Orthopedic Surgery Board Review MCQs: Trauma, Arthroplasty, Foot & Ankle | Part 105

Key Takeaway
This page presents Part 105 of a comprehensive orthopedic surgery board review quiz, featuring 100 high-yield MCQs. Designed for orthopedic surgeons and residents preparing for AAOS and OITE certification exams, it offers interactive study and exam modes with detailed explanations.
About This Board Review Set
This is Part 105 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 105
This module focuses heavily on: Ankle, Arthroplasty, Deformity, Dislocation, Foot, Hip, Trauma.
Sample Questions from This Set
Sample Question 1: A 42-year-old man undergoes right total hip arthroplasty for hip dysplasia. Postoperatively, he has a significant limb-length increase with a foot drop. A preoperative radiograph is shown in Figure 19. Which of the following should have bee...
Sample Question 2: What is the most common foot and ankle deformity in patients with arthrogryposis?...
Sample Question 3: Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?...
Sample Question 4: A 48-year-old woman with a history of a spinal cord injury as a teenager, has unilateral weakness in the left lower extremity. She has used an ankle-foot orthosis for many years without difficulty but recently has had a recurrent painful ca...
Sample Question 5: -Figure is the radiograph of a 55-year-old veteran who developed avascular necrosis after a traumatic hip dislocation. He was treated with hemiarthroplasty 10 years ago and also has posttraumatic stress disorder and chronic pain. He has had...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 42-year-old man undergoes right total hip arthroplasty for hip dysplasia. Postoperatively, he has a significant limb-length increase with a foot drop. A preoperative radiograph is shown in Figure 19. Which of the following should have been considered preoperatively to avoid this complication?
Explanation
REFERENCES: Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement: Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080.
Papagelopoulos PJ, Trousdale RT, Lewallen DG: Total hip arthroplasty with femoral osteotomy for proximal femoral deformity. Clin Orthop 1996;332:151-162.
Huo MH, Zatorski LE, Keggi KJ: Oblique femoral osteotomy in cementless total hip arthroplasty: Prospective consecutive series with a 3-year minimum follow-up period.
J Arthroplasty 1995;10:319-327.
Question 2
What is the most common foot and ankle deformity in patients with arthrogryposis?
Explanation
REFERENCES: Guidera KJ, Drennan JC: Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop 1985;194:93-98.
Handelsman JE, Badalamente MA: Neuromuscular studies in clubfoot. J Pediatr Orthop 1981;1:23-32.
Dias LS, Stern LS: Talectomy in the treatment of resistant talipes equinovarus deformity in myelomeningocele and arthrogryposis. J Pediatr Orthop 1987;7:39-41.
Question 3
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
REFERENCES: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
MacDonald SJ, Hersche O, Ganz R: Periacetabular osteotomy in the treatment of neurogenic acetabular dysplasia. J Bone Joint Surg Br 1999;81:975-978.
Question 4
A 48-year-old woman with a history of a spinal cord injury as a teenager, has unilateral weakness in the left lower extremity. She has used an ankle-foot orthosis for many years without difficulty but recently has had a recurrent painful callus beneath the great toe that has been recalcitrant to nonsurgical management. Examination reveals intact sensation with an intractable plantar keratosis (IPK) beneath the first metatarsal head. Motor examination reveals no active ankle or great toe dorsiflexion, and 4/5 plantar flexion strength at the ankle and great toe. Passive ankle dorsiflexion is 10 degrees, whereas passive plantar flexion is 40 degrees. Passive great toe dorsiflexion is 30 degrees and plantar flexion is 10 degrees. Foot alignment on standing is normal. Radiographs are shown in Figures 47a and 47b with a marker beneath the IPK. Based on her request for surgical treatment, what is the most appropriate procedure?
Explanation
REFERENCES: Grace DL: Sesamoid problems. Foot Ankle Clin 2000;5:609-627.
Mizel MS, Miller RA, Scioli MW (ed): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 135-150.
Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.
Question 5
-Figure is the radiograph of a 55-year-old veteran who developed avascular necrosis after a traumatic hip dislocation. He was treated with hemiarthroplasty 10 years ago and also has posttraumatic stress disorder and chronic pain. He has had multiple spinal surgeries and takes 30 mg of methadone daily. He now has severe groin pain and is unable to ambulate. Laboratory studies showed a C-reactive protein level of 0.2 mg/L (reference range, 0-3 mg/L), erythrocyte sedimentation rate of 50 mm/h (reference range, 0-20 mm/h), hip aspiration of 500/mm3 white blood cell count, 50% polynucleated cells, 30%monocytes, and 20% lymphocytes What is the most likely cause of his hip pain?
Explanation
Question 6
- A consecutive series of 50 patients is randomized to receive either treatment A or treatment B. At a 10-year follow up, patient satisfaction with treatment is measured. Which of the following statistical calculations will provide the most information regarding the magnitude of possible differences between the two groups of patients?
Explanation
Question 7
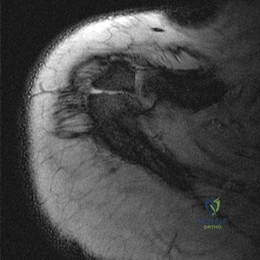
Figure 1 is the MR image of a 43-year-old man who has left shoulder pain and weakness after a fall. An examination reveals active forward elevation at 120° and positive Yergason and lift-off test examination findings. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time?

Explanation
Question 8
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?

Explanation
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Question 9
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of
Explanation
REFERENCES: Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655.
Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 10
A 10-year-old girl is treated for a tibia/fibula fracture with a long leg cast. The on-call resident is called to evaluate the patient for increasing pain medicine requirements and tingling in her foot. Examination of the cast reveals that the ankle has been immobilized in 10 degrees of dorsiflexion. What ankle position results in the safest compartment pressures in a casted lower leg?

Explanation
Weiner et al measured intramuscular compartment pressure in the anterior and deep posterior compartments of the leg in seven healthy adults who had long leg casts placed. They found that in a casted leg the intramuscular pressure in the anterior compartment was lowest with the ankle in neutral, and the deep posterior compartments was lowest when the ankle joint was in the resting position to approximately 37 degrees of plantar flexion. Based on this, they concluded that the safest ankle casting position regarding compartment pressure is between 0 and 37 degrees of plantar flexion. After the cast was bivalved, they noted a significant decrease in intramuscular pressure of 47 per cent in the anterior compartment and of 33 per cent in the deep posterior compartment. Constrictive casts and abberant ankle positioning can exacerbate pain/symptoms. Loosening of the cast by bivalving, spreading, and cutting underlying stockinette/softroll should always be the first step in management of possible compartment syndrome.
Question 11
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 12
At a minimum 2-year follow-up and compared with the metacarpophalangeal (MCP) joint, pyrolytic carbon resurfacing arthroplasties of the proximal interphalangeal (PIP) joint
Explanation
Wall and Stern published a report on MCP joint pyrolytic carbon arthroplasty for osteoarthritis and another on PIP joint pyrolytic carbon resurfacing arthroplasty for osteoarthritis. They found different outcomes, and MCP joint implants outperformed PIP joint implants. Of eleven MCP joint arthroplasties, two produced asymptomatic squeaking and clicking, whereas eleven of 31 PIP joint implants produced this problem. No dislocations were reported among the MCP joint implants, but five PIP joint dislocations were observed. Outcomes were measured by the Michigan Hand Outcomes Questionnaire in both studies and were satisfactory for the MCP joint implants, with an average score of 80. The PIP implants did not fare as well, showing a higher degree of pain along with an average score of 53. The authors noted that, in the 15 patients in the PIP study who had unilateral surgery, the uninvolved, nonsurgical hand motion was actually statistically significantly (P<0.01) better than the surgical hand. MCP joint motion increased from 62º before surgery to 76º after surgery, whereas PIP joint motion got worse after surgery, with the average motion decreasing from 57º to 31º.
Question 13
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 14
- A 40-year-old woman has progressive pain and limited range of motion in her long finger. Figure 28a shows the radiograph, and Figure 28b shows a biopsy specimen of the same lesion. What is the most likely diagnosis?
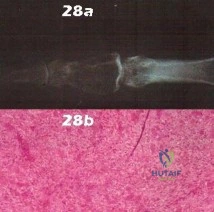
Explanation
Question 15
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 16
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm 3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T 2 -weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of
Explanation
definitive treatment.
REFERENCES: Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Vaughan PA, Newman NM, Rosman MA: Acute hematogenous osteomyelitis. J Pediatr Orthop 1987;7:652-655.
Question 17
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Explanation
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 18
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
REFERENCES: Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362.
Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307.
Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 19
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
REFERENCES: Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Raaymakers EL: Complications of talar fractures, in Tscherne H, Schatzker J (eds): Major Fractures of the Pilon, the Talus, and Calcaneus: Current Concepts of Treatment. Berlin, Springer-Verlag, 1993, pp 137-142.
Question 20
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?
Explanation
REFERENCES: Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints.
J Am Acad Orthop Surg 1995;3:166-173.
Coughlin MJ, Mann RA: Surgery of the Foot and Ankle, ed. 7. St Louis, MO, Mosby, 1999,
pp 325-328.
Question 21
Figures 1 and 2 are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 9 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem?

Explanation
Plating of the proximal radius from a dorsal or Thompson approach (between the extensor carpi radialis brevis and extensor digitorum communis) allows complete visualization of the PIN through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 1 and 2.Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the extensor indicis proprius and the EDC of the ring finger to the extensor digiti quinti proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the mobile wad and the digital extensors will be more easily found.
Question 22
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
Explanation
REFERENCE: Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB,
Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1,
pp 1052-1108.
Question 23
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma-irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 24
Figure 30 shows the AP radiograph of a 9-month-old girl who has been referred for evaluation of unequal leg lengths. Examination reveals symmetrical abduction of the hips. When the hips are flexed 90°, the right knee height is greater than the left knee. The girth of the right thigh and calf is larger than the contralateral side. There are no cutaneous lesions, and examination of the spine is normal. The infant is moving all extremities equally and spontaneously. Management should consist of
Explanation
REFERENCES: Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont Ill, American Academy of Orthopaedic Surgeons, 1996, pp 185-193.
Sponseller PD: Localized disorders of bone and soft tissue, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 305-344.
Beals RK: Hemihypertrophy and hemihypotrophy. Clin Orthop 1982;166:199-203.
Question 25
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991,
pp 1712-1718.
Question 26
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve?

Explanation
Question 27
A year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic
feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 28
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
REFERENCES: Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Amstutz HC, Campbell PA, Le Duff MJ: Fracture of the neck of the femur after surface arthroplasty of the hip. J Bone Joint Surg Am 2004;86:1874-1877.
Question 29
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?
Explanation
REFERENCES: Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 30
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 31
- The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to
Explanation
Question 32
Figure A is an AP radiograph of a 68-year-old man who presents to clinic with shoulder pain and dysfunction. On examination of his shoulder, he has pseudoparalysis with attempt at forward elevation and a positive hornblower's sign while demonstrating normal belly press test. Treatment should consist of: Review Topic

Explanation
RTSA can improve pain and function in shoulders with forward elevation pseudoparalysis secondary to rotator cuff tear arthropathy. Following arthroplasty, the deltoid alone can restore overhead elevation but it does not address active external rotation deficit. LDT is a well described procedure for treatment of irreparable posterosuperior rotator cuff tear. Combining RTSA and LDT can address both deficits and in select patients yields significant pain relief and restoration of function.
Walch et al found that hornblower's sign had 100% sensitivity and 93% specificity for irreparable degeneration of teres minor.
Puskas et al present clinical outcomes of RTSA combined with LDT for treatment of chronic combined pseudoparesis of elevation and external rotation of the shoulder in 40 patients. At a mean follow-up of 53 months, the author report excellent clinical outcomes.
Figure A demonstrates a proximal migration of the humerus resulting in femoralization of the humeral head and acetabularization of the acromion from a massive rotator cuff tear.
Incorrect answers:
Question 33
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical management has failed to provide relief. What is the treatment of choice?
Explanation
REFERENCES: Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.
Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
Question 34
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?
Explanation
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006. Question 74
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?
Discoid meniscus
Posterolateral comer injury
Vertical meniscal tears
Middle third lateral meniscal tears
Popliteus tendon tears
DISCUSSION: Lateral meniscal cysts often arise from myxoid degeneration that progresses from the meniscal center and then outside the meniscus. Horizontal cleavage tears are commonly associated with the condition.
Cysts of the lateral meniscus are most commonly the consequence of a tear located in the medial third. If the
tear communicates with the joint, arthroscopic partial meniscectomy and cyst decompression are indicated. If the tear does not open into the joint, arthroscopy should be followed by an open cystectomy.
REFERENCES: Hulet C, Souquet D, Alexandre P, et al: Arthroscopic treatment of 105 lateral meniscal cysts with 5-year average follow-up. Arthroscopy 2004;20:831-836.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part I. Macroscopic and histologic findings. Clin Orthop
Relat Res 1980;146:289-300.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part II. Horizontal cleavages and lateral cysts. Clin Orthop Relat Res 1980:146:301-307.
Question 35
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
REFERENCES: Gambardella RA: Techical pitfalls of patellofemoral surgery. Clin Sports Med 1999;18:897-903.
Post WR: Clinical evaluation of patients with patellofemoral disorders. Arthroscopy 1999;15:841-851.
Question 36
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
REFERENCES: Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Fahrer H, Rentsch HU, Gerber NJ, et al: Knee effusion and reflex inhibition of the quadriceps: A bar to effective retraining. J Bone Joint Surg Br 1988;70:635-638.
Question 37
By which mechanism can a true aneurysm of the ulnar artery result?
Explanation
Question 38
Which component position is associated with poor patellar tracking during total knee arthroplasty (TKA)?
Explanation
Internal malrotation of the femoral or tibial component is associated with lateral tracking of the patella in TKA. Lateral placement of the femoral component and medial placement of the patella component can aid in preventing lateral tracking of the patella. Varus alignment of the proximal tibia has not been associated with patella maltracking.







RESPONSES FOR QUESTIONS 106 THROUGH 109
Immobilization/nonsurgical management
Irrigation and debridement
stage reimplantation total knee arthroplasty (TKA)
Increased constraint/polyethylene exchange
Revision of the femoral component only
Revision of the tibial component only
Revision of both components
Revision of the patellar component
Select the treatment listed above that most appropriately addresses each scenario described below.
Question 39
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 40
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
Question 41
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management? Review Topic
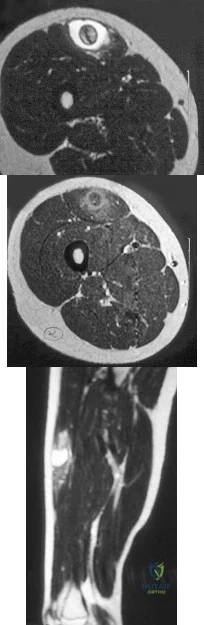
Explanation
Question 42
BMP is FDA approved for well-defined medical conditions in limited patient populations. In which of the following clinical scenarios is use of rhBMP-2 FDA approved?
Explanation
rhBMP-2 is also FDA approved for use in open tibial shaft fractures stabilized with an IM nail and treated within 14 days of initial injury. rhBMP-7 has received FDA humanitarian device exemption approval as an alternative to autograft in recalcitrant long bone nonunions where use of autograft is unfeasible and alternative treatments have failed. It is also approved as an alternative to autograft in compromised patients (with osteoporosis, smoking or diabetes) requiring revision posterolateral/intertransverse lumbar fusion for whom autologous bone and bone marrow harvest are not feasible or are not expected to promote fusion.
Epstein reviewed the indications for rhBMP-2 use and its off-label use. She found that
anterior cervical surgery with BMP2 led to dysphagia and airway complications. With posterior lumbar spine surgery, complications included vertebral osteolysis (bone resorption) and ectopic bone formation/heterotopic ossifications, which made revision surgery difficult.
Burkus et al. prospectively compared 46 patients undergoing single-level ALIF with BMP-2 vs with autograft in an industry sponsored study. They found that patients receiving BMP-2 had higher rates of fusion and improvement in pain and neurologic status at 12 and 24 months compared with autograft, and there were no adverse events. They recommend rhBMP-2 in ALIF procedures to eliminate pain and scarring from iliac crest bone harvest.
Illustration A shows the FDA approved combination of INFUSE (rhBMP-2) and LT-CAGE device.
Incorrect Answers:
Question 43
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of
Explanation
REFERENCES: Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: Long-term follow-up of 29 cases treated by microvascular bone transfer. Clin Orthop 1995;314:37-44.
Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV: Congenital pseudarthrosis of the tibia associated with neurofibromatosis - 1: Treatment with Ilizarov’s device. J Pediatr Orthop 1997;17:675-684.
Anderson DJ, Schoenecker PL, Sheridan JJ, Rich MM: Use of an intramedullary rod for the treatment of congenital pseudarthrosis of the tibia. J Bone Joint Surg Am 1992;74:161-168.
Question 44
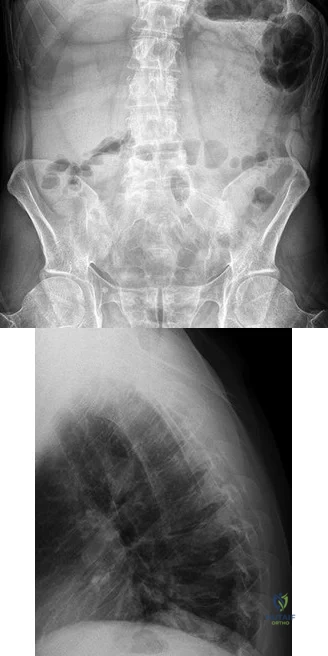
A B Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
Explanation
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. View Abstract at PubMed
Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. View Abstract at PubMed
Question 45
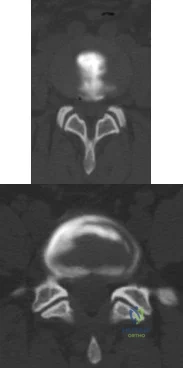
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time? Review Topic
Explanation
sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter.
Question 46
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. What imaging study is most appropriate to determine treatment options for this patient?
Explanation
Question 47
What is the most common surgical cause of the foot deformity shown in Figure 9?
Explanation
REFERENCES: Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Myerson MS, Komenda GA: Results of hallux varus correction using an extensor brevis tenodesis. Foot Ankle Int 1996;17:21-27.
Question 48
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed? Review Topic
Explanation
Question 49
Figures 129a through 129b are the radiographs and MRI and CT scans of the lumbar spine of a 10-yearold premenarchal girl who has back pain and scoliosis. What is the most likely etiology of her scoliosis?

Explanation

Question 50
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 51
The cavovarus deformity associated with Charcot-Marie-Tooth (CMT) disease is caused by which of the following?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-143.
Charcot-Marie-Tooth Disease (CMT) Penn State Hershey Medical Center.
www.hmc.psu.edu/healthinfo/c/cmt.htm
Question 52
Which of the following nerves is most commonly injured during arthroscopy of the ankle?
Explanation
Question 53
The Coleman block test is used to test for Review Topic
Explanation
Question 54
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 55
-What is the most appropriate initial treatment for her condition?
Explanation
This patient has a history most consistent with multidirectional instability. A lax capsule causes subluxation of the shoulder and strain on the rotator cuff and may result in pain and instability. The capsule is most closely associated with the cause of her problem. Initial treatment for multidirectional instability is physical therapy focusing on restoring balance to the shoulder with rotator cuff and scapular stabilization exercises. Nonsurgical therapy should be protracted and is the mainstay of treatment in this scenario. This patient has exhausted all nonsurgical measures and is now a candidate for surgical reconstruction. Capsular plication will best address the lax capsule and provide the best option for reducing her symptoms. The rotator cuff and biceps tendon may be secondarily strained but are not the primary sources of the problem. The brachial plexus does not address the etiology, but rather the symptoms that may occur as a result of instability of the shoulder joint.
Complete rest will not alleviate the patient's underlying condition because the shoulder girdle may still be weak and symptoms likely will return. A corticosteroid injection and arthroscopic surgery are too invasive as initial treatment for this condition. Arthroscopic rotator cuff repair, a biceps tenodesis, and superior labral anterior-posterior repair are unlikely to result in symptomatic improvement for this patient and are not associated with pathologic findings in the setting of multidirectional instability.
Question 56
During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
Explanation
REFERENCE: Bingol H, Cingoz F, Yilmaz AT, et al: Vascular complications related to lumbar disc surgery: J Neurosurg 2004;100:249-253.
Question 57
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Den Hartog BD: Flexor hallucis longus transfer for chronic Achilles tendinosis. Foot Ankle Int 2003;24:233-237.
Question 58
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
Explanation
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
Question 59
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them? Review Topic
Explanation
Question 60
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
REFERENCES: Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.
Question 61
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 62
-Ten or more years after severe polytrauma, premenopausal women, compared to men
Explanation
Question 63
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings? Review Topic
Explanation
Question 64
Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 65
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?
Explanation
REFERENCES: Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393.
Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Skrede O: Non-osteogenic fibroma of bone. Acta Orthop Scand 1970;41:362-380.
Question 66
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
REFERENCE: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 67
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle? Review Topic

Explanation
such as Parsonage-Turner syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
Question 68
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
REFERENCES: Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Shaffer B, Tibone JE, Kerlan RK: Frozen shoulder: A long-term follow-up. J Bone Joint Surg Am 1992;74:738-746.
Question 69
A 47-year-old obese man with a body mass index of 42 comes in with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of his UKA secondary to poor patient selection. This young, heavy man likely loosened his component secondary to the ongoing varus alignment of the knee and his elevated weight. Despite this likely scenario, the next step is to determine if an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order an ESR and CRP to determine if aspiration is warranted. If laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.

CLINICAL SITUATION FOR QUESTIONS 69 THROUGH 72
Figures 69a through 69c are the radiograph and MR images of a 37-year-old woman who has had a 2-month history of left hip pain.
Question 70
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 71
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Goldenberg RR, Campbell CJ, Bonfiglio M: Giant cell tumor of bone: An analysis of two hundred and eighteen cases. J Bone Joint Surg Am 1970;52:619-664.
Question 72
A patient with a valgus knee and lateral compartment bone loss undergoes a total knee arthroplasty using posterior condylar referencing instrumentation. Six months after surgery, the patient reports significant anterior knee pain, and radiographs reveal severe lateral patellar tilt. Management should consist of
Explanation
REFERENCES: Berger RA, Della Valle CJ, Rubash HE: Patellofemoral problems in total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1245-1258.
Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop 1995;321:168-172.
Question 73
A 61-year-old right-hand-dominant woman falls down the stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
Explanation
<3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range
of motion is important to avoid stiffness.
Question 74
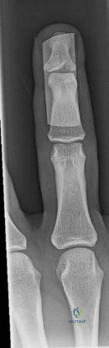
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew Eikenella corrodens . The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?

Explanation
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection and not a tumor, and MRI already has provided enough diagnostic information.
Question 75
A patient with an unstable pelvic ring injury has just undergone an emergent laparotomy and currently has a packed abdomen. Stabilization of the pelvic ring is performed with an anterior external fixator. What is an advantage of using an external fixator with pins in the iliac crest rather than pins in the anterior inferior iliac spine?
Explanation
Question 76
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T 1 -weighted, sagittal T 2 -weighted, axial T 1 -weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 4241-4252.
Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:1-11.
Question 77
below show the radiograph and the MRI scan obtained from a year-old woman with a month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge
score cannot be determined presurgically.
Question 78
What is the most common site of metastases from a soft-tissue sarcoma?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 255-259.
Question 79
-A 37-year-old woman has a 2-month history of weakness in thumb and finger extension, but has normal radial deviation during extension of the wrist. An MRI scan of her forearm shows no abnormality. She does not recall any traumatic event. Needle electromyography findings show fibrillations and reduced
Explanation

Question 80
Which factor is most important when attempting to prevent interbody graft subsidence?
Explanation
Osteoporosis can affect all aspects of spinal stability and is the most critical factor regarding spinal implant failure. Burring of the end plates may decrease strength of the interface with the uncovering of "softer" cancellous bone. Increasing the surface contact area may help prevent subsidence but is not as important as bone quality. Stress shielding through rigid fixation may lead to construct failure.
RECOMMENDED READINGS
Benzel E (ed): Biomechanics of Spine Stabilization. Rolling Meadows, IL, American Association of Neurological Surgeons, 2001, pp 446-447.
Goldhahn J, Reinhold M, Stauber M, Knop C, Frei R, Schneider E, Linke B. Improved anchorage in osteoporotic vertebrae with new implant designs. J Orthop Res. 2006 May;24(5):917-25. PubMed PMID: 16583445. View Abstract at PubMed
Question 81
The most compelling clinical reason to convert a hip arthrodesis to a total hip arthroplasty is that the latter
Explanation
REFERENCES: Strathy GM, Fitzgerald RH Jr: Total hip arthroplasty in the ankylosed hip: A ten-year follow-up. J Bone Joint Surg Am 1988;70:963-966.
Lubahn JD, Evarts CM, Feltner JB: Conversion of ankylosed hips to total hip arthroplasty. Clin Orthop 1980;153:146-152.
Question 82
-What is the most likely area of injury?
Explanation
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
Question 83
A patient has multidirectional instability of the shoulder that has not responded to nonsurgical management. Successful surgical treatment will most likely include which of the following? Review Topic
Explanation
instability treated surgically following failure to respond to nonsurgical management has been shown to be associated with classic Bankart lesions, Hill-Sachs defects, glenoid chondral lesions, and even SLAP lesions (Werner). However, these lesions were seen in a lower percentage than that found for unidirectional anterior dislocations. Likewise, these lesions do not appear to be significant in influencing treatment in the majority of patients.
Question 84
A 12-year-old gymnast has had elbow pain for 4 weeks. She denies any specific trauma to the elbow. Examination reveals lateral pain and no instability on testing. Range of motion is as follows: 15 degrees, loss of elbow extension, normal flexion, and normal pronation and supination. Radiographs reveal a 3- x 7-mm radiolucency of the capitellum. A T1-weighted MRI scan reveals a single solitary lesion, and T2-weighted images show no signal around the lesion. There are no intra-articular loose bodies. Appropriate management should include which of the following? Review Topic
Explanation
Question 85
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
REFERENCES: Denis F, Davis S, Comfort T: Sacral fractures: An important problem.
A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.
Wood KB, Denis F: Fractures of the sacrum and coccyx, in Vacarro AR (ed): Fractures of the Cervical, Thoracic and Lumbar Spine. New York, NY, Marcel Dekker, 2003, pp 473-488.
Question 86
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 1010-1017.
Question 87
Figures 1 through 5 show the radiographs obtained from a 37-year-old man who has a 10-year history of right, ulnar-sided wrist pain and a volar ulnar prominence with wrist supination. Approximately 20 years ago, he had a forearm injury that was definitively treated in a long arm cast. What surgical treatment option is most likely to improve his symptoms and maintain pronosupination?

Explanation
The patient sustained a radial shaft fracture with subsequent apex volar malunion. As a result, his distal ulna subluxates volarly with wrist supination. Radiographs of the wrist reveal minimal arthritic changes. The most appropriate treatment option is to surgically correct his radial shaft malunion, which would indirectly address his DRUJ instability. A DRUJ ligament reconstruction or triangular fibrocartilage complex repair could be used to augment DRUJ stability; however, they might be unnecessary after correction of the radial shaft malunion. A DRUJ ligament reconstruction alone would not achieve stability of the DRUJ joint and maintain full wrist pronosupination. An ulnar head implant arthroplasty would not be reliable in eliminating the instability or the pain. Similarly, a one-bone forearm procedure might
improve the patient's pain and instability but at the cost of abnormal wrist and forearm mechanics and kinematics.
Question 88
A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
Explanation

OrthoCash 2020
Question 89
You are evaluating a patient with recurrent patellar instability who has failed conservative management. MRI demonstrates articular cartilage loss in the patella. In addition to a cartilage restoration procedure, you recommend the procedure depicted in Figures A and B. Which of the following imaging findings best supports your decision? Review Topic

Explanation
Recurrent patellar instability is often associated with chondral lesions of the patellofemoral joint. In addition to managing the cartilage injury, the underlying etiology of the instability must also be addressed to ensure a successful outcome. Patellar instability may arise from coronal or rotational malalignment, patella alta, trochlear dysplasia or damage to soft tissue restraints including the medial patellofemoral ligament (MPFL). Rotational malalignment, defined by a TT-TG distance > 20mm, can be addressed by AMZ. Medialization of the tubercle restores a normal TT-TG distance while anteriorization of the tubercle unloads patellofemoral contact forces.
Beck et al performed a cadaveric study measuring patellofemoral contact pressures on the trochlear surface following AMZ. They found that anteromedialization decreased the mean contact pressures and shifted contact pressures to the medial trochlea. The authors concluded that while this procedure successfully unloads the lateral trochlea, it likely has minimal benefit for central chondral defects and may be detrimental for medial chondral defects where contact pressures are increased.
Strauss et al authored a review article detailing the surgical treatment options for patellofemoral cartilage lesions, including concomitant realignment/unloading procedures. AMZ is designed to correct rotational malalignment while unloading the patellofemoral compartment in the setting of cartilage restoration surgery. While AMZ has demonstrated good outcomes for lesions located in the lateral facet or distal
pole of the patella, poor outcomes have been seen with medial facet or central trochlear lesions.
Figures A and B are the AP and lateral radiographs, respectively, of a knee s/p AMZ, also know as a Fulkerson procedure. Illustration A is an algorithm detailing the approach to recurrent patellar instability in both skeletally immature and mature patients. Illustration B demonstrates how to measure the TT-TG distance, the distance between two lines drawn perpendicular to the posterior condylar axis to the tibial tubercle and deepest portion of the trochlear groove (normal 8-10mm). Illustration C depicts the measurement of the femoral trochlear angle or sulcus angle (normal 137°
+/- 8°). Illustration D shows how to measure lateral patellar tilt (normal < 5°). Illustration E is a postoperative radiograph after AMZ. A long (> 5cm) and thick (> 0.75cm) osteotomy cut is required to allow adequate fixation with two screws.
Incorrect Responses:
Question 90
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 91
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a “foot” fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
REFERENCES: Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 92
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 93
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. J Shoulder Elbow Surg 1999;8:17-21.
Question 94
Figures 45a and 45b show the radiographs of a 46-year-old man who reports the acute onset of right knee pain and is unable to bear weight on the extremity. His medical history is unremarkable. The next most appropriate step in management should consist of
Explanation
REFERENCE: Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 95
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?
Explanation
REFERENCES: Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855.
Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases.
J Shoulder Elbow Surg 1992;1:283-286.
Question 96
Kinematic analysis of the medial and lateral menisci has demonstrated that the lateral meniscus has which of the following characteristics compared with the medial meniscus?
Explanation
REFERENCES: Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. New York, NY, Churchill Livingstone, 2001, vol 1, p 474.
Thompson WO, Thaete FL, Fu FH, et al: Tibial meniscal dynamics using 3D reconstructions
of MR images, in Proceedings of the Orthopaedic Research Society 1990;389.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy
of Orthopaedic Surgeons, 2005, pp 15-28.
Question 97
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
Explanation
REFERENCES: Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
Question 98
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 99
A 24-year-old man is involved in a motor vehicle accident at 60 mph. He sustains multiple injuries including an intra-abdominal injury requiring a splenectomy and a closed right femoral shaft fracture. Which variable will best indicate the patient's resuscitation status when deciding whether to proceed with definitive care of the fracture at the conclusion of the laparotomy? Review Topic
Explanation
Question 100
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
