Orthopedic Board Review MCQs: Trauma, Arthroplasty & Foot Surgery | Part 245
Key Takeaway
This page presents Part 245 of a professional orthopedic surgery board review quiz. Designed for orthopedic surgeons and residents, it offers 100 high-yield, verified MCQs. Content mirrors OITE/AAOS exam format, covering key topics like Arthroplasty, Fracture, Hip, Knee, and Trauma, to ensure rigorous board certification preparation.
About This Board Review Set
This is Part 245 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 245
This module focuses heavily on: Arthroplasty, Foot, Fracture, Hip, Knee, Trauma.
Sample Questions from This Set
Sample Question 1: Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?...
Sample Question 2: A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of...
Sample Question 3: A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline Intern...
Sample Question 4: A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploratio...
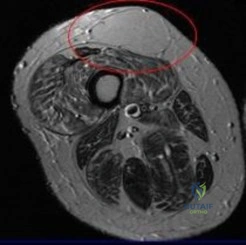
Sample Question 5: A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T 2 -weighted ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
Explanation
REFERENCES: Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Yang KH, Han DY, Park HW, et al: Fracture of the ipsilateral neck of the femur in shaft nailing: The role of CT in diagnosis. J Bone Joint Surg Br 1998;80:673-678.
Question 2
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
REFERENCE: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 3
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , include
Explanation
Question 4
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Explanation
REFERENCES: Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res
2003;408:86-91.
Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.
Question 5
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T 2 -weighted MRI scans. What is the most likely diagnosis?
Explanation
REFERENCE: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 2189-2216.
Question 6
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 7
An 84-year-old female community ambulator with a history of hypertension undergoes a right hip hemiarthroplasty for a femoral neck fracture. When performed in the post-operative period, the timed up and go (TUG) test may be used to predict which patient outcome?
Explanation
Hip fractures are a cause of significant functional decline for elderly patients. Many outcome tests have been developed to prediction function after hip fracture to manage patient expectations and to assist in rehabilitation planning. The TUG test objectively measures functional mobility and dynamic balance. The test is performed by timing the amount of seconds it requires for a patient to stand up from a chair, walk 10ft (3.05m), return to the chair, and sit.
Laflamme et al performed a prospective study evaluating the utility of the TUG test to predict functional outcomes in patients undergoing hip hemiarthroplasty for femoral neck fracture. The TUG scores were significantly higher at 4-days and 3-weeks postoperatively in patients requiring a walking aid compared with patients walking independently at two-years. Patients who performed the test in >58s at 4-days postoperatively had an eightfold greater risk of requiring an assistive device.
Springer et al prospectively analyzed the unipedal stance test (UPST) with eyes open and closed in healthy subjects to establish normative values for the test across age and gender groups. Performance on the test was found to be age-specific and not related to gender. The UPST is a method of quantifying static balance ability.
Kristensen et al studied the relative and absolute inter tester reliability of TUG in patients with hip fractures. The authors found that the TUG has a high interobserver reliability and an improvement by 6.2 seconds for a patient with a baseline of 20s indicates a change in functional mobility.
Video A shows the timed up and go test.
Incorrect Answers:
Question 8
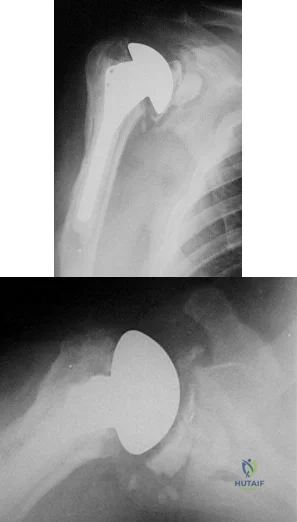
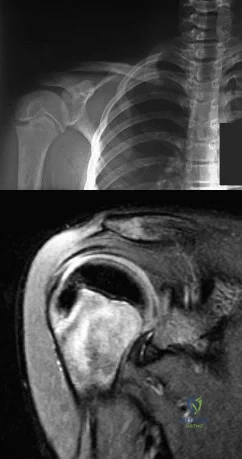
A 55-year-old man who underwent total shoulder arthroplasty 10 years ago recently reports an increase in shoulder pain. Laboratory studies consisting of a white blood cell count, erythrocyte sedimentation rate, and C-reactive protein are all negative, as is joint aspiration. Radiographs are shown in Figures 95a and 95b. If all intraoperative frozen sections are negative, what is the appropriate treatment during revision surgery to provide pain relief and improved function? Review Topic
Explanation
Question 9
Where is the most common site for tuberculosis (TB) spondylitis in children? Review Topic
Explanation
Question 10
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Explanation
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.
Question 11
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
REFERENCES: Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Apelqvist J, Castenfors J, Larson J, Stenstrom A, Agardh CD: Prognostic value of systolic ankle and toe blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 1989;12:373-378.
Question 12
A 3-year-old girl has had wrist pain, a fever, and has refused to move her right wrist for the past 10 days. She has an oral temperature of 102 degrees F (38.7 degree C). Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h, a WBC count of 11,000/mm 3 , and a left shift. AP and lateral radiographs are shown in Figures 57a and 57b. What is the most likely diagnosis?
Explanation
REFERENCES: Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 13
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
REFERENCES: Warren MP: Health issues for women athletes: Exercise-induced amenorrhea.
J Clin Endocrinol Metab 1999;84:1892-1896.
Rencken ML, Chesnut CH III, Drinkwater BL: Bone density at multiple skeletal sites in amenorrheic athletes. JAMA 1996;276:238-240.
Question 14
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain? Review Topic
Explanation
Question 15
A 71-year-old woman has a failed revision hip arthroplasty and is undergoing a re-revision hip arthroplasty. Her last hip surgery was 4 years ago with revision of the acetabular component. Radiographs show a well-fixed extensively porous-coated femoral component and a failed acetabular component with proximal and medial migration through the floor of the acetabulum. Preoperative laboratory studies reveal an erythrocyte sedimentation rate (ESR) of 70 mm/h (normal 0-29 mm/h), a C-reactive protein (CRP) of 23.3 (normal 0.2-8.0), and a negative hip aspiration. At the time of surgery, tissues look inflamed and a frozen section shows 20 WBC per high power field; however, a Gram stain is negative. What is the most appropriate action at this point?
Explanation
REFERENCES: Sanzen L, Sundberg M: Periprosthetic low-grade hip infections: Erythrocyte sedimentation rate and C-reactive protein in 23 cases. Acta Orthop Scand 1997;68:461-465.
Spangehl MJ, Hanssen AD, Osman DR: Diagnosis and treatment of the infected hip arthroplasty, in Morrey BF(edA)L:-MJoaidnetnaRCeopplyacement Arthroplasty, ed 3. Philadelphia, PA, Churchill Livingstone, 2003, pp 856-874. Question 71
A 79-year-old patient has a history of peripheral vascular disease and reports chronic knee pain. She has had coronary artery disease treated with angiography and stents on two occasions. Peripheral pulses are absent in both lower extremities, but the patient is disabled by advanced chronic degenerative arthritis in her right knee and would like to proceed with a total knee arthroplasty. The next most appropriate evaluation should include which of the following?
Ankle-brachial index of the affected lower extremity
Femoral popliteal angiography
Venous Dopplers of both lower extremities
MRI of the popliteal fossa
Radiographs to identify calcified plaques in the femoral artery
DISCUSSION: This question is designed to draw attention to the fact that peripheral vascular disease carries an increased risk of complications for the patient and should be carefully evaluated. The vascular surgeon will make the choice of revascularization or surgical clearance for knee reconstruction based on the initial results of the ankle-brachial index.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9:253-257.
Question 16
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Dearolf WW III, Betz RR, Vogel LC, Levin J, Clancy M, Steel HH: Scoliosis in pediatric spinal cord injured patients. J Pediatr Orthop 1990;10:214-218.
Question 17
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?
Explanation
REFERENCE: Gelehrter TD, Collins FS: Principles of Medical Genetics. Baltimore, Md, Williams & Wilkins, 1990, pp 27-45.
Question 18
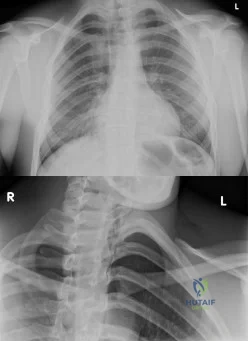
An 19-year-old male presents to the emergency room following an motor vehicle accident as an unrestrained driver. Examination reveals unilateral jugular vein engorgement. Chest and special view radiographs are seen in Figures A and B respectively. Following CT scan of the chest, the next step in management is Review Topic
Explanation
The SC joint can dislocate anteriorly or posteriorly. Posterior dislocations are first treated with closed reduction. If closed reduction fails, open reduction is indicated. Early complications of posterior SC dislocation include pneumothorax, laceration/erosion/occlusion of great vessels, esophageal rupture and brachial plexus compression. Late complications include tracheoesophageal fistula, stridor and dysphagia.
Groh et al. reviewed traumatic SC injuries. Reduction maneuvers in posterior SC dislocation include: (1) traction on the arm and slowly bringing it into extension, (2) traction with the arm in adduction and posterior pressure applied to the shoulder, and
(3) pulling anteriorly on a towel clip encircling the medial clavicle. Chronic instability after posterior SC dislocations can be managed with figure-of-8 semitendinosus graft or medial clavicle resection and reattachment of the clavicle to the first rib with dacron tape.
Glass et al. performed a systematic review on SC dislocations. They found mediastinal compression occurred 30% of the time with posterior dislocations.
Figures A and B are radiographs demonstrating asymmetry of the SC joints, characteristic of a right posterior SC dislocation (Figure B is not a serendipity view). Illustration A demonstrates how in POSTERIOR dislocation, the clavicle appears INFERIOR, and in ANTERIOR dislocation, the clavicle appears SUPERIOR on a serendipity view radiograph respectively. Illustration B shows the imaging technique for a serendipity view radiograph. Illustration C is a reconstructed CT image of the patient showing left posterior SC dislocation.
Incorrect Answers:
Question 19
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 20
Up to what time frame are the risks minimized in anterior revision disk replacement surgery?
Explanation
REFERENCE: Tortolani JP, McAfee PC, Saiedy S: Failures of lumbar disc replacement. Sem Spine Surg 2006;18:78-86.
Question 21
- A 32-year-old man has swelling of the knee as a result of falling with the knee flexed and his foot in plantar flexion. A Lachman’s test reveals an apparent increase in anterior translation. Passive external tibial rotation at 30 degrees and 90 degrees is equal to the contralateral side, and the quadriceps active test is positive on the affected side. The neurovascular examination is normal. Treatment should consist of
Explanation
Question 22
A complication unique to computer navigation of total knee arthroplasty (TKA) is
Explanation
Threaded pins are frequently inserted into the femoral shaft and tibial shafts or proximal tibia to attach arrays for tracking devices. There have been case reports of fractures propagating through the pin tracks, which is a complication unique to computer navigation. Intercondylar fractures can occur following posterior stabilized TKA. Vascular injury, ligament disruption, and nerve palsy are rare complications following TKA performed with or without computer navigation.

CLINICAL SITUATION FOR QUESTIONS 111 THROUGH 113
Figure 111 is the anteroposterior radiograph of a 79-year-old woman with a presurgical diagnosis of osteonecrosis who sustained a periprosthetic tibia fracture following her total knee arthroplasty (TKA).
Question 23
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
Explanation
Question 24
What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
Explanation
Question 25
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?
Explanation
REFERENCES: McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
Hodges SD, Humphreys SC, Eck JC, Covington LA: The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations: A modified technique and outcomes analysis of 25 patients. Spine 1999;24:1243-1246.
Question 26
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?
Explanation
REFERENCE: Norris TR: Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, p 342.
Question 27
A 65-year-old man has a painful and often audible crepitus after undergoing a total knee arthroplasty 8 months ago. His symptoms are reproduced with active extension of about 30°. Examination reveals no effusion or localized tenderness, a stable knee, and a range of motion of 5° to 120°. Radiographs are shown in Figures 37a and 37b. Management should consist of
Explanation
REFERENCES: Beight JL, Yao B, Hozack WJ, Hearn SL, Booth RE Jr: The patellar “clunk” syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142.
Lintner DM, Bocell JR, Tullos HS: Arthroscopic treatment of intra-articular fibrous bands after total knee arthroplasty: A follow-up note. Clin Orthop 1994;309:230-233.
Question 28
What is the most frequent complication of percutaneous repair of an acute Achilles tendon rupture?
Explanation
REFERENCES: Aracil J, Pina A, Lozano JA, et al: Percutaneous suture of Achilles tendon ruptures. Foot Ankle 1992;13:350-351.
Sutherland A, Maffulli N: A modified technique of percutaneous repair of the ruptured Achilles tendon. Oper Orthop Traumatol 1998;10:50-58.
Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am
2002;84:161-170.
Question 29
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi Y: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7;223-227.
Question 30
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Explanation
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 31
Figure 177 is an intra-articular photograph taken while viewing from the anterior superior portal during arthroscopy of a right shoulder. Which of the following findings identified at the time of surgery would be the most predictive for recurrence following arthroscopic repair of the demonstrated pathology? Review Topic

Explanation
Question 32
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
Question 33
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 34
A 47-year-old man is seen in consultation in the ICU after being admitted and treated emergently for a dissecting aortic aneurysm. Current examination reveals generalized weakness of the lower extremities with a significant decrease in pain and temperature sensation from approximately the waist down. Proprioception is maintained. What is the most likely diagnosis at this time? Review Topic
Explanation
Question 35
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
Explanation
REFERENCES: Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642
Question 36
Anterior penetration of an iliosacral screw through the sacral ala would most likely lead to weakness of which of the following movements?

Explanation
The referenced study by Routt et al reviewed 177 patients with pelvic ring injuries treated with these screws and found that quality triplanar imaging decreased intraoperative and postoperative complications. They also recommend supplemental fixation of iliosacral screws with posterior plating in noncompliant patients.
Question 37
What is the most likely explanation for the change between the initial intraoperative radiograph (Figure 11a) and the radiograph taken 4 weeks after surgery (Figure 11b) in an 87-year-old man who underwent primary hip replacement for osteoarthritis?

Explanation
The image demonstrates subsidence of the femoral implant. The implant subsided because it did not have good initial stability. The tapered femoral implant was placed after initial preparation for an anatomic femoral stem. A limited, nondisplaced femoral neck fracture was encountered during the procedure and treated. Two advantages of tapered stems are the efficient transfer of stress to the proximal femur and the ability to accommodate some subsidence to achieve enhanced stability. Although subsidence of a tapered stem to a more stable position can produce a good result, quality of metaphyseal bone should be considered. Attention to surgical technique remains important to optimize component stability for biological fixation.
RECOMMENDED READINGS
Savory CG, Hamilton WG, Engh CA Sr, Della Valle CJ, Rosenberg AG, Galante JO. 15 Hip designs. In: Barrack RL, Booth RE Jr, Lonner JH, McCarthy JC, Mont MA, Rubash HE, eds. Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:345-368.
Blaha JD, Borus TA. Press-fit femoral components. In: Callaghan J, Rosenberg A, and Rubash H, eds The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:1036-1043.
Question 38
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 39
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
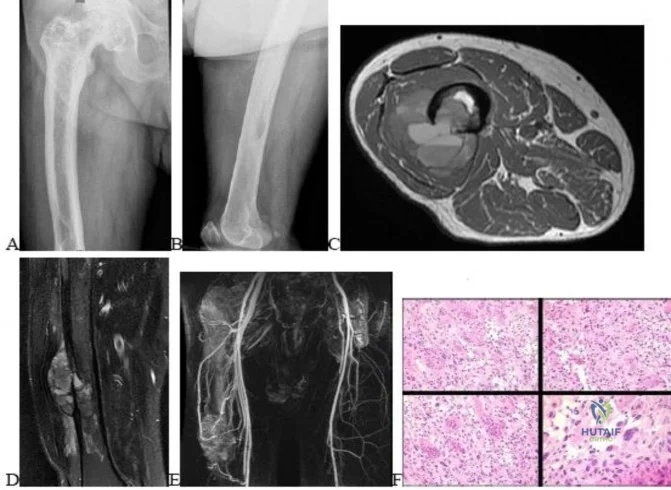
Explanation
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.


Question 40
A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination reveals that the patellae cannot be brought into a reduced position. Management should consist of
Explanation
REFERENCES: Dugdale TW, Renshaw TS: Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-413.
Mendez AA, Keret D, MacEwen GD: Treatment of patellofemoral instability in Down’s syndrome. Clin Orthop 1988;234:148-158.
Question 41
- Which of the following injuries is most commonly associated with a fracture of the scapular body?
Explanation
Question 42
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 43
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 44
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?
Explanation
REFERENCE: Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2002;84:873-874.
Question 45
What is the most common malignant tumor of the foot?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 11-26.
Bos GD, Ester RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 46
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 3-23.
Question 47
In Dupuytren’s disease, the retrovascular cord typically displaces the radial proper digital nerve of the ring finger in what direction?
Explanation
REFERENCE: Rayan GM: Palmar fascial complex anatomy and pathology in Dupuytren’s disease. Hand Clin 1999;15:73-86.
Question 48
Which of the following best describes the legal definition of standard of care?
Explanation
REFERENCES: Lewis MH, Gohagan JK, Merenstein DJ: The locality rule and the physician’s dilemma: Local medical practices vs the national standard of care. JAMA 2007;297:2633-2637.
AAOS Expert Witness Program, www3.aaos.org/member/expwit/expertwitaess.cfm
Question 49
- The pharmacologic action of botulinum-A toxin can be best described as
Explanation
Question 50
- Which of the following medicolegal relationships between an attending surgeon and a resident assistant applies when a patient files a malpractice suit relating to surgical complications following a total knee arthroplasty?
Explanation
Question 51
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35°. Neurologic examination is normal. Management should consist of
Explanation
REFERENCES: Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767.
Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Farley FA, Song KM, Birch JG, Browne R: Syringomyelia and scoliosis in children. J Pediatr Orthop 1995;15:187-192.
Question 52
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 53
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Sim FH: Metastatic bone disease of the pelvis and femur. Instr Course Lect 1992;41:317-327.
Question 54
An otherwise healthy 75-year-old man has a painful mass in the popliteal fossa of his right knee. A lateral radiograph of the knee, a CT scan of the distal femur, and a histopathologic specimen are shown in Figures 13a through 13c. Management should consist of
Explanation
REFERENCES: Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma: A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Campanacci M: Bone and Soft Tissue Tumors. New York, NY, Springer-Verlag, 1990, pp 433-454.
Question 55
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
REFERENCES: Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238.
Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
Lonstein JE, Denis F, Perra JH, et al: Complications associated with pedicle screws. J Bone Joint Surg Am 1999;81:1519-1528.
Question 56
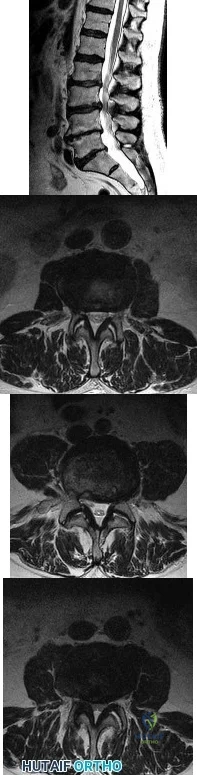
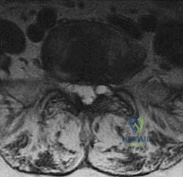
A 78-year-old man has a history of worsening bilateral calf pain with activity. MRI scans are shown in Figures 31a through 31d. His symptoms are not improved with forward flexion of the lumbar spine. His lower extremity pain is relieved when he sits or ceases activity. Which of the following tests would be most helpful in establishing a diagnosis? Review Topic
Explanation
Decreased range of motion and hip joint pain, especially in internal rotation and abduction, are common findings in patients with degenerative arthritis of the hip. While post-myelography CT has been found superior to MRI as a single study for the preoperative planning of decompression for lumbar spinal stenosis, it will not assist in differentiating vascular from neurogenic claudication.
Question 57
A 64-year-old man who underwent an L4-5 decompression approximately 1 year ago reported relief of his claudicatory leg pain initially, but he now has increasing low back pain and recurrent neurogenic claudication despite nonsurgical management. Radiographs show new asymmetric collapse and spondylolisthesis at the decompressed segment, and MRI scans show lateral recess stenosis. The next most appropriate step in management should consist of
Explanation
REFERENCES: Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Hansraj KK, O’Leary PF, Cammisa FP Jr, et al: Decompression, fusion, and instrumentation surgery for complex lumbar spinal stenosis. Clin Orthop 2001;384:18-25.
Question 58
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
REFERENCES: Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 689-691.
Question 59
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Explanation
REFERENCES: Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Lee D, Ferlic R, Neviaser R: Hand infections, in Berger R, Weiss AP (eds): Hand Surgery. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 1784-1785.
Question 60
Commotio cordis is best treated with
Explanation
REFERENCES: McCrory P: Commotio cordis. Br J Sports Med 2002;36:236-237.
Boden BP, Tacchetti R, Mueller FO: Catastrophic injuries in high school and college baseball players. Am J Sports Med 2004;32:1189-1196.
Question 61
Which of the following zones of articular cartilage has the highest concentration of proteoglycans?
Explanation
Question 62
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
REFERENCES: Amaral JF: Thoracoabdominal injuries in the athlete. Clin Sports Med 1997;16:739-753.
Perron AD: Chest pain in athletes. Clin Sports Med 2003;22:37-50.
Question 63
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
REFERENCE: Gross AE, Allan DG, Catre M, et al: Bone grafts in hip replacement surgery: The pelvic side. Orthop Clin North Am 1993;24:679-695.
Question 64
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?
Explanation
REFERENCES: Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Mäenpää H, Lehto MU, Belt EA: What went wrong in triple arthrodesis? An analysis of failures in 21 patients. Clin Orthop Relat Res 2001;391:218-223.
Question 65
..A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized at the fracture site. Appropriate imaging studies are performed and show no other lesions. What is the next treatment step?
Explanation
Question 66
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time? Review Topic
Explanation
point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.
(SBQ12SP.20) Amphotericin B is most appropriate for the treatment of which type of spine infection? Review Topic
Fungal osteomyelitis
Bacterial osteomyelitis with a gram-positive organism
Bacterial osteomyelitis with a gram-negative organism
Tuberculous osteomyelitis
Viral meningomyelitis
Amphotericin B would be most appropriate for the treatment of fungal infections of the spine.
Amphotericin B is a broad-spectrum anti-fungal medication. It is commonly used as the first-line agent for treatment of fungal infections of the spine. The most common fungi involving the spine include cryptococcus, candida, and aspergillus. The indications for débridement and stabilization with spinal fusion, includes resistance to antibiotic therapy, spinal instability, and/or neurologic deficits.
Kim et al. reviewed fungal infections of the spine. They comment that fungus infections are most commonly spread by hematogenous or direct spread. Access to the vascular system may include intravenous lines, during implantation of prosthetic devices, or during surgery.
Frazier et al. retrospectively reviewed 11 patients with fungal osteomyelitis of the spine. Nine of the patients were immunocompromised secondary to diabetes mellitus, corticosteroid use, chemotherapy for a tumor, or malnutrition. All were treated with anti-fungal medication. 10 of 11 patients were also treated with surgical debridement. Paralysis secondary to the spine infection developed in eight patients. After an average of 6.3 years of follow-up, the infection had resolved in all nine surviving patients.
Illustration A shows the mechanism of action of Amphotericin. Illustration B shows T1- (Image A and B) and T2-weighted (Image C) images of the lower thoracic and lumbar spine. There are hypointense signals within the T12 and L1 vertebral bodies (Images A and B) indicative of fungal osteomyelitis.
IncorrectAnswers:
Question 67
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 68
A B C Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with

Explanation
MIS TLIF involves a steep learning curve but is associated with similar longterm outcomes as open TLIF, arguably comparable or possibly lower complication rates, and equivalent fusion rates. The major distinguishing feature comparing open to minimally invasive surgery for this and other spinal diagnoses has been shorter hospital stays.
RECOMMENDED READINGS
Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. View
Abstract at PubMed
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
Question 69
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T 1 - and T 2 -weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?
Explanation
REFERENCES: Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21.
Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing’s sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Lazar A, Abruzzo LV, Pollock RE, et al: Molecular diagnosis of sarcomas: Chromosomal translocations in sarcomas. Arch Path Lab Med 2006;130:1199-1207.
Question 70
A 20-year-old basketball player sustains a knee injury during a game and is seen in the orthopaedic clinic 3 days after injury. Examination reveals a positive Lachman, pivot shift, joint line tenderness, and moderate effusion. Which of the following tissue injuries is most likely causing the jointline tenderness?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 201.
Greis PE, Bardana DD, Holmstrom MC, et al: Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002;10:168-176.
Duncan JB, Hunter R, Purnell M, et al: Meniscal injuries associated with acute anterior cruciate ligament tears in alpine skiers. Am J Sports Med 1995;23:170-172.
Question 71
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
REFERENCES: Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop 2001;390:17-30.
Question 72
A 35-year-old man has a brachial plexus injury affecting the lateral cord. He partially improves with observation and now has complete return of median nerve function and pectoral muscle function. What nerve transfer is most likely to restore the motor function he is lacking?
Explanation
The lateral cord of the brachial plexus gives off the lateral pectoral nerve, the musculocutaneous nerve, and then contributes to the median nerve. The patient has had recovery of function of these components except for the musculocutaneous nerve. The musculocutaneous nerve innervates the biceps and the brachialis, which provide elbow flexion. To restore motor function, a nerve transfer would have to provide reinnervation of the biceps and brachialis.
Question 73
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 74
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include
Explanation
a 7-day course of broad-spectrum antibiotics. Fragment removal is not indicated.
REFERENCES: Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Velmahoos GC, Demetriades D: Gunshot wounds of the spine: Should retained bullets be removed to prevent infection? Ann R Coll Surg Engl 1976;94:85-87.
Question 75
A 6-year-old boy had a 4-day history of worsening atraumatic right thigh and knee pain. He was seen in the emergency department, where he had a temperature of 39.1°C. Laboratory studies reveal a white blood cell count of 15000 /µL (reference range, 4500-11000 /µL). He had a small knee effusion with range of motion 0 to 90 degrees and a swollen, painful, hot distal thigh. The knee effusion was aspirated, revealing a white blood cell (WBC) count of 2000 with negative gram stain (reference range < 2000 WBC/mL). The boy was admitted to the pediatric medical service and intravenous (IV) antibiotics were initiated. The next day, MR imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?
Explanation
The MRI scans show an advanced distal femur osteomyelitis with a substantial subperiosteal abscess. This necessitates open drainage; by definition, an abscess is avascular, so antibiotics cannot be delivered to the area without drainage.

CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
Question 76
After the athlete undergoes the appropriate treatment of the postsurgical complication and recovers without further incident, which muscle most likely will be last to experience return of function?
Explanation
This patient sustained an eccentric contracture (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest
potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed.
The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared to the 2-incision technique. The most troubling complication for most surgeons is the development of a PIN palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABC nerve injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button.
Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The EIP is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC followed by the ECU, EDQ, and, finally, the EIP.
RESPONSES FOR QUESTIONS 26 THROUGH 27
Anterior tibial artery
Posterior tibial artery
Superficial peroneal nerve
Deep peroneal nerve
Match the neurovascular structure at risk (listed above) with the compartment undergoing fasciotomy (listed below).
Question 77
Which of the following is an FDA approved adjunctive treatment for an acute open tibia fracture being treated with an intramedullary nail?
Explanation
Open tibial shaft fractures can present many treatment challenges. Although its use remains somewhat controversial, rhBMP-2 has been shown to have many positive effects when used to treat acute open tibia fractures. These benefits include accelerated early fracture healing, decreased rates of hardware failure, decreased need for subsequent bone grafting procedures, and decreased infection rates. rhBMP-2 does have FDA approval specifically for use in open tibia fractures being treated with an intramedullary nail.
Alt et al. present a comparison of patients with Grade III open tibia fractures treated
with un-reamed nails with or without rhBMP-2. They found significant decreases in need for secondary interventions such as bone grafting or nail exchange. Mean time to fracture healing was less in the rhBMP-2 group, but this difference was not statistically significant.
Govender et al. present a prospective randomized study of 450 patients with open tibia fractures treated with an intramedullary nail with or without rhBMP-2. They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Wei et al. provide a meta analysis regarding use of rhBMP-2 in open tibia fractures. Due to decreased rates of secondary interventions they estimated a net savings of
$6,000 per case when rh-BMP2 was used. They found no significant difference in rates of infection, postoperative pain, hardware failure, or fracture healing at 20 weeks.
Incorrect answers:
Question 78
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
Explanation
REFERENCES: O’Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
Warner JP: The gross anatomy of the joint surfaces, ligaments, labrum and capsule, in Matsen FA, Fu FF, Hawkins RJ (eds): The Shoulder: A Balance of Mobility and Stability. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 7-28.
Question 79
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
REFERENCES: Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
L’Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Question 80
A 50-year-old pipefitter falls from a ladder at work and dislocates his non-dominant shoulder. His MRI scan shows supraspinatus and infraspinatus tears with retraction to the glenoid. He cannot actively raise his arm away from his side. He denies prior shoulder symptoms before his fall. Three weeks of physical therapy have failed to improve his function. Which factor has been demonstrated to result in a poor clinical outcome following surgical intervention?
Explanation
Question 81
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 82
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5 to 110 degrees, and his mechanical axis is 18 degrees of valgus. What is the most appropriate surgical treatment for this patient?
Explanation
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15-degree valgus mechanical axis and range of motion of at least 15 to 90 degrees. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
RESPONSES FOR QUESTIONS 138 THROUGH 141
Acute periprosthetic infection
Chronic periprosthetic infection
Joint dislocation
Periprosthetic fracture
Pseudotumor
Femoral nerve palsy
Sciatic nerve palsy
Aseptic prosthetic loosening
Select the total hip arthroplasty (THA) complication listed above that most commonly is associated with the clinical scenario described below.
Question 83
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of

Explanation
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an infection, and revascularization is not indicated.
Question 84
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?
Explanation
REFERENCE: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 265-266.
Question 85
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?
Explanation
REFERENCES: De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607.
Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 86
What is the most common cause of rotator cuff injury in high school athletes?
Explanation
REFERENCES: Wilkins KE: Shoulder injuries: Epidemiology, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 175-182.
Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannnotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 3-30.
Question 87
Which of the following medications has been shown to improve skeletal muscle regeneration and decrease fibrosis following muscle injury in an animal model? Review Topic
Explanation
Skeletal muscle undergoes a natural process of healing and regeneration after injury. The formation of fibrous tissue in place of normal muscle is also part of this process. However, fibrous tissue in place of muscle can predispose the area to re-injury and impaired function. Administration of angiotensin II receptor blockade medications (e.g. losartan) after skeletal muscle injury has been shown to decrease the apoptotic cascade response and the formation of fibrous tissue. The mechanism of benefit is thought to be associated with blockade of insulin-like growth factor.
Terada et al. looked at the affect of platelet-rich plasma (PRP) and losartan on muscle healing after contusion injuries. They showed that PRP plus losartan combination
therapy improved overall skeletal muscle healing by enhancing angiogenesis and follistatin expression as well as reducing the expression of phosphorylated Smad2/3 and the development of fibrosis.
Bedair et al. used a rat model to investigate the effect of angiotensin receptor blockade on muscle fibrosis after injury. They found that angiotensin receptor blockade therapy significantly reduced fibrosis and led to an increase in the number of regenerating myofibers in acutely injured skeletal muscle.
Incorrect
Question 88
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
REFERENCES: Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Question 89
A coach of three football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on one team are different from those on the other teams?
Explanation
Question 90
What is the most likely contributory factor to this patient's problem?
Explanation
Proximal humeral epiphysiolysis (little leaguer’s shoulder) is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Factors that contribute to the condition include excessive throwing, improper throwing mechanics, and muscle-tendon imbalance. Radiographic findings typically are normal but may indicate subtle widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms. Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to throwing is implemented until the patient’s condition returns to baseline. This protocol has a long-term success rate exceeding 90%. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The most common cause of this condition is overuse, as is seen in pitchers who throw all year. Internal rotation deficit and internal impingement is typically a finding in older athletes without open physes. This patient had no evidence of rotation deficit upon examination, making this diagnosis unlikely.
Question 91
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
REFERENCES: Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Aronow MS, Diaz-Doran V, Sullivan RJ, et al: The effect of triceps surae contracture force on plantar foot pressure distribution. Foot Ankle Int 2006;27:43-52.
Question 92
The most appropriate surgical approach includes which of the following? Review Topic

Explanation
Question 93
What is the most common causative bacteria in septic arthritis in children? Review Topic
Explanation
Question 94
The essential lesion in recurrent or posterior instability following simple dislocation of the elbow typically involves which of the following structures?
Explanation
Question 95
Which of the following is the most sensitive parameter to detect the increased inflammatory response seen with both postoperative infection and the use of instrumentation in spinal surgery?

Explanation
DISCUSSION: The most sensitive parameter to detect inflammation elicited by implants and infection is the C-reactive protein (CRP).
CRP is an acute phase reactant that increases sharply immediately after surgery within 6 hours after tissue damage. CRP then peaks 2-3 days later and returns to normal levels 5-21 days after the inciting event. In contrast, ESR reaches its peak on days 4-11, then remains elevated for a prolonged period of time.
Takahashi et al performed a Level 3 study of patients who had undergone spinal surgery with and without instrumentation, with a primary outcome of infection. They concluded that renewed elevation of C-reactive protein, white blood cell count, and body temperature after postoperative days 4 to 7 may be a key indicator of postoperative infection.
Question 96
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Torg J, Pavlov H, Cooley LH, et al: Stress fractures of the tarsal navicular: A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64:700-712.
Question 97
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of
Explanation
REFERENCES: Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123.
Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Kuo RS, Tejwani NC, Digiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 98
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
REFERENCES: Carson WG Jr, Gasser SI: Little Leaguer’s shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 99
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 100
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
REFERENCES: Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 51.
