Orthopedic Board Review MCQs: Arthroplasty, Spine & Trauma | Part 204

Key Takeaway
This page offers Part 204 of a comprehensive OITE & AAOS Orthopedic Surgery board review series. Featuring 100 high-yield, verified MCQs in exact exam format, it's designed for orthopedic residents and surgeons. Utilize study or exam mode to master key topics like Arthroplasty, Hip, and Knee, ensuring rigorous board certification preparation.
About This Board Review Set
This is Part 204 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 204
This module focuses heavily on: Arthroplasty, Dislocation, Foot, Hip, Knee, Nerve, Tendon.
Sample Questions from This Set
Sample Question 1: Figure 10 is the radiograph of a 44-year-old man with a long-standing history of severe hip pain and a limp. Which clinical scenario most likely could occur when performing total hip arthroplasty on this patient?...
Sample Question 2: Which of the following symptoms are most commonly associated with piriformis syndrome?...
Sample Question 3: A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sen...
Sample Question 4: A 40 year-old-man was involved in a motor vehicle accident and sustained the pelvic injury seen in Figures 24a and 24b. Definitive management of the injury should consist of reduction by...
Sample Question 5: Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflamm...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 10 is the radiograph of a 44-year-old man with a long-standing history of severe hip pain and a limp. Which clinical scenario most likely could occur when performing total hip arthroplasty on this patient?
Explanation
The radiograph reveals hip dysplasia. Patients with hip dysplasia and severe limb shortening are at high risk for sciatic nerve palsy from overlengthening. Overmedializing the acetabular component is not the preferred response because overlateralization is more of a concern if the cup is placed in the pseudoacetabulum instead of in the true acetabulum. Placing the hip center too inferior is not the preferred response because the concern in this scenario is placing the hip center too superior if the cup is placed in the pseudoacetabulum or if a large-diameter cup is used. Acetabular fractures are possible because of osteoporotic bone at the true hip center, but is less likely than overlengthening of the extremity.

CLINICAL SITUATION FOR QUESTIONS 11 THROUGH 13
Figures 11a and 11b are the radiographs of a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, she has failed nonsurgical treatment including weight loss, activity modifications, and intra-articular injections. Her infection workup reveals laboratory findings within defined limits.
Question 2
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
REFERENCES: Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002,
pp 114-139.
Levin SM: Piriformis syndrome. Orthopedics 2000;23:183-184.
Question 3
A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sensory, or deep tendon reflexes. Because nonsurgical management has failed to provide relief, he has chosen surgery to allow him to complete his season. The MRI scan and myelogram shown in Figures 19a and 19b show minimal disk bulge, but a root cutoff is noted at the left C7 foramen. Electromyography demonstrates C7 nerve root irritation. Which of the following procedures will best optimize his chances for completing the season?
Explanation
REFERENCES: Henderson, CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R: Cervical radiculopathy: A review. Spine 1986;11:988-991.
Chen BH, Natarajan RN, An H, Andersson GB: Comparison of biomechanical response to surgical procedures used for cervical radiculopathy: Posterior keyhole foraminotomy versus anterior foraminotomy and discectomy versus anterior discectomy with fusion. J Spinal Disord 2001;14:17-20.
Question 4
A 40 year-old-man was involved in a motor vehicle accident and sustained the pelvic injury seen in Figures 24a and 24b. Definitive management of the injury should consist of reduction by
Explanation
REFERENCES: Tile M: Management of pelvic ring injuries, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 168-202.
Kabak S, Halici M, Tuncel M, et al: Functional outcome of open reduction and internal fixation for completely unstable pelvic ring fractures (type C): A report of 40 cases. J Orthop Trauma 2003;17:555-562.
Question 5
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20°. Management should now consist of
Explanation
REFERENCES: Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Fulkerson JP: Patellofemoral pain disorders: Evaluation and management. J Am Acad Orthop Surg 1994;2:124-132.
Question 6
The failure of the acetabular component shown in Figure 15 is most likely the result of the use of a 32-mm head and
Explanation
REFERENCE: Astion DJ, Saluan P, Stulberg BN, Rimnae CM, Li S: The porous-coated anatomic total hip prosthesis: Failure of the metal-backed acetabular component. J Bone Joint Surg Am 1996;78:755-766.
Question 7
Figure 42 shows the radiograph of a 12-year-old boy who has a limp and pain in the left hip with athletic activity. Examination reveals decreased abduction and internal rotation of the left hip, with pain at the extremes of motion and a 1-cm limb-length discrepancy. Management should consist of
Explanation
REFERENCES: Skaggs DL, Tolo VT: Legg-Calve-Perthes disease. J Am Acad Orthop Surg 1996;4:9-16.
Quain S, Catterall A: Hinge abduction of the hip: Diagnosis and treatment. J Bone Joint Surg Br 1986;68:61-64.
Question 8
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent?
Explanation
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
Question 9
Figure 43 shows an arthroscopic view of the posteromedial compartment of a patient’s left knee using a 70-degree arthroscope placed through the intercondylar notch. The arrow is pointing to what structure?
Explanation
REFERENCES: Miller MD: Basic arthroscopic principles, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, pp 224-237.
Gold DI, Schaner PJ, Sapega AA: The posteromedial portal in knee arthroscopy: An analysis of diagnostic and surgical utility. Arthoscopy 1995;11:139-145.
Question 10
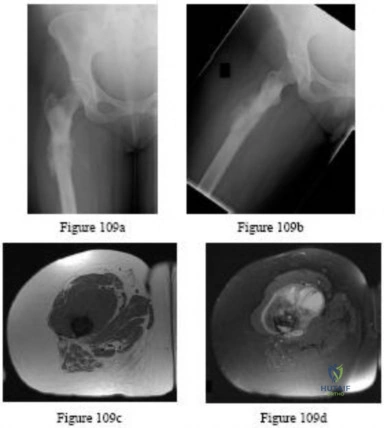
Figures 86a through 86c are the radiographs and biopsy specimen of a 14-year-old boy who has had left knee pain for 4 weeks. What is the most likely diagnosis?
Explanation
Question 11
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 12
Figures 1a and 1b show the sagittal T 2 - and T 1 -weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm 3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of
Explanation
REFERENCES: Tay BK, Deckey J, Hu SS: Spinal Infections. J Am Acad Orthop Surg 2002;10:188-197.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 431-439.
Question 13
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?
Explanation
the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy
active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time
of less than 6 hours.
REFERENCES: Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Boulas HJ: Amputations of the fingers and hand: Indications for replantation. J Am Acad Orthop Surg 1998;6:100-105.
Question 14
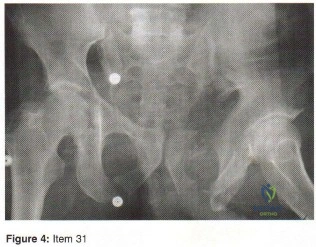
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
Explanation
REFERENCES: Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg
2000;93:53-57.
Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Question 15
03 An 18 month old child has bilateral “corner fractures” of the distal femoral metaphyses of unknown origin. Following a skeletal survey, the first step in management should consist of
Explanation
back to this question next question
Question 16
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 295-297.
Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 379.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 23.
Ebraheim NA, Elgafy H, Xu R: Bone-graft harvesting from iliac and fibular donor sites: Techniques and complications. J Am Acad Orthop Surg 2001;9:210-218.
Question 17
Examination of a 23-year-old female college basketball player who has had anterior knee pain for the past 3 weeks reveals tenderness and fullness over the inferior patella and proximal patellar tendon. There is no patellofemoral crepitus, patella apprehension sign, or anterior or posterior instability. Initial management should include
Explanation
REFERENCES: Stanish WD, Rubinovich RM, Curwin S: Eccentric exercise in chronic tendinitis. Clin Orthop 1986;208:65-68.
Witvrouw E, Bellemans J, Lysens R, Danneels L, Cambier D: Intrinsic risk factors for the development of patellar tendinitis in an athletic population: A two-year prospective study. Am J Sports Med 2001;29:190-195.
Question 18
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 19
During total hip arthroplasty, which characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma-irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of this material is inferior to traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.

RESPONSES FOR QUESTIONS 76 THROUGH 80
Cemented full revision
Cemented femoral revision
Cemented acetabular revision
Cementless full revision
Cementless femoral revision without an extended trochanteric osteotomy
Cementless femoral revision with an extended trochanteric osteotomy
Cementless acetabular revision
Isolated liner/head exchange
Isolated liner/head exchange with cementing of the liner Select the most appropriate treatment for each clinical scenario.
Question 20
A 65-year-old man has a painful right hip mass that has been growing for several years. A radiograph, CT scan, and photomicrograph are shown in Figures 56a through 56c. What is the most appropriate treatment?
Explanation
REFERENCES: Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome.
J Bone Joint Surg Am 1999;81:326-338.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 21
A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
Explanation
REFERENCES: Harwood PJ, Giannoudis PV, Probst C, et al: The risk of local infective complications after damage control procedures for femoral shaft fracture. J Orthop Trauma 2006;20:181-189.
Roberts CS, Pape HC, Jones AL, et al: Damage control orthopaedics: Evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect
2005;54:447-462.
Question 22
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
REFERENCES: Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Question 23
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. Based on the radiographs shown in Figures 1 and 2, her tibia is a

Explanation
Question 24
- An infected total knee replacement with symptoms occurring within 4 weeks of surgery and no radiographic signs of osteomyelitis would be best managed with
Explanation
Arthroscopic debridement not recommended secondary to missing cutaneous tracks and soft tissue/muscle involvement.
Question 25
What type of metastatic tumor most often has a lytic radiographic appearance?
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Mulvey RB: Peripheral bone metastasis. Am J Roentgenol 1964;91:155.
Question 26
What complication is most likely to develop after right total hip arthroplasty in the patient shown in Figure 5?
Explanation
REFERENCES: Goel A, Sharp DJ: Heterotopic bone formation after hip replacement: The influence of the type of osteoarthritis. J Bone Joint Surg Br 1991;73:255-257.
Nollen JG, van Douveren FQ: Ectopic ossification in hip arthroplasty: A retrospective study of predisposing factors in 637 cases. Acta Orthop Scand 1993;64:185-187.
Question 27
Which presurgical condition is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MR imaging reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common pain location among patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain with sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear.
The lateral center edge angle is pictured in Figure 70a. This angle is considered abnormal when it is less than 25 degrees, which may indicate inadequate head coverage. The Tonnis angle and acetabular inclination are different terms for the same angle as seen in Figure 70b. The normal value is between 0 and 10 degrees. The head center position is the distance from the medial aspect of the femoral head to the ilioischial line, as measured in Figure 70c. The head is considered lateralized if the measurement exceeds 10 mm. Figure 70d marks the outline of the anterior and posterior wall, confirming the absence of a cross-over sign. A cross-over sign is present when the 2 lines cross below the lateral aspect of the acetabulum, and it indicates acetabular retroversion.
An arthroscopy to treat the labral tear is probably the best option for this patient. A PAO with prior hip arthroscopy might be considered based on the mildly increased anterior center edge angle; the Tonnis angle finding is normal, the femoral head is not lateralized, and the patient is approaching age 40. A PAO without addressing the anterior labral tear could lead to failure and is not the best choice. The patient does not have an acetabular pincer lesion and would not benefit from an acetabular edge resection.
Although age beyond 40 years and body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures (PAO, hip arthroscopy, and femoral acetabular impingement surgery), the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tonnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the Outerbridge cartilage score is
determined by direct visualization at the time of surgery. An Outerbridge score cannot be determined presurgically.
Question 28
A 70-year-old man underwent primary total knee arthroplasty 3 months ago. Figures 7a and 7b show the radiograph and clinical photograph following incision and drainage of the wound 1 week ago. Aspiration of the joint reveals methicillin-sensitive Staphylococcus aureus. What is the next most appropriate step in management?
Explanation
REFERENCES: Harwin SF: The diagnosis and management of infected total knee replacement. Seminars Arthroplasty 2002;13:9-22.
Goldmann RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Morrey BF, Westholm F, Schoifet S, Rand JA, Bryan RS: Long-term results of various treatment options for an infected total knee arthroplasty. Clin Orthop 1989;248:120-128.
Question 29
Figures 35a and 35b show the radiographs of a 7-year-old patient who has progressive deformity of the right thigh accompanied by a dull persistent pain radiating to the knee. Examination reveals an obvious bulge in the right thigh, with flexion of the hip beyond 50° only if the hip is allowed to externally rotate. Management should consist of
Explanation
REFERENCES: Zionts LE, Ebramzadeh E, Stott NS: Complications in the use of the Bailey-Dubow extensible nail. Clin Orthop 1998;348:186-195.
Luhmann SJ, Sheridan JJ, Capelli AM, Schoenecker PL: Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88-94.
Glorieux FH, Bishop NJ, Plotkin H, Chabot G, Lanoue G, Travers R: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1988;339:947-952.
Question 30
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include Review Topic
Explanation
Question 31
Histologically, synovial chondromatosis is characterized by
Explanation
REFERENCES: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;l59:792-801.
Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1962;44:77.
Question 32
Studies have shown that the parents and grandparents of people with developmental dysplasia of the hip (DDH)
Explanation
The hip arthritis RR is significantly increased in patients with DDH (RR = 82.4; P < 2e-16), their parents (RR = 2.22; P = 0.0003), and their grandparents (RR = 1.33; P = 0.011). The THA RR also is significantly increased for patients with DDH (RR = 1168; P < 3e-08) and their grandparents (RR = 2.06; P = 0.01). First-degree and second-degree relatives were not at higher risk for knee arthritis or knee arthroplasty. The RR for DDH was significantly increased for first-degree relatives (RR = 12.1; P < 0.000001) and siblings (RR = 11.9; P < 0.000001).
Question 33
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of
Explanation
REFERENCES: Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Question 34
The brachialis muscle is innervated by what two nerves?
Explanation
REFERENCES: Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
King A, Johnston GH: A modification of Henry’s anterior approach to the humerus. J Shoulder Elbow Surg 1998;7:210-212.
Question 35
03 Which of the following findings is one of the diagnostic criteria for diffuse idiopathic skeletal hyperostosis?
Explanation
Diffuse idiopathic skeletal hyperostosis is a common disease, most prevalent in those over 50 years of age. The usual presentation is a middle-aged or older patient with chronic mild pain in the middle to lower back, spinal stiffness, and typical radiographic changes in the thoracic spine. Diffuse idiopathic skeletal hyperostosis is predominantly a radiographic diagnosis with 3 major diagnostic criteria. 1. Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae. 2. Preservation of disk height in the involved vertebral segment; the relative absence of significant degenterative changes, such as marginal sclerosis in vertebral bodies or vacuum phenomenon. 3.
Absence of facet-joint ankylosis; absence of sacroiliac erosion, sclerosis, or intra-articular osseous fusion. Treatment is typically non-operative, with anti-inflammatories, activity modification and PT.
back to this question next question
Question 36
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?
Explanation
REFERENCES: Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 37
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
REFERENCES: Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 38
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 degrees to 120 degrees. Radiographs are shown in Figure 67. Management should include
Explanation
REFERENCES: Wattenbarger JM, Gerardi J, Johnson CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;223:94-398.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 39
Which of the following conditions is associated with palmoplantar pustulosis?
Explanation
REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Sonozaki H, Azuma A, Okai K, et al: Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg 1979;95:13-22.
Question 40
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
Explanation
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail,
residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
Question 41
What is the most common malignancy involving the hand?
Explanation
REFERENCES: Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Fleegler EJ: Skin tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 2184-2205.
Question 42
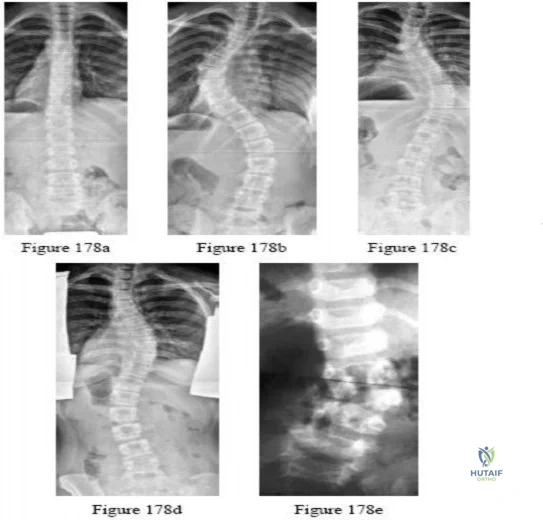
-Figures a and b are the posteroanterior and lateral radiographs of a 13-year-old girl with a progressive curve despite bracing with a thoracolumbosacral orthosis. Examination reveals no pain or neurologic findings. The lumbar curve measures 59 degrees and the thoracic curve measures 52 degrees.The most appropriate treatment is

Explanation
Question 43
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain? Review Topic
Explanation
Question 44
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
Explanation
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to 1a,25(OH)2D3].
Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
Question 45
Figure 6 shows the clinical photographs of a newborn who underwent a colostomy for an imperforate anus. Examination shows extended knees, flexed hips, and equinovarus feet. Dimpling is noted over the buttocks. Patients with these findings differ from patients with myelodysplasia in that they
Explanation
REFERENCE: Renshaw TS: Sacral agenesis. J Bone Joint Surg Am 1978;60:373-383.
Question 46
Which of the following terms describe a rehabilitative exercise in which the foot is mobile and the motion of the knee is independent of hip and ankle motion?
Explanation
Question 47
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
REFERENCES: Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 48
Which of the following hip fracture patterns is at increased risk of proximal fragment flexion malreduction with dynamic hip screw fixation?

Explanation
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Question 49
A 5-year-old boy has had midfoot pain with activity for the past 3 months. He has no pain at rest. Radiographs are shown in Figures 29a and 29b. Management should consist of
Explanation
REFERENCE: Williams GA, Cowell HR: Koehler’s disease of the tarsal navicular. Clin Orthop 1981;158:53-58.
Question 50
An 83-year-old man is seen in the emergency department for evaluation of neck pain after a motor vehicle accident. The patient has no neurologic deficits. The patient has a history significant for late stage ankylosing spondylitis with cervicothoracic kyphosis. What is the most appropriate method of immobilization for the cervical spine while diagnostic testing is performed? Review Topic
Explanation
(SBQ12SP.43) The right vertebral artery sustains a complex injury during a occipitocervical (C3-O) fusion. Bleeding cannot be controlled with local tamponade and a hemostatic agent. After clamping the vessel a segmental defect is noted in the vessel. The patient undergoes urgent angiography, which reveals adequate collateral circulation. What is the next step in the management of this injury? Review Topic
Addition of a systemic antifibrolytic solution
Direct repair
Contralateral vetebral artery anastomosis
Acute synthetic grafting
Embolization treatment
When (1) vetebral artery [VA] bleeding cannot be controlled with local tamponade and a local hemostatic agent, and (2) collateral circulation is maintained in the non-dominant artery (left vertebral artery is usually dominant), the next best step would be to achieve local control with an intraoperative endovascular procedure such as embolization, stenting or clipping.
The management of VA injury is difficult. If local tamponade can be achieved, the next best step would be to consider direct repair of the artery. If tamponade fails to achieve proper hemostasis, additional procedures may be considered, such as intraoperative endovascular embolization, or clipping and ligation. When considering these intraoperative endovascular treatments, the collateral circulation should be assessed. If collateral circulation is inadequate, direct repair or stenting should be reconsidered.
Peng et al. reviewed the anatomical considerations, management, and preventive measures of vertebral artery injury in cervical spine surgery. They showed that
ligation-associated morbidities such as cerebellar infarction, cranial nerve palsies, or hemiplegia can occur in up to 12% of cases. They suggest direct repair should be considered as first-line treatment when local hemostasis can be controlled.
Lall et al. reviewed the perioperative complications associated with occipitocervical fusion. The most commonly encountered complications were related to instrumentation failure after nonunion (6-7%). Other complications included vertebral artery injury (1.3%-4.1% during placement of C1-C2 transarticular screws, most commonly in the case of high-riding vertebral artery), dural tears, and wound infections.
Illustration A shows the treatment algorithm of VA injuries as suggested by Peng et al.
Incorrect Answers:
Question 51
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 52
The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injury. This band is a portion of the
Explanation
REFERENCES: Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofibular ligament: A cause of chronic pain in the ankle after inversion sprain.
J Bone Joint Surg Am 1990;72:55-59.
DiGiovanni BF, Fraga CJ, Cohen BE, et al: Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 2000;21:809-815.
Question 53
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
Explanation
REFERENCES: Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Yang KH, Han DY, Park HW, et al: Fracture of the ipsilateral neck of the femur in shaft nailing: The role of CT in diagnosis. J Bone Joint Surg Br 1998;80:673-678.
Question 54
An elderly woman with osteoporosis falls from a standing height, sustaining a low-energy fracture of the acetabulum. What structures are most likely fractured?
Explanation
may present as atypical fracture patterns not always conforming to classic injury patterns described by Judet and associates. This fracture pattern seen commonly in geriatric patients results from low-energy falls with force directly applied to the greater trochanter. Fractures involving the posterior column and/or wall and transverse fracture patterns involving both the anterior and posterior columns occur infrequently in this age group. They are, however, more commonly encountered in younger age groups as a result of higher energy trauma.
Question 55
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
Explanation
REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.
Question 56
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Jehovah’s Witnessess Official Web Site: Medical Care and Blood, 2008, http://www.watchtower.org/e/medical_care_and_blood.htm
Question 57
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
REFERENCES: Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Shin AY, Moran ME, Wenger DR: Superior gluteal artery injury secondary to posterior iliac crest bone graft harvesting: A surgical technique to control hemorrhage. Spine 1996;21:1371-1374.
Question 58
Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).
Explanation
Figures 14a through 14e show a 13-year-old boy with osteomyelitis of the distal tibia and a large subperiosteal abscess. The patient has failed treatment with IV ceftriaxone, and methicillin-resistant Staphylococcus aureus infection is likely. Aspiration, cultures, irrigation and debridement, IV vancomycin, an infectious disease consult, and an evaluation for possible deep vein thrombosis is prudent initial treatment. Figure 15a through 15c show a 7-year-old girl who sustained a deer tick bite while vacationing in Connecticut. She has Lyme arthritis and a Lyme “bulls-eye” rash on the same leg. Aspiration, cultures, Lyme serology, and oral amoxicillin for 30 days is prudent initial treatment. Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with a probable minor fracture via a benign cyst of the distal femur. The geographic cyst may be a nonossifying fibroma, eosinophilic granuloma, Brodie abscess, or simple bone cyst. Biopsy, culture, curettage and bone graft, and possible internal fixation is reasonable initial treatment.

Question 59
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of
Explanation
REFERENCES: Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123.
Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Kuo RS, Tejwani NC, Digiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 60
A 70-year-old healthy man had total knee arthroplasty 18 years ago, and it now is painful. Radiographs reveal aseptic loosening and the range of motion before surgery is 15 to 85 degrees. The strongest indication for performing a tibial tubercle osteotomy to aid in exposure in his knee would be
Explanation

Question 61
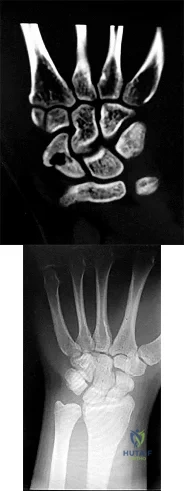
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?
Explanation
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
Question 62
intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
Explanation
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is
positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
Ig antibodies at the neuromuscular (NM) junction
Decreased release of acetylcholine at the NM junction
Decrease in myelin sheath of axonal nerves with loss of NM junction
Absence of dystrophin with excess calcium at sarcolemma
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
Analysis of variance (ANOVA)
Regression analysis
Student t test
Mann-Whitney U test
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
Which of the following is the mechanism of action of aspirin?
Inhibition of vitamin K-dependent carboxylation
Inhibition of factor Xa through antithrombin binding
Binding of cyclooxygenase (COX)-1 and COX-2
Direct thrombin inhibition
Glycoprotein IIIb agonist binding
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Intermediate doses (650 mg to 4 g/day) inhibit COX-1 and COX-2, blocking prostaglandin (PG) production, and have analgesic and antipyretic effects. Illustration A shows the mechanism of action of aspirin.
InCORRECT Answers: 1,2,4,5: Aspirin does not have any of these mechanisms of action.
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Crossover design trial
Parallel design trial
Cohort study
Case series
In a parallel design trial, participants are randomized to 2 or more groups, each of which receives a different treatment or intervention. For example, Group A receives the drug and Group B receives the placebo. This type of
design allows for comparison between groups. In a crossover design clinical trial, both groups receive both interventions over a defined time period. For example, Groups A and B both receive the drug as well as the placebo. This allows for within-participant comparisons. In a cohort study, patient groups are followed over time on the basis of having or not having received an exposure. Cohort studies are not randomized. In a case series, patients often receive a particular treatment and the outcomes are then examined.
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Increase calcium and vitamin D intake
Avoid all nonsteroidal anti-inflammatory drugs (NSAIDs)
Maintain smoking cessation
Engage in early physical therapy to strengthen the trunk musculature
Smoking is the biggest risk factor for nonunion and should be strictly avoided. NSAIDs interfere with bone healing, but not as strongly as smoking. Early mobilization would potentially stress the construct, inducing movement that leads to nonunion. Without history of calcium and vitamin D deficiency, increasing intake would not decrease the risk of nonunion.
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
occurs earlier.
occurs later.
is prolonged.
is shortened.
Compared to similar autograft, allograft tissue demonstrates a prolonged inflammatory response, slower rate of biological incorporation and remodeling, and a higher proportion of large-diameter collagen fibrils. Native ACL inserts
into bone through a transition of 4 distinct zones: tendon, unmineralized fibrocartilage, mineralized fibrocartilage, and bone. This transition is not reproduced with tendon grafts, which instead heal with interposed fibrovascular scar at the graft-tunnel interface. The scar rapidly remodels to form perpendicular fibers resembling Sharpey fibers and, eventually, mature bone growth into the outer portion of the graft. The intra- articular portion of allograft undergoes an initial phase of necrosis followed by repopulation by host synovial cells into the acellular collagen scaffold.
Revascularization and maturation complete the ligamentization of graft tissue.
A researcher decides she wants to look at the current total number of patients who have methicillin-resistant Staphylococcus aureus (MRSA) infections in a hospital on 1 particular day. What is the researcher measuring?
Correlation coefficient of MRSA
Prevalence of MRSA
Incidence of MRSA
Relative risk of MRSA
The prevalence of a disease is a measure of the number of cases of a disease at or during a specific time point or time period. In this case, the researcher wants to know the prevalence of disease on a given day. Incidence measures new cases of a disease or event per unit of time. Correlation coefficient is a measure of how 2 things correlate with one another, while relative risk is a statistical outcome that is often used in case-control or cohort studies to provide a measure of the risk of a particular disease occurring when a certain exposure has already occurred.
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
protein C and S.
vitamin K.
von Willebrand factor.
factor VIII.
Hemophilia A is an X-linked recessive deficiency of factor VIII that can lead to significant bleeding problems including recurrent spontaneous hemarthroses that can lead to synovitis and joint destruction. von Willebrand disease is a lack of von Willebrand factor that leads to decreased platelet aggregation; more commonly patients have mucosal bleeding and not hemarthroses. Vitamin K deficiency is not hereditary; it is typically attributable to inadequate dietary intake, malabsorption, and loss of storage sites from hepatocellular disease. Protein C and S deficiencies are autosomal-dominant diseases that lead to thrombosis, not bleeding, as protein C and S shut off thrombin formation.
What is the recommended optimal timing of presurgical antibiotic administration to prevent infection in patients undergoing total joint replacement surgery?
Within 1 hour before incision
Within 2 hours before incision
Immediately after incision
Within 1 hour after incision
The current recommendation for antibiotic prophylaxis for major orthopaedic surgical procedures is to administer intravenous antibiotics within 1 hour of surgical incision. Redosing of antibiotics should occur 3 to 4 hours after the initial dose for procedures that extend beyond 3 to 4 hours. Little evidence supports postsurgical antibiotic use beyond 24 hours. As you move beyond 1 hour from time of administration of antibiotics, risk for infection increases and rates of bacterial cell death decline. It is not acceptable to
administer presurgical antibiotics after incision.
Bacterial resistance to antibiotics in biofilm is an example of
avoidance.
decreased susceptibility.
inactivation.
mutation. CORRECT answer: 1
Three basic mechanisms of antibiotic resistance have been identified: avoidance, decreased susceptibility, and inactivation. Biofilm formation is a classic example of avoidance, whereby the biofilm creates a physical barrier to the antibiotic. Bacteria can decrease their susceptibility to antibiotics by mutating the antibiotic target or generating a mechanism to inactivate the antibiotic. Biofilm formation develops when a sufficient mass of bacteria forms on a surface. The cell-to-cell signaling becomes sufficient to activate transcription of genes needed for biofilm formation in a process known as quorum sensing. Once the bacteria produce a mature biofilm, they enter a greatly reduced or stationary phase of growth. Lastly, high-shear
environments seem to stimulate biofilm production.
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Promotes reabsorption of phosphate in the renal tubules
Interferes with osteoclast maturation
Interferes with intestinal absorption of calcium
Upregulates osteoblast formation
Calcitonin is a hormone that reduces serum calcium concentration by directly interfering with osteoclast maturation via receptors. Calcitonin inhibits phosphate reabsorption and decreases calcium reabsorption in the kidneys. By attenuating cartilage breakdown and stimulating cartilage formation via inhibitory pathways of matrix metalloproteinases, calcitonin also has a
chondro-protective effect on articular cartilage. Calcitonin has no major effects on intestinal absorption of calcium, but may aid in small-bowel secretion of sodium, potassium, chloride, and water. Calcitonin also has no receptor effect on osteoblasts.
A cartilage water content increase is the hallmark of which
osteoarthritis stage?
Prearthritis
Early
Late
Terminal
The first stage of osteoarthritis is marked by an increase in water content secondary to disruption of the matrix framework. This is followed by an increase in chondrocyte anabolic and catabolic activity in response to tissue damage. Wnt-induced signal protein 1 increases chondrocyte protease expression. Failure to restore tissue balance ultimately leads to continued destruction and osteoarthritis. One hallmark of osteoarthritic cartilage is a reduced repair mechanism attributable to decreased chondrocyte response to growth factor stimulation (transforming growth factor-alpha and insulin-like growth factor-1).
Mitochondrial dysfunction and increased production of reactive oxygen species may promote cell senescence, a progressive slowing of cellular activity. Microscopic evidence of cartilage degeneration begins with fibrillation of the superficial and transition zones, followed by disruption of the tidemark by subchondral blood vessels and eventual subchondral bone remodeling. This process ultimately leads to cartilage degradation with decreased water content in the late and terminal phases of osteoarthritis.
What is the plasma half-life of warfarin?
1 to 2 hours
4 to 6 hours
12 to 18 hours
36 to 42 hours
Warfarin, which is dosed daily, can take 72 to 96 hours to reach therapeutic levels. It has a plasma half-life of 36 to 42 hours. Low-molecular heparins have a plasma half-life of 4 to 5 hours, and fondaparinux has a half-life of 17 to 21 hours. Warfarin will not affect the International Normalized Ratio (INR) until 2 to 3 days after it is given. Patients on chronic warfarin therapy should
have treatment stopped 3 to 5 days before elective surgery to allow the INR to normalize.
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has Factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Type of surgery, age, and BMI
Type of surgery, hypercholesterolemia, and age
Age, BMI, and hypercholesterolemia
BMI, type of surgery, and hypercholesterolemia
Risk stratification is one of the most critical clinical evaluations before undergoing total joint arthroplasty. Many factors have been identified to increase risk for venous thromboembolism (VTE). The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormonal replacement therapy.
Hypercholesterolemia is not a risk factor for thromboembolic disease.
DNA replication occurs during which phase of the cell cycle?
M
S
R
G1
G2
The cell cycle consists of four distinct phases: initial growth (G1), DNA replication/synthesis (S), a gap (G2), and mitosis (M) (see illustration).
The G1 and G2 phases of the cell cycle represent the “gaps” or growth phases in the cell cycle that occur between DNA synthesis and mitosis. G0 cells are in a stable state and have not entered the cell cycle. During the S phase, the DNA is synthesized and replicated. During the M phase or mitosis, all genetic material divides into two daughter cells.
The cells are diploid (2N) in the G0 and G1 phases. The cells become tetraploid (4N) at the end of S and for the entire G2 phases. There is no R phase in the cell cycle.
What antithrombotic agent is a selective factor I0a inhibitor?
Warfarin
Low-molecular-weight heparin
Rivaroxaban
Aspirin
Rivaroxaban is a selective factor I0a inhibitor. Aspirin is a cyclooxygenase inhibitor. Low-molecular-weight heparin is a nonspecific anticoagulant. Warfarin is a vitamin K antagonist and reduces production of clotting factors II, VII, IX, and X.
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic
disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee
Arthroplasty, include
use of mechanical prophylaxis (eg, pneumatic calf compressors) while in the hospital.
oral warfarin with a goal INR between 2.0 and 3.0.
low-dose warfarin for 3 weeks postsurgically beginning 48 hours after surgery.
no prophylaxis because this patient already is partially anticoagulated secondary to her liver disease.
The 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty, recommends the use of mechanical prophylaxis for patients at increased risk
for bleeding (including those with liver disease or hemophilia). This recommendation is the consensus of the workgroup that established these guidelines because there was insufficient evidence to justify a stronger recommendation in this clinical scenario. The other responses use no prophylaxis or pharmacological prophylaxis. Pharmacological prophylaxis is not recommended in patients who are at increased risk for bleeding.
The pharmacokinetics of which deep venous thrombosis (DVT) prophylactic agent are affected by liver function and dietary intake?
Dalteparin
Warfarin
Fondaparinux
Enoxaparin
Warfarin is an oral vitamin K antagonist that is rapidly absorbed from the gastrointestinal tract. It accumulates in the liver, where it is metabolized and excreted. The pharmacokinetics of warfarin can be affected by certain drugs or disease states that influence liver function. Fondaparinux is a synthetic factor Xa inhibitor that is eliminated through the kidneys. Both Dalteparin and Enoxaparin are low-molecular-weight heparins that activate antithrombin and inhibit factors Xa and IIa. Like Fondaparinux, they are eliminated through the kidneys and should be used with caution in patients with kidney disease.
What infection-control measure has been shown to have the most notable impact in reducing surgical-site infections?
Intravenous antibiotic administration within 1 hour of surgical incision
Screening and decolonization of patients colonized with methicillin-resistant
<em>Staphylococcus aureus</em>
Horizontal laminar flow
Use of enclosed body exhaust suits
Timely administration of prophylactic antibiotics is the most important factor shown to decrease surgical-site infections. The use of horizontal laminar flow and body exhaust suits has not been shown to significantly affect infection rates.
The resistance to pullout of a screw in osteoporotic bone is increased by all of the following EXCEPT?
Placement parallel to the trabecular pattern
Purchase in cortical bone
Use of a fixed angle (locking screw construct)
Tapping prior to screw placement
Augmentation with polymethylmethacrylate
Of the options listed, tapping prior to screw placement is the only variable that does not increase the pullout strength of a screw in osteoporotic bone.
Cornell reviews internal fixation in osteoporotic bone. According to this article, the quality of the bone is the primary determinant of the holding power of an individual screw. Other factors that increase the pullout strength include fixation in cortical bone (cortical bone has greater mineral density and, therefore, greater resistance to screw pullout than trabecular bone), screws placed parallel to the trabecular pattern, and screw fixation augmented with PMMA. The addition of a locking plate will also increase the resistance to failure by creating a fixed angle construct. Tapping prior to placement of the screw has not been shown to increase resistance to pullout, on the contrary studies have shown
this decreases resistance to pullout.
Turner et al examined the holding strength of small and large diameter screws in healthy bovine and diseased human bone. They found the screw diameter, trabecular orientation of the bone, and mineral content of the bone all affect the holding strength. A larger diameter screw, parallel placement to the trabecular pattern, and purchase in bone with a higher density all increase the holding strength.
Gigantism affects which region of the growth plate labeled in Figure A?
A
B
C
D
E
Gigantism, like achondroplasia, affects the proliferative zone (Region C of Figure A) of the growth plate. In Figure A, Region A is the epiphysis, Region B is the resting zone, Region D is the hypertrophic zone, and Region E is the metaphysis. Illustration A is another depiction of the physis which is labeled. Gigantism is typically caused by a pituitary adenoma which over secretes growth hormone. Its effect on the proliferative zone results in bone overgrowth and excessive height and limb length. Acromegaly may also be
caused by a pituitary adenoma that over secretes growth hormone, but has its effect once the physis has closed.
Plain radiographs do not provide an accurate assessment of bone mineral density (BMD) until what percentage of mineral has been lost?
Question 63
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
REFERENCES: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 64
Figure 1 shows the clinical photograph obtained from a child with a congenital difference of the hand. What clinical feature(s) is/are characteristic of this condition?

Explanation
The clinical photograph reveals a child with amniotic band syndrome or constriction band syndrome. If a band causes an autofusion of the digits without amputation, acrosyndactyly can occur, as demonstrated in the clinical photograph. Typically, a proximal sinus tract with a distal syndactyly is present. Radial deviation of the thumb can be seen most frequently in Apert syndrome. Cardiac anomalies are associated with many congenital upper extremity differences but are not characteristic of amniotic band syndrome. Ulnar longitudinal deficiency is characterized by hypoplasia or complete absence of the ulna.
Question 65
- Examination of a 45 year old construction worker who was crushed by falling dirt and buried to midchest level reveals hemodynamic instability; however, radiographs of the chest are normal, and results of a diagnostic peritoneal lavage are negative. Despite the administration of a fluid bolus and packed red blood cells, hemodynamic instability persists. A radiograph of the pelvis is shown in Figure 4. The next step in the management should be
Explanation
Question 66
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
REFERENCES: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
MacDonald SJ, Hersche O, Ganz R: Periacetabular osteotomy in the treatment of neurogenic acetabular dysplasia. J Bone Joint Surg Br 1999;81:975-978.
Question 67
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 68
A 28-year-old man underwent open reduction and internal fixation of a closed, displaced, intra-articular calcaneal fracture 8 weeks ago. Examination now reveals that the lateral wound is red and draining purulent material. Cultures obtained from the wound grow out Staphylococcus aureus. Radiographs show early healing of the fracture. What is the next most appropriate step in management?
Explanation
REFERENCES: Benirschke SK, Kramer PA: Wound healing complications in closed and open calcaneal fractures. J Orthop Trauma 2004;18:1-6.
Lim EV, Leung JP: Complications of intra-articular calcaneal fractures. Clin Orthop
2001;391:7-16.
Folk JW, Starr AJ, Early JS: Early wound complications of operative treatment of calcaneus fractures: Analysis of 190 fractures. J Orthop Trauma 1999;13:369-372.
Question 69
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Explanation
85% of patients undergoing arthroscopy for various indications in one study. Internal impingement is defined as impingement of the posterior-superior rotator cuff between the humerus and posterior-superior glenoid rim. Symptomatic internal impingement is felt to be due to the frequency and magnitude of the impingement in throwers.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 252.
Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Question 70
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 181-193.
Question 71
A 56-year-old laborer sustained a subcoracoid dislocation of the shoulder as a result of falling off a scaffold 3 weeks ago. He now is unable to actively raise his arm and has constant pain. What is the most likely diagnosis?
Explanation
Question 72
When treating thoracolumbar spine fractures, which of the following is considered the major advantage of using a thoracolumbosacral orthosis (TLSO) when compared to a three-point fixation brace (Jewett)?
Explanation
REFERENCES: Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 347-349.
Krompinger WJ, Fredrickson BE, Mino DE, Yuan HA: Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am 1986;17:161-170.
Stauffer ES (ed): Thoracolumbar Spine Fractures without Neurological Deficit. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993.
Question 73
A 42-year-old patient has had a fever and low back pain for several days. Laboratory studies show an elevated erythrocyte sedimentation rate and a WBC count of 9,500 mm3 with 75% neutrophils. A CT scan is shown in Figure 15. Examination will most likely reveal what other findings?
Explanation
REFERENCES: Cellier C, Gendre JP, Cosnes J, et al: Psoas abscess complication Crohn’s disease. Gastroenterol Clin Biol 1992;16:235-238.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 470-471, 506.
Question 74
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
Explanation
REFERENCES: Mears DC: Management of pelvic pseudarthroses and pelvic malunion. Orthopade 1996;25:441-448.
Matta JM, Dickson KF, Markovich GD: Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206.
McLaren AC, Rorabeck CH, Halpenny J: Long-term pain and disability in relation to residual deformity after displaced pelvic ring fractures. Can J Surg 1990;33:492-494.
Question 75
A 32-year-old woman has had progressive left foot pain over the first metatarsophalangeal (MTP) joint. Footwear is becoming problematic. There is full range of motion of the first MTP with medial eminence pain. Her weightbearing radiograph reveals a hallux valgus angle (HVA) of 35 degrees and a 1-2 intermetatarsal angle (IMA) of 10 degrees. What is the best next step?
Explanation
Patients with painful progressive hallux valgus are surgical candidates. Presurgical evaluation includes radiographic examination. The IMA between the first and second metatarsals as well as the HVA must be measured. If the IMA is smaller than 15 degrees and the HVA is smaller than 35 degrees, a distal osteotomy is preferred. Distal soft-tissue reconstruction is only useful for IMAs smaller than 11 degrees and HVAs smaller than 25 degrees. Proximal osteotomies and the Lapidus bunionectomy are reserved for larger hallux valgus deformities with IMAs exceeding 15 degrees and HVAs exceeding 35 degrees.
RECOMMENDED READINGS
Pentikainen I, Ojala R, Ohtonen P, Piippo J, Leppilahti J. Distal Chevron Osteotomy: Preoperative Radiological Factors Contributing to Long-Term Radiological Recurrence of Hallux
Valgus. Foot Ankle Int. 2014 Sep 5. pii: 1071100714548703. [Epub ahead of print] PubMed PMID: 25192724. View Abstract at PubMed
Fakoor M, Sarafan N, Mohammadhoseini P, Khorami M, Arti H, Mosavi S, Aghaeeaghdam A. Comparison of Clinical Outcomes of Scarf and Chevron Osteotomies and the McBride Procedure in the Treatment of Hallux Valgus Deformity. Arch Bone Jt Surg. 2014 Mar;2(1):31-
Question 76
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 77
The additional risk of complications in organ transplant patients receiving a total joint arthroplasty is attributed to
Explanation
REFERENCE: Tannenbaum DA, Matthews LS, Grady-Benson JC: Infection around joint replacements in patients who have a renal or liver transplantation. J Bone Joint Surg Am 1997;79:36-43.
Question 78
A 2-year-old child refused to walk 3 days prior to being seen because of pain in the left hip. The pain has gradually subsided and the child is now walking. He is afebrile and has full motion of the hips. Laboratory studies show a normal CBC with differential and C-reactive protein. An ultrasound shows a joint effusion in the right hip. What is the most likely diagnosis?
Explanation
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2068-2070.
Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between
2010 Pediatric Orthopaedic Examination Answer Book • 11
septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004:86:1629-1635.
AL-Madena Copy
12 • American Academy of Orthopaedic Surgeons

Figure 7a Figure 7b
Question 79
Complications following a reverse shoulder prosthesis occur most frequently when performed for what diagnosis? Review Topic
Explanation
Question 80
A 16-year-old right-hand dominant male pitcher has had increasing pain in his dominant shoulder for the past 6 months without treatment. A coronal T2-weighted MRI scan is shown in Figure 80. What is the most appropriate treatment plan? Review Topic

Explanation
Question 81
A 31-year-old man sustained an unstable closed left posterior hip dislocation in a motorcycle accident. A postreduction radiograph is shown in Figure 51a. 3-D CT scans are shown in Figures 51b and 51c. What is the optimal surgical approach that will allow for the most appropriate treatment?

Explanation
Question 82
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
REFERENCES: Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 83
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Davis AM, O’Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 84
Which of the following would be associated with the spinal deformity shown in Figures 79a and 79b? Review Topic
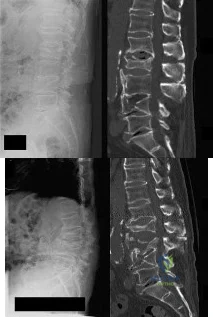
Explanation
Question 85
-Which gene mutation is associated with the condition shown in Figures a and b?

Explanation

Question 86
Figures 47a through 47d are the plain radiographs, axial MRI scan, and biopsy specimen of an 8-yearold boy with progressive right elbow pain that awakens him from sleep. Examination reveals soft-tissue fullness around his elbow and pain with active or passive motion. What is the most likely diagnosis?
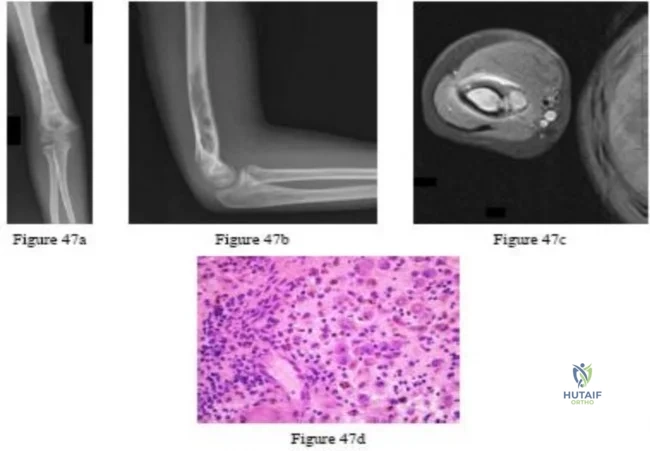
Explanation
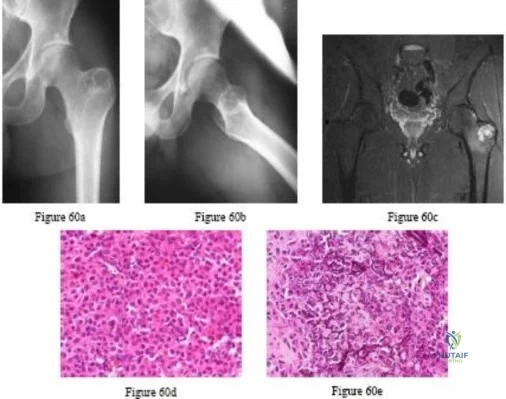
Question 87
Which of the following is an advantage of using blocking screws for tibial nailing?

Explanation
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
Question 88
Figure 19 shows the current radiograph of a 48-year-old man who reports hip pain and marked difficulty walking after undergoing revision of a failed total hip replacement 2 years ago. What is the mechanism of failure?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Gruen TA, McNiece GM, Amstutz HC: “Modes of Failure” of cemented stem-type femoral components: A radiologic analysis of loosening. Clin Orthop 1979;141:17-27.
Question 89
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of
Explanation
REFERENCES: Sailer SL: The role of radiation therapy in localized Ewing’ sarcoma. Semin Radiat Oncol 1997;7:225-235.
Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing’s sarcoma. United Kingdom Children’s Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704.
Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Terek RM, Brien EW, Marcove RC, Meyers PA, Lane JM, Healey JH: Treatment of femoral Ewing’s sarcoma. Cancer 1996;78:70-78.
Question 90
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 312.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 304.
Question 91
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
REFERENCES: DeHaven KE: Meniscus repair. Am J Sports Med 1999;27:242-250.
Dervin GF, Downing KJ, Keene GC, McBride DG: Failure strengths of suture versus biodegradable arrow for meniscal repair: An in vitro study. Arthroscopy 1997;13:296-300.
Barber FA: Endoscopic meniscal repair: The T-fix technique. Sports Med Arthroscopy Rev 1999;7:28-33.
Question 92
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
Explanation
implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
Question 93
A 10-year-old child reports acute leg pain after wrestling with his brother. AP and lateral radiographs are shown in Figures 21a and 21b. What is the best course of action?
Explanation
REFERENCES: Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377.
Ponseti IV, Friedman B: Evaluation of metaphyseal fibrous defects. J Bone Joint Surg Am 1949;31:582.
Question 94
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross-sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 95
A 68-year-old patient undergoes total knee arthroplasty for end-stage degenerative joint disease. Two years later, she trips and falls at home and sustains a fracture seen in Figures A and B. Before her fall, she was a community ambulator and had no knee pain. The component is determined to be stable and the surgeon decides to treat this fracture with closed reduction and retrograde intramedullary fixation with a supracondylar nail. Which of the following statements is true?

Explanation
Periprosthetic femur fractures above total knee implants occur in 2% of patients. It is important to note: (1) pre-injury function, to determine if the prosthesis was loose, (2) the type of implant (CR vs posterior stabilized, PS) as a PS implant with a closed box would make retrograde intramedullary nailing more difficult (the surgeon has to consider the size of the box vs size of the nail, and if the box is smaller than the nail,
must be prepared to enlarge the box with a metal-cutting burr, which has inherent problems of introducing wear debris into the joint), (3) pre-fracture radiographs help determine the position of the implants (flexion-extension, varus-valgus). These fractures can be treated with non-locking condylar buttress plates (not recommended today), fixed angle devices and intramedullary nailing.
McLaren et al. describe 7 osteopenic patients (mean age, 61yrs, range 47-84yrs) treated with retrograde supracondylar nailing. They suggest not reaming, and placing 2-3 screws in the distal fragment. This may require leaving the nail protruding by 1cm. They then suggest removing the protruding segment with a burr at the end of the procedure.
Haidukewych et al. debate plating vs nailing in a 80yr old osteopenic patient. It may be difficult to introduce retrograde intramedullary nails through the same incision if dense scar tissue is present. On the other hand, most plates require extensive dissection and do not respect the soft tissues and fracture biology, except for LISS plates and nails.
Figures A and B show a displaced Lewis and Rorabeck type II periprosthetic fracture. Illustration A shows the technique of retrograde supracondylar nailing. With the knee flexed, the fracture is reduced and the entry point is in the intercondylar notch. Illustration B shows a comparison between PS and CR implants. Note the "box" in the PS implant. This is absent in the CR implant. Illustration C shows the Lewis and Rorabeck classification.
Incorrect Answers:
1 (at most 2) point of fixation in the distal segment. Answer 5: The backup plan should include devices that resist varus collapse (especially in cases with medial comminution), such as angle-stable devices (ABP, DCS and locking plates). Non-locking condylar buttress plates will not resist varus collapse.
Question 96
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
Explanation

Question 97
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 98
-What is the most appropriate initial treatment for her condition?
Explanation
This patient has a history most consistent with multidirectional instability. A lax capsule causes subluxation of the shoulder and strain on the rotator cuff and may result in pain and instability. The capsule is most closely associated with the cause of her problem. Initial treatment for multidirectional instability is physical therapy focusing on restoring balance to the shoulder with rotator cuff and scapular stabilization exercises. Nonsurgical therapy should be protracted and is the mainstay of treatment in this scenario. This patient has exhausted all nonsurgical measures and is now a candidate for surgical reconstruction. Capsular plication will best address the lax capsule and provide the best option for reducing her symptoms. The rotator cuff and biceps tendon may be secondarily strained but are not the primary sources of the problem. The brachial plexus does not address the etiology, but rather the symptoms that may occur as a result of instability of the shoulder joint.
Complete rest will not alleviate the patient's underlying condition because the shoulder girdle may still be weak and symptoms likely will return. A corticosteroid injection and arthroscopic surgery are too invasive as initial treatment for this condition. Arthroscopic rotator cuff repair, a biceps tenodesis, and superior labral anterior-posterior repair are unlikely to result in symptomatic improvement for this patient and are not associated with pathologic findings in the setting of multidirectional instability.
Question 99
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 100
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)? Review Topic
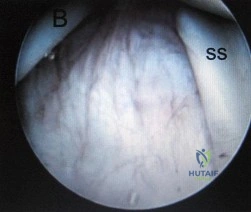
Explanation
