Orthopedic Board Review MCQs: Hip Arthroplasty, Elbow & Spine | Part 209

Key Takeaway
This page offers Part 209 of an interactive orthopedic surgery board review quiz. Featuring 100 high-yield MCQs by Dr. Hutaif, it's designed for orthopedic residents and surgeons preparing for their AAOS and OITE certification exams. It provides authentic clinical scenarios and detailed explanations.
About This Board Review Set
This is Part 209 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 209
This module focuses heavily on: Arthroplasty, Elbow, Hip, Nerve, Tendon.
Sample Questions from This Set
Sample Question 1: A right-hand-dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted for...
Sample Question 2: Analysis of primary total hip arthroplasty using press-fit acetabular components without supplementary screw fixation reveals that screw fixation...
Sample Question 3: What is the most common maxillofacial/dental injury in ice hockey?...
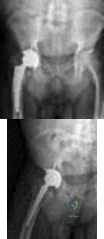
Sample Question 4: Figures below demonstrate the radiographs obtained from a 63-year-old man who had right total hip arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical act...
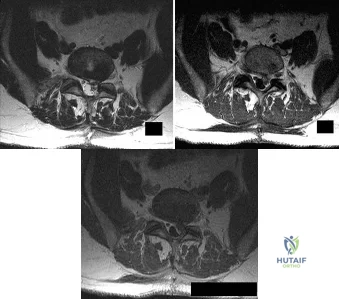
Sample Question 5: A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted M...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A right-hand-dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
the radial tuberosity.
Question 2
Analysis of primary total hip arthroplasty using press-fit acetabular components without supplementary screw fixation reveals that screw fixation
Explanation
REFERENCE: Udomkiat P, Dorr LD, Wan Z: Cementless hemispheric porous-coated sockets implanted with press-fit technique without screws: Average ten-year follow-up. J Bone Joint Surg Am 2002;84:1195-1200.
Question 3
What is the most common maxillofacial/dental injury in ice hockey?
Explanation
displacement of the tooth from aleveolar support. A crown fracture is an incomplete loss or fracture of the tooth enamel without loss of the tooth. The other injuries (mandible fracture, lip laceration, tooth
avulsion, and temporomandibular contusion) occur but are not nearly as common.
REFERENCES: Lahti H, Sane J, Ylipaavalniemi P: Dental injuries in ice hockey games and training. Med Sci Sports Exerc 2002;34:400-402.
Minkoff J, Stecker S, Varlotta GP, et al: Ice hockey, in Fu FH, Stone DA (eds): Sports Injuries, ed 2.
Philadelphia, PA, 2001, pp 516-517.
Question 4
Figures below demonstrate the radiographs obtained from a 63-year-old man who had right total hip arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals a normal gait and painless range of motion with flexion of 70°, extension of 0°, internal rotation of 20°, external rotation of 20°, abduction of 10°, and adduction of 10°. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
Explanation
Question 5
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the patient's symptoms? Review Topic
Explanation
Question 6
Which of the following is considered a contraindication to the use of a reverse total shoulder arthroplasty? Review Topic
Explanation
Question 7
- The lateral fragment of bone (Segond fracture) associated with an injury of the anterior cruciate ligament is the result of an avulsion of the
Explanation
Question 8
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 9
The development of complex regional pain syndrome (CRPS) following distal radius fracture is associated with what factor?
Explanation
CRPS is an uncommon complication following distal radius fractures; its incidence is reported to range between 1% and 37%. Two recent studies have evaluated for risk factors in the development of CRPS following distal radius fractures. Female gender, concomitant fracture of the distal ulna, and surgical treatment were all associated with an increased likelihood of CRPS, as was fibromyalgia. Older age was identified as conferring both an increased and a decreased risk for CRPS in the two studies.
Question 10
Figures 54a and 54b are the radiographs of a 23-year-old man who fell from a height and sustained an isolated injury to his right leg. Which of the following is a useful surgical technique to optimize alignment during intramedullary nailing?

Explanation
(SBQ12TR.65) A patient falls and sustains the isolated injury seen in Figures A and
B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?

Full pronation
25 degrees pronation
Neutral
25 degrees supination
Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial
head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with < 3 fragments. Radial head replacement is considered for comminuted fractures (Mason Type III) with 3 or more fragments.
Cheung et al. reviewed the surgical approaches to the elbow. The lateral approach (Kocher or Kaplan) is most commonly used with these injuries. The Kocher approach utilizes the intramuscular plane between anconeus and extensor carpi ulnaris. Kaplan utilizes the plane between extensor digitorum commons and extensor carpi radialis brevis.
Figure A and B show AP and lateral radiographs of the left elbow. There is a displaced radial head fracture. Illustration A shows a schematic diagram of the radial head "safe zone" between the radial styloid to Lister's tubercle.
Incorrect Answers:
Question 11
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of
Explanation
REFERENCES: Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655.
Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 12
No fractures were identified and the patient was treated nonsurgically in a range-of-motion brace. Two months later, he continued to experience elbow pain and was unable to return to sports. He regained motion and strength with physical therapy, there was no gross instability with varus or valgus testing, and he had a negative moving-valgus stress test. The orthopaedic surgeon performed an examination under anesthesia in the operating room (Video 54). Which anatomic structure is injured?
Explanation
Ninety percent of elbow dislocations occur in a posterolateral direction. O’Driscoll and associates described the mechanism of injury in posterolateral elbow dislocations in 1992, reporting that they occur most typically after a fall onto an outstretched arm. As the arm hits the ground it causes axial compression, forearm supination, and valgus load across the elbow. The triceps fires, pulling the olecranon posterior; the forearm supinates while simultaneous shoulder internal rotators fire; and the elbow falls into valgus. These 3 mechanisms cause the elbow to subluxate and dislocate posterolaterally. The elbow is most stable following posterolateral dislocation in a flexed and pronated position. The elbow is least stable in extension and supination. Simple dislocation often can be treated nonsurgically, while fracture dislocation will usually necessitate surgical intervention. The video shows the elbow pivot-shift test, which evaluates for posterolateral rotatory instability. A positive test finding elicits apprehension and, in this case, radial head subluxation and confirms an insufficient lateral UCL.
Question 13
Figure 37a is the initial radiograph of a 7-year-old boy who fell from monkey bars 4 hours ago. He has intact motor function in his fingers and normal capillary refill, but his radial pulse is not palpable. Figures 37b and 37c are the radiographs following closed reduction and pinning. This boy’s hand and fingers remain pink, but his radial pulse remains nonpalpable. What is the best next step?
Explanation
Figure 37a shows a completely displaced supracondylar humerus fracture. The first step in the situation described, which involves a pink pulseless hand, is to perform an urgent closed manipulation and pinning. The vascular examination should be reassessed following the reduction. When adequate reduction has been achieved and the pulse remains nonpalpable but the hand is pink and capillary refill is normal, the fracture may be splinted and the patient observed closely in the hospital. Arteriography is not useful and may delay revascularization or increase vessel spasm. Although some investigators have concluded that exploration of the brachial artery may be indicated, the algorithm that includes observation only is the most supported and the most commonly practiced treatment. The radiographs show adequate reduction and fixation without medial widening at the fracture site, which might indicate a site of brachial artery entrapment. Therefore, pin removal and fracture rereduction is not indicated.
RESPONSES FOR QUESTIONS 38 THROUGH 45
Sclerosis of the proximal femoral epiphysis with subchondral lucency
Abnormal femoral head-neck junction offset
Widening of the proximal femoral physis with normal femoral head-neck junction offset
Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
Question 14
A 65-year-old man has had “catching” in front of his knee since he had a total knee arthroplasty 9 months ago. Examination reveals a palpable and audible snap in the anterior aspect of the knee at about 40 degrees of flexion as the knee is being actively extended. A radiograph of the prosthetic knee will most likely show
Explanation
Pathologically, the clunk is produced by a suprapatellar fibrous nodule seen superior to the patellar component at re-operation. This nodule has been seen to catch in the intercondylar notch in primarily first generation TKAs. Current component designs have decreased this phenomenon through better engineering of femoral components. Treatment is by arthroscopic debridement or open arthroplasty resection. The nodule may be recurrent.
Question 15
Triple arthrodesis in a reduced position
Explanation
Question 16
The cavovarus deformity associated with Charcot-Marie-Tooth (CMT) disease is caused by which of the following?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-143.
Charcot-Marie-Tooth Disease (CMT) Penn State Hershey Medical Center.
www.hmc.psu.edu/healthinfo/c/cmt.htm
Question 17
- Which of the following is considered an advantage of an unreamed intramedullary nail over a reamed intramedullary nail?
Explanation
Question 18
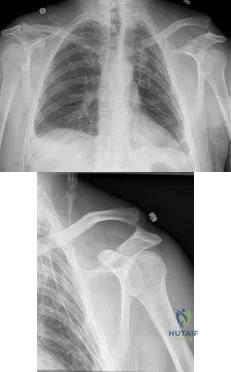
A 50-year-old man fell from a ladder onto his left shoulder and sustained the injury shown in the radiographs in Figures 71a and 71b. He underwent surgery with repair of the coracoclavicular ligaments and deltotrapezial fascia with coracoclavicular screw placement. Which of the following statements regarding postoperative complications is most accurate? Review Topic
Explanation
Question 19
Figures 1 and 2 are radiographs of a 25-year-old man who has had persistent right hip pain for over a year. There was an acute injury and the pain has progressively worsened and is now 9/10 in severity. The pain interferes with activities of daily living and the patient's capacity to participate in sports. The patient has failed nonsurgical treatment in the form of physical therapy and activity modification. On physical examination, forward flexion is limited to 90°, internal rotation is limited to 10°, and flexion adduction internal rotation examination is positive. The hip pain was relieved on physical examination after intra-articular administration of local anesthetic. The patient had an MRI and CT scan. What is the most appropriate surgical option?
Explanation
A. Belly press
B. Hornblower's test
C. External rotation strength
D. Empty can test
A fall on an outstretched upper extremity can commonly result in a traumatic rotator cuff tear. The images require appropriate interpretation of an acute subscapularis tendon rupture with medial subluxation of the biceps tendon. Subscapularis tendon tears result in a positive belly press or lift-off test. Hornblower's tests for external rotation strength with the arm abducted 90° (teres minor weakness). Empty can tests supraspinatus strength. External rotation strength with the arm at the side tests for infraspinatus weakness.
38- Videos 1 and 2 are the coronal plane MRI scan and arthroscopic evaluation of a 48-year-old woman with 2 weeks of posterior knee pain after feeling a “pop” in the knee while climbing stairs. Physical examination reveals passive range of motion of +5° to 120°, with pain limiting her in terminal extension. Failure of surgical repair of the injured structure is most associated with
A. poor vascularity of the injured tissue.
B. BMI >35 kg/m^2.
C. valgus alignment >5°.
D. repair technique. 30
The MRI scan and surgical video are showing an example of a posterior medial meniscal root tear/avulsion. Many studies have shown successful treatment of these tears with repair using various techniques and minimal progression to osteoarthritis (OA). Most studies exclude patients with high BMI. Brophy and associates demonstrated in their series that high BMI was associated with higher rates of clinical OA and need for subsequent surgery.
Multiple studies in the literature demonstrate good results with a variety of techniques. A valgus alignment in this setting would be considered protective, as opposed to a varus alignment >5°, which has also been associated with worse outcomes. The vascularity of the meniscus is consistently poor throughout most of its volume, including the root, and is not considered to be significantly different from person to person and should affect all root repairs equally.
39- A 47-year-old man who is an avid tennis player and laborer has had one year of shoulder pain and weakness. His pain occurs at night and radiates to the deltoid laterally. The patient denies any anterior based pain. He reports no prior surgeries and has been managed with steroid injections and physical therapy. On examination, he has full passive motion with significant weakness with external rotation. His neurologic examination is unremarkable. MRI evaluation reveals a posterior- superior rotator cuff tear with Goutallier grade 4 fatty infiltrate in the supraspinatus and infraspinatus with retraction beyond the glenoid. He is concerned about the lack of rotation of his arm and reports that this disability creates significant disability with his occupation as a mason. What is the best next step?
A. Shoulder arthroscopy and subacromial decompression
B. Tendon transfer
C. Total shoulder arthroplasty
D. Reverse total shoulder arthroplasty
In younger active patients, tendon transfer is considered a preferable treatment option. The patient has failed a course of nonoperative management. Subacromial decompression may offer pain relief but may not be advisable in a patient with rotator cuff deficient shoulder. A total shoulder arthroplasty requires functionality of the supraspinatus and infraspinatus. A reverse total shoulder is an option to alleviate pain and perhaps improve forward flexion height and strength; however, reverse arthroplasty would not improve external rotation in this patient, and there is concern for longevity of the implant in younger patient populations.
40- A multicenter prospective study of 7,500 patients that assesses differences in rerupture rates after anterior cruciate ligament (ACL) reconstruction using hamstring autograft shows a decreased rate of rerupture when the graft diameter is >9.0 mm versus <9.0 mm (p = 0.05). A follow-up study done at a single institution of 200 patients fails to show any difference in rerupture rates based upon graft size. If the multicenter trial is assumed to be accurate, which statistical error occurred in the follow-up study?
A. Type-I error
B. Type-II error
C. Selection bias
D. Alpha error
Type-II errors, or beta errors, occur when the null hypothesis is accepted and should have been rejected. An underpowered study is at risk of this type of error. Power is defined as 1-probability of a type-II (beta error), and this is generally set at a level of 80% for most studies. The type-II error occurs when a study concludes that there is no association between the studied variables when in fact one exists. The type-I error, or alpha error, is defined as rejecting the null hypothesis when it should have been accepted. Alpha errors occur when a study suggests an association does exist when in reality it does not. Selection bias occurs when proper randomization is not achieved and therefore, the study cohort is not representative of the population intended to be analyzed.
41- A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). A 60-degree anteromedialization is planned to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
A. Grade III chondrosis of the proximal patella
B. Caton-Deschamps ratio of 1:1
C. Tibial tubercle-trochlear groove (TT-TG) distance of 21 mm
D. Q angle of 17°
TO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and
medialize the tubercle. This will consistently result in a change of 32
patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.
42- During preseason training camp, a 23-year-old football player comes to the sideline complaining of nausea, dizziness and headache after a 2- mile run. Vital signs include blood pressure 110/80, heart rate 115 bpm and core body temperature of 39°C (102°F). He is otherwise alert and oriented. What is the recommended initial treatment?
A. Immediate ice water bath immersion
B. Immediate return to training
C. Rehydration with a carbohydrate- electrolyte beverage
D. Emergent transportation to a local emergency department
The patient has exertional heat exhaustion (EHE). In cases of exertional heat illness with elevated core body temperature, it is critical to differentiate between EHE and exertional heat stroke (EHS). Patients suffering from EHE often complain of dizziness, nausea, cramping and headache. Vital signs can show mild tachycardia and normal to low blood pressure. EHS is defined by elevated core body temperature >40°C (104°F) and organ failure. Rapid cooling is critical in the setting of EHS, but not EHE. In the setting of EHE, the patient should be placed in a cool, shaded area and given fluids. Studies suggest that the presence of carbohydrate (<8%) in combination with electrolytes mildly promotes fluid retention better than drinking water alone.
43- Surgical repair of the injury shown in the MRI scans in Figures 1 through 4 through a single-incision approach has a higher incidence of
Question 20
What is the greatest benefit of external fixation for treatment of displaced and unstable pelvic ring injuries with hemodynamic instability? Review Topic
Explanation
Question 21
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 22
Which of the following clinical disorders is the result of a mutation in fibroblast growth factor recepter 3 (FGFR3)?
Explanation
REFERENCES: Wagner T, Wirth J, Meyer J, et al: Autosomal sex reversal and camptomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell 1994;79:1111-1120.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
Dietz FR, Murray JC: Update on the genetic bases of disorders with orthopaedic manifestations, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 23
Which of the following foot deformities is commonly seen in patients with Charcot-Marie-Tooth disease? Review Topic
Explanation
Question 24
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
REFERENCES: Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
Scaduto AA, Cracchiolo A III: Lacerations and ruptures of the flexor or extensor hallucis longus tendons. Foot Ankle Clin 2000;5:725-736.
Question 25
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic
Explanation
Question 26
- Which of the following types of sarcoma of the bone is most sensitive to external beam radiation?
Explanation
Question 27
What is the next most appropriate step in the orthopaedic management of this patient?

Explanation
OrthoCash 2020
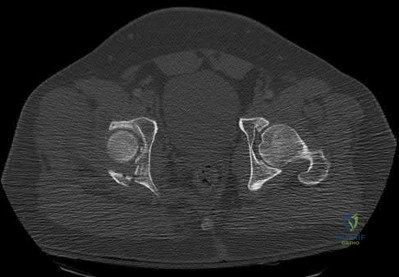
Which of the following findings best describes the acetabular fracture shown in Figure 38?
Posterior column with articular impaction and a free fragment
Anterior column with articular impaction
Posterior wall with an intra-articular fragment
Posterior wall with articular impaction and a free intra-articular fragment
Posterior wall with articular impaction Corrent answer: 4
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment.
OrthoCash 2020
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
normal sexual function and normal vaginal childbirth.
sexual dysfunction (dyspareunia) and normal vaginal childbirth.
normal sexual function and caesarean section childbirth.
sexual dysfunction (dyspareunia) and caesarean section childbirth.
normal sexual function and caesarean section childbirth until hardware removal.
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is
almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not.
OrthoCash 2020
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Closed treatment and casting
Open reduction and internal fixation
Primary subtalar arthrodesis
Percutaneous fixation
External fixation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures.
OrthoCash 2020
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Radial head resection, open reduction and internal fixation of the coronoid, and medial collateral ligament repair
Radial head resection and lateral collateral ligament repair
Radial head arthroplasty alone
Radial head arthroplasty and lateral collateral ligament repair
Radial head arthroplasty, open reduction and internal fixation of the coronoid, and lateral collateral ligament repair
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region.
OrthoCash 2020
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C).
What is the most appropriate management for the femoral shaft fracture at this point?
Reamed intramedullary nailing
Traction
External fixation
Open plating
Mast suit
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome.
OrthoCash 2020
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?

MRI scan
Physical examination
Workers’ compensation status
Surgeon availability
Patient age
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
OrthoCash 2020
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
Consult the ethics committee before giving blood.
Use cell saver blood.
Ask the patient’s family for consent to give blood.
Use plasma expanders.
Give the patient blood.
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah’s Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah’s Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open wound is not recommended nor would there likely be enough from an open pelvic fracture to salvage. The patient’s family may be expressing their own beliefs rather than the patient’s beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability.
OrthoCash 2020
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

talectomy.
reimplantation of the talus.
reimplantation of the talus with acute triple arthrodesis.
Syme amputation.
transtibial amputation.
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures.
OrthoCash 2020
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Spiral
Oblique
Transverse
Segmental
Comminuted
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism.
OrthoCash 2020
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?

Kocher-Langenbeck
Iliofemoral
Ilioinguinal
Extended iliofemoral
Triradiate approach
The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate
approaches although useful for this fracture, have a higher rate of complications.
OrthoCash 2020
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes

plating of the radial shaft fracture then open repair of the triangular fibrocartilage complex.
open reduction and internal fixation of the radius and ulna.
plating of the radius then closed reduction and evaluation of the distal radioulnar joint (DRUJ).
closed reduction of the radius and DRUJ.
plating of the radius then pinning of the DRUJ in pronation.
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
OrthoCash 2020
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?

Chronic osteomyelitis
Planovalgus hindfoot
Plantar nerve entrapment
Wound dehiscence
Painful hardware
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence.
OrthoCash 2020
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
A primed immune system with an increased risk of a systemic inflammatory response
Nothing since they are no longer in uncompensated shock and their vital signs have normalized
Higher nonunion rates after fracture fixation
Higher infection rates after definitive fracture fixation
Higher complication rates after temporizing external fixation of long bone fractures
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a “primed” immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered.
OrthoCash 2020
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is
intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?

Emergent four compartment fasciotomies
Emergent four compartment fasciotomies and open reduction and internal fixation of the fracture
Elevation of the limb overnight and four compartment fasciotomies in the morning
Elevation of the limb overnight and a recheck of compartment pressures in the morning
Emergent MRI of the knee and leg Corrent answer: 2
The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
OrthoCash 2020
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
The mean arterial blood pressure is above 90 mm Hg.
The pulse pressure has normalized.
Urine output is greater than 0.5 to 1 mL/kg/h.
Oxygen delivery has been maximized.
Aerobic metabolism has been restored in all tissue beds.
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems.
OrthoCash 2020
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Infection
Malunion
Loss of forearm rotation
Refracture
Delayed union/nonunion
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution.
OrthoCash 2020
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
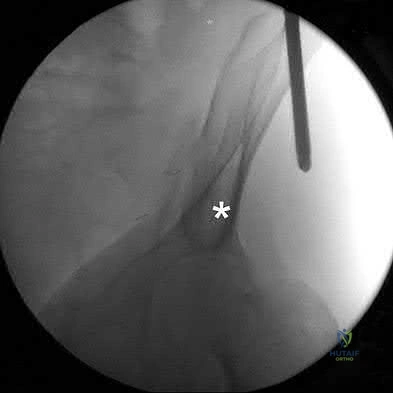
Anterior superior iliac spine
Sciatic buttress
A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
The most superior portion of the roof of the acetabulum
Iliopectineal line
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures.
OrthoCash 2020
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure
Question 28
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?
Explanation
REFERENCE: Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 29
A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiographs show that the left distal femoral growth plate is now closed; however, the tibial growth plate is still open. Her bone age matches her chronologic age. Management should consist of
Explanation
long-term solution.
REFERENCES: Westh RN, Menelaus MB: A simple calculation for the timing of epiphyseal arrest: A further report. J Bone Joint Surg Br 1981;63:117-119.
Sasso RC, Urquhart BA, Cain TE: Closed femoral shortening. J Pediatr Orthop 1993;13:51-56.
Nordsletten L, Holm I, Steen H, Bjerkreim I: Muscle function after femoral shortening osteotomies at the subtrochanteric and mid-diaphyseal level: A follow-up study. Arch Orthop Trauma Surg 1994;114:37-39.
Question 30
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Explanation
Question 31
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
Question 32
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
REFERENCES: Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Schulte KR, Callaghan JJ, Kelley SS, Johnston RC: The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up: The results of one surgeon. J Bone Joint Surg Am 1993;75:961-975.
Question 33
A 31-year-old high school football coach has right medial knee pain that is made worse with prolonged standing. His knee is minimally painful in the morning but by the end of the school day, he must sit down. The pain often makes sleeping difficult. He states that several years ago he underwent a surgical procedure to "clean out" the cartilage of the knee; however, he only had several months of pain relief. He is noted to be an athletic male (BMI of less than 30). Knee examination is unremarkable except for medial joint line pain that is exacerbated with standing and walking. Radiographs, including a long-leg view, and MRI scans are seen in Figures 153a through 153d. He wishes to remain active and asks whether he would be a candidate for allograft meniscus transplantation. You advise him that Review Topic

Explanation
Question 34
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
Explanation
REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 212-213.
Manoli A II, Smith DG, Hansen ST Jr: Scarred muscle excision for the treatment of established ischemic contracture of the lower extremity. Clin Orthop Relat Res 1993;292:309-314.
Early JS, Ricketts DS, Hansen ST: Treatment of compartmental liquefaction as a late sequelae of a lower limb compartment syndrome. J Orthop Trauma 1994;8:445-448.
Question 35
The 73-year-old patient undergoes shoulder hemiarthroplasty. What is a risk factor for a poor outcome?
Explanation
Surgical treatment is favored for young, active patients with displaced proximal humerus fractures. Nonsurgical treatment is favored to treat fractures with minimal displacement among low-demand elderly patients. When ORIF is used, a number of strategies are employed to prevent failure, including restoration of medial cortical support (medial calcar), incorporation of the rotator cuff into the construct, and placement of screws of adequate length to gain purchase in the subchondral bone of the humeral head. Intramedullary allograft is not routinely required but is useful when dealing with osteoporotic bone. Cancellous allograft has not been shown to prevent
failure. Varus collapse and failure of fixation are more prevalent in patients with osteoporotic bone, and, in these cases, strategies for supplemental fixation are advisable. In cases of severe osteoporosis, comminution, or poor bone quality, shoulder arthroplasty may be a better choice. Without a functioning rotator cuff, as would happen with a tuberosity nonunion, outcomes after shoulder hemiarthroplasty and TSA are poor.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 36
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?
Explanation
REFERENCES: Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423.
Question 37
Figures 70a and 70b show the sagittal MRI scan and axial CT of a patient who has decreased range of motion in the cervical spine. In which of the following directions would the cervical motion be most significantly limited?
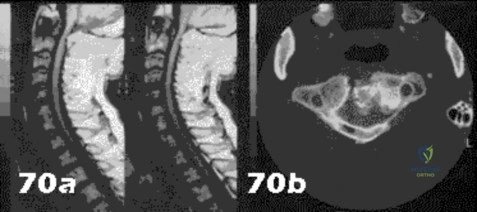
Explanation
Question 38
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of
Explanation
REFERENCES: Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Warren SB, Brooker AF Jr: Excision of heterotopic bone followed by irradiation after total hip arthroplasty. J Bone Joint Surg Am 1992;74:201-210.
Question 39
A 7-year-old boy is seen for follow-up for a scoliotic deformity. His parents are concerned because his deformity seems to have increased. He has no pain and is neurologically intact. A radiograph is shown in Figure 94, and measurement of his curve reveals that it has increased 10 degrees. What is the most appropriate recommendation for this patient at this time?
Explanation
REFERENCES: Nakamura H, Matsuda H, Konishi S, et al: Single-stage excision of hemivertebrae via the posterior approach alone for congenital spine deformity: Follow-up period longer than ten years.
Spine 2002;27:110-115.
Ruf M, Harms J: Posterior hemivertebra resection with transpedicular instrumentation: Early correction in children aged 1 to 6 years. Spine 2003;15:2132-2138.
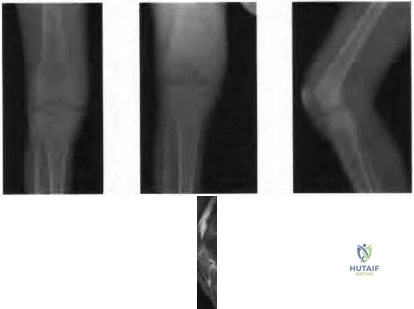
Figure 95a Figure 95b Figure 95c Figure 95d
Question 40
A 34-year-old man presents to clinic with 4 months of right elbow pain. He began going to the gym and playing squash about 3 months ago. On exam, he is tender over the lateral aspect of the elbow and has pain with resisted wrist extension. Which of the following choices lists the correct compartment of the muscle typically involved in this disease and then lists its antagonist muscle? Review Topic
Explanation
Lateral epicondylitis is an overuse injury, typically secondary to repetitive pronation and supination motion in extension, that leads to inflammation of the ECRB origin at the elbow. Histological analysis typically shows vascular hyperplasia and disorganized collagen. Clinically, patients will have pain over the lateral elbow exacerbated by resisted wrist extension. ECRB, the most commonly involved muscle origin, is innervated by the deep branch of the radial nerve and inserts on the base of the 3rd metacarpal. As it is radial wrist extensor, its antagonist is the ulnar sided wrist flexor.
Brummel et al. reviewed the clinical presentation and management options for lateral epicondylitis. They report acute symptoms in younger patients and chronic symptoms in older patients. NSAIDs, extensor stretching and activity modification are the mainstay of nonsurgical treatment.
Bunata et al. studies 85 cadavar elbows to determine anatomic factors contributing to tennis elbow. They found that the ECRB undersurface rubs against the lateral capitellium in elbow extension leading to tendinosis.
Illustration A is cross-sectional diagram of the forearm with muscle bellies labeled. Notice the location of ECRB in the mobile wad. Illustration B is a coronal T2 MRI showing fluid signal and undersurface tearing near the extensor origin as can be seen in lateral epicondylitis.
Incorrect Answers:
1-4: The ECRB is in the mobile wad and its antagonist is flexor carpi ulnaris. All other answers are incorrect.
Question 41
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
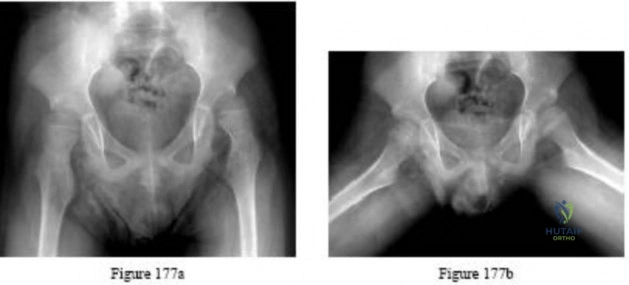
Explanation

Question 42
1% of all studies from nine orthopaedic journals were Level 4 evidence. Further investigation of more current trends is likely warranted with the current emphasis on publishing higher level-of-evidence studies in orthopaedic journals.
Explanation
failure, hyperhomocystinemia, diseases that alter blood viscosity (eg, polycythemia, sickle cell disease, multiple myeloma), and inherited thrombophilias. In addition to the risk associated with embolization of PMMA, the patient has been immobile for 7 days and was ultimately diagnosed with multiple myeloma.
Which key factor that induces osteoclastogenesis is secreted by osteoblasts in response to inflammatory stimuli?
Osteoprotegerin (OPG)
Tumor necrosis factor (TNF)
Insulin growth factor-1 (IGF)
Bone morphogenetic protein (BMP)
Receptor activator of nuclear factor kappa-B ligand (RANKL) Corrent answer: 5
Osteoclasts are derived from cells of the monocyte/macrophage lineage. They are multinucleated and develop by fusion of mononuclear precursors, a process that requires receptor activator for nuclear factor kappa-B ligand (RANKL) and macrophage-colony stimulating factor (M-CSF). RANKL is secreted by osteoblasts in response to inflammatory signals and is a key component of inflammation-mediated osteolysis. OPG binds to and sequesters RANKL, thus inhibiting osteoclast differentiation and activity.
BMP and IGF-1 are potent regulators of osteoblast differentiation and activation. TNF is a cytokine secreted by macrophages and degranulating platelets infiltrated in the fracture site and impacts a variety of cells, not osteoclasts.
A prospective outcome study is performed at a single institution to analyze the potential differences in treating intertrochanteric hip fractures with a plate/screw device versus an intramedullary device. No specific randomization is performed because an equal number of surgeons have preferences for the use of one of these devices and they are allowed to continue their preferred method. Hip- specific and general health-related outcome measures are used, an excellent follow-up rate of 85% of the patients at 2 years is accomplished, and there appears to be results that favor the intramedullary device but the confidence intervals are wide. This study would be considered to carry what level of evidence?
I
II
III
IV
V
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
The fracture seen in Figures A and B is most likely to occur in which of the following growth plate zones?
Resting zone
Proliferative zone
Zone of maturation
Zone of degeneration
Zone of provisional calcification
Physeal fractures typically occur through the zone of provisional calcification. Answers 3-5 are all part of the hypertrophic zone which is labeled "D" on the histologic illustration A. Illustration B shows the relationship of the physeal zones to the epiphysis and metaphysis of a growing bone. However, the stress concentration is greatest in the sub-layer where there is a transition from the soft cartilagenous physis to the harder calcific metaphysis.
As discussed in the review by Ballock and O'Keefe, the growth plate is a remarkable portion of the skeleton that requires precise coordination between multiple endocrine, paracrine, and autocrine signaling systems. While fractures can occur in any portion of the growth plate, the zone of provisional calcification is the most common.
Since the adoption by the American Academy of Orthopaedic Surgeons in 1997 of the presurgical protocol in which the surgeon signs the surgical site and the mandate for this protocol by the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO)
in 2003, the total number of wrong-site surgeries reported per year in the United States has
increased.
decreased.
decreased for orthopaedic surgery but stayed the same for other surgeries.
remained the same.
only improved for hospital-based surgery.
Despite the initiatives by the American Academy of Orthopaedic Surgeons and the
JCAHO, the number of reported cases of wrong-site surgery has continued to increase yearly since 1997. Because reporting of these events is not mandated by JCAHO, it is possible that the continued increase is due to a greater awareness of the problem and thereby a greater level of reporting. The U.S. estimates are 12.7 wrong-site surgeries per million cases performed. Orthopaedic surgery and podiatry are the most common specialties associated with wrong-site surgery (41%) followed by general surgery (21%), neurosurgery (14%), and urologic surgery (11%).
The use of evidence-based studies among professions associated with health care, including purchasing and management, is known as
decision analysis.
cost-utility analysis.
cost-benefit analysis.
cost-effectiveness analysis.
evidence-based health care.
Evidence-based health care extends the application of the principles of evidence-based medicine to all professions associated with health care. This concept is becoming more important because data will be used by the different parties for their decision making (policy makers, health insurances, hospitals, doctors, and the public). Cost-benefit analysis refers to the conversion of effects into the same monetary terms as the costs and compares them. Cost- effectiveness analysis refers to the conversion of effects into health terms and describes the costs for some additional health gain (eg, cost per additional event prevented). Cost-utility analysis refers to the conversion of effects into personal preferences (or utilities) and describes how much it costs for some additional quality gain (eg, cost per additional quality-adjusted life-year).
Decision analysis refers to the application of explicit, quantitative methods to analyze decisions under conditions of uncertainty.
All of the following medications have been associated with an increased risk of osteoporosis EXCEPT:
Selective serotonin reuptake inhibitors (SSRI)
Glucocorticoids
Non-steroidal anti-inflammatories (NSAIDs)
Phenytoin
Protease inhibitors
Numerous drugs are associated with an increased risk of osteoporosis in
adults, including oral corticosteroids, androgen-deprivation therapy, aromatase inhibitors, protease inhibitors, selective serotonin reuptake inhibitors,
prolactin-raising antiepileptic agents and many cytotoxic agents.
Additionally, a number of disease states are associated with osteoporosis, including endocrinopathies such as hyperparathyroidism, thyrotoxicosis and type I diabetes, hypogonadism, chronic glucocorticoid therapy, malnutrition, malabsorption states, chronic immobilization, rheumatoid arthritis, alcoholism, vitamin D deficiency, and multiple myeloma.
NSAIDs have not been shown to increase risk of osteoporosis.
A 65-year-old woman with rheumatoid arthritis is unable to actively extend her index, middle, ring, and little fingers secondary to tendon rupture. In performing a flexor digitorum sublimis (FDS) of the middle/ring finger to extensor digitorum communis (EDC) transfer to restore active metacarpophalangeal (MCP) joint extension, the FDS should be passed
ulnarly, around the ulna in a dorsal direction.
radially, around the radius in a dorsal direction.
through the interosseous membrane.
through the intermetacarpal spaces between the index, middle, ring, and little fingers.
through the lumbrical canals of the index, middle, ring, and little fingers. Corrent answer: 2
Although the early use of FDS as a transfer to restore finger extension in patients with radial nerve palsy was performed by passing the tendon through the interosseous membrane, Nalebuff and Patel later modified this procedure for the rheumatoid arthritis patient by passing the FDS radially, around the radius in a dorsal direction. They felt that this provided a number of advantages, including: 1. technical ease, 2. avoidance of synovial disease on the dorsum of the wrist, and 3. correction of ulnar deviation of the fingers through the line of pull from the radial side of the forearm.
Based on the clinical photograph, radiographs, and biopsy specimen shown in Figures 68a through 68d, what is the most likely diagnosis?
Calcium pyrophosphate deposition disease
Bacterial infection
Fungal infection
Gout
Giant cell tumor
The patient has gout. Unfortunately, gout may mimic several conditions affecting the small joints of the hand, including infection. The histologic specimen shows negatively birefringent intracellular rods consistent with gout. The histology rules out giant cell tumor and calcium pyrophosphate deposition disease.
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Continued observation and monitoring
Obtain arterial blood gas measurements
Obtain emergent spiral CT scan to assess for pulmonary embolism
Insertion of a chest tube
Airway control and, if necessary, endotracheal intubation
Because the phrenic nerve lies in close proximity to the site of anesthetic injection, temporary hemidiaphragmatic paresis is a very common side effect of interscalene brachial plexus block. Pulmonary function and chest wall mechanics may be slightly compromised, but can easily be compensated in a healthy patient. Therefore, with
sufficient oxygenation, aggressive assessments or treatments such as arterial blood gas measurements,
emergent spiral CT scans, chest tube insertions, or endotracheal intubation are not warranted. For this stable patient, continued monitoring with gradual withdrawal of oxygen is the most appropriate treatment.
A 67-year-old woman with rheumatoid arthritis has had a 3-year history of gradually progressive right elbow pain and limited function despite intra-articular injections and medical management. She previously underwent a rheumatoid hand reconstruction, and has no pain or dysfunction of the ipsilateral shoulder.
Radiographs are shown in Figures 93a and 93b. What is the most appropriate treatment?
Soft-tissue interposition arthroplasty with radial head resection
Arthroscopic synovectomy with radial head resection
Elbow arthrodesis
Total elbow arthroplasty
Resection arthroplasty
Total elbow arthroplasty is the treatment of choice. The patient has end-stage rheumatoid involvement of the ulnohumeral and radiocapitellar joints. Given the advanced nature of the disease and evidence of bony erosion, arthroscopic
synovectomy and interposition arthroplasty are unlikely to provide lasting benefit or functional improvement. Elbow arthrodesis and resection arthroplasty are considered salvage techniques and are generally not considered as a primary treatment method.
A 66-year-old woman with known poorly controlled rheumatoid arthritis reports that for the past 4 weeks she has been unable to extend the metacarpophalangeal (MCP) joints of her right hand index, middle, ring and little fingers. She cannot hyperextend the thumb interphalangeal joint. Active wrist extension is possible, but shows radial deviation. Examination reveals mild synovitis at the wrist and MCP joints of the affected hand. There is no ulnar deviation at the MCP joints with normal alignment. When the MCP joints are passively extended, the patient is unable to maintain them in this position.
There is no piano key sign at the distal ulna. Passive wrist motion shows a normal tenodesis effect. Which of the following would most likely confirm your diagnosis?
Radiographs of the hand
Radiographs of the cervical spine
Electrodiagnostic studies of the affected upper extremity
Surgical exploration of the extensor tendon ruptures
MRI of the elbow
There are many causes of inability to extend the MCP joints in a patient with rheumatoid arthritis. The most common cause is rupture of the extensor tendons. An intact tenodesis test suggests that the extensor tendons are intact, thus surgical exploration is not indicated and would not confirm the diagnosis. The patient has normal alignment of the fingers without ulnar deviation, suggesting that there are no MCP dislocations to account for the inability to extend the MCP joints; therefore, radiographs would not confirm the diagnosis. The most likely cause of inability to extend the fingers in this patient is posterior interosseous nerve (PIN) palsy. Electrodiagnostic studies would confirm the presence of PIN palsy. An MRI of the elbow may show synovitis at the radiocapitellar joint, which can cause the PIN palsy. This finding however, is nonspecific and many patients without PIN palsy would also demonstrate synovitis at the radiocapitellar joint.
Therefore, although an MRI would be helpful in localizing a potential cause of PIN compression, it would not in itself confirm the diagnosis.
What is the predominant type of collagen found in the nucleus pulposus of the intervertebral disk?
Type I
Type II
Type V
Type VI
Type XII Corrent answer: 2
Types I and II collagen are the predominant types of collagen found in the intervertebral disk. Type I collagen is present in the highest concentration in the annulus fibrosus and type II collagen in the nucleus pulposus. Type V collagen is present in small concentration in the annulus fibrosus. Type VI collagen is a non-fibrillar, short-helix collagen found in both the annulus and nucleus. Type XII is present in the annulus fibrosus only.
What complication is associated with the use of epidural morphine and steroid paste after laminectomy?
Surgical site infection
Arachnoiditis
Urinary retention
Disk space infections
Nerve irritation
Kramer and associates conducted a retrospective review during an "epidemic" period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications. There is no evidence in the literature verifying the incidence of postoperative urinary retention and arachnoiditis.
Which of the following materials has the highest modulus of elasticity?
Cortical bone
Cobalt-chrome
Ceramic
Titanium
Stainless steel
Young's modulus of elasticity is a measure of the stiffness of a material and its ability to resist deformation. This is the slope of the stress/strain curve in the elastic range. The highest modulus is ceramic, followed by: cobalt-chrome alloy, stainless steel, titanium, and then cortical bone.
What medication has been shown to decrease osteolysis after total joint replacement surgery?
Bisphosphonates
NSAIDs
TNF-alpha inhibitors
Calcium and vitamin D supplementation
BMP-7
Bisphosphonates have been shown to decrease osteolysis after total joint replacement surgery.
Aseptic loosening and osteolysis are the primary causes of implant failure in total joint arthroplasty. Early findings indicate that bisphosphonates upregulate bone morphogenetic protein-2 production and stimulate new bone formation, leading to decreased osteolysis in total joint replacement surgery. While
further investigation is required, bisphosphonates may play a future role in improving the long-term duration of joint arthroplasties.
Shanabhag et al. reviewed the use of bisphosphonates and reported that they had the potential to enhance bone ingrowth into implant porosities, prevent bone resorption under adverse conditions, and dramatically extend the long- term durability of joint arthroplasties. They recommended further investigation into the subclasses to determine which ones are most beneficial.
Arabmotlagh el al. performed a prospective study on use of alendronate after total hip arthroplasty. They reported that the alendronate-treated patients had significantly less periprosthetic bone loss on DXA scans after 6 years.
Illustration A shows evidence of osteolysis (arrows) around a total hip arthroplasty.
Incorrect Answers:
5: These medication classes do not decrease osteolysis after total joint arthroplasty.
A 60-year-old woman has progressive neck pain, upper extremity pain, and paresthesias. A lateral cervical spine radiograph and an MRI scan are shown in Figures 52a and 52b. What is the most likely underlying diagnosis?
Osteomyelitis
Ankylosing spondylitis
Age-related degenerative changes
Rheumatoid arthritis
Previous cervical decompression Corrent answer: 4
The radiograph and sagittal T2-weighted MRI scan show multilevel degenerative changes and subaxial subluxations with anterolisthesis at C3-C4 and C4-C5 and retrolisthesis at C5-C6. In addition, there is evidence of midcervical kyphosis. Such findings are often seen in patients with rheumatoid arthritis. Patients with osteomyelitis typically show increased signal intensity in the disks and vertebral bodies. Patients with ankylosing spondylitis typically show ankylosis of the disks and vertebral bodies. Age-related degenerative changes typically manifest as degenerative disk disease with occasional single- level spondylolisthesis, but not typically multilevel spondylolisthesis, as seen in this patient. The spinous processes are intact; these changes do not appear to be postoperative.
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
The use of lead glasses, thyroid shield, and a lead apron with a equivalent lead thickness of 0.25 mm
Orienting the cathode ray tube beneath the patient with the image intensifier receptor as close to the patient as possible
Limiting the beam on time to only what is clinically important
The use of continuous fluoroscopy to ensure proper placement of implants
Orienting the beam in the opposite direction of the working team and keeping the team outside a 6-foot radius from the fluoroscopy machine
Continuous fluoroscopy and cineradiography exposes the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray
tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Nicotine impairs osteoblast activity, thus interfering with bone remodeling.
The effects of smoking on bone healing are multifactorial and not yet fully understood.
The vasoconstrictive and platelet-activating properties of nicotine inhibit fracture healing.
Nicotine inhibits the function of fibroblasts, red blood cells, and macrophages.
Hydrogen cyanide inhibits oxidative metabolism at the cellular level. Corrent answer: 2
Tobacco smoking is now the leading avoidable cause of morbidity and mortality in the United States. The musculoskeletal effects of smoking have been implicated in osteoporosis, low back pain, degenerative disk disease, poor wound healing, and delayed fusion and fracture healing. A number of studies have demonstrated the relationship between smoking and development of pseudarthrosis. Numerous studies have been performed to
offer an explanation of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have
demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
In which of the following scenarios should a physician be relieved of their duties?
After 24 hours of continuous work
A significant error in care is noted
The physician appears fatigued
Physician is recovering from an ankle fracture
Chemical impairment is suspected
Impairment of a healthcare professional is the inability or impending inability to practice according to accepted standards as a result of substance use, abuse, or dependency (addiction). A surgeon (resident, fellow or attending) who discovers chemical impairment, dependence, or incompetence in a colleague or supervisor has the responsibility to ensure that the problem is identified and treated. Mechanisms exist for the proper identification and treatment of the impaired physician. Misconduct can be reported to state and local agencies. One must be sure to act in good faith with reasonable evidence when reporting such an incident. If a patient is at risk for immediate harm or injury by an impaired physician, one should assert authority and relieve the physician of the patient care and then address the problem with the senior hospital staff as soon as possible. The referenced article by Baldisseri is a review on the ethics of dealing with impaired healthcare professionals, with a focus on physicians.
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure 88. She denies any acute worsening of her symptoms, although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What is the next most appropriate step in management?
DEXA scan
Brace treatment with a Jewett hyperextension brace
Anterior lumbar corpectomy and arthrodesis with instrumentation
Posterior lumbar decompression and fusion
Vertebral cement augmentation
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and
begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
Figure 10 is the radiograph of a middle-aged woman who has had midfoot pain for the past several years without antecedent trauma. What is the most likely etiology of her condition?
Osteomyelitis
Kohler disease
Rheumatoid arthritis
Primary osteoarthritis
Osteochondritis dissecans
The radiograph shows isolated degeneration in the talonavicular joint that is symmetric. The symmetry of the degeneration is characteristic of an inflammatory arthritis. In the absence of trauma, isolated arthritis in this joint is uncommon. The navicular is normal sized, ruling out Kohler disease (as well as the patient being in the wrong age group). There are no erosions indicative of osteomyelitis. Osteochondritis dissecans appears as focal osteochondral lesions, which are not present in the radiograph.
Figure 39 is the radiograph of a 67-year-old woman with rheumatoid arthritis who reports an 8-month history of increasing pain, swelling, and deformity. Anti- inflammatory drugs, orthotics, and extra-depth shoes have failed to provide relief. What is the next most appropriate step in treatment?
First metatarsophalangeal joint arthrodesis and lesser metatarsal head resections
First metatarsophalangeal joint replacement and lesser metatarsal head resections
Keller arthroplasty and lesser metatarsal head resections
Distal Chevron osteotomy and lesser metatarsal head resection
Lapidus procedure and Weil osteotomies
The patient has a severe rheumatoid forefoot deformity involving all metatarsophalangeal joints. Coughlin and Mann have found that 90% of patients have excellent and good results with combined first metatarsophalangeal fusion and lesser metatarsal head resection. Keller arthroplasty does not provide a stable platform for walking and is associated with recurrent deformity and pain. The first metatarsophalangeal joint replacement has not been shown to provide reliable long- term results. Osteotomies may be indicated in patients without erosive joint changes. The Lapidus procedure is an arthrodesis of the first tarsometatarsal joint, which would not address the patient's arthritic first metatarsophalangeal joint.
The operative report of a recent patient incorrectly documents the timing of peri-operative antibiotic administration. How should the
medical record be legally altered?
Obtain written approval from the hospital medical director
Obtain written approval from the risk management team
Obtain written approval from your lawyer and the senior partners of his law firm
No approval is needed, as you were the treating surgeon and have identified
the error
It is illegal to alter the medical record, but an addendum can be made
It is illegal to alter the medical record under any circumstance. If a documentation error has occurred, you may addend the medical record by identifying the error and noting the correction.
The review article by Bal discusses medical practice and highlights the four legal elements that must be proven in litigation: (1) a professional duty owed to the patient; (2) breach of such duty; (3) injury caused by the breach; and (4) resulting damages.
A 31-year-old woman underwent a left Kidner procedure 3 months ago. She now has pain overlying the medial column of the foot. She withdraws the foot when touching of the medial foot is attempted. Examination reveals allodynia, pain, hyperalgesia, and edema of the medial foot. What is the most likely diagnosis?
Shingles
Cellulitis
Charcot foot
Osteomyelitis
Reflex sympathetic dystrophy
Patients with reflex sympathetic dystrophy (RSD) have a history of trauma, minor rather than major (eg, Colles fracture), in about 50% to 65% of cases. The condition may also follow a surgical procedure. Patients usually have symptoms and signs of RSD including: pain, described as burning, throbbing, shooting, or aching; hyperalgesia; allodynia; and hyperpathia. There are trophic changes within 10 days of onset of RSD in 30% of the extremities affected, including stiffness and edema and atrophy of hair, nails, and/or skin.
Finally there can be autonomic dysfunction, such as abnormal sweating, either
in excess or anhydrosis, heat and cold insensitivity, or redness or bluish discoloration of the extremities. Shingles, also called herpes zoster or zoster, is a painful skin rash caused by the varicella zoster virus (VZV). VZV is the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays in the body.
Usually the virus does not cause any problems; however, the virus can reappear years later, causing shingles. Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from
Question 43
- A 35-year-old machinist sustains a crush injury to the forearm in an industrial accident. Figure 34 shows the arm following skeletal stabilization and fasciotomy. Wound closure is best accomplished by
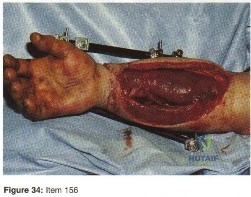
Explanation
Question 44
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as arthroscopic debridement and lavage).
Question 45
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 46
In the setting of a proximal tibial plateau fracture and its repair, which of the following materials is an isotropic material?
Explanation
REFERENCE: Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 58-59.
Question 47
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
REFERENCES: Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Sharrard J, Drennan JC: Osteotomy excision of the spine for lumbar kyphosis in older children with myelomeningocele. J Bone Joint Surg Br 1972;54:50-60.
Question 48
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
Question 49
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure 2. Which interposed structure is preventing reduction?

Explanation
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
Question 50
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T 2 -weighted MRI scans. What is the most likely diagnosis?
Explanation
REFERENCE: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 2189-2216.
Question 51
A 52-year-old woman has a 60-degree extensor lag following a right total knee arthroplasty performed 16 months ago. Since the time of her primary total knee arthroplasty she has undergone primary repair of a patellar tendon rupture that occurred after a fall 8 months ago. A lateral radiograph of the knee is shown in Figure 52. A CT scan obtained to determine component rotation showed that the femoral component is internally rotated 9 degrees and the tibial component is internally rotated 12 degrees. Appropriate management at this time should include
Explanation
Attempts at secondary repair have been associated with high failure rates whereas the use of an extensor mechanism allograft has been shown to more effectively restore active extension in a substantial percentage of patients. Important aspects of the technique include fully tensioning the graft in full extension and immobilization of the extremity for 6 to 8 weeks postoperatively to allow for graft healing. Nonsurgical management will not result in an acceptable outcome for a young patient, and attempted secondary repair is associated with a high rate of failure, even when augmented with local tissues. This patient has gross rotational
malalignment of the components and the surgeon faced with this problem should consider obtaining a CT scan to determine component rotation preoperatively.
REFERENCES: Burnett RS, Berger RA, Paprosky WG, et al: Extensor mechanism allograft reconstruction after total knee arthroplasty: A comparison of two techniques. J Bone Joint Surg Am 2004;86:2694-2699.
Nazarian DG, Booth RE: Extensor mechanism allografts in total knee arthroplasty. Clin Orthop Relat Res
1999;367-123-129. , „. H
AL-Madena Copy ^Lj-^M) <UjJlU

Question 52
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126.
Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, p 158.
Question 53
The best definitive treatment for this patient’s left knee is
Explanation
This patient now has a major fixed flexion contracture and severe varus alignment and instability. Infection of the knee joint has to be ruled out. The radiograph shows all the hallmarks of Charcot arthropathy, including disintegration and fragmentation of the joint with major deformity. Infection of the knee joint and contiguous osteomyelitis still have to be ruled out. The clinical and radiographic findings are highly suggestive of a Charcot neurogenic arthropathy associated with uncontrolled diabetes. This patient is an unsuitable candidate for total knee arthroplasty (TKA) because he is noncompliant regarding his diabetes and has had a previously infected native joint that now is associated with Charcot arthropathy. He is nonambulatory. The failure rate of TKA or knee arthrodesis is extremely high in this setting. He will best be served with observation or amputation depending upon his symptom severity.
Question 54
Figures 186a and 186b are the radiographs of a 10-year-old girl who sustained an injury 2 days ago after jumping off another girl's shoulders while cheerleading. She is unable to walk and has no other injuries. Examination reveals swelling below the knee and a palpable defect at the tibial tubercle. The knee is ligamentously stable medial-lateral and anterior-posterior. What is the next most appropriate step in management? Review Topic

Explanation
Question 55
A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
Explanation
Question 56
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 57
Which patient would expect to have the longest implant survivorship after undergoing total elbow arthroplasty (TEA)? Review Topic
Explanation
The primary surgical management of the rheumatoid elbow is mainly synovectomy or total elbow arthroplasty (TEA). The indications for TEA include advanced disease of the elbow (grade III or IV), significant pain, and limitations in activities of daily living. Contraindications include active or historical elbow infection, upper extremity paralysis, and refusal to abide by postoperative instructions. Implant options are traditionally classified as linked (semiconstrained) or unlinked - with improved stability and survivorship of semiconstrained designs.
Aldridge et al. provide a 10- to 31-year survival analysis on total elbow arthroplasty with the Coonrad/Coonrad-Morrey prosthesis. They reviewed 40 patients (41 elbows) who had undergone a Coonrad/Coonrad-Morrey elbow arthroplasty. Of the 41 elbows, 21 were functional between 10 and 14 years after operation, ten between 15 and 19 years and ten between 20 and 31 years.
Skytta et al. reviewed 1,457 primary TEAs for rheumatoid elbow. 87% of the TEAs were performed in women. The most frequent reason for revision was aseptic loosening (47%). They found no differences in survival rates between different TEA designs.
Schneeberger et al. examined 41 post-traumatic osteoarthritic elbows treated with semiconstrained Coonrad-Morrey TEA. 11 patients (27 per cent) had major complications. These were attributed to lifting more weight across the implant than adviced by the surgeon; excessive preoperative deformity of the joint; and/or an unstable traumatic injury.
Cil et al. reviewed 91 patients who underwent total elbow arthroplasty for the treatment of a distal humeral nonunion. The rate of prosthetic survival without removal or revision for any reason was 96% at two years, 82% at five years, and 65% at both ten and fifteen years. They conclude that semiconstrained TEA is a salvage procedure in patients with a distal humeral nonunion that is not amenable to internal fixation.
Incorrect Answers:
Question 58
In the most common condition causing a winged scapula, which of the following nerves is affected? Review Topic
Explanation
Question 59
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 60
Which of the following best describes heat stroke? Review Topic
Explanation
Question 61
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m 2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?

Explanation
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 62
-What is the most appropriate course of action for this patient’s condition?
Explanation
The anterior drawer test is performed with the ankle in 10 degrees of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician or examiner uses one hand to stabilize the distal leg and with the other applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement greater than 15 degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments.The diagnosis is a severe lateral ligament complex sprain. Considering the involvement of the anterior talofibular ligament and calcaneofibular ligaments, early mobilization with a cast or controlled ankle movement walker boot has been documented to result in better patient outcomes than compression or air casting.
Question 63
Which factor has the most negative influence on the success of knee osteochondral allograft transplantation?
Explanation
The images illustrate a large unstable osteochondral lesion of the medial femoral condyle. Radiographs and MR images clearly show deep subchondral bone involvement. The appropriate choice of surgery is OCA transplantation, which is indicated for primary treatment of large cartilage lesions, osteochondral lesions, and salvage procedure from failed prior cartilage surgery. Correction of mechanical axis malalignment, ligamentous insufficiency, and meniscal deficiency should also be addressed. ACI alone or an arthroscopic microfracture procedure would not address the bone defect, leaving an uneven articular surface. Although an osteotomy may be a viable choice, a distal femoral varus osteotomy would increase the contact pressure in the medial compartment and worsen the situation.
The histologic anatomy of articular cartilage is well described. The superficial layer or lamina splendens contains a small amount of proteoglycan with collagen fibrils arranged parallel to the articular surface. In contrast, the deep zone contains the largest-diameter
collagen fibrils, oriented perpendicular to the joint surface, and the highest concentration of proteoglycans.

Video 54 this video is uploaded at
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a and 51b are the radiographs of an 18-year-old football linebacker who was involved in a tackle and fell onto an outstretched left arm. He had immediate pain and deformity of his left elbow.
Question 64
1 and 2 demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 65
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
REFERENCES: Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949.
Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Meyers WC, Foley DP, Garrett WE, et al: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Question 66
Figure A is the lateral view of a left knee cadaveric specimen that has the extensor mechanism removed. Which two structures labeled provide the most rotational stability in knee flexion? Review Topic
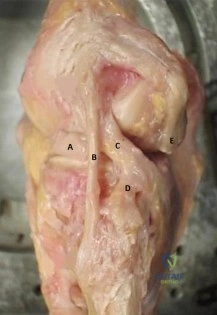
Explanation
extension.
The lateral knee is stabilized by 28 unique static and dynamic structures. These structures work in concert to resist varus gapping and rotational knee instability. The three primary stabilizers include the fibular or lateral collateral ligament (LCL), the popliteus tendon (PT) and the popliteofibular ligament (PFL). Injury to these ligaments results in increased forces seen on ACL and PCL ligament reconstruction grafts with combined posterolateral corner (PLC) injuries, which can result in graft failure if the PLC is not reconstructed as well.
James et al reviewed the anatomy and biomechanics of the lateral knee stabilizers, detailing the specific functional contributions of the individual structures. The LCL is the primary restraint to varus instability, the highest forces occurring at knee extension (0°-30°). The PT and PFL serve as restraints to rotational instability, the highest forces occurring at knee flexion (60°-90°).
LaPrade et al reviewed the anatomy and biomechanics of the medial knee stabilizers. The three key static stabilizers are the superficial medial collateral ligament (sMCL), the deep medial collateral ligament (dMCL), and the posterior oblique ligament (POL). The sMCL is the primary restraint to valgus instability (proximal sMCL) and secondary restraint to rotational instability (distal sMCL) at all knee flexion angles. The dMCL is a secondary restraint to valgus and rotational instability. The POL is the primary restraint to rotational instability.
Figure A depicts the lateral knee structures in a cadaver specimen (A = lateral meniscus, B = LCL, C = PT, D = PFL, E = lateral head of gastrocnemius). Illustration A is a labeled picture of the lateral knee structures. Illustration B is a table from James et al demonstrating the change in forces experienced by the different lateral stabilizers at varying degrees of knee flexion. You see the LCL resists rotation at 0°-30° (extension) while the PT and PFL resist rotation at 60°-90° (flexion).
Incorrect Responses:
Question 67
Risk of fat embolism is greatest during what step of total hip arthroplasty?
Explanation
REFERENCES: Pitto RP, Koessler M, Kuehle JW: Comparison of fixation of the femoral component without cement and fixation with use of a bone-vacuum cementing technique for the prevention of fat embolism during total hip arthroplasty. J Bone Joint Surg Am
1999;81:831-843.
Christie J, Burnett R, Potts HR, Pell AC: Echocardiography of transatrial embolism during cemented and uncemented hemiarthroplasty of the hip. J Bone Joint Surg Br 1994;76:409-412.
Question 68
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?
Explanation
REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 192.
Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106.
Scott AC, Scarborough N: The use of dynamic EMG in predicting the outcome of split posterior tibial tendon transfers in spastic hemiplegia. J Pediatr Orthop 2006;26:777-780.
Williams PF: Restoration of muscle balance of the foot by transfer of the tibialis posterior. J Bone Joint Surg Br 1976;58:217-219.
Question 69
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 70
Ewing’s sarcoma of bone most commonly occurs in which of the following locations?
Explanation
REFERENCES: Simon M, Springfield D, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Wold LA, et al: Ewing’s Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 210-211.
Question 71
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management? Review Topic
Explanation
in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.
Question 72
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 73
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a “lump” at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 1078-1079.
Rockwood CA, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 74
A coach of three football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on one team are different from those on the other teams?
Explanation
Question 75
A 32-year-old male electrical worker complains of isolated left shoulder pain after a fall from 6 feet. Radiographs of the shoulder are seen in Figures A and B. The radiology technician was unable to obtain a good axillary view due to significant pain and muscle spasm. What would be the next most appropriate step in management? Review Topic
Explanation
Risk factors for posterior shoulder dislocation include epilepsy, electrocution and high-energy trauma. To make a diagnosis, standard views of the shoulder are required. These include an anteroposterior (AP) view, lateral scapular view and an axillary view. The axillary view is essential for diagnosis, but this requires the arm to be positioned in 20 - 30 degrees of abduction. If pain and muscle spasm restrict arm movement, the next most appropriate view would include a modified axially view,
such as a Velpeau view.
Robinson et al. reviewed posterior shoulder dislocations and fracture-dislocations. They state that apical oblique, Velpeau, or modified axial radiographs are preferable to other alternative axillary views, as they can be obtained with the arm in a sling. When an osseous injury is suspected, a CT scan and three-dimensional reconstruction can be useful in planning operative management.
Millet et al. wrote a JAAOS article on recurrent posterior shoulder instability. They state that 5 radiographic views, or advanced imaging, is essential to evaluate the shoulder. Characteristics to consider include, joint location, humeral head position, glenoid morphology (e.g., retroversion, hypoplasia, posterior glenoid rim), and impaction fracture of the humeral head.
Figure A and B show a normal shoulder radiograph with the shoulder positioned in internal rotation and external rotation. Illustration A shows the correct positioning of a patient to obtain a Velpeau view of the shoulder. Illustration B shows the correct positioning of a patient to obtain a Stryker notch view of the shoulder. This is used to asses for humeral head defects.
Incorrect Answers:
Question 76
A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
Explanation
REFERENCES: Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
McGuire R Jr: The role of anterior surgery in the treatment of thoracolumbar fractures. Orthopedics 1997;20:959-962.
Question 77
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy.
D. improved long-term survivorship profile.
Question 78
A 57-year-old man has right knee osteoarthritis and is indicated for a total knee arthroplasty (TKA). The patient has questions regarding the use of preoperative 3-dimensional imaging to develop custom cutting guides. Current data have been shown to support what proposed benefits with the use of custom cutting guides versus conventional instrumentation?
Explanation
Question 79
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment?
Explanation
REFERENCES: Poolman RW, Kocher MS, Bhandari M: Pediatric femoral fractures:
A systematic review of 2422 cases. J Orthop Trauma 2006;20:648-654.
Anglen JO, Choi L: Treatment options in pediatric femoral shaft fractures. J Orthop Trauma 2005;19:724-733.
Beaty JH: Operative treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 2005;434:114-122.
Question 80
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of
recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 81
A 42-year-old female with chronic discogenic back pain undergoes lumbar spine surgery via retroperitoneal approach. Figure A is the postoperative radiograph of her lumbar spine. Six weeks after the surgery the patient develops worsening low back pain. You obtain a radiograph of her lumbar spine, pictured in Figure B. What is the next best step in management? Review Topic
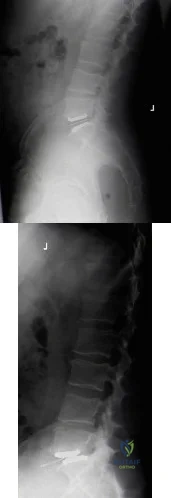
Explanation
Management of failed TDR is dictated by (1) patient symptoms and (2) radiographic implant position. Asymptomatic patients with implant subsidence without extrusion can be managed with close observation. Patients with persistent symptomatic back pain relating to facet joint or implant microinstability in the setting of an otherwise well-positioned TDR can be treated with posterior stabilization alone. Symptomatic patients with unacceptable implant position (i.e. complete dislodgement, fracture) require either revision arthroplasty or conversion to arthrodesis (anterior +/-
posterior).
Harrison et al. authored a report detailing a case of failed L5-S1 TDR with anterior dislocation of the polyethylene inlay and bilateral L5 pars fractures noted 2 weeks postoperatively. It is unclear whether the pars defect was missed following previous microdiscectomy, acquired during instrumentation, or acquired postoperatively due to abnormal endplate forces during rehabilitation. The patient underwent removal of TDR components and revision to anterior arthrodesis followed by percutaneous fixation of the bilateral L5 pars fractures.
Patel et al. published a review of the literature regarding revision lumbar TDR. Retroperitoneal revision procedures are complicated by higher risk of injury to vascular structures (16.7% versus 3.6% at primary surgery) and urogenital structures due to adhesions. Revision surgery should only be performed by surgeons familiar with the retroperitoneal approach to the spine. Alternative surgical approaches, such as the far lateral approach, should be considered to access the anterior spine at L4-L5 and above.
Madigan et al. reviewed the management of lumbar degenerative disc disease (DDD). They state that TDR is a motion-sparing surgical option designed to temper the problem of adjacent-segment disease. They report that long-term studies are limited, but point out that several short-term comparisons between TDR and ALIF show equivalent improvement in pain and function, equal complication rate, shorter hospitalization and lower rate of reoperation in the TDR group.
Figure A is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement. Figure B is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement with anterior dislocation of the polyethylene inlay.
Incorrect Responses:
Question 82
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 83
Pain emanating from the sacroiliac (SI) joint is best identified by which of the following maneuvers?
Explanation
Though no gold standard exists, a reduction of concordant pain by at least 75 to 80% following an intra-articular, image-guided anesthetic injection is considered to be the most reliable method of identifying the SI joint as the cause of a patient's pain. Although provocation tests including the Gaenslen test, the compression test, thigh thrust, and Yeoman test are commonly used and can be helpful in diagnosing non-specific SI joint pain, individually they are not as reliable as the response to a diagnostic, anesthetic injection. Of note, the combination of all 4 manuevers has proven to be more useful than any one individual test. An MRI of the SI joint showing bony erosion and bone marrow edema suggests inflammatory arthritis and may not necessarily be associated with pain.
RECOMMENDED READINGS
Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine
J. 2007 Oct;16(10):1539-50. Epub 2007 Jun 14. PubMed PMID: 17566796. View Abstract at PubMed
Visser LH, Nijssen PG, Tijssen CC, van Middendorp JJ, Schieving J. Sciatica-like symptoms and the sacroiliac joint: clinical features and differential diagnosis. Eur Spine J. 2013 Jul;22(7):1657-64. doi: 10.1007/s00586-013-2660-5. Epub 2013 Mar 2. PubMed PMID:
Question 84
What would be the advantage of surgery for the patient described in this scenario?
Explanation
The MR image of the lumbar spine postgadolinium contrast shows a ring-enhancing fluid collection. Ring-enhancing lesions within the spinal canal on postgadolinium MR images are indicative of epidural abscess. It is important to obtain a culture-specific diagnosis to inform the choice of antibiotics and educate patients regarding the likelihood of failure for standalone antibiotic therapy. Infection with MSSA, age younger than 65 years, the absence of neurologic deficit, and lumbar abscess location are all factors that point toward a patient being a reasonable candidate for a trial of culture-specific IV antibiotics. In this case, nafcillin is a suitable treatment for MSSA. The antibiotic should be initiated and closely observed with serial labs (WBC, ESR, CRP, repeat blood cultures) to ensure that the patient responds appropriately to therapy and that neurologic deficits do not develop. In the setting of epidural abscess, surgery is performed to evacuate the abscess and reverse or prevent neurologic deterioration. In the current scenario in which sepsis is not an issue, scant high-quality evidence shows that surgical intervention influences risk for mortality or chronic pain following epidural abscess.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Adogwa O, Karikari IO, Carr KR, Krucoff M, Ajay D, Fatemi P, Perez EL, Cheng JS, Bagley CA, Isaacs RE. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014 Mar;20(3):344-9. doi: 10.3171/2013.11.SPINE13527. Epub 2013 Dec 20. Review.
PubMed PMID: 24359002.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014
Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 85
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 86
A collegiate division I football player ruptures his anterior cruciate ligament (ACL). After counseling him, you agree to perform a double-bundle ACL reconstruction. Which of the following is a correct statement for this technique? Review Topic
Explanation
Question 87
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus (Granulicatella adiacens), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
belowshowtheradiographs,andtheCTobtainedfromayear-oldwomanwhounderwent
cementlesslefttotalhiparthroplasty.Ninemonthsaftersurgery,shecontinuedtohavegroinpainwhen activelyflexingherhip.Shehastroublewalkingupstairsandgettingoutofhercar.Acourseof appropriatenonsurgicaltreatmentfailed.Whatisthenextstepindefinitivetreatment?
A. Acetabularcomponentrevision
B. Femoralcomponentrevision
C. Acetabularlinerexchange
D. Trochanteric bursectomy
Submit Answer
Question 88
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?
Explanation
REFERENCES: Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 89
A 5-year-old girl has had a low-grade fever, right hip and buttock pain, and a right-sided limp for the past 5 days. Examination shows diffuse tenderness and extreme pain on range of motion of the hip. Laboratory studies show a peripheral WBC count of 13,500/mm 3 and an erythrocyte sedimentation rate of 55 mm/h. A radiograph is shown in Figure 46a, and an axial postgadolinium T 1 -weighted MRI scan with fat suppression and an axial T 2 -weighted fast spin echo MRI scan are shown in Figures 46b and 46c. What is the most likely diagnosis?
Explanation
REFERENCES: Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Herring JA: Tachdjian’s Pediatric Orthopaedics ed. 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 150-163.
Question 90
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Explanation
REFERENCES: Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 91
Currently, what is the most common clinical study type in the orthopaedic literature?
Explanation
Question 92
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 93
Presence of diabetes-induced peripheral neuropathy has been shown to be an independent risk factor for postoperative complications of which of the following injuries?

Explanation
Question 94
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 95
Which of the following antibiotics is contraindicated in children?
Explanation
REFERENCE: Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 96
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 97
The MRI scan of a patient with symptomatic shoulder pain reveals subacromial bursitis. What markers have been shown to be significant contributors to this pain? Review Topic
Explanation
Question 98
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time? Review Topic
Explanation
Question 99
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Dorfman HD, Bodgan C: Immunohematopoietic tumors, in Dorfman HD, Bogdan C (eds): Bone Tumors. St Louis, MO, Mosby, 1998, Chapter 12.
Question 100
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
