Orthopedic Board Review MCQs: Knee, Shoulder & Arthroplasty | Part 212

Key Takeaway
This page presents Part 212 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review quiz. Designed for orthopedic residents and surgeons, it offers 100 high-yield, verified MCQs on Arthroplasty, Knee, Ligament, Shoulder. Modelled after official exams, its purpose is to optimize your board certification preparation and success.
About This Board Review Set
This is Part 212 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 212
This module focuses heavily on: Arthroplasty, Knee, Ligament, Shoulder.
Sample Questions from This Set
Sample Question 1: Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Opt...
Sample Question 2: A 22-year-old man reports that he initially dislocated his shoulder while playing basketball 2 years ago and was subsequently treated with an arthroscopic Bankart repair. Despite appropriate rehabilitation, the patient continues to report r...
Sample Question 3: The posterior horn of the medial meniscus receives its primary blood supply from what artery? Review Topic...
Sample Question 4: Lipohemarthrosis of the knee is most likely secondary to which of the following?...
Sample Question 5: The artery located within the substance of the coracoacromial ligament is a branch of what artery?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Optimal management should consist of
Explanation
REFERENCES: Lachiewicz PF, Soileau ES: Ten-year survival and clinical results of constrained components in primary total knee arthroplasty. J Arthroplasty 2006;21:803-808.
Anderson JA, Baldini A, MacDonald JH, et al: Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res 2006;442:199-203.

Question 2
A 22-year-old man reports that he initially dislocated his shoulder while playing basketball 2 years ago and was subsequently treated with an arthroscopic Bankart repair. Despite appropriate rehabilitation, the patient continues to report recurrent instability. An axillary view radiograph and CT scan are shown in Figures 57a and 57b. What is the most appropriate management at this time? Review Topic

Explanation
Question 3
The posterior horn of the medial meniscus receives its primary blood supply from what artery? Review Topic
Explanation
Question 4
Lipohemarthrosis of the knee is most likely secondary to which of the following?

Explanation
Question 5
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
REFERENCES: Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Woodburne RT (ed): Essentials of Human Anatomy, ed 2. New York, NY, Oxford University Press, 1983, pp 75-76.
Question 6
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
Explanation
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.


Question 7
What is a risk factor for interdigital neuroma?
Explanation
The only proven risk factor for development of an interdigital neuroma is female gender, which likely is related to the use of fashionable shoes that force plantar flexion of the metatarsal heads and secondary hyperdorsiflexion of the metatarsophalangeal joints. The other factors listed have not been proven to cause interdigital neuroma, as well as mediolateral compression of the forefoot.
RECOMMENDED READINGS
Hill KJ. Peripheral nerve disorder. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:307-327.
Schon LC, Mann RA. Diseases of the nerves. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:613-686.
Question 8
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 9
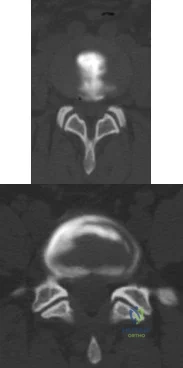
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time? Review Topic
Explanation
sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter.
Question 10
Rupture of the distal biceps tendon is predictably identified by the hook test, which is performed by bringing a finger from lateral to medial across the antecubital fossa of a flexed elbow, feeling for a cord-like structure on which the examiner can "hook" a finger. Bringing the finger from medial to lateral can cause a false-negative result, hooking the lacertus fibrosus, which can remain intact even with a ruptured distal biceps tendon. The Yergason test (option 3) and the Speed test (option 4) are used to assist in diagnosing proximal, not distal, biceps and labral pathology. Even if the distal biceps tendon is ruptured, the supinator remains intact. Although supination weakness may be present, an inability to supinate should not be observed. When treating a closed long finger central slip tendon rupture conservatively, what is the most appropriate plan of care?
Explanation
Closed central slip injuries treated nonsurgically require extension splinting of the PIP joint. DIP joint active range of motion is allowed during this time period. This allows the connections between the lateral bands and the central slip to pull the central slip distally with DIP joint active motion, minimizing the gap
across the central tendon injury and keeping the DIP joint from getting stiff as well.
Question 11
A year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Explanation
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 12
A year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 13
below depict the AP and lateral radiographs obtained from a year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 14
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. What is the most appropriate next step in treatment?
Explanation
Question 15
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of
Explanation
REFERENCES: Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761.
Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Anderson PA, Steinmann JC: Internal fixation of the cervical spine, in Frymoyer JW (ed): The Adult Spine, Principles and Practice, ed 2. Philadelphia, PA, Lippincott Raven, 1997, pp 1119-1147.
Question 16
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
REFERENCES: Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Shaffer B, Tibone JE, Kerlan RK: Frozen shoulder: A long-term follow-up. J Bone Joint Surg Am 1992;74:738-746.
Question 17
Figure 10 is the radiograph of a 44-year-old man with a long-standing history of severe hip pain and a limp. Which clinical scenario most likely could occur when performing total hip arthroplasty on this patient?
Explanation
The radiograph reveals hip dysplasia. Patients with hip dysplasia and severe limb shortening are at high risk for sciatic nerve palsy from overlengthening. Overmedializing the acetabular component is not the preferred response because overlateralization is more of a concern if the cup is placed in the pseudoacetabulum instead of in the true acetabulum. Placing the hip center too inferior is not the preferred response because the concern in this scenario is placing the hip center too superior if the cup is placed in the pseudoacetabulum or if a large-diameter cup is used. Acetabular fractures are possible because of osteoporotic bone at the true hip center, but is less likely than overlengthening of the extremity.

CLINICAL SITUATION FOR QUESTIONS 11 THROUGH 13
Figures 11a and 11b are the radiographs of a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, she has failed nonsurgical treatment including weight loss, activity modifications, and intra-articular injections. Her infection workup reveals laboratory findings within defined limits.
Question 18
A 72-year-old woman underwent a primary total hip arthroplasty 14 months ago. She states that the hip has now dislocated four times when rising from a low chair, requiring closed reduction. A radiograph is shown in Figure 3a and a CT scan of her pelvis is shown in Figure 3b. What is the most reliable method for rectifying her instability?
Explanation
will most reliably rectify the instability in the face of severe component malposition.
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Question 19
A 76-year-old woman has longstanding right shoulder pain affecting overhead function. Figures A and B are her original radiographs. She undergoes reverse total shoulder arthroplasty (rTSA) with iliac crest bone grafting behind the baseplate and is discharged from the hospital the following day. She returns for follow-up at 2 weeks. The incisions have healed and she has minimal pain, which is improving. What is the most accurate description for the cause of failure? Review Topic

Explanation
Glenoid complications are the primary concern of rTSA. Historically, rTSA fail at the glenoid interface because of inadequate fixation. The Grammont-style prosthesis has a medialized center of rotation to circumvent this, but this lead to inferior scapular notching. Newer prosthesis include locking peripheral screws and 15° inferior tilt of the base plate. Further, changing the neck-shaft angle from 155 deg to 143 deg or 135 deg has reduced notching and instability, and reduced the need to for subscapularis repair.
Boileau et al. examined revision surgery for rTSA. They found that the most common cause for revision was prosthetic instability (48%). Humeral complications (loosening/derotation/fracture) were 2nd most common and infection was 3rd most common. Underestimation of humeral shortening and excessive medialization were common causes of recurrent prosthetic instability. Proximal humeral bone loss was found to be a cause for humeral loosening or derotation.
Holcomb et al. reviewed failure of the rTSA glenoid baseplate in 14 patients, which was defined as shift of the baseplate with or without screw breakage. Strategies for success include: (1) Incorporating increased inferior baseplate tilt in post-revision prosthesis-scapular neck angle (PSNA) compared to pre-failure PSNA because inferior tilt maximizes compressive force across the baseplate-glenoid interface. (2) Locking peripheral 5.0mm screws (rather than non-locking 3.5mm screws). (3) Using larger glenospheres to tighten the patulous soft tissue envelope and secure the glenoid allograft. Four patients required structural allograft (2 iliac crest, 2 femoral head).
Figures A shows Hamada 4A cuff tear arthropathy. Figure B shows severe static posterior instability of the humeral head and posterior Walch B2 erosion of the glenoid. Figure C shows the same patient treated with rTSA and iliac crest bone graft. Because of technical error, the central peg was not implanted in the native glenoid. Illustration A shows catastrophic failure of the glenoid baseplate. Illustration B shows the PSNA, with increase in the PSNA from initial rTSA to revision rTSA. Illustration C shows baseplate-glenosphere dissociation. Illustration D shows correction of technical error/too short peg with exchange to a baseplate with a longer peg. Illustration E shows and algorithm for treating unstable rTSA.
Incorrect Answers:
Question 20
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 10a and 10b. Based on the history and imaging findings, what is the most likely diagnosis? Review Topic

Explanation
Question 21
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
REFERENCES: Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 22
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, Ogose A (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 23
A healthy, active year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in A radiograph taken after the fall is shown in He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 24
Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
Explanation
Question 25
A 12-year-old female is referred to the office by a community orthopaedic surgeon concerned that her shoulders appear to be at different heights. With Adam's forward bending, she is noted to have a significant right thoracic rib prominence. She denies pain. A detailed neurological examination reveals no abnormalities. Radiographs of her spine show an apex left lumbar curve measuring 32 degrees and an apex right thoracic curve measuring 28 degrees. She had her first menses last month and her Tanner-Whitehouse staging is consistent with an adolescent steady state. The most appropriate treatment would be? Review Topic
Explanation
Assessing a child's skeletal maturity has important clinical implications when treating patients with idiopathic scoliosis. The Tanner-Whitehouse III method specifically
uses the distal radial and ulnar epiphyses, as well as the metacarpal and phalangeal epiphyses of the first, third, and fifth digits for determination of skeletal age. A Tanner-Whitehouse Stage in 'adolescent steady-state' means she is past peak height velocity. However, as she is before skeletal maturity, and her lumbar and thoracic curvatures are > 25 deg., these curvatures may continue to progress. Therefore, bracing would be the best treatment option at this time.
Hasler et al. randomized twenty post-pubertal young women (20°–40° idiopathic scoliosis to an observation or complementary and alternative osteopathic treatment in a prospective study. Pre- and post- intervention trunk morphology and spine flexibility were assessed at 3 month intervals. A regression analysis of repeat measurements revealed no therapeutic effect on rib hump, lumbar prominence, plumb line, sagittal profile or global spinal flexibility with either treatment.
Sponsellar et al. examined the literature form the past 25 years to summarize the current practice of bracing in the treatment of adolescent idiopathic scoliosis. They found the highest level of existing evidence from a prospective center-randomized study, which showed that thoracolumbosacral bracing was most effective for single curves of 25 to 35 degrees in female patients with a starting Risser score of 0 to 2.
Illustration A shows the bones of interest in the hand and wrist for the the Tanner-Whitehouse III skeletal maturity assessment. Each are divided into epiphysis, metaphysis and diaphysis to help identify these different ossification centers in the phalanx proximity as seen in Illustration B. The development of each region is divided into discrete stages and given a letter (A,B,C,D, . . ., I). These correlate with a score that are added together to give an overall maturity score on the graph.
Incorrect Answers:
Question 26
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
REFERENCES: Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 27
Management of a grade IV osteochondritis dissecans lesion of the capitellum should consist of
Explanation
Lesions are graded I through V based on radiographic and arthroscopic appearance. Grade I lesions show intact but soft cartilage. Grade II lesions show fissuring of the overlying cartilage. Grade III lesions show exposed bone or an attached osteoarticular flap that is not loose. Grade IV lesions show a loose but nondisplaced osteoarticular flap. Grade V lesions show a displaced fragment.
Simple excision of the loose osteoarticular flap is the treatment of choice for grade IV and V lesions. More complex procedures such as drilling of the in situ lesion, bone grafting, or internal fixation are associated with significantly worse results. While some authors advocate abrasion chondroplasty, the long-term benefits of the procedure are yet to be proven.
REFERENCES: Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Shaughnessy WJ, Bianco AJ: Osteochondritis dissecans, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 282-287.
Question 28
A 69-year-old man reports pain over his bunion while wearing shoes and pain in the joint with push-off when barefoot. Nonsurgical management has failed to provide relief. Radiographs are shown in Figures 8a and 8b. What is the surgical procedure of choice?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 3-15.
Tourne Y, Saragaglia D, Zattara A, et al: Hallux valgus in the elderly: Metatarsophalangeal arthrodesis of the first ray. Foot Ankle Int 1997;18:195-198.
Question 29
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 30
A 65-year-old woman presents with neck pain for 18 months. She has taken NSAIDs and undergone physical therapy without improvement. Over the past 6 months, she has also noticed progressive hand clumsiness and difficulty with gait. Sagittal and axial MRI images are shown in figures A and B, respectively. What is the most appropriate next step in management? Review Topic

Explanation
Cervical myelopathy is typically caused compression on the spinal cord and classically present with neck pain, parasthesias, clumsiness, gait imbalance, and/or urinary retention. Nonoperative management is reserved for patients without functional impairment. ACDF is the treatment of choice for focal compression from anterior disc-ostephyte changes. Posterior decompression is indicated in patients with multi-level disease. It is important to note in patients with significant kyphosis, the kyphosis must be reversed in order for decompression alone to be effective.
Hsu reviewed posterior decompression techniques in the cervical spine. They state that the choice of anterior versus posterior approach is determined based on sagittal spine alignment, extent and location of pathological involvement, and patient preference. They recommend laminectomy and fusion for cervical stenosis and kyphosis <10 degrees. The use of BMP-2 as an adjunct in the cervical spine is not recommended by the author.
Emery reviewed cervical spondylotic myelopathy and recommend nonoperative treatment in patients with minimal symptoms without pathologic reflexes or gait imbalances. They suggest that the preferred posterior techniques are now laminectomy and fusion or laminoplasty.
Figure A and B are sagittal and axial T2 MRI sequences showing a degenerative disc osteophyte complex at C5-C6 with resultant canal stenosis and cord compression. Illustration A is a lateral C spine radiograph in a patient who is status post ACDF at C5-C6.
Incorrect Answers:
Question 31
A 26-year-old weightlifter has increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest fails to alleviate his symptoms. He undergoes an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reports mild pain and popping by his clavicle. His clavicle demonstrates mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
Explanation
Question 32
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O’Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.
Question 33
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
Question 34
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
Explanation
8 • American Academy of Orthopaedic Surgeons
DISCUSSION: Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
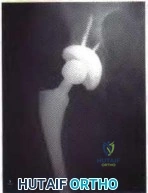
Figure 3a Figure 3b
Question 35
In a pilon fracture, the Chaput fragment typically maintains soft tissue attachment via which of the following structures?

Explanation
Question 36
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 37
What is the theoretical advantage of an open subpectoral technique of tenodesis of the long head of the biceps tendon compared to arthroscopic soft-tissue tenodesis techniques? Review Topic
Explanation
Question 38
Genetic analysis has revealed a strong linkage between osteoarthritis in women with which of the following molecules?
Explanation
of over 400 families showed that type IX collagen is linked to development of OA in women. Mice with a type IX collagen gene deletion are also susceptible to early arthritis. Other genes, such as cartilage enzyme aggrecanase ADAMTS-5, have also been associated with OA.
Question 39
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of
Explanation
REFERENCE: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Question 40
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?
Explanation
with polyethylene wear.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Dowd JE, Sychterz CJ, Young AM, et al: Characterization of long-term femoral-head-penetration rates: Association with and prediction of osteolysis. J Bone Joint Surg Am 2000;82:1102-1107.
Question 41
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 42
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 43
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Explanation
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
Lateral femoral circumflex
Medial femoral circumflex
Superior gluteal
Inferior gluteal
Obturator
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419-424.
Question 44
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
REFERENCES: Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 45
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
REFERENCES: Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Stambough JL, Davidson RS, Ellis RD, et al: Slipped capital femoral epiphysis: An analysis of 80 patients as to pin placement and number. J Pediatr Orthop 1986;6:265-273
Question 46
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?
Explanation
REFERENCES: Gabriel KG: Natural history of hip deformity in spina bifida, in Sarwark JR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 89-103.
Schoenecker PL: Surgical management of hip problems in children with myelomeningocele, in Sarwark KR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 117-131.
Question 47
A 46-year-old male sustains a patella fracture and is treated with cannulated screws and a tension band construct. Which of the following is correct regarding this treatment?
Explanation
Tension band constructs result in absolute stability when performed correctly. This technique works by converting tension from muscle pull into compressive force on the articular side of the fracture. Tension band constructs require a fracture pattern or bone that is able to withstand compression, an intact cortical buttress opposite to the tension band, and fixation that withstands tensile forces.
LeBrun et al. and associates evaluated functional outcomes of surgically isolated patella fractures. They reported that 52% of patients underwent surgery for hardware removal, and 38% of patients who retained their hardware reported pain at some time. They also found that nearly 20% had extensor lag, and almost 38% had restricted flexion. Extension power on testing showed significant mean deficits when compared to the contralateral side.
Bayar et al. evaluated 20 patients with patella fractures and found that articular incongruity of >1mm was the largest risk factor for quadriceps weakness at a mean of 30 months postoperatively. No significant differences were seen with sex, fracture pattern, or time from injury to surgery.
Illustration A shows patella fixation with plate/screw construct. Incorrect Answers:

OrthoCash 2020
Question 48
What is the most common physical examination finding in a patient with chronic painful spondylolysis? Review Topic
Explanation
Question 49
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 50
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?
Explanation
L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis.
REFERENCES: Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997:5:67-78.
Question 51
Which of the following processes does not account for decreased hematopoiesis in patients with metastatic disease?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 52
A 20-year-old soccer player who collapsed after a goal kick reports weakness and nausea. He appears slightly confused. Examination reveals that he is not sweating. His skin is warm and dry. The outdoor temperature is 80 degrees F (26.6 degrees C) with a relative humidity of 80%. Management should consist of
Explanation
REFERENCES: Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902.
Barker TA, Motz HA, Gersoff WK: Environmental factors in athletic performance, in Fu FH, Stone DA (eds): Sports Injuries, ed 2. Philadelphia, PA, Lippincott, 2001, pp 67-68.
Roberts WO: Environmental concerns, in Kibler WB (ed): ACSM’s Handbook for the Team Physician. Baltimore, MD, Williams & Wilkins, 1996, p 172.
Question 53
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure? Review Topic

Explanation
Question 54
A collegiate division I football player ruptures his anterior cruciate ligament (ACL). After counseling him, you agree to perform a double-bundle ACL reconstruction. Which of the following is a correct statement for this technique? Review Topic
Explanation
Question 55
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals?
Explanation
REFERENCES: Steinmann SP: Elbow arthroscopy. J Am Society of the Hand 2003 ;3:199-207.
Dodson CC, Nho SJ, Williams RJ III, et al: Elbow Arthroscopy. J Am Acad Orthop Surg 2008:16:574- 585.
Question 56
Deep anterior compartment
Explanation
Question 57
-A collegiate offensive football lineman has decreased bench-press strength and shoulder pain as off-season workouts begin. Examination revealed no atrophy, and deltoid and rotator cuff strength testing findings were normal. Translational testing was difficult to achieve because of his large size.Apprehension and relocation test findings were negative. An O’Brien’s active compression test result was negative. Jerk testing was positive on the affected side. Which diagnosis is most likely revealed on an MRI arthrogram?
Explanation
Question 58
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 59
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 60
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
Explanation
REFERENCES: Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg
2000;93:53-57.
Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Question 61
What is the minimum hours per day of wear that has been correlated with the effectiveness of bracing on curve progression in idiopathic scoliosis? Review Topic
Explanation
Question 62
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 63
Figure 30 shows the current radiograph of a 32-year-old woman who had a giant cell tumor of the distal radius that was treated with curettage/burring and packed with polymethylmethacrylate 2 years ago. What is the most likely diagnosis?
Explanation
Question 64
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
REFERENCE: Winter RB, Lonstein JE, Denis F, Sta-Ana de la Rosa H: Convex growth arrest for progressive congenital scoliosis due to hemivertebrae. J Pediatr Orthop 1988;8:633-638.
Question 65
A 78-year-old woman undergoes an uneventful semiconstrained total elbow arthroplasty through a Bryan-Morrey approach. Her immediate postoperative management should include which of the following? Review Topic
Explanation
Question 66
A 12-year-old girl has scoliosis at T5-T10 that measures 62°. A clinical photograph of the axilla is shown in Figure 56. Management should consist of
Explanation
REFERENCES: Goldberg Y, Dibbern K, Klein J, Riccardi VM, Graham JM Jr: Neurofibromatosis type 1: An update and review for the primary pediatrician. Clin Pediatr 1996;35:545-561.
Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 67
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
REFERENCES: Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 68
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Explanation
REFERENCES: Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: Observations from retrieved PCA knee implants. Clin Orthop 1992;276:126-134.
Landy MM, Walker PS: Wear of ultra-high molecular-weight polyethylene components of 90 retrieved knee prostheses. J Arthroplasty 1988;3:S73-S85.
Skyrme AD, Mencia MM, Skinner PW: Early failure of the porous-coated anatomic cemented unicompartmental knee arthroplasty: . A 5- to 9-year follow-up study. J Arthroplasty 2002;17:201-205.
Question 69
A 37-year-old laborer sustained a fracture of the posterior acetabular wall. Two years following operative management, the patient reports severely limited hip motion and back pain. Radiographs reveal extensive mature heterotopic ossification with preservation of the hip joint space. Management should now consist of
Explanation
Question 70
An obese 56-year-old woman with hypertension has had posterior heel pain for the past 6 months. She also notes some enlargement over the posterior aspect of the heel. Examination reproduces pain with palpation at the insertion of the Achilles tendon. A lateral radiograph is shown in Figure 45. What is the most likely diagnosis?
Explanation
REFERENCES: Schepsis AA, Wagner C, Leach RE: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619.
Saltzman CL, Tearse DS: Achilles tendon injuries. J Am Acad Orthop Surg 1998;6:316-325.
Question 71
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?
Explanation
REFERENCES: Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Temple HT, Kuklo TR, Sweet DE, et al: Rectus femoris muscle tear appearing as a pseudotumor. Am J Sports Med 1998;26:544-548.
Question 72
A 59-year-old woman who underwent a total hip arthroplasty 5 years ago now has recurrent dislocation following bariatric surgery and a weight loss of 200 lb. An attempt at converting to a larger head size and trochanteric advancement has failed. Her components are well aligned. What is the best course of action?
Explanation
REFERENCES: Goetz DD, Capello WN, Callaghan JJ, et al: Salvage of recurrently
dislocating hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Shrader MW, Parvizi J, Lewallen DG: The use of constrained acetabular component to treat instability after total hip arthroplasty. J Bone Joint Surg Am 2003;85:2179-2183.
Hamilton WG, McAuley JP: Evaluation of the unstable total hip arthroplasty. Inst Course Lect 2004;53:87-92.
Question 73
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 74
What is the most common MRI appearance of a malignant soft-tissue sarcoma?
Explanation
REFERENCES: Bancroft LW, Peterson JJ, Kransdorf MJ, Nomikos GC, Murphey MD: Soft tissue tumors of the lower extremities. Radiol Clin North Am 2002;40:991-1011.
Berquist TH, Ehman RL, King BF, et al: Value of MR imaging in differentiating benign from malignant soft-tissue masses: Study of 95 lesions. Am J Roentgenol 1990;155:1251-1255.
Crim JR, Seegar LL, Yao L, et al: Diagnosis of soft tissue masses with MR imaging: Can benign masses be differentiated from malignant ones? Radiology 1992;185:581-586.
Question 75
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of Review Topic

Explanation
Question 76
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
Explanation
REFERENCES: Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
Question 77
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 78
A 15-year-old male jumps off a 6 foot ramp and lands awkwardly. His knee swells up immediately and he is taken to the emergency room. Figures A is a sagittal CT scan image. In the next 3 hours, he complains of increasing leg pain. This is likely because of injury to which of the following structures? Review Topic

Explanation
Tibial tubercle fractures usually occur during aggressive quadriceps contraction during sports. The Ogden classification classifies this by site of fracture (Type I, through the tubercle; Type II, at the level of the tibial physis; Type III, extending through the anterior tibial epiphysis). Other complications include extensive soft tissue damage, periosteal stripping, vascular compromise and intra-articular damage.
Pandya et al. reviewed 41 tibial tubercle fractures. They found compartment syndrome or vascular compromise in nearly 10%. They found that the degree of injury was underestimated 50% of the time when classified using lateral radiographs alone. They recommend CT scan or MRI as an adjunct. If intra-articular involvement is seen, arthroscopy or open arthrotomy should be performed.
Pape et al. describe 2 case reports of anterior compartment syndrome after tibial tubercle fracture. The compartment syndrome occurs as a result of proximity of the tibial tubercle physis to the anterior tibial recurrent artery.
Figure A shows the sagittal reconstruction CT image showing intraarticular involvement. Illustrations A and B are axial and coronal CT images in the subchondral region showing the fracture line traversing the zone between fused and unfused physis (see Illustration C for physeal closure pattern). Illustration C shows the direction of closure of the proximal tibial physis. In the sagittal plane, the proximal tibial physis closes from posterior to anterior, then to the tubercle apophysis which closes from proximal to distal also. In the coronal plane, the physis closes from medial to lateral. In the axial plane, the physis closes from posteromedial to anterolateral. Illustration D shows the anterior tibial recurrent artery.
Incorrect Answers:
Question 79
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of

Explanation
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
Question 80
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
REFERENCES: Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.
Question 81
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
REFERENCES: Moiemen NS, Elliot D: Primary flexor tendon repair in zone I. J Hand Surg Br 2000;25:78-84.
Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 82
A 72-year-old man injured his right shoulder after tripping over a chair leg. Radiographs obtained in the emergency department reveal an isolated anterior dislocation. After successful closed reduction, the patient has recurrent anterior instability and is unable to elevate the arm. What is the most likely cause of the recurrent instability?
Explanation
REFERENCES: Nevaiser RJ, Nevaiser TJ: Recurrent instability of the shoulder after age 40.
J Shoulder Elbow Surg 1995;4:416-418.
Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Question 83
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
REFERENCES: Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998,
pp 1826-1844.
Mirkovic S, Garfin SR: Spinal stenosis: History and physical examination. Instr Course Lect 1994;43:435-440.
Question 84
The photomicrograph seen in Figure 41 shows which of the following conditions?
Explanation
REFERENCES: Krall RA, Kostianovsky M, Patchefsky AS: Synovial sarcoma: A clinical, pathological and ultrastructural study of 26 cases supporting the recognition of a monophasic variant. Am J Surg Pathol 1981;5:137-151.
Wright PH, Sim FH, Soule EH, Taylor WF: Synovial sarcoma. J Bone Joint Surg Am 1982;64:112-122.
Question 85
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 86
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?
Explanation
REFERENCES: Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Sharkey PF, Hozack WJ, Dorr LD, Maloney WJ, Berry D: The bearing surface in total hip arthroplasty: Evolution or revolution, in Price CT (ed): Instructional Course Lectures 49. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 41-56.
Question 87
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of
Explanation
REFERENCES: Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
Shereff MJ, Baumhauer JF: Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J Bone Joint Surg Am 1998;80:898-908.
Question 88
-Figures a and b are the plain radiographs of a 26-year-old man with an elbow contracture. He denies any specific elbow trauma but reports a history of a closed-head injury sustained in a motor vehicle collision. Examination reveals the elbow lacked 55 degrees of extension and has flexion of 85 degrees.Supination and pronation are well preserved. Release of which structure is essential to restore elbow flexion?

Explanation

Question 89
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
(p < 0.001) after surgery.
REFERENCES: Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Feagan BG, Wang CJ, Kirkley A, et al: Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: A randomized, controlled, trial. Ann Intern Med 2000;133:845-854.
Question 90
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
Explanation
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity
= 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Question 91
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20°. Management should consist of
Explanation
REFERENCES: Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Newton PO, Johnston CE II: Analysis and treatment of poor outcomes following in situ arthrodesis in adolescent spondylolisthesis. J Pediatr Orthop 1997;17:754-761.
Question 92
At the time of arthroscopy, a 9-year-old boy was found to have a Watanabe type II discoid lateral meniscus. What is the most appropriate treatment? Review Topic
Explanation
Question 93
Compared with surgically treated patients, patients with extra-articular distal third humeral shaft fractures that are treated nonsurgically with functional bracing can be expected to show which of the following findings?
Explanation
Question 94
Which of the following statements best describes results that have been reported with roentgen stereophotogrammetric analysis (RSA)?
Explanation
varus-coronal plane and retroversion-transverse plane, or both) has been associated with a higher risk of loosening of the component.
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 100.
Question 95
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 96
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
Explanation
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 97
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C 40- A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
A. Elbow arthroscopy with debridement
B. Immobilization and rest for 6 weeks
C. Corticosteroid injection
D. Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
42- Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 98
A 29-year-old recreational basketball player has developed pain to the distal aspect of her patella that occurs during warm-ups and returns toward the end of the game. She reports no history of trauma, effusions, instability, and no mechanical symptoms. On examination, she is point tender at the inferior pole of the patella, lacks patella apprehension, and has a Q-angle of 15°. She has no ligamentous laxity. Radiographs are unremarkable. What is the best next step?
Explanation
Question 99
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H,
Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3939-3962.
Question 100
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time? Review Topic
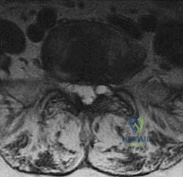
Explanation
point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.
(SBQ12SP.20) Amphotericin B is most appropriate for the treatment of which type of spine infection? Review Topic
Fungal osteomyelitis
Bacterial osteomyelitis with a gram-positive organism
Bacterial osteomyelitis with a gram-negative organism
Tuberculous osteomyelitis
Viral meningomyelitis
Amphotericin B would be most appropriate for the treatment of fungal infections of the spine.
Amphotericin B is a broad-spectrum anti-fungal medication. It is commonly used as the first-line agent for treatment of fungal infections of the spine. The most common fungi involving the spine include cryptococcus, candida, and aspergillus. The indications for débridement and stabilization with spinal fusion, includes resistance to antibiotic therapy, spinal instability, and/or neurologic deficits.
Kim et al. reviewed fungal infections of the spine. They comment that fungus infections are most commonly spread by hematogenous or direct spread. Access to the vascular system may include intravenous lines, during implantation of prosthetic devices, or during surgery.
Frazier et al. retrospectively reviewed 11 patients with fungal osteomyelitis of the spine. Nine of the patients were immunocompromised secondary to diabetes mellitus, corticosteroid use, chemotherapy for a tumor, or malnutrition. All were treated with anti-fungal medication. 10 of 11 patients were also treated with surgical debridement. Paralysis secondary to the spine infection developed in eight patients. After an average of 6.3 years of follow-up, the infection had resolved in all nine surviving patients.
Illustration A shows the mechanism of action of Amphotericin. Illustration B shows T1- (Image A and B) and T2-weighted (Image C) images of the lower thoracic and lumbar spine. There are hypointense signals within the T12 and L1 vertebral bodies (Images A and B) indicative of fungal osteomyelitis.
IncorrectAnswers:
