Orthopedic Surgery Board Review MCQs: Trauma, Arthroplasty & Hip | Part 247

Key Takeaway
This page offers Part 247 of a comprehensive, high-yield MCQ set for orthopedic residents and surgeons preparing for OITE and AAOS board certification exams. It contains 100 verified questions, covering Ankle, Hip, and Trauma, designed to simulate exam conditions and enhance preparation through interactive study and exam modes.
About This Board Review Set
This is Part 247 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 247
This module focuses heavily on: Ankle, Arthroplasty, Dislocation, Foot, Fracture, Hip, Trauma.
Sample Questions from This Set
Sample Question 1: What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?...
Sample Question 2: A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion...
Sample Question 3: A 63-year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coatedtitanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 ye...
Sample Question 4: Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?...
Sample Question 5: Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropat...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?
Explanation
(SBQ12TR.86) Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intraoperatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by >or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Question 2
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 3
A 63-year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 4
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
REFERENCES: Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119.
Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362.
Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
McKellup HA: Bearing surfaces in total hip replacement: State of the art and future developments. Instr Course Lect 2001;50:165-179.
Question 5
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
REFERENCES: Lin SS, Lee TH, Wapner KL: Plantar forefoot ulceration with equinus deformity of the ankle in diabetic patients: The effect of tendo-Achilles lengthening and total contact casting. Orthopedics 1996;19:465-475.
Armstrong DG, Stacpoole-Shea S, Nguyen H, Harkless LB: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 6
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs. New York, NY, Harper & Row, 1969.
Question 7
A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsophalangeal joint that was aggravated by weight bearing. A removable walker boot partially relieved the pain, and she was able to complete the season. Her pain has now returned; however, she denies any history of injury. Examination reveals tenderness over the medial sesamoid but no deformities. A radiograph and bone scan are shown in Figures 22a and 22b. What is the best treatment option at this time?
Explanation
REFERENCES: Sanders R: Fractures of the midfoot and forefoot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1601-1603.
Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals. Foot Ankle Int 2003;24:415-419.
Question 8
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of
Explanation
REFERENCES: Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine
1992;17:1137-1143.
Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Farey ID, McAfee PC, Davis RF, Long DM: Pseudarthrosis of the cervical spine after anterior arthrodesis: Treatment by posterior nerve root decompression, stabilization, and arthrodesis.
J Bone Joint Surgery Am 1990;72:1171-1177.
Question 9
- The Injury Severity Score (ISS), using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by
Explanation
Question 10
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Hofmann A, Wenger DR: Posteromedial bowing of the tibia: Progression of discrepancy in leg lengths. J Bone Joint Surg Am 1981;63:384-388.
Question 11
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 12
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Society for Surgery of the Hand, 1994, pp 197-205.
Question 13
A 10-year-old girl is treated for a tibia/fibula fracture with a long leg cast. The on-call resident is called to evaluate the patient for increasing pain medicine requirements and tingling in her foot. Examination of the cast reveals that the ankle has been immobilized in 10 degrees of dorsiflexion. What ankle position results in the safest compartment pressures in a casted lower leg?

Explanation
Weiner et al measured intramuscular compartment pressure in the anterior and deep posterior compartments of the leg in seven healthy adults who had long leg casts placed. They found that in a casted leg the intramuscular pressure in the anterior compartment was lowest with the ankle in neutral, and the deep posterior compartments was lowest when the ankle joint was in the resting position to approximately 37 degrees of plantar flexion. Based on this, they concluded that the safest ankle casting position regarding compartment pressure is between 0 and 37 degrees of plantar flexion. After the cast was bivalved, they noted a significant decrease in intramuscular pressure of 47 per cent in the anterior compartment and of 33 per cent in the deep posterior compartment. Constrictive casts and abberant ankle positioning can exacerbate pain/symptoms. Loosening of the cast by bivalving, spreading, and cutting underlying stockinette/softroll should always be the first step in management of possible compartment syndrome.
Question 14
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 15
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 16
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of
Explanation
REFERENCES: Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Kaplan H, Kiral A, Kuskucu M, et al: Report of eight cases of humeral fracture following the throwing of hand grenades. Arch Orthop Trauma Surg 1998;117:50-52.
Question 17
A 77-year-old man with diabetes mellitus has had a nonhealing Wagner grade I ulcer under the medial sesamoid for the past 3 months. He smokes tobacco regularly. He has undergone several debridements and total contact casting. Examination reveals no palpable pulses. He has no erythema or purulence, and he is afebrile. Radiographs reveal no abnormalities. What is the best initial diagnostic test to help determine why the ulcer has failed to heal?
Explanation
REFERENCE: Brodsky JW: Evaluation of the diabetic foot. Instr Course Lect 1999;48:289-303.
Question 18
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 19
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of
Explanation
REFERENCES: Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Gil JF, Haydar A: Isolated injury of the coracoid process: Case report. J Trauma
1991;31:1696-1697.
Question 20
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Explanation
Question 21
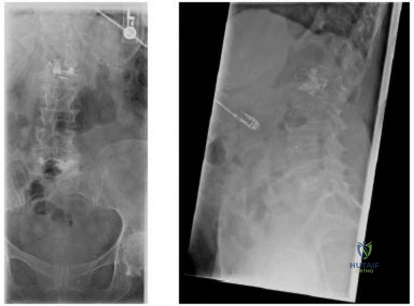
A 58-year-old African-American female who sustained an injury to her upper arm six months ago presents with persistent arm pain. She was initially treated with splinting, with conversion to fracture bracing. She is neurovascularly intact. An injury radiograph and a current radiograph are shown in Figures A and B respectively. What nutritional or metabolic disturbance is the most likely associated with this patient's diagnosis? Review Topic

Explanation
The incidence of nonunion with non-operative management of humeral shaft injuries ranges from 2-10%. Risk factors include vitamin D deficiency (most common), open fractures, segmental injuries, smoking and obesity. The optimal treatment is compression plating with bone grafting, which has been shown to be superior to intramedullary nailing with bone grafting or compression plating alone.
Ring et al. reviewed factors that contributed to humeral diaphyseal nonunion after fracture bracing. Fractures in the proximal to middle one-third of the shaft or fractures with a spiral/oblique pattern were more likely to go on to nonunion.
Brinker et al. reviewed 37 low-energy fractures that went onto nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having Vitamin D deficiency.
Figure A demonstrates a humeral shaft fracture. Figure B demonstrates an atrophic nonunion of the humeral shaft fracture.
Incorrect Answers:
Question 22
A 67-year-old woman has persistent anterior thigh and knee pain after undergoing total knee arthroplasty 1 year ago. Examination and radiographs reveal no problems in the knee, mild hip flexor weakness (grade 4+), and decreased sensation over the anterior thigh including and proximal to the incision. MRI of the lumbar spine will most likely reveal which of the following findings?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 250.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 23
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Kwong LM, Miller AJ, Lubinus P: A modular distal fixation option for proximal bone loss in revision total hip
arthroplasty: A 2- to 6-year follow-up study. J Arthroplasty 2003;18:94-97.
Question 24
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 25
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Goldenberg RR, Campbell CJ, Bonfiglio M: Giant cell tumor of bone: An analysis of two hundred and eighteen cases. J Bone Joint Surg Am 1970;52:619-664.
Question 26
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of
Explanation
REFERENCES: Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Stover S, Niemann K, Tullos J: Experience with surgical resection of heterotopic bone in spinal cord injury patients. Clin Orthop 1991;263:71-77.
Question 27
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
Question 28
Which of the following changes in the parameters of the gait cycle occurs in the transition from normal walking to running?
Explanation
Examination of a 5-year-old child who has fibular hemimelia reveals the foot has two rays and is stiff in equinus and valgus. The level of the foot is just proximal to the midshaft of the contralateral tibia, and the knee has full active flexion and extension, but slight valgus. Treatment should include
Amputation through the midshaft of the tibia
Correction of the foot deformity and lengthening with a ring fixator
Knee disarticulation
Ankle disarticulation
Ankle disarticulation and contralateral epiphyseodesis of the proximal tibia Answer: 4
Congenital absence of the fibula, also called fibula hemimelia, has several manifestations. These range from complete absence of the fibula with missing lateral rays of the foot (i.e. terminal longitudinal deficiency) to absence of only a portion of the fibula without foot involvement (i.e. intercalary longitudinal; deficiency). Congenital fibular deficiency usually occurs sporadically without a known cause. The child with complete absence of the fibula presents clinically with an anterolateral bow of the tibia, an equinovalgus deformity of the foot, and a tarsal coalition. The talotibial joint is usually malformed, with the fused talocalcaneus having a flat upper surface that articulates with the tibia in a valgus and equinus position. The foot may be missing one or two lateral rays. There is always significant shortening of the epsilateral femur. Treatment: There is a reasonable consensus that complete fibular hemimelia is best treated by performing an ankle disarticulation in early childhood and fitting a Syme-type prosthesis. Children with lesser (<5cm) at birth may be a candidate for lengthening procedures, but the exact indications and results of these procedures have not been well defined. Children with large discrepancies (>5cm) at birth and those with major foot deformities are better managed with amputation.
Question 29
Which of the following therapies has a direct anabolic effect on bone?
Explanation
Question 30
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
REFERENCES: Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362.
Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307.
Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 31
Which nerve is most commonly injured after total knee arthroplasty?
Explanation
The tibial or peroneal nerves usually are not injured during total knee arthroplasty. Incidence of peroneal nerve damage is highest in knees with a valgus deformity and an associated flexion contracture attributable to nerve stretch. This nerve injury occurs in as many as 9% of patients undergoing knee arthroplasty. Tibial nerve injury is a rare occurrence and usually an iatrogenic transection injury. The infrapatellar branch of the saphenous nerve and its nerve plexus is commonly injured after the medial parapatellar approach, and altered sensation attributable to injury is reported in up to 70% of cases. Injury typically manifests as numbness inferior to the patella. The sartorial branch of the saphenous nerve provides sensation distal to the knee and is uncommonly injured with a medial parapatellar approach. These concepts are illustrated in video 57, “Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition.”
RECOMMENDED READINGS
Clarke HD, Bush-Joseph CA, Wolf BR. Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition [DVD]. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2012.
Hunter LY, Louis DS, Ricciardi JR, O'Connor GA. The saphenous nerve: its course and importance in medial arthrotomy. Am J Sports Med. 1979 Jul-Aug;7(4):227-30. PubMed PMID: 474860.View Abstract at PubMed
Mistry D, O'Meeghan C. Fate of the infrapatellar branch of the saphenous nerve post total knee arthroplasty. ANZ J Surg. 2005 Sep;75(9):822-4. PubMed PMID: 16174002.View Abstract at PubMed
Schinsky MF, Macaulay W, Parks ML, Kiernan H, Nercessian OA. Nerve injury after primary total knee arthroplasty. J Arthroplasty. 2001 Dec;16(8):1048-54. PubMed PMID: 11740762.View Abstract at PubMed
Question 32
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 33
A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes an uncomplicated closed reduction under sedation in the emergency department. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, the patient has persistent pain at rest and forward elevation and external rotation weakness, but the remaining motor function in the extremity and sensation are intact. What is the best next step?
Explanation
modalities do not adequately address the concern over his potential for having sustained a rotator cuff tear.
Question 34
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
Explanation
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
Question 35
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 36
- A patient sustained a joint depression-type fracture of the calcaneus that healed despite lack of treatment. The loss of dorsiflexion the patient is now experiencing is most likely the result of
Explanation
Question 37
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
Explanation
REFERENCES: Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
Question 38
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of
Explanation
not indicated.
REFERENCES: Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Question 39
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
Explanation
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. View Abstract at PubMed Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. View Abstract at PubMed
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
Question 40
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
REFERENCES: Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 41
Following its exit from the sciatic notch, the sciatic nerve passes between what two muscles?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 335-348.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Williams,
1978, Figure 4-34.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 42
Figure 51 shows the standing AP radiograph of a 56-year old woman who has multiple toe deformities and pain beneath the metatarsal heads. Shoe modification has failed to provide relief. In addition to correction of the proximal interphalangeal joint deformities, surgical treatment should consist of
Explanation
A modification was then used that maintained the proximal phalangeal bases and used K-wires to fixate the MTP arthroplasty and IP joints which resulted in improved cosmetic result and simplified post-op management. Equal results were seen w/ no increase in recurrence or complications.
Question 43
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
Explanation
REFERENCE: Glassman SD, Anagnost SC, Parker A, et al: The effect of cigarette smoking and smoking cessation on spinal fusion. Spine 2000;25:2608-2615.
Question 44
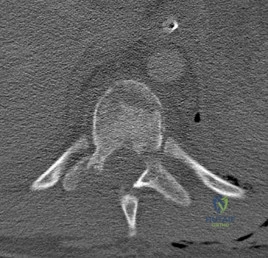
A B Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
Explanation
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.View Abstract at PubMed
Question 45
What structure provides the major blood supply to the humeral head?
Explanation
the major blood supply to the humeral head. The posterior circumflex humeral artery
supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Cushner MA, Friedman RJ: Osteonecrosis of the humeral head. J Am Acad Orthop Surg 1997;5:339-346.
Question 46
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 47
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management? Review Topic

Explanation
Question 48
From which artery does the princeps pollicis artery branch?
Explanation
The princeps pollicis artery can be located on the palmar aspect of the adductor pollicis and emerges into the subcutaneous tissue at the thumb metacarpophalangeal flexion crease. It branches from the radial artery just distal to the location of the deep palmar arch.
RECOMMENDED READINGS
Coleman SS, Anson B: Arterial patterns in the hand based on a study of 650 specimens. Surg Gynec Obstet 1961;4:409-424.
Ames EL, Bissonnette M, Acland R, Lister G, Firrell J. Arterial anatomy of the thumb. 78 J Hand Surg Br. 1993 Aug;18(4):427-36. PubMed PMID: 8409651. View Abstract at PubMed
Question 49
A 30-year-old man has had a slowly enlarging mass on the plantar medial aspect of the foot for the past 6 months. The mass is now 1 cm in diameter, adherent to the plantar fascia, and painful with weightbearing. The overlying skin is mobile. Management at this time should consist of
Explanation
Question 50
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 51
A 36-year-old man sustains blunt chest trauma, an open right femur fracture, and a closed left tibia fracture following a high-speed MVC. Upon presentation to the emergency room, blood pressure is 80/40, HR 135, and urine output is .4 cc/kg/hr. Fluids and blood products are administered, and the patient is transferred to the ICU for further care. Which of the following indicates adequate resuscitation has been achieved?

Explanation
Shock is an abnormality of the circulatory system that results in inadequate organ perfusion and tissue oxygenation. This leads to anaerobic metabolism with the development of lactic acidosis and oxygen debt. Shock is either classified as compensated or uncompensated. Compensated shock exists when there is evidence of ongoing inadequate tissue perfusion despite the normalization of blood pressure, heart rate, and urine output. Uncompensated shock occurs when there is inadequate tissue perfusion and abnormal blood pressure, heart rate, and urine output. Thus, a patient may have normal vital signs but still be in a state of compensated shock that requires additional resuscitation.
Porter et al. review the optimal end points of resuscitation in trauma patients. They conclude that using traditional end points such as blood pressure, urine output and heart rate, may leave up to 85% of patients in "compensated" shock. They urge the use of lactate, base deficit, and gastric intramucosal pH as appropriate end points of resuscitation.
Roberts et al. discuss various aspects of damage control orthopaedics in the multiply injured trauma patient. Although they do not discuss the end points for resuscitation, they note that they presence of shock is a clinical parameter associated with adverse outcomes in the trauma patient.
Incorrect answers:
Question 52
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 53
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
REFERENCE: Benassi MS, Magagnoli G, Ponticelli F, et al: Tissue and serum loss of metalloproteinase inhibitors in high grade soft tissue sarcomas. Histol Histopathol 2003;18:1035-1040.
Question 54
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
Question 55
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
Question 56
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?
Explanation
REFERENCES: Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systemic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956.
Edwards TB, Kadakia NR, Boulahia A, et al: A comparison of hemiarthroplasty and total shoulder arthroplasty in the treatment of primary glenohumeral osteoarthritis: Results of a multicenter study. J Shoulder Elbow Surg 2003;12:207-213.
Gartsman GM, Roddey TS, Hammerman SM: Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. J Bone Joint Surg Am 2000;82:26-34.
Question 57
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?

Explanation
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p < 0.01, respectively), lower nonunion (2 vs. 7, p=0.042) & lower malunion (0 vs. 9, p=0.001). Surgery resulted in quicker radiographic union (16.4 weeks vs. 28.4 weeks, p=0.001). However, 15% had hardware and wound complications. At one year, the operative group was more likely to be satisfied with the shoulder in general (p=0.002) and the appearance of the shoulder in particular (p=0.001) in comparison to the nonoperative group.
Prior studies have shown that greater than 2cm of shortening treated non-operatively results in increased fatigueability and poor outcome, but not necessarily nonunion. The Lazarides article concluded that “Final clavicular shortening of more than 18 mm in male patients and of more than 14 mm in female patients was significantly associated with an unsatisfactory result.”
Studies have shown no difference in outcome when treated with a Figure-of-8 harness compared to a simple sling
Question 58
What acetabular procedure for developmental dysplasia of the hip does not require a concentric reduction of the femoral head in the acetabulum?
Explanation
REFERENCES: Staheli LT, Chew DE: Slotted acetabular augmentation in childhood adolescence. J Pediatr Orthop 1992;12:569-580.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 618-650.
Question 59
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 60
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?

Explanation
DISCUSSION: A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
Question 61
A 29-year-old male sustained a mid-shaft femur fracture in a motor cycle accident. Even if asymptomatic, what additional radiographs must be obtained either preoperatively or intraoperatively before performing intramedullary nailing of the femoral shaft fracture?

Explanation
Question 62
Figure 26 is the radiograph of a 33-year-old woman who was involved in a high-speed motor vehicle crash. Her initial blood pressure is 80/50 mm Hg and she has a pulse rate of 120 bpm. After hemodynamic stabilization and temporizing measures have been performed, the patient is cleared for surgery. What is the most appropriate method of definitive fixation?

Explanation
Question 63
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches
Explanation
REFERENCES: Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000.
Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Gilliland MD, Ward RE, Barton RM, et al: Factors affecting mortality in pelvic fractures.
J Trauma 1982;22:691-693.
Question 64
All of the following are considered contraindications to the use of functional bracing of a humeral shaft fracture EXCEPT:

Explanation
Commonly accepted parameters for closed treatment include less than 30 degrees of varus angulation, 20 degrees of anterior/posterior angulation, and 3 cm of shortening. Operative indications are: associated vascular injuries, bilateral humeral shaft fractures, polytrauma patient (including paraplegia), segmental fractures, injury to the brachial plexus, pathological fractures, floating elbow, and floating shoulder.
The article by Rutgers and Ring found that proximal one-third oblique humeral shaft fractures had an unacceptably high 29% rate of nonunion treated with a functional brace.
The article by Sarmiento et al found a 97% rate of union, a radial nerve palsy incidence of 11%, and no contraindication to the use of functional braces in humeral shaft fractures associated with radial nerve palsy.
The review article by Defranco and Lawton states that 70% of these radial nerve injuries recover spontaneously. They note that it "seems reasonable, however, to consider surgical intervention (radial nerve exploration) between 4 and 6 months based on the patient’s clinical course."
Question 65
Video 1 shows a 20-year-old right-hand dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?
Explanation
A. Abductor pollicis longus reconstruction with palmaris autograft
B. Extensor pollicis brevis repair
C. Extensor pollicis longus (EPL) repair
D. Extensor indicis proprius (EIP) to extensor pollicis longus tendon transfer
The EPL is the only tendon that will lift a thumb off of a table as described. It is the most frequently ruptured tendon associated with distal radius fractures. Rupture is more common with nondisplaced fractures. Rupture after a nondisplaced or minimally displaced fracture suggests an ischemic etiology. The patient will not be able to lift her thumb off of a table with her hand lying flat, palm-down. Direct repair is often difficult because of retraction of tendon ends, atrophy, and fraying. The EIP has a similar amplitude and direction of pull. Prerequisites for the use of the EIP to EPL tendon transfer include independent extension of the index finger.
15- Figure 1 is the clinical photograph of a very functional 17-year-old boy with cerebral palsy and quadriplegia. He has no active supination but has full passive supination. His ability to determine position and sensibility without visual input are good. Radiographs show no osseous malalignment. Which treatment can best improve this patient's function?
A. Physical therapy for supination strengthening
1- Figures 1 through 3 are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?
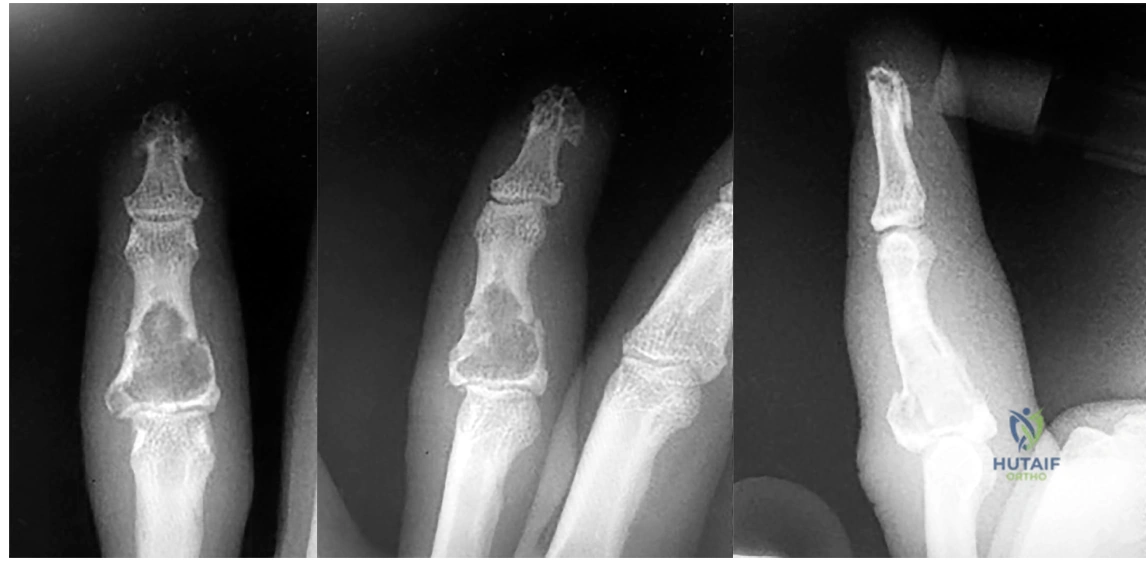
A. Observation only
B. Fluoroscopic-guided intralesional steroid injection followed by serial radiographs
C. Immediate curettage without bone grafting
D. Splint immobilization with curettage and possible grafting after the fracture has healed
This patient has a fracture of the middle phalanx attributable to the presence of an enchondroma. Enchondromas are the most common benign bone tumor affecting the hand. This particular enchondroma has thinned the cortices extensively so that even minor trauma can cause a pathologic fracture. Observation is not the best treatment because a fracture is present, and, at a minimum, the digit should be immobilized.
Question 66
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
Explanation
REFERENCES: Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Field LD, Savoie FJ: Common elbow injuries in sport. Sports Med 1988;26:193-205.
Wilson FD, Andrews JR, Blackburn TA, et al: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 67
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
REFERENCE: Murphy S, Deshmukh R: Periacetabular osteotomy: Preoperative radiographic predictors of outcome. Clin Orthop 2002;405:168-174.
Question 68
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 69
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 70
A 16-year-old right-hand dominant male pitcher has had increasing pain in his dominant shoulder for the past 6 months without treatment. A coronal T2-weighted MRI scan is shown in Figure 80. What is the most appropriate treatment plan? Review Topic

Explanation
Question 71
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
REFERENCE: Mancini F, Landolfi C, Muzio M, et al: Acetaminophen down-regulates interleukin-1beta-induced nuclear factor-kappaB nuclear translocation in a human astrocytic cell line. Neurosci Lett 2003;353:79-82.
Question 72
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice.
REFERENCES: Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 73
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Baumhauer JF: Superficial peroneal nerve entrapment. Foot Ankle Clin 1998;3:439-446.
Question 74
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
Explanation
REFERENCES: Gibson JN, Waddell G: Surgery for degenerative lumbar spondylosis: Updated Cochrane Review. Spine 2005;30:2312-2320.
Fritzell P, Hagg O, Wessberg P, et al: 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-2532.
Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 75
What is the correct order of the elastic modulus of the following materials from greatest to least?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 182-215.
Brinker MR: Basic science section 8: Biomechanics and biomaterials, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 120-123.
Question 76
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
REFERENCES: Sady SP, Wortman M, Blanke D: Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil 1982;63:261-263.
Tanigawa MC: Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys Ther 1972;52:725-735.
Wallin D, Ekblom B, Grahn R, Nordenberg T: Improvement of muscle flexibility: A comparison between two techniques. Am J Sports Med 1985;13:263-268.
Question 77
- A 14-year-old patient who has homocystinuria and is Risser 3 is referred for surgical treatment of scoliosis. In addition to the usual risks associated with posterior spinal fusion, the family should be advised that the patient ‘s underlying condition significantly increases the perioperative risk of
Explanation
1 and 2 are concerns during spinal fusion but are not specific to this disease. 4 may occur with homocystinuria but is not related to spinal fusion. 5 occurs with PSF in the younger population because of the growth potential remaining.
Question 78
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
Explanation
REFERENCES: Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695.
Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 79
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 80
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
REFERENCES: Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20.
Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Solomonow M, Baratta R, Zhou BH, et al: The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 1987;15:207-213.
Question 81
Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?
Explanation
Titanium is a material that is light, highly ductile, strong and corrosion resistant. However, titanium has poor wear resistance and is notch sensitive. It is commonly used as an orthopaedic implant materials because it has torsional and axial stiffness (moduli) that most closely mimics bone. Young’s modulus is constant and different for each material and represents the material's ability to maintain shape under external loading.
Rho et al found that the average Young's modulus for trabecular bone measured ultrasonically and mechanically was 14.8 GPa (S.D. 1.4) and 10.4 (S.D. 3.5), respectively. The average Young's modulus of microspecimens of cortical bone measured ultrasonically and mechanically was 20.7 GPa (S.D. 1.9) and 18.6 GPa (S.D. 3.5), respectively.
Illustration A depicts a stress vs. strain curve. The slope of the line in the elastic zone represents the Young Modulus of Elasticity.
Incorrect Answers:
Question 82
A 27-year-old man has recurrent anterior shoulder instability following an arthroscopic Bankart repair 4 years ago. Current CT scans are shown in Figures 19a and 19b. Deficiency of what mechanism is most likely to contribute to the current joint instability? Review Topic

Explanation
Question 83
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Explanation
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 84
Figures 1 through 3 are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?

Explanation
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal
row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
Question 85
A 15-year-old boy with epilepsy who is treated with phenytoin sustains a vertebral compression fracture during a breakthrough seizure. Radiographs of the spine reveal generalized osteopenia. What is the most likely cause of the osteopenia?
Explanation
REFERENCE: Chung S, Ahn C: Effects of anti-epileptic drug therapy on bone mineral density in ambulatory epileptic children. Brain Dev 1994;16:382-385.
Question 86
Which of the following diagnostic studies best distinguishes Ewing’s sarcoma from small cell osteosarcoma?
Explanation
REFERENCES: Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498.
Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing’s sarcoma family. Eur J Cancer 2003;39:19-30.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 87
Primary chondrosarcoma of bone most commonly occurs in which of the following locations?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Simon M, Springfield D, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 88
-Figures a and b are the MRI scans of the cervical spine without contrast of a 38-year-old man with neck pain radiating into the right upper extremity for the past 4 weeks. He denies numbness or weakness.Examination was significant for reproduction of pain going down the right arm with neck extension and right lateral rotation. What is the next treatment step?
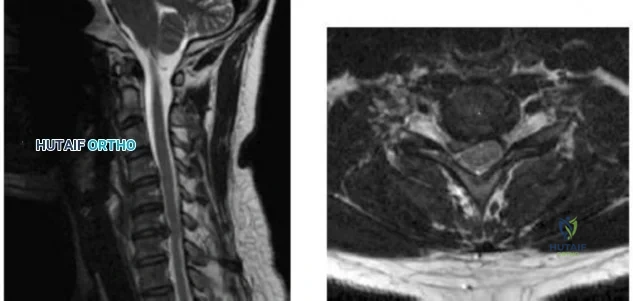
Explanation
Question 89
A 52-year-old woman slips in her bathroom and strikes her right hand on a cabinet. She notes swelling, ecchymosis, and pain with attempted motion. There are no open wounds. Radiographs are shown in Figures 5a through 5c. What is the most appropriate treatment?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 90
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ,
Ciba-Geigy, 1991, vol 8, p 53.
Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA,
Harper and Row, 1982, vol 3, pp 428-429.
Question 91
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
REFERENCES: Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238.
Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Fisher DA, Kiley K: Constrained acetabular cup disassembly. J Arthroplasty 1994;9:325-329.
Question 92
What is the goal of surgical treatment in this scenario?
Explanation
This patient has a metastatic neuroendocrine tumor. Surgical treatment should prioritize palliation of her symptoms. She has high-grade spinal cord compression without neurologic signs or symptoms. Steroids are beneficial for patients with high-grade spinal cord compression caused by tumors, and these drugs should be administered in the acute setting. This patient was appropriately initially treated with conventional radiation. However, she is not a candidate for further radiation because of spinal cord tolerance limits and insufficient clearance between the tumor and spinal cord. Consequently, stereotactic radiation is not an option.
The goal of surgical treatment of this tumor should be palliation of her symptoms rather than cure. A costotransversectomy approach offers the advantage of ventral and dorsal spinal cord access, which is necessary in this case. A sternotomy or transthoracic approach would offer ventral access, but dorsal access would be less than optimal.
RECOMMENDED READINGS
Rose PS, Buchowski JM. Metastatic disease in the thoracic and lumbar spine: evaluation and management. J Am Acad Orthop Surg. 2011 Jan;19(1):37-48. Review. PubMed PMID: 21205766.View Abstract at PubMed
Rades D, Abrahm JL. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol. 2010 Oct;7(10):590-8. doi: 10.1038/nrclinonc.2010.137. Epub 2010 Aug
Question 93
A teenage female is referred to you for evaluation of curvature in her back that was discovered on routine school screening. She is diagnosed with adolescent idiopathic scoliosis. In which of the following scenarios is a bracing program the most appropriate treatment? Review Topic

Explanation
The treatment of adolescent idiopathic scoliosis (AIS) depends on the magnitude and location of curve as well skeletal maturity of the patient. For curves less than 20 degrees, observation is appropriate until skeletal maturity, with closer intervals during
times of peak growth. Curves between 20-25 and 45 degrees in patients who are Risser stage 0,1 or 2 are best treated with bracing to stop progression. Curves with an apex at T7 or below are typically treated with a Boston brace. Curves over 50 degrees generally warrant a discussion about surgery to prevent progression past maturity.
In a landmark study, Weinstein et al. evaluated both a randomized and preference based cohort of bracing versus observation. The trial was stopped early due to efficacy of bracing. The rate of treatment success was 72% after bracing and 48% after observation. Treatment success was strongly correlated to time of brace wear.
Schlenzka et al. reviewed indications, treatment, and complications associated with brace treatment of AIS. They state that further evidence is necessary to evaluate the efficacy of bracing in AIS.
Figure 1, 2, and 3 are radiographs depicting Risser stage 0, 1, and 4 respectively. Illustration B shows radiographs of all Risser stages. Illustration C is the Lenke classification system for idiopathic scoliosis.
Incorrect Answers:
Question 94
A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm 3 (normal 3,500 to 10,500/ mm 3 ) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 95
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?
Explanation
REFERENCE: Simon M, Springfield D, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 200.
Question 96
A 69-year-old woman is seen in the emergency department with a bilateral C5-6 facet dislocation and complete quadriplegia after falling down a flight of stairs. After initial evaluation and treatment by the trauma service, she is moved to the intensive care unit. Examination reveals a blood pressure of 90/50 mm/Hg, a pulse rate of 50/min, a respiration rate of 12/min, and urine output of 1 mL/kg/h. Her hemodynamic status should be addressed by
Explanation
output suggests proper fluid resuscitation. Instead, she is bradycardic, possibly indicating neurogenic shock and loss of sympathetic tone to the heart. A Swan-Ganz catheter should be used to help differentiate these problems and guide appropriate fluid resuscitation and use of vasopressor agents.
REFERENCES: Hadley MN: Management of acute spinal cord injuries in an intensive care unit or other monitored setting. Neurosurgery 2002;50:S51-S57.
Vaccaro AR, An HS, Betz RR, et al: The management of acute spinal trauma: Prehospital and in-hospital emergency care. Instr Course Lect 1997;46:113-125.
Question 97
During the implantation of a cementless acetabular component in total hip arthroplasty, placement of a screw in the anterior superior quadrant puts which of the following structures at risk for damage?
Explanation
REFERENCES: Keating EM, Ritter MA, Faris PM: Structures at risk from medially placed acetabular screws. J Bone Joint Surg Am 1990;72:509-511.
Wasielewski RC, Cooperstein L, Kruger MP, Rubash HE: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am
1990;72:501-508.
Question 98
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 99
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
REFERENCES: Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 100
Video 1 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?
Explanation
Upon examination, this patient is exhibiting dislocation of the ECU tendon because of a disrupted sheath. He has failed nonsurgical measures, so surgery that would involve either direct repair or reconstruction of the tendon sheath is indicated. An option for reconstruction is to use a portion of the extensor retinaculum as a sheath substitute. Deepening of the ECU tendon groove at the distal ulna with direct repair of the sheath is another option, although a 2016 paper by Ghatan and associates did not find depth of the groove as a risk factor for subluxation. TFCC repair, lunotriquetral fusion, and DRUJ tenodesis are not appropriate because the examination clearly shows ECU tendon dislocation. TFCC and lunotriquetral ligament tears can occur along with ECU tendon dislocation, but no other examination findings suggest these conditions for this patient.
