OITE & ABOS Orthopedic Board Prep MCQs: Trauma, Shoulder & Deformity | Part 202

Key Takeaway
This page offers Part 202 of a comprehensive OITE/ABOS orthopedic board review. It features 100 high-yield MCQs for orthopedic surgeons and residents preparing for certification exams. Questions mirror OITE/AAOS formats, covering Deformity, Fracture, Ligament, Shoulder, Trauma. Study with detailed explanations to ace your boards.
About This Board Review Set
This is Part 202 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 202
This module focuses heavily on: Deformity, Fracture, Ligament, Shoulder, Trauma.
Sample Questions from This Set
Sample Question 1: Figure 91 shows the radiograph of a 57-year-old man who fell 6 feet off a ladder. He is neurovascularly intact but reports shoulder pain. What is the most appropriate acute treatment for this patient?...
Sample Question 2: When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?...
Sample Question 3: An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilate...
Sample Question 4: Dorsal intercalated segment instability (DISI) describes which carpal deformity?...
Sample Question 5: A 33-year-old female with generalized ligamentous laxity is diagnosed with spontaneous atraumatic subluxation of the sternoclavicular joint. She notes mild, intermittent pain and a small amount of prominence to that area. What is the most a...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 91 shows the radiograph of a 57-year-old man who fell 6 feet off a ladder. He is neurovascularly intact but reports shoulder pain. What is the most appropriate acute treatment for this patient?

Explanation
Question 2
When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?
Explanation
Question 3
An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilateral pubic rami fractures with minimal displacement. He has a systolic blood pressure of 80/40 mm Hg despite fluid resuscitation. A radiograph is shown in Figure 17. Spiral CT does not identify any thoracic or abdominal injuries. What is the next most appropriate step in management?
Explanation
REFERENCES: Althausen PL, Lee MA, Finkemeier CG: Scapulothoracic dissociation: Diagnosis and treatment. Clin Orthop 2003;416:237-244.
Witz M, Korzets Z, Lehmann J: Traumatic scapulothoracic dissociation. J Cardiovasc Surg 2000;41:927-929.
Question 4
Dorsal intercalated segment instability (DISI) describes which carpal deformity?
Explanation
Question 5
A 33-year-old female with generalized ligamentous laxity is diagnosed with spontaneous atraumatic subluxation of the sternoclavicular joint. She notes mild, intermittent pain and a small amount of prominence to that area. What is the most appropriate treatment at this time?

Explanation
Question 6
A 22-month-old child has scrapes and bruises on his head and a severe deformity of the forearm after being thrown from a car as an unrestrained passenger in a motor vehicle accident. Examination reveals a Glasgow Coma Scale score of 12. Prior to treatment of the forearm, management should include
Explanation
REFERENCES: Hall DE: Head injuries, in Hoekelman RA (ed): Primary Pediatric Care. St Louis, Mo, Mosby, 1997, pp 1709-1712.
Nelson WE, Behrman RE, Kliegman RM (eds): Nelson Essentials of Pediatrics. Philadelphia, Pa, WB Saunders, 1998, p 712.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 123-130.
Question 7
below show the radiographs obtained from an year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 8
Which of the following pieces of equipment currently offers the greatest opportunity for lowering the number of equestrian injuries?
Explanation
REFERENCES: Ball CG, Ball JE, Kirkpatrick AW, et al: Equestrian injuries: Incidence, injury patterns, and risks factors for 10 years of major traumatic injuries. Am J Surg 2007;193:636-640.
Frankel HL, Haskell R, Digiacomo JC, et al: Recidivism in equestrian trauma. Am Surg 1998;64:151-154.
A 38-year-old man is three quarters of the way through the Hawaiian Ironman events run in a temperature of 60°F. He is sweating profusely and suddenly collapses. Prior to this he had been drinking large amounts of bottled water at every water stop. What is the most likely diagnosis?
Hypernatremia
Hypothermia
Hyponatremia
Subendocardial myocardial infarction
Ruptured berry aneurysm
DISCUSSION: Hyponatremia is often seen in endurance athletes such as triathloners, ultramarathoners, and marathoners after prolonged exertion. It is commonly attributed to excess free water intake that fails to replete massive sodium losses that result from sweating as reported by O’Connor. Exercise-induced hyponatremia is generally asymptomatic, particularly in patients in whom the sodium is only mildy reduced. Up to 10% of ultradistance athletes have a sodium level of 135 mEq/L or less, but those who are symptomatic usually have a sodium level of 125 mEq/L as reported by Noakes and O’Connor. The best way to prevent hyponatremia is to maintain the proper volume and types of fluid intake to ensure fluid balance during exercise. Beverages containing carbohydrates in concentrations of 4% to 8% (ie, “sports drinks”) are recommended for athletes participating in exercise lasting more than an hour (eg, marathon runners, etc.) To avert brainstem herniation and death, severe, acute hyponatremia requires rapid correction. Oral rehydration with salty solutions is safe and effective in patients with mild symptoms.
Too rapid correction has been reported to cause central pontine myelinolysis; therefore, correction ought to be performed slowly. Hypernatremia, hypothermia, subendocardial myocardial infarction, or ruptured berry aneurysm are unlikely in this scenario.
REFERENCES: O’Connor RE: Exercise-induced hyponatremia: Causes, risks, prevention, and management. Cleve Clin J Med 2006;73:S13-S18.
Noakes T: Hyponatremia in distance runners: Fluid and sodium balance during exercise. Curr Sports Med Rep
2002;1:197-207.
Laureno R, Karp BI: Myelinolysis after correction of hyponatremia. Ann Int Med 1997;126:57-62. Question 50
A 20-year-old male tennis player reports the acute onset of ulnar-sided wrist pain after hitting a forehand shot. Examination reveals dorsoulnar tenderness and minimal swelling. The pain is recreated with supination, wrist flexion, and ulnar deviation. Radiographs are normal. What structure is most likely involved?
Ulnar styloid
Flexor carpi radialis tendon
Extensor carpi ulnaris tendon
Scapholunate ligament
Transverse carpal ligament PREFERRED RESPONSE: 3
DISCUSSION: Extensor carpi ulnaris (ECU) lesions produce pain at the dorsoulnar aspect of the wrist, particularly during wrist supination, wrist flexion, and ulnar deviation. It has been frequently described in tennis players. Most ECU tenosynovitis can be successfully treated nonsurgically with immobilization techniques. Surgical treatment is generally indicated for ECU tenosynovitis or tendinopathy that does not respond to rest. Anatomically, the ECU retinaculum can rupture and the tendon can leave its sheath. With supination, the tendon can leave the sheath and then return to its position during pronation.
REFERENCES: Montalvan B, Parier J, Brasseur JL, et al: Extensor carpi ulnaris injuries in tennis players: A study of 28 cases. Br J Sports Med 2006;40:424-429.
Allende C, Le Viet D: Extensor carpi ulnaris problems at the wrist: Classification, surgical treatment and results. J Hand Surg Br 2005;30:265-272.
Question 9
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?
Explanation
REFERENCES: Ghalambor N, Warner JJP: Arthroscopic capsular release: Evolution of the technique and its applications. Tech Shoulder Elbow Surg 2000;1:52-60.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 10
Of the following variables, which has the strongest influence on external fixator stiffness?
Explanation
Question 11
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Bell SN, Morrey BF, Bianco AJ Jr: Chronic posterior subluxation and dislocation of the radial head. J Bone Joint Surg Am 1991;73:392-396.
Question 12
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves?
Explanation
REFERENCE: Beldner S, Zlotolow DA, Melone CP, et al: Anatomy of the lateral antebrachial cutaneous and superficial radial nerves in the forearm: A cadaveric and clinical study. J Hand Surg Am 2005;30:1226-1230.
Question 13
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
REFERENCES: Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257.
Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
Mileti J, Boardman ND III, Sperling JW, et al: Radiographic analysis of polyethylene glenoid components using modern cementing techniques. J Shoulder Elbow Surg 2004;13:492-498.
Question 14
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
Explanation
REFERENCES: Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34.
Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 15
Figure A shows intraoperative images of a right knee in an 8-year-old boy after he sustained an injury. Which of the following is the most common indication for performing this procedure? Review Topic

Explanation
Arthroscopic treatment of lateral discoid meniscus injuries has the advantages of reducing trauma, precise resection or repair of the meniscus and saucerization of the remaining discoid meniscus. Operative treatment is usually limited to patients with pain and mechanical symptoms that are undergoing partial meniscectomy or repair. Asymptomatic discoid meniscus without tears are not considered a surgical indication for routine saucerization.
Kramer et al. reviewed the diagnosis and treatment of traumatic discoid meniscal tears in children. They report that knee shape, size and skeletal maturity must be considered when determining the optimal method of repair. However, all symptomatic torn discoid menisci are best treated with saucerization and repair.
Good et al. looked at the arthroscopic techniques of discoid meniscus repair. Arthroscopic saucerization was successful in 28 of 30 knees and meniscal repair in 23 of 30 knees. At final follow-up, all patients exhibited full knee flexion beyond 135 degrees. In 3 of 30 patients there was residual knee pain, and four reported intermittent mechanical symptoms.
Figure A shows a series of arthroscopic images of the right knee lateral compartment. There is a sequential saucerization of the discoid meniscus.
Incorrect Answers:
(SBQ13PE.83) 8-year-old boy complains of intermittent painless clicking in his knee. His physical examination is normal. His family doctor orders an MRI, which reveals an incomplete lateral discoid meniscus without evidence of tear. What is the most appropriate treatment? Review Topic
Observation only
Diagnostic arthroscopy
Saucerization of meniscus
Saucerization of meniscus and microfracture
Saucerization and stabilization of the mensicus
The clinical presentation is consistent with a asymptomatic discoid meniscus. The most appropriate treatment at this time would be observation only.
MRI scans of the knee are very sensitive for identifying discoid menisci. Diagnosis is usually made when there are 3 or more 5mm sagittal MRI images showing meniscal continuity. Treatment is mostly focused on conservative modalities. Asymptomatic tears are usually treated with observation only. Saucerization is indicated for recurrent locking, swelling, persistent pain, or radiographic evidence of a meniscal tear.
Watanabe et al. described three types of discoid lateral menisci based on arthroscopic appearance. In this classification, discoid menisci with normal peripheral attachments are either type I (complete) or type II (incomplete). Type III discoid menisci, the so-called Wrisberg ligament type, are lacking posterior capsular attachments with the exception of the posterior meniscofemoral ligament.
Kramer et al. looked at the presentation of pediatric knee pain and discoid meniscus. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the meniscus.
Illustration A shows the cross-section of normal meniscus. Illustration B shows the Watanabe classification.
Incorrect Answers:
Question 16
.Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg. The histopathology is shown in Figure 59c. A radiograph of her leg showed no mineralizations or osseous erosions. The chromosomal abnormality that is associated with this disease is
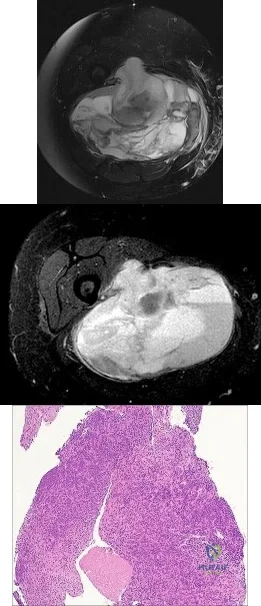
Explanation
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The patient first noticed it about 6 months after she had a low-impact fall. The general surgeon evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient underwent a surgical procedure to remove the mass.
Question 17
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
REFERENCES: Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Weber TG, Manoli A II: Compartment syndromes of the foot. Foot Ankle Clin 1999;4:473-486.
Question 18
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 19
A 14-year-old male soccer player was seen initially in the emergency room 1 week ago after an acute right hip injury during a soccer tournament. The patient reports that the hip pain has improved, but still requires crutches for long distance ambulation. His radiograph is seen in Figure A. What would be the next most appropriate step in management? Review Topic

Explanation
The diagnosis of an avulsion fracture of the anterior superior iliac spine is made on the basis of: 1. History (sudden contraction of the sartorial and tensor fasciae latae muscle), 2. Physical findings (tenderness over the anterior superior iliac spine [ASIS] and pain with straight-leg raise), 3. Patient's age (most commonly in adolescents or young adults), and 4. Radiographs (confirmed fracture on standard views of the pelvis). Treatment of these injuries is almost always conservative with crutches and progressive weight-bearing activities as tolerated. The relative indications for operative treatment include displacement of the fracture fragment > 3 cm or painful non-union.
White et al. defined two types of anterior superior iliac spine avulsion fractures. A sartorius avulsion fracture (Type 1) usually occurs when sprinting. The fracture fragment is usually small and displaced anteriorly. The tensor avulsion fracture (Type 2) usually occurs when twisting the trunk (e.g. swinging a bat). This fragment is usually larger than Type 1 fractures and more likely to be displaced laterally.
Holden et al. reviewed pediatric pelvic fractures. They state that avulsion fractures of the anterior superior iliac spine are usually low-energy injures, and are not associated with other life-threatening injuries. They do not require an extensive workup (e.g. CT scanning)
Figure A is an antero-posterior view of the pelvis with a small right-sided avulsion fracture of the anterior superior iliac spine.
Incorrect Answers:
Question 20
..Figure 93 is the radiograph of a 72-year-old woman. Treatment includes fixation of the ulna. What options are recommended for the radius?
Explanation

Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
Question 21
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of
Explanation
REFERENCES: Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737.
Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Blair B, Rokito AS, Cuomo F, et al: Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
Question 22
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?
Explanation
REFERENCES: Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 23
A 72-year-old woman has had progressively increasing pain in the right knee for the past 6 months. She denies any trauma and has no pain in any other joints, but she notes occasional swelling in the knee and a catching sensation. Figures 31a and 31b show the plain radiographs and Figure 31c shows the MRI scan. Treatment should consist of
Explanation
REFERENCES: Lotke PA, Ecker ML: Osteonecrosis of the knee. J Bone Joint Surg Am 1988;70:470-473.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 24
A B C D E Figures 45a through 45c are the MR images of a 22-year-old woman who has had 6 months of ankle pain related to activities of daily living. She recently completed a course of cast immobilization and protected weight bearing without symptom resolution. Figures 45d and 45e are the intraoperative arthroscopy images after minimal probing. What is the most appropriate treatment?
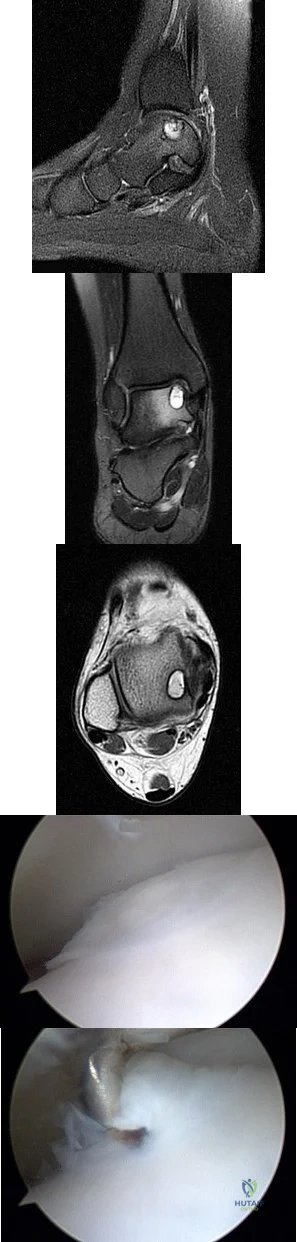
Explanation
The MR images reveal a large cystic medial talar dome osteochondral lesion (OCL) in a patient who has failed nonsurgical treatment. Ankle fusion is inappropriate because the patient has an otherwise normal ankle. Arthroscopic debridement and drilling are appropriate for smaller (< 1.5 cm sq) noncystic lesions. Retrograde drilling and bone grafting is an option in the treatment of cystic OCL if the cartilage surface is intact; however, intraoperative arthroscopy images show that this patient's cartilage surface is unstable. Osteochondral allografts and autografts are effective in the treatment of large cystic talar dome OCLs but are not appropriate for the initial surgical treatment of smaller lesions like this one.
RECOMMENDED READINGS
Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71. doi: 10.1302/0301-620X.96B2.31637. Review. PubMed PMID:
Question 25
Which of the following best describes the course of the ulnar nerve in the midforearm?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 26
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
Explanation
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit. Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon
repair causes limited flexion of the injured finger.
Question 27
What is the recommended optimal timing of presurgical antibiotic administration to prevent infection in patients undergoing total joint replacement surgery?
Explanation
Question 28
The spring ligament of the foot connects what two bones?
Explanation
REFERENCES: Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Davis WH, Sobel M, DiCarlo EF, et al: Gross, histological and microvascular anatomy and biomechanical testing of the spring ligament complex. Foot Ankle Int 1996;17:95-102.
Question 29
A 65-year-old man who underwent cemented right total hip arthroplasty 6 years ago now reports acute pain for the past week. He denies any trauma, recent illnesses, or symptoms other than pain. Plain radiographs show possible loosening of the femoral component. A normal result from which of the following studies will most specifically rule out infection?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 137-148.
Question 30
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Wootten ME, Kadaba MP, Cochran GV: Dynamic electromyography II: Normal patterns during gait. J Orthop Res 1990;8:259-265.
Question 31
below show the radiographs obtained from a year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m 2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Explanation
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 32
A 17-year-old high school football linebacker sustains an injury while making a tackle. His initial symptoms are right shoulder pain, bilateral biceps weakness, and right arm numbness. The symptoms only last a few minutes, and he continues to play in the game. He tells his parents after the game, and they bring him to your office for evaluation the next day. He no longer has any symptoms, and his examination findings and cervical spine radiographs are normal. What is the best next step?
Explanation
Question 33
A teenage female is referred to you for evaluation of curvature in her back that was discovered on routine school screening. She is diagnosed with adolescent idiopathic scoliosis. In which of the following scenarios is a bracing program the most appropriate treatment? Review Topic

Explanation
The treatment of adolescent idiopathic scoliosis (AIS) depends on the magnitude and location of curve as well skeletal maturity of the patient. For curves less than 20 degrees, observation is appropriate until skeletal maturity, with closer intervals during
times of peak growth. Curves between 20-25 and 45 degrees in patients who are Risser stage 0,1 or 2 are best treated with bracing to stop progression. Curves with an apex at T7 or below are typically treated with a Boston brace. Curves over 50 degrees generally warrant a discussion about surgery to prevent progression past maturity.
In a landmark study, Weinstein et al. evaluated both a randomized and preference based cohort of bracing versus observation. The trial was stopped early due to efficacy of bracing. The rate of treatment success was 72% after bracing and 48% after observation. Treatment success was strongly correlated to time of brace wear.
Schlenzka et al. reviewed indications, treatment, and complications associated with brace treatment of AIS. They state that further evidence is necessary to evaluate the efficacy of bracing in AIS.
Figure 1, 2, and 3 are radiographs depicting Risser stage 0, 1, and 4 respectively. Illustration B shows radiographs of all Risser stages. Illustration C is the Lenke classification system for idiopathic scoliosis.
Incorrect Answers:
Question 34
Surgical arthroscopy performed 1 week after injury presents increased risk for
Explanation
The MR images show injuries to the ACL, PCL, and PLC consistent with a knee dislocation. The optimal timing of surgery after multiligament knee injury remains unclear. Two systematic reviews demonstrated superior clinical outcome scores after early treatment, including higher mean Lysholm scores and a higher percentage of good/excellent International
Knee Documentation Committee scores. Early treatment was associated with increased residual anterior knee instability but no difference in posterior instability, varus laxity, or valgus laxity. Although numbers were limited, the average range of motion and rate of extension loss of at least 5 degrees was similar between groups. More patients in the early-treatment group demonstrated a higher rate of flexion loss of 10 or more degrees and an increased need to undergo a second procedure to address arthrofibrosis, including manipulation under anesthesia and arthrolysis. Return to work did not significantly differ between groups, but return to sports was lower in the early-treatment group. Evidence demonstrates a higher rate of low-energy mechanisms resulting in multiligament knee injury and an increased odds ratio for complications among obese (= 30 degrees kg/m2 patients, including wound complications and neurovascular injury. The complication rate increased 9.2% for every 1-point increase in body mass index. There is no association between complication rate and age, injury mechanism, or timing of surgery. Orthopaedic surgeons performing arthroscopy during the early postinjury period must be mindful of the extensive soft-tissue damage present in these patients, including potential capsular defects. Use of high-pressure irrigation can lead to substantial fluid extravasation into the thigh or lower leg compartments, placing patients at increased risk for compartment syndrome. In addition to avoiding high-pressure irrigation, some orthopaedic surgeons have advocated the creation of generous capsular incisions during portal establishment to allow for ready egress of irrigation fluid from the portal sites rather than into soft tissues.
RESPONSES FOR QUESTIONS 85 THROUGH 88
Excessive medial placement of coracoid autograft
Excessive lateral placement of coracoid autograft
Excessive inferior dissection during the procedure
Excessive retraction and dissection of the medial portion of the conjoint tendon
A 20-year-old right-hand-dominant football player sustained a traumatic shoulder dislocation during a tackle. He has had multiple recurrent dislocations, and radiographs reveal anterior glenoid bone loss. He underwent a Latarjet procedure. Match the most likely complication described below with the surgical error listed above.
Question 35
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?
Explanation
REFERENCES: Sun TC, Swee TC: Chondrosarcoma in Maffucci’s syndrome. J Bone Joint Surg Am 1985;67:1214-1219.
Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Began WB: Dyschondroplasia and hemangiomata (Maffucci’s syndrome). Arch Intern Med 1958;102:544.
Question 36
-Figure is the radiograph of a 55-year-old veteran who developed avascular necrosis after a traumatic hip dislocation. He was treated with hemiarthroplasty 10 years ago and also has posttraumatic stress disorder and chronic pain. He has had multiple spinal surgeries and takes 30 mg of methadone daily. He now has severe groin pain and is unable to ambulate. Laboratory studies showed a C-reactive protein level of 0.2 mg/L (reference range, 0-3 mg/L), erythrocyte sedimentation rate of 50 mm/h (reference range, 0-20 mm/h), hip aspiration of 500/mm3 white blood cell count, 50% polynucleated cells, 30%monocytes, and 20% lymphocytes What is the most likely cause of his hip pain?
Explanation
Question 37
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T 1 - and T 2 -weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?
Explanation
REFERENCES: Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21.
Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing’s sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Lazar A, Abruzzo LV, Pollock RE, et al: Molecular diagnosis of sarcomas: Chromosomal translocations in sarcomas. Arch Path Lab Med 2006;130:1199-1207.
Question 38
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
REFERENCES: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000,
pp 12-13.
Lieber RL: Form and function of skeletal muscle, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 39
When obtaining grafts from a trochlear donor site during an osteochondral autograft transplantation procedure, where on the trochlea are the lowest contact pressures found? Review Topic
Explanation
Question 40
What type of thoracolumbar spinal injury is associated with an increased risk of neurologic deterioration following admission to the hospital?
Explanation
REFERENCES: Gertzbein SD: Neurologic deterioration in patients with thoracic and lumbar fractures after admission to the hospital. Spine 1994;19:1723-1725.
Magerl F, Aebi M, Gertzbein SD, et al: A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994;3:184-201.
Question 41
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of
Explanation
REFERENCES: Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 42
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
REFERENCES: AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. http://www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf
The Orthopaedic Surgeon’s Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. http://www.aaos.org/about/papers/ethics/1204eth.asp
AdvaMed Code of Ethics on Interactions with Health Care Professionals 2005. http://www.advamed.org/MemberPortal/searchresults.htm?query=Advamed%20Code%20of%20Ethics%20on%20Interactions%20with%20Health%20Care%20Professionals%202005
Question 43
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 44
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 28-29.
Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991,
pp 1255-1272.
Zancolli E: Reconstructive surgery in brachial plexus sequelae, in Gupta A, Kay S, Scheker L (eds): The Growing Hand. London, England, Mosby, 1999, p 807.
Question 45
A 47-year-old male with a history of a Putti-Platt procedure 20 years ago presents with right shoulder pain with decreased range-of-motion. Radiograph is shown in Figure A. What is the most accurate diagnosis? Review Topic

Explanation
Post-stabilization procedure arthritis is thought to occur due to changes in contact loading in the shoulder joint due to fixing the joint in an incongruent posistion. It can be severe and debilitating, and lead to arthroplasty as a salvage procedure. The Putti-Platt procedure involves a division of the subscapularis tendon and anterior capsule, and realignment of the lateral tendon stump and capsule sewn into the anterior glenoid neck capsular insertion. The "pants-over-vest" style of repair is then finished by sewing the medial tendon stump into the tuberosity, so that external rotation is significantly limited by the soft tissue imbrication. There is no coracoid transfer for this stabilization procedure.
Bigliani et al. reported on a series of similar patients who developed arthritis following surgery for recurrent glenohumeral dislocation. Authors have theorized that instability repair may excessively tighten the joint in one direction and cause a fixed subluxation in the direction opposite from the side of repair, leading to severe degenerative arthritis due to inappropriate contact loading. 77% of patients following arthroplasty after post-capsulorrhaphy arthropathy had an excellent or satisfactory outcome, with improved pain and range of motion.
Figure A demonstrates severe osteoarthrosis of the affected shoulder, with significant joint space narrowing, periarticular osteophyte formation, and subchondral sclerosis.
Incorrect Answers:
performed for traumatic dislocation, but the best answer choice for this stem is Answer 2.
Question 46
A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
Explanation
REFERENCES: Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370.
Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
Question 47
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Question 48
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
REFERENCES: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348.
Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 49
Use of long-term (at least 5 years) bisphosphonate medications for osteoporosis is associated with
Explanation
Fragility or osteoporotic fractures are common in postmenopausal women and older men and include fractures of the proximal humerus and distal radius and hip and vertebral compression fractures. The most reliable predictor of a fragility fracture is a past fragility fracture; consequently, it is important to elicit history. Assessment of vitamin D and calcium levels is important when treating these patients because many of them have low levels.
Use of bisphosphonates for treatment of osteoporosis results in atypical femur fractures and a decrease in risk for fragility fractures (including hip fractures). There also are reports of osteonecrosis of the mandible with prolonged use of these drugs. Current medical literature suggests stopping these drugs after 3 to 5 years to allow bone remodeling.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. View Abstract at PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone
Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 92 THROUGH 95
A 23-year-old man is involved in a motorcycle collision and sustains a displaced transcervical femoral neck fracture with an associated open comminuted femoral shaft fracture.
Question 50
With respect to femoral component design, stress relief osteopenia in the proximal femur following noncemented total hip arthroplasty appears to be most strongly influenced by the
Explanation
Question 51
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient participates in physical therapy for 8 weeks with his team's trainer but notes little improvement. What is the most appropriate next diagnostic step to determine the cause of his pain?

Explanation
used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 52
A 68-year-old man presents with severe right shoulder pain. He had a prolonged course of physical therapy and received several cortisone injections for his pain without improvement. Examination reveals pseudoparalysis of the right shoulder with a 20-degree external rotation lag with the shoulder adducted. With the shoulder placed in 90 degrees of abduction, he can actively externally rotate his shoulder. The patient was treated with a medialized reverse prosthesis shown in Figure A. Which of the following statement is true regarding this treatment option? Review Topic

Explanation
RTSA is most commonly indicated for rotator cuff arthropathy. However, indications for use now include shoulder pseudoparalysis, anterosuperior escape of the humeral head, acute 3 or 4-part proximal humerus fractures, and greater tuberosity fracture nonunions. Contraindications to RTSA included deltoid dysfunction, insufficient glenoid bone stock, and bony deficiency of the acromion.
Edwards et al. prospectively evaluated the risk of shoulder dislocation after reverse TSA. They found a significantly increased risk of dislocation (p=0.012) in patients with an irreparable subscapularis at time of surgery. There were no dislocations in the reparable group. Dislocations were more likely in patients with proximal humeral nonunions and failed prior arthroplasty.
Mulieri et al. looked at the use of reverse TSA in patients with irreparable massive rotator cuff tears without evidence of glenohumeral arthritis. All outcomes were improved postoperatively, and they advocate for reverse TSA in this subset of patients. Survivorship was over 90% at more than 4 years average follow up.
Boileau et al. evaluated the clinical outcomes of isolated biceps tenotomy/tenodesis in patients with massive rotator cuff tears and a biceps lesion. They found that the procedure can effectively treat pain and improve function in these patients. There was no difference in patients undergoing tenotomy versus tenodesis.
Figure A is a right shoulder radiograph status post RTSA with components in adequate position.
Incorrect Answers:
Question 53
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 54
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
REFERENCES: Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 233-245.
Question 55
Which gene correlates with severity of disease in spinal muscular atrophy (SMA)? Review Topic
Explanation
Question 56
The patient in Figure 99 has pain at the first MTP joint.

Explanation
General principles can be used as bunion surgery guidelines even though there is extensive debate on the topic. A distal metatarsal osteotomy is most appropriate for patients with mild deformity and no transfer metatarsalgia. A proximal osteotomy potentially can correct more severe
deformities. A lapidus procedure, or tarsometatarsal fusion, provides the highest potential to correct deformity plus the advantage of stabilizing the first tarsometatarsal joint and limiting or eliminating transfer metatarsalgia. A first MTP fusion is most appropriate for patients with severe first MTP arthrosis.
RECOMMENDED READINGS
Easley ME, Trnka HJ. Current concepts review: hallux valgus part II: operative treatment. Foot Ankle Int. 2007 Jun;28(6):748-58. Review. PubMed PMID: 17592710.View Abstract at PubMed
Coughlin MJ, Shurnas PS. Hallux rigidus. Grading and long-term results of operative treatment. J Bone Joint Surg Am. 2003 Nov;85-A(11):2072-88. PubMed PMID: 14630834. View Abstract at PubMed
Question 57
A 45-year-old coach sustains a complete distal biceps tendon rupture at the elbow. Surgical repair is most indicated to Review Topic
Explanation
Question 58
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?
Explanation
REFERENCES: Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Callaghan JJ, Salvati EA, Pellicci PM, Wilson PD Jr, Ranawat CS: Results of revision for mechanical failure after cemented total hip replacement, 1979 to 1982: A two- to five-year follow-up. J Bone Joint Surg Am 1985;67:1074-1085.
Question 59
An 76-year-old woman falls from standing and sustains the injury shown in Figure A. Her most recent T score was -1.9, 3 months prior to presentation. If labwork were performed, which values would be consistent with her bone density score?

Explanation
In the setting of osteopenia/osteoporosis, there is a positive feedback to increase PTH in response to low serum calcium levels. In response, there is a corresponding increase in alkaline phosphatase and decrease in phosphorous and circulating vitamin D levels.
Fraser writes a concise, yet thorough synopsis on primary and secondary hyperparathyroidism. In the article, the summary regarding osteopenia/osteoporosis (typically a state of hypovitamin D) begins by stating an initial state of decreased ionised calcium, which increases PTH, results in 3 primary effects: an attempt to increase gut absorption of Ca, mobilize Ca from the bone via osteoclasts and activate vitamin D at the kidney (1,25-vitamin D).
Figure A exhibits a left femoral neck fracture, which is a fragility fracture associated with poor bone density. Illustration A is a figure from Fraser's article exhibiting the feedback loop from the hypothalamus, pituitary, adrenal/glandular axis.
Incorrect answers:
Question 60
Glenohumeral inferior stability in the adducted shoulder position is primarily a function of the
Explanation
REFERENCES: Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Harryman DT II, Sidles JA, Harris SL, Matsen FA III: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Question 61
A lower chance of failure when using an extensor mechanism allograft to address a chronic disruption of an extensor tendon is associated with
Explanation
Disruption of the extensor mechanism is a rare but devastating complication of knee arthroplasty. Primary repair is associated with a high rate of failure. The results associated with using an extensor mechanism allograft are still variable overall, but the literature on the subject supports tensioning of the allograft in full extension. In studies conducted by Burnett and associates and Nazarian and Booth, the patellar remnant is excised. The use of a fresh-frozen nonirradiated allograft is recommended, and patellar resurfacing of the insensate patella is unnecessary and potentially weakens the allograft.
CLINICAL SITUATION FOR QUESTIONS 133 THROUGH 135
A middle-age man who had an anterior cruciate ligament (ACL) reconstruction with a carbon fiber ligament as a teenager also had a debridement, synovectomy, and a medial unicompartmental arthroplasty. Fourteen years later, he has a painful knee (mainly laterally and anteriorly) that swells with activity. His range of motion is 0 to 120 degrees.
Question 62
The most important radiographic predictor of a good clinical outcome following adult spinal deformity surgery is correction of Review Topic
Explanation
Question 63
A study is conducted to measure the difference in bone mineral density between postmenopausal women taking a drug treatment versus those taking a placebo. What is the most important result to be reported from this study?
Explanation
(ie, the means and standard deviations).
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 64
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 65
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
Question 66
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182.
Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293.
Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 67
A 30-year-old man requires surgical stabilization of a hypermobile spondylolisthesis of L5 on S1. History reveals that he has smoked one pack of cigarettes a day for 15 years. During preoperative counseling, the patient should be advised to
Explanation
REFERENCES: Silcox DH III, Daftari T, Boden SD, Schimandle JH, Hutton WC, Whitesides TE Jr: The effect of nicotine on spinal fusion. Spine 1995;20:1549-1553.
Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
Glassman SD, Anagnost SC, Parker A, Burke D, Johnson JR, Dimar JR: The effect of cigarette smoking and smoking cessation on spinal fusion. Spine 2000;25:2608-2615.
Question 68
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 69
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time? Review Topic
Explanation
sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter.
Question 70
below show the radiographs, and the MRIs obtained from a year-old man with worsening left knee pain. A foot hip-to-ankle radiograph shows a degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL
reconstruction alone is not indicated for this patient.
Question 71
Patellofemoral arthroplasty is contraindicated in the presence of
Explanation
Any inflammatory disease, including crystalline arthropathy, is a contraindication for patellofemoral arthroplasty. Patellar tilt and dysplasia frequently occur in the setting of patellofemoral arthritis and do not constitute a contraindication to this procedure. Severe crepitus is common and frequently addressed with patellofemoral arthroplasty.

CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 50
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken nonsteroidal anti-inflammatory medications and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals range of motion of 15 to 80 degrees with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity.
Question 72
A 77-year-old man has had increasing right knee pain for the past 3 months. A radiograph and coronal T 1 -weighted MRI scan are shown in Figures 19a and 19b. A biopsy specimen is shown in Figure 19c. What is the most likely diagnosis?
Explanation
REFERENCES: Mitchell AD, Ayoub K, Mangham DC, et al: Experience in the treatment of dedifferentiated chondrosarcoma. J Bone Joint Surg Br 2000;82:55-61.
Frassica FJ, Unni KK, Beabout JW, Sim FH: Dedifferentiated chondrosarcoma: A report of the clinicopathological features and treatment of seventy-eight cases. J Bone Joint Surg Am 1986;68:1197-1205.
Question 73
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 74
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
Mankin HJ, Mow VC, Buckwalter JA: Articular cartilage structure, composition, and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 75
- A 20-year-old college football player sustains a forceful hyperextension injury to his shoulder 4 months after undergoing an anterior capsular shift. Examination 2 weeks later reveals anterior tenderness. He is unable to lift the dorsum of his hand away from his back. What is the most likely diagnosis?
Explanation
Question 76
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 77
A 50-year-old patient underwent multiple débridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
The patient developed a large bone defect after undergoing multiple débridements for an open fracture. The most appropriate graft in this setting is a vascularized bone graft. Considering the length of the defect, a free vascularized fibular graft would be a suitable graft. The indications for a vascularized bone graft include infection, inadequate vascularity of the surrounding tissues, bone defects larger than 6 centimeters, and previous failed bone grafts. The osteocytes survive in the vascularized graft, allowing primary bone healing and thereby limiting a loss of graft strength. In contrast, nonvascularized bone graft heals by creeping substitution with a loss of its initial strength. Calcium sulfate pellets and calcium phosphate cement are synthetic bone substitutes with osteoconductive properties. Their role in fracture healing is limited. Demineralized bone matrix is the matrix remaining after allograft undergoes decalcification processing. These products alone would not be optimal in the treatment of such a large bone defect.
Question 78
A 45-year-old male auto mechanic presents to your office with left lateral elbow pain for 6 weeks. On physical exam he has tenderness to palpation over the lateral epicondyle and pain with resisted wrist extension. An MRI is shown in figures A and B. After failing non-surgical treatment modalities, he undergoes arthroscopic surgical management. At 3 months post-operatively, the patient reports persistent left elbow pain and an audible clicking since surgery which occurs when he lifts heavy objects and when he pushes himself up out of a chair. What is the best surgical treatment option? Review Topic
Explanation
PLRI is the result of an incompetent lateral ulnar collateral ligament (LUCL), a component of the elbow lateral collateral ligament complex. The LUCL originates on the lateral epicondyle of the humerus and inserts upon the supinator crest of the ulna. When deficient from acute trauma or from repetitive microtrauma, the elbow becomes rotationally unstable with elbow extension, supination, and an applied valgus force. In this case, the patient has had iatrogenic damage to the LUCL from an arthroscopic release of the extensor carpi radialis brevis (ECRB) for treatment of lateral epicondylitis. This patient exhibits an important manifestation of this: a positive chair pushup test. This test is positive when pushing off of a chair with a supinated forearm causes pain and instability. Due to the chronicity of the injury (3 months) and his persistent symptoms of instability (pain and clicking) the patient would benefit from surgical reconstruction of the damaged LUCL using either palmaris longus or gracilis allograft.
Kelly et. al. reviewed the known major and minor complications of elbow arthroscopy among 473 consecutive cases at their institution from 1980-1998. The most common complications were transient nerve palsies in 10 patients. Among them, the major
nerves involved included the anterior interosseous nerve, posterior interosseous nerve, ulnar nerve, superficial radial nerve, and medial antebrachial cutaneous nerve. The risk of iatrogenic nerve injury was increased among patients with rheumatoid arthritis. The most frequent complication was prolonged drainage from the portal sites.
Calfee et. al. reviewed the management of lateral epicondylitis. The authors suggest open or arthroscopic surgical debridement of the common extensor origin after failure of rest, orthoses, nonsteroidal drugs, physical therapy, cortisone and platelet-rich plasma injections. They do acknowledge that excessive debridement may compromise lateral elbow stability and cause PLRI.
O'Brien et. al. described the surgical techniques for managing PLRI, including an open technique for chronic injuries or revision treatment. In this setting, the authors suggest use of palmaris or gracilis allograft for reconstruction.
Figures A and B are an axial and coronal T2 weighted MRI of an elbow demonstrating signal intensity in the origin of the ECRB, consistent with lateral epicondylitis.
Incorrect Answers:
Question 79
A 56-year-old woman presents with left hip pain and diminishing range of motion. Examination reveals pain with range of motion of the hip. Radiographs reveal multiple calcific lesions within the hip and well-preserved joint space. MRI scan shows thickened synovium nodular loose bodies with decreased signal on T1 and T2. What is the best next step?
Explanation
Question 80
A 7-year-old boy with spastic diplegia is a limited community ambulator. He has a moderately severe crouched gait. The parents request a treatment that will result in a permanent decrease in lower extremity muscle tone. This is best accomplished with
Explanation
REFERENCES: Arens LJ, Peacock WJ, Peter J: Selective posterior rhizotomy: A long-term follow-up study. Childs Nerv Syst 1989;5:148-152.
Koman LA, Paterson Smith B, Balkrishnan R: Spasticity associated with cerebral palsy in children: Guidelines for the use of botulinum-A toxin. Paediatr Drugs 2003;5:11-23.
Johnson MB, Goldstein L, Thomas SS, et al: Spinal deformity after selective dorsal rhizotomy in ambulator patients with cerebral palsy. J Pediatr Orthop 2004;24:529-536.
Question 81
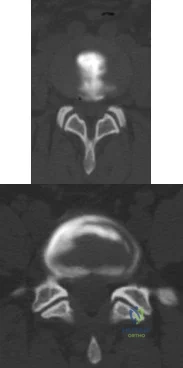
Figure 83 is the CT scan of a 36-year-old man who fell from a roof. Eight hours later at the emergency department he describes low-back pain with numbness and weakness in his bilateral lower extremity. A neurologic examination reveals 2/5 strength in his quadriceps and iliopsoas bilaterally, 2/5 strength in his right anterior tibialis and gastrocsoleus, and 1/5 strength in his left anterior tibialis and gastrocsoleus. Two hours later, strength in his lower extremities has diminished markedly. What is the best next step?

Explanation
Any progressive neurologic deficit requires emergent surgical intervention. Lumbar injuries cannot be reliably reduced with traction. Although IV steroids and management of mean arterial blood pressure are appropriate interventions for injuries in the region of the conus medullaris, steroids are only indicated when given within 8 hours of injury and are not appropriate as a sole means of management for progressive neurologic deficit.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Question 82
When planning pin placement for external fixation of the tibia, what is the maximum extent of the knee capsular reflection from the subchondral joint line?
Explanation
Question 83
Treatment of an atrophic nonunion of the radial diaphysis should include which of the following?

Explanation
Question 84
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of
Explanation
REFERENCES: Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 161-166.
Question 85
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?
Explanation
REFERENCES: Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248.
Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289.
Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis
with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200.
Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372.
Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170.
Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
Billings A, Scott DF, Camargo MP, et al: High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion: Long-term follow-up. J Bone Joint Surg Am 2000;82:70-79.
Question 86
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCES: Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower’s exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136.
Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 87
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of
Explanation
REFERENCES: Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Whalen JL, Bishop AT, Linscheid RL: Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17:507-511.
Question 88
Figures 39a and 39b are the radiographs of a 45-year-old man with diabetes who fell 12 feet from a ladder and sustained an isolated closed injury to his left leg. Examination revealed that he was neurovascularly intact and compartments were soft. A damage control knee spanning external fixator was applied and after 2 weeks in the frame, his blisters have resolved and his skin now wrinkles. What is the most appropriate treatment?

Explanation
alignment while the soft-tissue injury recovers and to allow for surveillance and examination of the limb. The radiographs reveal a comminuted bicondylar pattern with significant depression of the lateral articular surface and a split fracture with condylar widening. This element of the fracture will require direct elevation of the joint surface and reduction/buttress of the lateral condyle. This is best achieved with a lateral plate with subchondral rafting screws. The medial articular surface is coronally split and the posteromedial fragment is displaced. This fragment requires direct reduction and buttress via a separate posteromedial approach which is frequently performed prior to the lateral approach and fixation. A lateral buttress plate or a lateral locking plate alone does not reliably capture or adequately support the displaced posteromedial fragment. A medial and lateral plate construct is less soft-tissue friendly, particularly if inserted through a single incision. A medial plate would also fail to give direct buttress to the posteromedial fragment.
Question 89
A 13-year-old boy who has a history of a pituitary adenoma has an unstable unilateral slipped capital femoral epiphysis. What is the indication for prophylactic pinning of the contralateral, unslipped side? Review Topic
Explanation
Question 90
What is the principal advantage of surgical repair for the lesion shown in Figure 19?
Explanation
REFERENCES: Bhandari M, Guyatt GH, Siddiqui F, et al: Treatment of acute Achilles tendon ruptures: A systematic overview and meta-analysis. Clin Orthop 2002;400:190-200.
Schepsis AA, Jones HE, Haas AL: Achilles tendon disorders in athletes. Am J Sports Med 2002;30:287-305.
Question 91
A 41-year-old male underwent intramedullary nailing for a low-energy left femoral shaft fracture. At his follow-up appointment, he complains that his feet are pointing in opposite directions when walking. Using the imaging study shown in Figure A, which of the following represents this patient's left femur malalignment?
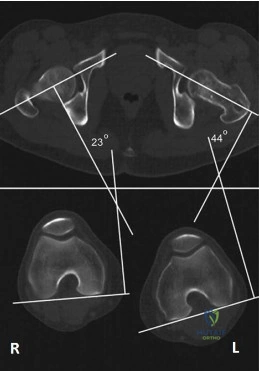
Explanation
Radiographic rotational malalignment after fixation of femoral shaft fractures may be measured by comparing the femoral anteversion of both femurs. This can be determined by measuring the angle between a line tangential to the dorsal bony contours of the femoral condyles and a line drawn through the axis of the femoral neck. Rotational differences of less than 10° are considered variations of normal.
Jaarsma et al. reviewed rotational malalignment after intramedullary nailing of femoral fractures. They report that rotational measurements by CT are superior to clinical assessment. They note a high incidence of malrotation after IM nailing of fractures. This has shown to be in the range 15% to 30%.
Figure A shows left femoral malrotation using CT-torsion measurements with axial cuts of the femoral neck and distal femoral condyles. Note the normal anteversion of the right femur (23 degrees; normal range 10-25).
Incorrect Answers:
Question 92
1 to 1 micron
Explanation
For many years, it was believed that large particles incited the histiocytic response. It is now well established that submicron-size particles stimulate this response.
Question 93
Figures 23a through 23h are the radiographs and MR images of a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability symptoms. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to decrease stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but, if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should only be performed at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
Question 94
What is the most common mode of failure following unconstrained total elbow arthroplasty? Review Topic
Explanation
Question 95
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 96
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
REFERENCES: Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Kraemer WJ, Schemitsch EH, Lever J, McBroom RJ, McKee MD, Waddel JP: Functional outcome of thoracolumbar burst fractures without neurological deficit. J Orthop Trauma 1996;10:541-544.
Question 97
- Examination of a 32-year old woman who has pain in her shoulder as a result of a head-on motor vehicle accident reveals tenderness directly over the scapula and painful motion of the shoulder. Radiographs show a displaced extra-articular fracture of the scapula. Which of the following studies would best detect commonly associated injuries?
Explanation
Question 98
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
Question 99
What is the most common complication of halo vest immobilization in adults?
Explanation
REFERENCES: Baum JA, Hanley EN Jr, Pullekines J: Comparison of halo complications in adults and children. Spine 1989;14:251-252.
Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Nemeth JA, Mattingly LG: Six-pin halo fixation and the resulting prevalence of pin-site complications. J Bone Joint Surg Am 2001;83:377-382.
Question 100
Commotio cordis is best treated with
Explanation
REFERENCES: McCrory P: Commotio cordis. Br J Sports Med 2002;36:236-237.
Boden BP, Tacchetti R, Mueller FO: Catastrophic injuries in high school and college baseball players. Am J Sports Med 2004;32:1189-1196.
