation after previous dislocation, Type IIIA is an atraumatic, voluntary subluxation in patients with psychological problems, Type IIIB is and atraumatic, voluntary subluxation in a patient without psychological problems and Type IV is an involuntary subluxation. In their study they found that
shoulders that have traumatic instability (type I or type II) had a 15 per cent chance of a good or excellent outcome with a rehab program as compared with atraumatic subluxations (type III or type IV) which had an 83 per cent good to excellent result. Since answer 5 is the only atraumatic type of subluxation it would statistically stand the best chance for improvement with a rehab program.
Question 40
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 41
An 18-year-old male soccer player sustains a knee injury during a game. Examination is notable for a positive pivot shift test. What other physical examination finding is most likely to be present? Review Topic
Explanation
ACL tears usually occur as a result of a non-contact pivoting injury. Abnormal anterior translation results in bone contusions of mid-lateral femoral condyle and posterolateral tibia, which can be seen on MRI. Other concomitant intraarticular injuries include meniscal tears (lateral > medial), chondral damage and other ligamentous injury (MCL, LCL, PLC) usually found in cases of higher energy trauma such as a knee dislocation.
Piasecki et al prospectively analyzed intraarticular injuries associated with ACL tears in high school athletes by gender and sport. There was no significant difference in mechanism of injury between sexes. Female basketball and soccer players had fewer intraarticular injuries (medial femoral condyle lesions, medial and lateral meniscus tears) compared to male athletes. The authors hypothesized that women may therefore enjoy a better prognosis following reconstruction.
Spindler et al performed a prospective cohort study investigating concomitant intraarticular injuries in patients who underwent ACL reconstruction. Eighty percent of patients had a bone bruise on MRI, 68% involving the lateral condyle. At time of arthroscopic reconstruction, meniscal tears were identified in 56% of lateral menisci and 37% of medial menisci.
Incorrect Responses:
Question 42
-What is the etiology of this patient’s problem?
Explanation
Little leaguer’s shoulder is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Factors that contribute to the condition include excessive throwing,improper throwing mechanics, and muscle-tendon imbalance. Radiographs usually show widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. Treatment involves rest until symptoms resolve, followed by initiation of an interval throwing program. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The dominant shoulders of throwing athletes undergo adaptive changes, resulting in increased external rotation and decreased internal rotation. These changes occur secondary to softtissue and bony adaptations, including increased humeral retroversion. Ischemia has been implicated as a potential cause of osteochondritis dissecans lesions. Rotator cuff tendonitis presents with anterolateral shoulder pain that is worse with activity. Pain is reproduced with resisted supraspinatus testing, and radiograph findings are typically normal.
Adolescent shoulder injuries are often caused by subtle, atraumatic instability most often sustained in sports with overhead movements, including baseball. These symptoms are more likely to occur in athletes with evidence of increased soft-tissue laxity.
Question 43
Figure 100 is the MRI scan of a 52-year-old runner who has right knee pain that has been occurring 10 minutes into her run for 2 months. On examination, she has tenderness over the lateral epicondyle. Her Ober test result is positive. What is the most appropriate initial treatment? Review Topic
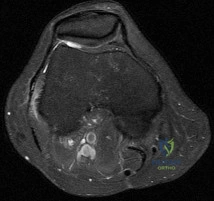
Explanation
Question 44
One year after undergoing a primary total knee arthroplasty, a 65-year-old man has a 1-week history of new onset anterior knee pain. He can perform a straight-leg raise with no extension lag. Radiographs reveal a transverse patella fracture with 8 mm of displacement and an intact patellar component. The best course of treatment is
Explanation
This patient has a displaced periprosthetic patella fracture with an intact extensor mechanism. Surgical treatment for this condition has been associated with relatively poor clinical results because the fracture occurs late (attributable to patella osteonecrosis). The optimal initial treatment is to treat the fracture nonsurgically with immobilization of the knee in extension either with a long-leg cast or knee immobilizer.
Question 45
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 46
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 47
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?
Explanation
REFERENCE: Robbins MI, Wilson MG, Sella EJ: MR imaging of anterosuperior calcaneal process fractures. Am J Roentgenol 1999;172:475-479.
Question 48
A 42-year-old woman complains of ankle pain with weightbearing for the last 2 years. She recalls spraining her ankle more than 10 years ago. She plays tennis and regularly walks 5 miles a day for exercise, but has had to give up these activities over the last few months because of pain. Examination reveals limitation in ankle dorsi- and plantar flexion. A course of non-operative management has been unsuccessful. Which of the following options will most likely provide pain relief and allow her to return to her previous activity level?

Explanation
Supramalleolar osteotomy may be performed for varus (medial opening wedge or lateral closing wedge) or valgus (lateral opening wedge or medial closing wedge) ankles. They are suited for near-normal ROM minimal talar-tilt or varus heel alignment, asymmetric ankle arthritis (confined to medial or lateral compartment; corresponding to Takakura Stage II or IIIA for medial ankle arthritis).
Pagenstert et al. looked at realignment surgery for posttraumatic arthritis in 35 patients. For valgus ankles, they performed 18 medial closing wedge and 1 lateral opening wedge osteotomies. For varus ankles, they performed 7 medial opening wedge and 4 lateral closing wedge osteotomies. There was improvement in pain (7/10 to 3/10), ROM (33° to 38°) and Takakura score (2.3 to 1.3).
Lee et al. described supramalleolar osteotomy for medial arthritis in 16 patients. There was improvement in AOFAS score (62 to 82), Takakura stage (2.9 to 2.3), tibial-anterior surface angle (85 to 100°). Patients with low postoperative talar tilt (TT) had better clinical and radiographic results than those with high TT. Greater postoperative heel valgus predicted for postoperative subfibular pain.
Figure A shows valgus alignment at the ankle. Illustration A shows the same ankle following medial closing wedge supramalleolar osteotomy. Illustration B is a table showing the Takakura classification. Illustration C demonstrates correction of the tibial-anterior surface angle (TAS) following supramalleolar osteotomy.
Incorrect Answers:
Question 49
- Which of the following is considered an advantage of an unreamed intramedullary nail over a reamed intramedullary nail?
Explanation
Question 50
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of
Explanation
not indicated.
REFERENCES: Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Question 51
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton’s neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657.
Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 52
The recurrent motor branch of the median nerve innervates which of the following muscles?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 170.
Question 53
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?
Explanation
REFERENCE: Ogut T, Akgun I, Kesmezacar H, et al: Navigation for ankle arthroscopy: Anatomical study of the anterolateral portal with reference to the superficial peroneal nerve. Surg Radiol Anat 2004;26:268-274.
Question 54
Which of the following body positions is associated with the highest intradiskal pressure?
Explanation
REFERENCES: Nachemson A, Morris JM: In vivo measurements of intradiscal pressure.
J Bone Joint Surg Am 1964;46:1077-1092.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 547-556.
Question 55
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 56
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi V: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7:223-227.
Question 57
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
REFERENCES: Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Fahrer H, Rentsch HU, Gerber NJ, et al: Knee effusion and reflex inhibition of the quadriceps: A bar to effective retraining. J Bone Joint Surg Br 1988;70:635-638.
Question 58
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?
Explanation
REFERENCES: Bach BR, O’Brien SJ, Warren RF, et al: An unusual neurologic complication of the Bristow procedure. J Bone Joint Surg Am 1988;70:458-460.
McIlveen SJ, Duralde XA: Isolated nerve injuries about the shoulder, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 214-239.
Question 59
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?
Explanation
REFERENCES: Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.
Fang A, Hu SS, Endres N, et al: Risk factors for infection after spinal surgery. Spine 2005;30:1460-1465.
Question 60
Of all the pelvic ring injury types, anteroposterior compression type III pelvic ring injuries have the highest rate of which of the following?

Explanation
Question 61
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?
Explanation
REFERENCES: Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Glasser DB, Lane JM, Huvos AG, Marcove RC, Rosen G: Survival, prognosis, and therapeutic response in osteogenic sarcoma: The Memorial Hospital experience. Cancer 1992;69:698-708.
Question 62
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 63
What structure is located at the tip of the arrow in Figure 18?
Explanation
REFERENCE: An H: Diagnostic imaging of the spine, in Principles and Techniques of Spine Surgery. Baltimore, MD, Lippincott Williams & Wilkins, 1998, pp 102-125.
Question 64
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
REFERENCES: Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 65
Which of the following aids in correction of patellar tracking after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 1245-1258.
Merkow RL, Soudry M, Insall JN: Patellar dislocation following total knee replacement. J Bone Joint Surg Am 1985;67:1321-1327.
Question 66
Which gene mutation or polymorphism has been shown to most increase the risk for venous thromboembolic disease after elective total joint arthroplasty?
Explanation
Simultaneous bilateral TKA accounts for approximately 6% of the TKAs performed in the United States and is more frequently performed for women. The incidence of pulmonary embolism in this group was between 0.57 and 1.14, according to a 1999 to 2008 registry-based study in the United States. There was not a significant change in incidence during that period. Hypoxemia alone is not an indication for advanced testing for pulmonary embolism. Winters and associates demonstrated that to avoid unnecessary testing, the use of a hypoxia algorithm is a reasonable first step. The use of pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty and who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a Moderate grade of recommendation in the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty. Various genetic factors are associated with increased risk for venous thromboembolic disease after TKA. A recent meta-analysis evaluated the genetic and polymorphism profiles associated with venous thromboembolism after arthroplasty. The mutation MTHFR/C677T/TT carried the highest risk (OR 2.36; 95% CI, 1.03-5.42, P = 0.04) for the gene mutations and polymorphisms studied. With the increased use of TXA as a blood-conservation strategy for total joint arthroplasty, there is a theoretical concern about an increased risk for venous thromboembolic disease. A recent study by Duncan and associates included 13,262 elective total joint arthroplasty procedures and demonstrated that TXA does not increase the risk of venous thromboembolism.

Question 67
A 47-year-old woman has a right bunion that has been symptomatic despite modifications in shoe wear. She requests surgical correction. An AP radiograph is shown in Figure 37. Treatment should consist of
Explanation
REFERENCES: Coughlin MJ, Carlson RE: Treatment of hallux valgus with an increased distal metatarsal articular angle: Evaluation of double and triple first ray osteotomies. Foot Ankle Int 1999;20:762-770.
Coughlin MJ: Hallux valgus. Instr Course Lect 1997;46:357-391.
Question 68
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 69
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
application of a hinged external fixator may be considered.
Question 70
Exostoses in which of the following anatomic locations is the most likely to undergo malignant transformation in a patient with multiple hereditary exostosis (MHE)?
Explanation
REFERENCES: Peterson HA: Multiple hereditary osteochondromata. Clin Orthop 1989;239:222.
McCornack EB: The surgical management of hereditary multiple exostosis. Orthop Rev 1981;10:57.
Question 71
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child’s back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of Review Topic

Explanation
Question 72
What gene is expressed the earliest during the differentiation of a chondrocyte during endochondral ossification?
Explanation
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Sandell LJ: Genes and gene expression. Clin Orthop 2000;379:S9-S16.
Question 73
below shows the standing AP radiograph obtained from a year-old man who has a year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 74
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
REFERENCES: Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531.
Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 75
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?
Explanation
REFERENCES: Kelly MA: Extensor mechanism complications in total knee arthroplasty.
Instr Course Lect 2004;53:193-199.
Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Norman AJ, Scott S, David GN (eds): Master Techniques in Knee Arthroplasty, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2003.
Question 76
- A 15-year-old girl has a thoracic kyphosis that causes mild pain. Examination reveals a sagittal curve measuring 55 degrees and wedging of the eighth through tenth vertebrae. The iliac apophyses are Risser 4. Management should include
Explanation
(2) with surgical fusion if >75o and Risser 3 or less, (3) with surgical fusion if >65o and Risser 4/5 if necessary or symptomatic. Posterior instrumentation, anterior release and interbody fusion is the treatment of choice for curves >75o, or those >55o on hyperextension. Other causes of kyphosis include trauma, infection, spondylitis, bone dysplasia, neoplasia, neurofibromatosis.
Question 77
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Explanation
REFERENCES: Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 78
What is the principal advantage of surgical repair for the lesion shown in Figure 19?
Explanation
REFERENCES: Bhandari M, Guyatt GH, Siddiqui F, et al: Treatment of acute Achilles tendon ruptures: A systematic overview and meta-analysis. Clin Orthop 2002;400:190-200.
Schepsis AA, Jones HE, Haas AL: Achilles tendon disorders in athletes. Am J Sports Med 2002;30:287-305.
Question 79
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of
Explanation
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 80
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
REFERENCES: Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Shin AY, Moran ME, Wenger DR: Superior gluteal artery injury secondary to posterior iliac crest bone graft harvesting: A surgical technique to control hemorrhage. Spine 1996;21:1371-1374.
Question 81
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 82
Which of the following is considered a major characteristic of hyaluronate?
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78.
Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Hurd ER: Extraarticular manifestations of rheumatoid arthritis. Semin Arthritis Rheum 1979;8:151-176.
Question 83
A 65-year-old woman undergoes a lumbar laminectomy for spinal stenosis at the L3-L4 level. The surgery and postsurgical course are uncomplicated. Eight weeks after surgery she has severe left anterior thigh, groin, and knee pain with ambulation and standing. Which condition is the most likely cause of her symptoms?
Explanation
Disorders of the hip can mimic and/or coexist with lumbar spine disorders. The prevalence of hip pain lasting longer than 1 month in patients ages 65 to 74 years is 19%. There is often overlap between their respective signs and symptoms. In a patient with failed back surgery syndrome, hip pathology may have been present before back surgery and not recognized. Osteoarthritis of
the hip typically causes groin and anterior thigh pain. Meralgia paraesthetica is more likely to manifest immediately after surgery. Trochanteric bursitis usually affects the proximal lateral thigh and often can radiate to the distal thigh. Facet joint pain causes low-back pain that can be referred to the gluteal region. Epidural hematoma 6 weeks after surgery is highly unlikely.
RECOMMENDED READINGS
Bolt PM, Wahl MM, Schofferman J: The roles of the hip, spine, sacroiliac joint, and other structures in patients with persistent pain after back surgery. Seminars in Spine surgery 2008;20:14-19.
Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;(419):280-4. PubMed PMID: 15021166. View Abstract at PubMed
Question 84
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 85
What is the most common bone tumor in the hand?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Kuur E, Hansen SL, Lindequist S: Treatment of solitary enchondromas in fingers. J Hand Surg Br 1989;14:109-112.
Question 86
Patient outcome after open reduction and internal fixation of tibial plateau fractures shows that patients older than 50 years of age when compared to younger patients have
Explanation
Question 87
A senior resident is scheduled to perform a posterior medial release on a 10-month-old infant who has a congenital clubfoot deformity. Informed consent is obtained for the procedure. The supervising surgeon is obligated to give the parents what information?
Explanation
gave consent.
REFERENCES: Kocher MS: Ghost surgery: The ethical and legal implications of who does the operation. J Bone Joint Surg Am 2002;84:148-150.
Holmes MK: Ghost surgery. Bull NY Acad Med 1980;56:412-419.
Question 88
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
Question 89
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
Explanation
REFERENCES: Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears.
Am J Sports Med 2005;33:1405-1417.
Fukuda H: The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br 2003;85:3-11.
Question 90
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 91
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?
Explanation
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 92
- Successful healing of a meniscal repair is most likely associated é which of the following tear patterns?
Explanation
Arnoczky et al described the vascular supply to the meniscus and showed that tears within the outer one third of the meniscus have the best healing potential. Rim width is the most important prognostic factor for meniscal repairs; the vascular one third of the meniscus is most conductive to healing. Scott et al found better results when the tear was within 2mm of the meniscosynovial junction. Stone et al found improved healing with rim widths of 6mm or less. Tenuta et al found best results within a rim width of 3mm or less.
Question 93
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.
Question 94
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
Question 95
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient’s knee joint. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Kier R, McCarthy SM: Lipohemarthrosis of the knee: MR imaging. J Comput Assist Tomogr 1990;14:395-396.
Question 96
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 97
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286, 339-365.
Question 98
- What is the treatment of choice for an adult who has an isolated fracture of the ulna at the junction of the distal and middle thirds, with 5 degrees apex dorsal angulation and 25% displacement?
Explanation
Question 99
A 70-year-old man has a posterior dislocation 20 years after undergoing cementless THA with a metal-on-polyethylene bearing. Acetabular inclination is 55 degrees with neutral version. This is his third dislocation, and he has been treated with closed reduction 3 times during the past month. His ESR is 42 mm/h (reference range [rr], 0-20 mm/h) and CRP level is 16.2 mg/L (rr, 0.08-3.1 mg/L). Joint aspiration reveals a cell count of 865 cells (55% neutrophils).
Explanation
Treatment options for various pathologic conditions after THA can be challenging, and there are often multiple potential options. Question 91 involves a patient who has fractured a modular ceramic acetabular liner, and an isolated head and liner exchange should be sufficient. Question 92 involves a patient with markedly elevated serum metal ions and abductor dysfunction, suggesting poor bearing function and a probable adverse local tissue reaction (ALTR). Additionally, the acetabular component position is suboptimal, and complete
acetabular revision would be appropriate. Question 93 involves a patient with elevated serum metal ions, with cobalt disproportionately higher than chromium in a roughly 7:1 ratio, suggesting corrosive changes at the prosthetic femoral neck (trunnionosis). Cross-sectional imaging continues to be a key part of the evaluation and treatment of patients with metal reactions. This patient’s pain and Trendelenburg gait are suggestive of ALTR. An isolated head and liner exchange should be performed, typically using a ceramic head and titanium sleeve adapter. Question 94 involves late, recurrent instability, probably related to bearing surface wear and acetabular component position. Continued nonsurgical management is unlikely to succeed at this point, so it would be appropriate to proceed with acetabular component revision.
Question 100
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Frankle MA, Ondrovic LE, Markee BA, et al: Stability of tuberosity reattachment in proximal humeral hemiarthroplasty. J Shoulder Elbow Surg 2002;11:413-420.
