Orthopedic Board Review MCQs: Adult Reconstruction, Trauma, & Deformity | Part 182

Key Takeaway
This page presents Part 182 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. Designed for orthopedic residents and surgeons, it features 100 high-yield MCQs, mirroring board exam format. Utilize interactive study or exam modes with clinical explanations to confidently prepare for certification and in-training examinations.
About This Board Review Set
This is Part 182 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 182
This module focuses heavily on: Ankle, Arthroplasty, Deformity, Fracture, Hip, Ligament, Nerve.
Sample Questions from This Set
Sample Question 1: As an orthopaedic surgery resident, you arrive late to a medial patellofemoral ligament reconstruction procedure in your institution's outpatient surgical center. It is standard practice in your residency program to miss the start of the fi...
Sample Question 2: -Which of the following nerves lying between the gluteus medius and minimus is at risk for injury in a lateral approach to the hip?...
Sample Question 3: Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of...
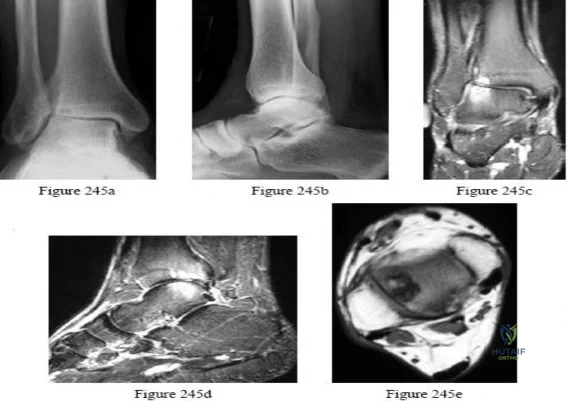
Sample Question 4: Figures 245a through 245e are the radiographs and MRI scans of a 50-year-old ice hockey referee with a 3-year history of progressive anterolateral ankle pain, a history of multiple ankle sprains, and a fibular fracture he sustained 30 years...
Sample Question 5: A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
As an orthopaedic surgery resident, you arrive late to a medial patellofemoral ligament reconstruction procedure in your institution's outpatient surgical center. It is standard practice in your residency program to miss the start of the first case because of didactic requirements on Tuesdays. The surgical team has your gown and gloves ready, and following scrubbing and gowning, you join the surgical team and assist the attending with the procedure. Which of the following represents a violation of standard surgical safety checklists?
Explanation
The World Health Organization and nearly every professional surgical subspecialty group advocates for safety checklists prior to operations. Although there are institutional variations to individual items on the checklists, it is important to include a system for marking the surgical site, verifying the patient's identity and procedure planned, identifying all team members in the room and agreement regarding the type of anesthesia, antibiotic prophylaxis, instrumentation used. Simply put, safety checklists have been shown to drastically reduce costly errors in other high-risk
industries, and they have been universally adopted by hospitals and surgery centers and the organizations that inspect and validate healthcare settings.
The Joint Commission Guidelines and the WHO surgical safety checklists are examples of governing bodies of healthcare implementing safety checklists in procedural settings.
Illustration A is the WHO surgical safety checklist. Incorrect Answers:
Question 2
- Which of the following nerves lying between the gluteus medius and minimus is at risk for injury in a lateral approach to the hip?
Explanation
The direct lateral approach (Transgluteal approach). No true intervenous plane (“split the fibers” of the gluteus medius “distal to the point where the superior gluteal nerve supplies the muscle”). “Do not (split) more than 3 cm above the upper boarder of the trochanter.”
Question 3
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of
Explanation
REFERENCES: Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: Long-term follow-up of 29 cases treated by microvascular bone transfer. Clin Orthop 1995;314:37-44.
Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV: Congenital pseudarthrosis of the tibia associated with neurofibromatosis - 1: Treatment with Ilizarov’s device. J Pediatr Orthop 1997;17:675-684.
Anderson DJ, Schoenecker PL, Sheridan JJ, Rich MM: Use of an intramedullary rod for the treatment of congenital pseudarthrosis of the tibia. J Bone Joint Surg Am 1992;74:161-168.
Question 4
Figures 245a through 245e are the radiographs and MRI scans of a 50-year-old ice hockey referee with a 3-year history of progressive anterolateral ankle pain, a history of multiple ankle sprains, and a fibular fracture he sustained 30 years ago. Examination reveals mild bilateral pes planovalgus feet with passive ankle joint dorsiflexion range of motion of 10 degrees and plantar flexion of 45 degrees without pain. The physician should recommend
Explanation

Question 5
A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
Explanation
are several treatment options available. The best option for survivorship is a cementless
porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants.
REFERENCES: Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936.
D’Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.
Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.
Question 6
An year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 7
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
REFERENCES: Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Weber TG, Manoli A II: Compartment syndromes of the foot. Foot Ankle Clin 1999;4:473-486.
Question 8
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Howard FM: Fracture of the basal joint of the thumb. Clin Orthop 1987;220:46-51.
Question 9
The patient develops an inability to dorsiflex her foot 2 days after surgical intervention while she is sitting in a chair after physical therapy. Initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis.
This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis, observation for 1 year would not be appropriate.
The psoas is the anatomic structure that runs anterior to the acetabulum. The femoral neurovascular structures are at risk if the retractor is placed anterior and inferior to the psoas tendon.
The patient develops a foot drop 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MR imaging or a CT scan may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be decreased by flexing the surgical knee and positioning the bed flat.
Question 10
Which of the following results cannot be achieved with an in-shoe orthosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 55-64.
Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Buonomo LJ, Klein JS, Keiper TL: Orthotic devices: Custom-made, prefabricated, and material selection. Foot Ankle Clin 2001;6:249-252.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 11
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
REFERENCE: Ebraheim NA, Haman SP, Xu R, Stanescu S, Yeasting RA: The lumbosacral nerves in relation to dorsal SI screw placement and their locations on plain radiographs. Orthopedics 2000;23:245-247.
Question 12
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 13
The sartorius muscle is innervated by which of the following nerves?
Explanation
REFERENCES: Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 139.
Question 14
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
Explanation
REFERENCES: Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34.
Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 15
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
REFERENCES: Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed):
Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 16
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Explanation
REFERENCES: Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Question 17
During fracture healing, granulation tissue tolerates the greatest strain before failure so that mature bone can eventually bridge the fracture gap during healing. What is the definition of strain?
Explanation
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary bone healing and secondary bone healing takes place at tissue strain of 2-10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40% or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
Question 18
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 19
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in
Explanation
REFERENCES: O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 20
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel’s sign is noted plantar medially and no Mulder’s click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?
Explanation
REFERENCES: Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. Philadelphia, PA, JB Lippincott, 1983.
Question 21
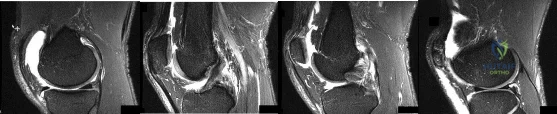
Figures 1 through 4 are selected sagittal MR images of an otherwise healthy 20-year-old collegiate football running back who was tackled during a game and has immediate onset of right knee pain. Video analysis of the injury shows that his flexed knee impacted the field. He is not able to return to play. On examination in the training room the following morning, he has a moderate effusion, no patellar instability, minimal joint line tenderness, and is stable to varus and valgus stress at 30° of knee flexion. A dial test is also negative. He has increased laxity in the anterior to posterior direction. What is the most appropriate next step in treatment?
Explanation
This athlete sustained an isolated PCL injury. The mechanism of injury is typical for a PCL injury. When a PCL injury is identified, one must rule out other ligamentous injuries to the knee. The patient has a stable examination to varus and valgus and a negative dial test, so the lateral collateral, medial collateral, and posterolateral corner (respectively) are intact. It is common to have increased anterior to posterior translation in isolated PCL injuries, even with an intact ACL, as the tibia will rest posterior to the medial femoral condyle. Treatment of isolated PCL injuries is typically nonoperative, with an initial focus on quadriceps strengthening. Hamstring strengthening and rehabilitation is added at a later time, as this places increased stress on the healing PCL. The images reveal an isolated PCL injury with intact menisci and ACL, ruling out ACL reconstruction using autograft tissue and PCL reconstruction using autograft tissue.
Question 22
A patient undergoing joint arthroplasty is put on a drug that competitively inhibits the activation of an enzyme that breaks down Factor Ia. The drug is
Explanation
Tranexamic acid competitively inhibits the activation of plasminogen to plasmin by binding to specific sites on both plasminogen and plasmin. Tranexamic acid has roughly eight times the antifibrinolytic activity of an older analogue, e-aminocaproic acid. It is used during joint replacement surgery to reduce blood loss and the need for transfusion.
Watts et al. review strategies for minimizing blood loss and transfusion. They recommend 1g of TXA prior to incision, and 1g at wound closure. They also recommend giving fluids for symptoms of anemia, rather than transfusion, as even high risk patients do well with sufficient intravascular volume even with low hemoglobin levels.
Imai et al. evaluated TXA in 107 patients undergoing THA. They found that intraoperative blood loss after preoperative TXA administration was lower than both control and postoperative TXA administration groups. They recommend using 1 g of TXA 10 minutes before surgery and 6 hours after the first administration to best reduce blood loss during THA.
Gillette et al. retrospectively reviewed 2046 patients receiving TXA for THA or TKA together with either aspirin, warfarin or dalteparin. They found that the rates of symptomatic DVT (0.35%, 0.15%, and 0.52%, respectively) and nonfatal PE were similar (0.17%, 0.43%, and 0.26%, respectively) for the 3 drugs respectively. They recommend TXA to decrease blood loss and transfusion.
Illustration A shows the role of tranexamic acid in the fibrinolytic cycle and the
clotting cascade.
Incorrect Answers:
Question 23
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
Explanation
REFERENCES: Levine AM: Traumatic spondylolisthesis of the axis (Hangman’s fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
Question 24
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
REFERENCES: Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 25
Which of the following statements best describes the relationship between tissue response to thermal capsulorrhaphy and the type of device used?
Explanation
REFERENCES: Arnoczky SP, Aksan A: Thermal modification of connective tissues: Basic science considerations and clinical implications. J Am Acad Orthop Surg 2000;8:305-313.
Hayashi K, Markel MD: Thermal modification of joint capsule and ligamentous tissues: The use of thermal energy in sports medicine. Operative Techniques Sports Med 1998;6:120-125.
Naseef GS III, Foster TE, Trauner K, et al: The thermal properties of bovine joint capsule: The basic science of laser- and radiofrequency-induced capsular shrinkage. Am J Sports Med 1997;25:670-674.
Question 26
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 27
Figures 63a and 63b show the radiographs of an 11-year-old girl who sustained a twisting injury of the knee playing soccer. She is now asymptomatic. What is the appropriate treatment of the lesion?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 77-85.
Question 28
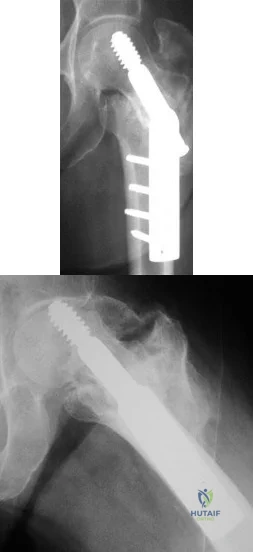
Figures A and B show the six-month follow-up radiographs of a 62-year-old woman who sustained a hip fracture in a fall. Prior to the fall, the patient was active and had no difficulty with ambulation. The patient underwent open reduction and internal fixation with a sliding hip screw device. She has difficulty with ambulation, continues to walk with a walker, and reports startup pain. What is the most appropriate management at this time? Review Topic
Explanation
Question 29
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
REFERENCES: Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
Scaduto AA, Cracchiolo A III: Lacerations and ruptures of the flexor or extensor hallucis longus tendons. Foot Ankle Clin 2000;5:725-736.
Question 30
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport? Review Topic
Explanation
stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing.
Question 31
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
REFERENCES: Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting
limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 32
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future? Review Topic
Explanation
Question 33
Figures 124a and 124b are the radiographs of a 30-year-old man who sustained an ankle injury and has swelling with lateral tenderness. The patient denies any previous ankle injuries. After 6 weeks of rest and use of a removable ankle brace, he continues to have swelling, lateral pain, and popping. An anterior drawer test reveals a solid end point. Recommended treatment should include which of the following?

Explanation
of lateral ankle ligament instability. Ankle rehabilitation and physical therapy may further damage the unstable tendons.
Question 34
-A 32-year-old man who is a smoker sustained an open tibial fracture and underwent a staged treatment with placement of an intramedullary nail. Four weeks after surgery, he developed a pseudomonas deepwound infection. What is the strongest predictor of persistent infection if implants are retained until fracture union?
Explanation

Question 35
A 45-year-old man feels a pop in the anterior aspect of his elbow while lifting furniture. He denies any antecedent pain or injury. Which examination method is best for diagnosing a distal biceps rupture?
Explanation
Question 36
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 37
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
Question 38
A 29-year-old man reports severe knee instability and popliteal pain. History reveals that he had polio of the left lower extremity as a child and has been brace-free his entire life. Examination reveals that he walks with 40° of knee hyperextension and has a fixed ankle equinus deformity of 30° . He has no active motors about the knee or ankle. Which of the following methods will provide knee stability and pain relief?
Explanation
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
Question 39
All of the following conditions are associated with the female athlete triad EXCEPT? Review Topic
Explanation
The female athlete triad is an interrelationship of menstrual dysfunction (i.e., amenorrhea or oligomenorrhea), low energy availability (insufficient caloric intake for demand, with or without an eating disorder) and decreased bone mineral density. It is relatively common among young women participating in sports. More recently, it has been suggested that endothelial dysfunction also results, due to an imbalance between vasodilating and vasoconstricting agents triggered from inappropirate levels of nitric oxide on the microscopic level, which predisposes these women to atherosclerotic changes and increases their risk of cardiovascular disease in the future.
Matheson et al. analyzed cases of 320 athletes with bone scan-positive stress fractures (M = 145, F = 175) seen over 3.5 years and assessed the results of conservative management. They found that conservative treatment of stress fractures in athletes is satisfactory in the majority of cases.
Constantini et al. evaluated the prevalence of vitamin D insufficiency and deficiency among young athletes and dancers. They found a higher rate of vitamin D insufficiency among participants who practice indoors, during the winter months, and in the presence of iron depletion.
Nazem et al. reviewed the major components and health consequences of the female athlete triad as well as strategies for diagnosis and treatment of the conditions. They concluded that treatment requires a multidisciplinary approach involving health care professionals as well as coaches and family members.
Yagi et al. followed 230 runners participating in high school running teams for a total of 3 years to report occurrence of medial tibial stress syndrome (MTSS) and stress fracture. Predictors of MTSS and stress fracture were investigated. The authors reported a significant relationship between BMI, internal hip rotation angle and MTSS infemales.
Incorrect Answers:
Question 40
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 41
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?
Explanation
High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics.
REFERENCES: Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Penner MJ, Masri BA, Duncan CP: Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J Arthroplasty 1996;11:939-944.
Question 42
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Kwon BK, Vaccaro AR, Grauer JN, et al: Subaxial cervical spine trauma. J Am Acad Orthop Surg 2006;14:78-89.
Question 43
An active 65-year-old man has pain in the left shoulder 5 years after undergoing a hemiarthroplasty. He has a remote history of two previous instability operations. Examination reveals that forward elevation is 140 degrees and external rotation is 40 degrees. Serologic studies for infection are negative. AP and axillary radiographs are shown in Figures 7a and 7b. What surgical procedure will provide the most predictable pain relief and function? Review Topic

Explanation
Question 44
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 45
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
REFERENCES: Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997;79:874-880.
Frazier DD, Campbell DR, Garvey TA, et al: Fungal infections of the spine: Report of eleven patients with long-term follow-up. J Bone Joint Surg Am 2001;83:560-565.
Hadjipavlou AG, Mader JT, Necessary JT, et al: Hematogenous pyogenic spinal infections and their surgical management. Spine 2000;25:1668-1679.
Question 46
A 52-year-old man sustained the left elbow injury shown in Figure A while playing basketball 2.5 months ago. He underwent the procedure shown in Figure B. Post-operatively he was mobilized in a hinged brace. On examination today, his arc of elbow flexion is 75 degrees with loss of 45 degrees of full extension. His Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure score is 45 points. What initial treatment option will likely provide the greatest improvement in this patients DASH score and functional range of motion? Review Topic

Explanation
Post-traumatic elbow stiffness is often difficult to manage. The ultimate goal of treatment is to restore a functional range of elbow motion (30° to 130°). Nonoperative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static progressive elbow splinting with a turnbuckle, alongside aggressive physical therapy, has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Doornberg et al. looked at a retrospective case series of 29 patients with posttraumatic elbow stiffness. They showed that static progressive splinting can help gain additional motion when standard exercises fail to produce additional improvements.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12 month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Figure A shows a posterior elbow dislocation with an associated medial epicondyle fracture. Figure B shows ORIF of the fracture seen in Figure A. Illustration A shows a static progressive turnbuckle elbow splint used for post-traumatic elbow stiffness.
Incorrect Answers:
Question 47
A 22-year-old man who plays recreational soccer (Figure 41)
Explanation

Question 48
A 68-year-old woman with serologically proven rheumatoid arthritis underwent an open synovectomy and radial head resection 10 years ago. She now has severe pain that has failed to respond to nonsurgical management. Examination reveals a flexion arc of greater than 90 degrees. Radiographs are shown in Figures 15a and 15b. What is the most appropriate management?
Explanation
REFERENCES: Whaley A, Morrey BF, Adams R: Total elbow arthroplasty after previous resection of the radial head and synovectomy. J Bone Joint Surg Br 2005;87:47-53.
Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.
Schemitsch EH, Ewald FC, Thornhill TS: Results of total elbow arthroplasty after excision of the radial head and synovectomy in patients who had rheumatoid arthritis. J Bone Joint Surg Am 1996;78:1541-1547.
Question 49
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
Explanation
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. View Abstract at PubMed
Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.View Abstract at PubMed
Question 50
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 51
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
Question 52
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of
Explanation
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Boyd JB, Anderson LD: A method for reinsertion of the distal biceps brachii tendon. J Bone Joint Surg Am 1961;43:1041-1043.
Morrey BF, Askew LJ, An KN, Dobyns JH: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418-421.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 53
A right-hand-dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
the radial tuberosity.
Question 54
A subtrochanteric femur fracture in which the lesser trochanter is intact is associated with what deformity?
Explanation
Question 55
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 56
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 57
A 71-year-old woman reports the insidious onset of shoulder pain at night and when moving her shoulder. She cannot raise her arm above shoulder level. Physical therapy has failed to provide pain relief or improve function. An injection relieved her pain in the office, but she could not raise her arm above shoulder level. A radiograph is shown in Figure 21. What surgical procedure will provide the best chance of restoring above shoulder function and pain relief? Review Topic

Explanation
Question 58
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 59
A 24-year-old professional basketball player reports the gradual onset of pain that is poorly localized to the left midfoot for the past 2 months. Examination reveals diffuse tenderness to palpation, full range of motion of the ankle and subtalar joint, and a normal neurovascular examination to the foot. An AP radiograph is shown in Figure 10. Definitive treatment should include
Explanation
REFERENCES: Torg JS, Pavlov H, Cooley JH, et al: Stress fractures of the tarsal navicular.
J Bone Joint Surg Am 1982;64:700-712.
Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2391-2409.
Question 60
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis?

Explanation
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 61
A 35-year-old woman is involved in a head-on collision while driving. Initial radiographs are shown in Figures 8a and 8b. Injury to what vessel increases the risk for osteonecrosis of the injured bone?

Explanation
Question 62
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
REFERENCES: Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 63
Duchenne’s muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?
Explanation
REFERENCES: Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Smith SA, Swaiman HF: Muscular dystrophies, in Swaiman KF, Ashwall S (eds): Pediatric Neurology Principles and Practice, ed 3. St Louis, MO, Mosby, 1999, pp 1235-1237.
Question 64
What are the four most common soft-tissue sarcomas to spread via the lymph node system?
Explanation
REFERENCES: Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Blazer DG III, Sabel MS, Sondak VK: Is there a role for sentinel lymph node biopsy in the management of sarcoma? Surg Oncol 2003;12:201-206.
Question 65
Which of the following statements best describes synovial fluid?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 443-470.
Question 66
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident. The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria? Review Topic
Explanation
Question 67
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 68
A 28-year-old professional football player reports painless loss of ankle motion after sustaining a “severe” ankle sprain 12 months ago. A mortise radiograph is shown in Figure 1. Surgical treatment should be reserved for which of the following conditions?
Explanation
REFERENCES: Whiteside LA, Reynolds FC, Ellsasser JC: Tibiofibular synostosis and recurrent ankle sprains in high performance athletes. Am J Sports Med 1978;6:204-208.
Henry JH, Andersen AJ, Cothren CC: Tibiofibular synostosis in professional basketball players. Am J Sports Med 1993;21:619-622.
Andrish J: The leg, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2155-2181.
Question 69
What is the most common neurologic problem associated with a simple shoulder dislocation? Review Topic
Explanation
Question 70
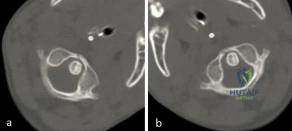
A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynamic computed tomographic (CT) was obtained and shown in Figure A. Panel (a) shows an axial image with maximal rotation to the left. Panel (b) shows an axial image with maximal rotation to the right. What is the most appropriate next step in management? Review Topic
Explanation
Common causes of Atlantoaxial rotatory displacement (AARD) include infection, trauma, and recent neck surgery. Diagnosis is challenging and is best confirmed with dynamic CT (CT with the head turned maximally to either side and at neutral). If the symptoms are acute (less than 7 days) then initial treatment with a soft collar and anti-inflammatory medications is indicated. If the condition has been present for more than a week, more aggressive treatment with halter traction (present 1 week to 1 month) or halo traction (present for 1-3 months) is indicated. If nonoperative modalities fail, the condition has been present for > 3 months, or the patient has neurologic deficits, then posterior C1-C2 fusion is indicated.
Copley et al discuss the evaluation and treatment of various congenital and traumatic conditions of the pediatric cervical spine. They report that the underlying mechanism of Atlantoaxial rotatory displacement (AARD) is inflammation and spasm which can be caused by infection, prior surgery, trauma, and rheumatoid arthritis.
Subach et al reviewed at 20 children with atlantoaxial rotatory subluxation. They found that of the 20 patients treated overall, conservative management failed in 6 (30%), and they required posterior fusion because of recurrence of the atlantoaxial rotatory subluxation or unsuccessful reduction. The major factor predicting the failure of conservative management was the duration of subluxation before initial reduction. Patients with long-standing subluxation were more likely to experience recurrence and require surgery.
Figure A shows an asymmetric placed odontoid within the ring of C1. There is an increased distance from the odontoid to the right arch of C1 which is fixed and minimally changes with maximal rotation to the left. This radiographic finding is indicative of fixed subluxation. Illustration A further demonstrates this.
Incorrect
(SBQ12SP.1) A 65-year-old female with a history of breast cancer presents with bilateral buttock and leg pain that is worse with walking and improves with sitting. In addition, she reports that she feels unsteady on her feet and requires holding the railing when going up and down stairs. On physical exam she is unable to complete a tandem gait and has hip flexion weakness, ankle dorsiflexion weakness, and ankle plantar flexion weakness. Her reflex exam shows 3+ bilateral patellar reflexes. Radiographs and an MRI are shown in Figure A and B. What is the next most appropriate step in management. Review Topic

Lumbar epidural injection
Physical therapy with core strengthening and anti-inflammatory medications as needed
Lumbar decompression
Lumbar decompression and fusion
MRI of the cervical and thoracic spine
The clinical scenario is consistent with a patient with symptoms of degenerative spondylolisthesis AND symptoms of myelopathy. Myelopathy must be ruled out by performing an MRI of the cervical and thoracic spine.
Tandem stenosis occurs in approximately 5 to 25% of patients. Because of the stepwise progressive nature of myelopathy, treatment of myelopathy often takes precedence over lumbar spinal stenosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies. Both the upward babinski reflex and the presence of clonus were found to be very non-sensitive (13%). The most sensitive provacative test was found to be the Hoffman sign (59%).
Salvi et al. reviewed the classic presentations for cervical myelopathy including demographics, history, and physical exam findings (the inability to preform a tandem gait, hyperreflexia, an abnormal babinksi and hoffman reflex, the inability to preform rapid movements and bilateral muscle weakness). Additionally they identify other potential causes for myelopathy, including multiple sclerosis, amyotrophic lateral sclerosis, multifocal motor neuropathy, and Guillain-Barre´syndrome.
Maezawa et al. showed that gait analysis can identify a pattern in patients with myelopathy. Patients with severe myelopathy have a characteristic gait with hyperextension of the knee in the stance phase without plantar flexion of the ankle in the swing phase. They also have decreased walking speed and stride length with a prolonged stance phase.
Figure A and B show a classic degenerative spondylolisthesis.
Incorrect Answers:
Question 71
The quadrilateral space in the shoulder contains which of the following structures?
Explanation
REFERENCES: Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 61-62.
Question 72
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient’s symptoms at this time?
Explanation
REFERENCES: Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 73
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Explanation
Question 74
- The radiograph shown in Figure 50a and the CT scan shown in Figure 50b reveal a lesion in the left femoral neck of a 12-year-old boy who has pain in the left hip. The most likely cause of the osteopenia of the left proximal femur is
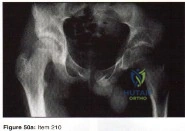
Explanation
Question 75
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 76
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 77
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 78
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review Topic
Explanation
Question 79
A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
Explanation
REFERENCES: Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56.
O’Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
Question 80
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of
Explanation
REFERENCES: Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
Hyman J, Breazeale NM, Altchek DW: Valgus instability of the elbow in athletes. Clin Sports Med 2001;20:11-24.
Question 81
A 40-year-old male patient sustains a bimalleolar ankle fracture and undergoes open reduction and internal fixation. Four months later, he returns for follow-up with mild ankle discomfort, and a radiograph is shown in Figure A. What is the most appropriate next step in treatment?

Explanation
Malunion of the fibula component of ankle fractures lead to tibiotalar instability and post-traumatic ankle arthritis. The distal fragment is usually shortened and externally rotated. The osteotomy can restore length and correct rotation. Markers for potential instability include: (1) asymmetry of the medial-lateral clear spaces, (2) talar tilt
>2mm, (3) talar subluxation, (4) abnormal talocrural angle (normal, 75-86deg).
Chu et al. opined that reconstruction for distal fibula malunions should include: (1) osteotomy, (2) +/- syndesmotic fixation and (3) autologous bone graft. They recommend: (1) low oblique osteotomy for fractures below the syndesmosis, (2) transverse osteotomy above the syndesmosis for high fractures (PER4) and low fractures with tibiofibular instability, (3) inspection of the tibiofibular joint through an anterolateral window to ensure anatomic reduction.
Weber et al. described a method of corrective lengthening osteotomy of the fibula in 23 cases. They described 3 criteria for assessing normal fibular length. Seventeen patients had good-excellent results, and 6 had fair-poor results (1 of these 6 needed ankle fusion).
Figure A is an AP radiograph of a distal fibula fracture fixed in a shortened position with lateral talar tilt and degenerative changes at the anterolateral tibiotalar joint. Illustration A is an anteroposterior radiograph after fibular osteotomy and correction
with medial distal tibial autograft to correct talar tilt and restore anatomic fibular length. Illustration B shows the normal talocrural angle. Illustration C shows the Weber-Simpson method of fibula lengthening used in Illustration A.
Incorrect Answers:
Question 82
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?
Explanation
REFERENCE: Gelehrter TD, Collins FS: Principles of Medical Genetics. Baltimore, Md, Williams & Wilkins, 1990, pp 27-45.
Question 83
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?
Explanation
REFERENCES: Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Lowell TD, Errico TJ, Eskenazi MS: Use of steroids after discectomy may predispose to infection. Spine 2000;25:516-519.
Question 84
The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?
Explanation
REFERENCES: Ebraheim NA, Lu J, Yang H, et al: The fibular incisure of the tibia on CT scan: A cadaver study. Foot Ankle Int 1998;19:318-321.
Ebraheim NA, Lu J, Yang H, et al: Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int 1997;18:693-698.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 85
A 29-year-old woman is seen in the emergency department with a 24-hour history of severe back and leg pain precipitated by weight-lifting. The patient reports bilateral leg pain and is unable to urinate. She has dense anesthesia in the perineal region on examination. A MRI scan is shown in Figure 38. The patient is taken to surgery urgently. What is her prognosis for recovery? Review Topic

Explanation
Question 86
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include
Explanation
REFERENCES: Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Aprin H, Bowen JR, MacEwen GD, et al: Spinal arthrodesis in patients with spinal muscle atrophy. J Bone Joint Surg Am 1982;64:1179-1187.
Question 87
A 32-year-old male hockey player who is right-hand dominant was checked from behind and landed with full force into the boards. In the emergency department he reports shortness of breath. Figure 113 shows a 2-D CT scan. What is the best initial treatment for this injury?
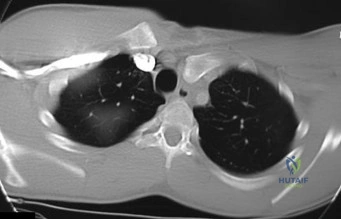
Explanation
Question 88
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
Question 89
A 23-year-old male is an unrestrained driver in a motor vehicle accident and sustains an unstable pelvic ring fracture. During fluoroscopic-aided fixation, a lateral sacral view is required for proper placement of which of the following fixation methods?

Explanation
Routt et al (1997) examined the sacral slope and sacral alar anatomy in cadavers and a series of patients. They determined that the pelvic outlet and lateral sacral plain films provide the best plain radiographic view of the sacral ala. They recommended routine usage of these views intraoperatively to guide screw placement.
Routt et al (2000) reported on the early complications of percutaneous placement of iliosacral screws for treatment of posterior pelvic ring disruptions. While technically challenging, this technique leads to less blood loss and lower rates of infection compared to traditional open techniques.
Barei et al described methods of anterior and posterior pelvic ring disruptions. They determined that successful placement depends on accurate closed reduction, excellent intraoperative fluoroscopic imaging, and detailed preoperative planning. Early treatment decreased hemorrhage, provides patient comfort, and allows early mobilization.
Question 90
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Explanation
85% of patients undergoing arthroscopy for various indications in one study. Internal impingement is defined as impingement of the posterior-superior rotator cuff between the humerus and posterior-superior glenoid rim. Symptomatic internal impingement is felt to be due to the frequency and magnitude of the impingement in throwers.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 252.
Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Question 91
A 6 year-old-boy falls from his bunk bed and suffers the injury seen in Figures A and B. Upon presentation to the emergency room he is noted to have a pink hand with brisk capillary refill, but no palpable pulses. After closed reduction in the operating room and the procedure seen in Figures C and D, he remains well perfused, pulses are still not palpable, but triphasic pulses can be heard on doppler examination. What is the most appropriate course of action? Review Topic

Explanation
Pediatric supracondylar humerus fractures presenting with vascular compromise can present a challenge for clinical decision making. If the hand lacks adequate perfusion on presentation it requires emergent treatment with closed reduction and pinning. If perfusion does not return, then surgical exploration of the antecubital fossa is required. Treatment of the "pink pulseless hand" remains controversial. If the hand is well perfused but lacks palpable pulses then it should be expeditiously reduced and pinned. If the hand remains well perfused with triphasic doppler signals, no additional intervention is required. Recommendations vary if the hand is perfused, and pulses cannot be detected on palpation or doppler.
If there is a normal neurovascular exam on presentation, but abnormal after reduction and pinning, then one must consider that the reduction may have entrapped the brachial artery. If hardware removal and fracture re-displacement does not improve pulses/perfusion of the hand, or if the fracture can not be reduced without diminishing perfusion, then open reduction is indicated to evaluate the brachial artery.
Shah et al. present their preferred algorithm for treatment of a pink pulseless hand. They note that even with good clinical perfusion there may be a vascular injury or entrapment of the brachial artery. Thus they recommend if the hand is pink with no palpable pulse, perform a doppler exam. Triphasic doppler signals allow for observation, while abnormal or non-detectable doppler signals require surgical exploration. If an AIN or median nerve injury is present, exploration is considered. A diagram of their algorithm can be seen in Illustration A.
Weller et al. present a retrospective review of 1297 supracondylar humerus fractures. They had 20 patients (1.5%) with a pink pulseless hand with good doppler signals following closed reduction and fixation. These patients were treated with close observation. One patient developed inadequate perfusion nine hours after reduction and required vascular repair. The remaining 19 patients regained palpable pulses prior to discharge or prior to the first follow-up visit. They recommend observation despite non-palpable pulses as long as other signs of perfusion (capillary refill and doppler signals) suggest the hand is well perfused.
Figures A and B are AP and lateral radiographs of a type III supracondylar humerus fracture. Figures B and C demonstrate this fracture following closed reduction and percutaneous pinning with three lateral pins. Illustration A is a flow chart of a proposed decision making algorithm for a pink pulseless hand as presented by Shah et al.
Incorrect Answers:
reduction and fixation. Answer 2- Changing the pattern of fixation would only be indicated if the current construct did not provide stable fixation of the fracture. Answer 3- Following reduction and fixation of a supracondylar humerus fracture the most appropriate dressing is rigid long arm immobilization in a splint or cast. If there is concern for edema or perfusion then a cast should be bivalved. Answer 5- Surgical exploration of the antecubital fossa would be indicated if the hand had inadequate perfusion, or if the fracture could not be reduced and fixed without causing a notable decrease in pulses or perfusion.
Question 92
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 93
Figure 70 is the radiograph of a 14-year-old girl with increasing posterior ankle pain, especially during pointe technique exercises. Nonsurgical measures such as modification, stretching, and injection have been unsuccessful. Which nerve is most vulnerable to injury during endoscopic excision of this lesion?
Explanation
The pathology is that of posterior ankle impingement, which is secondary to a symptomatic os trigonum. Endoscopic excision necessitates posteromedial and posterolateral ankle portals. Although plantar numbness has been described as a relatively common postsurgical complication, the neurovascular structure most commonly injured is the sural nerve.
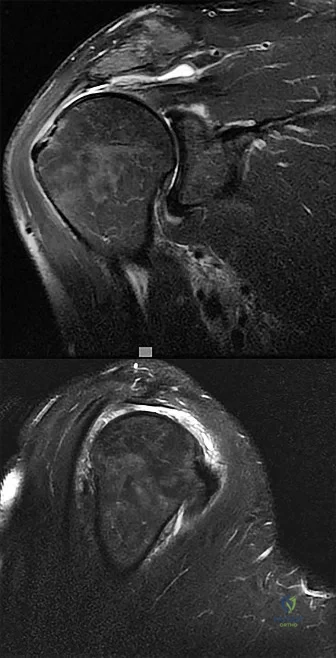
Question 94
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
REFERENCES: McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 95
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?

Explanation
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter. Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
Question 96
- A 17-year old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to actively raise his arm above his head. A radiograph is shown in Figure 1. Management should now include
Explanation
Selection (1) would not provide adequate fixation to promote healing. (2) Electrical stimulation would not be sufficient for the above reasons. (3) Resection of the distal clavicle would not be indicate for this case because it promote further instability of the clavicle and increasing the affected forces to the clavicle.
(5) Kirschner wire fixation with bone graft, the author stated would provide fixation, but they achieved better results with plate fixation and bone graft Question 6 -
A 75-year-old woman sustains a fracture below the level of a total hip prosthesis. Radiographs demonstrate loosening of the prosthetic component. Treatment should consist of
a cast brace
a spica cast
plate fixation
allograft strut fixation
long stem revision
The key to this question lies in the radiographic evidence of loosening of the prosthetic component. The long stem revision is clearly indicated in this case because of various factors, one decreases impingement of the loose stem against the lateral femoral cortex. A non-surgical approach in the elderly patient will only increase the many risk factors such as atelectasis, pneumonia, and thromboembolic disease.[Instructional Course 44 pg. 293-303]
Question 97
Figures 70a and 70b show the sagittal MRI scan and axial CT of a patient who has decreased range of motion in the cervical spine. In which of the following directions would the cervical motion be most significantly limited?
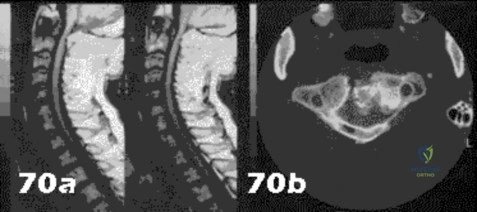
Explanation
Question 98
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?
Explanation
REFERENCES: Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.
Fernandez DL, Wolfe SW: Distal radius fractures, in Green DP, Hotchkiss RN, Pederson WC,
et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 693.
Question 99
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 100
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
