Orthopedic Board Review MCQs: Cartilage, Elbow & Tumor | Part 101

Key Takeaway
This page offers Part 101 of an interactive orthopedic surgery board review quiz. Featuring 100 high-yield, verified MCQs on Cartilage, Elbow, and Tumor, it is designed for orthopedic surgeons and residents preparing for OITE and AAOS certification exams. Utilize Study or Exam modes for comprehensive board preparation and clinical understanding.
About This Board Review Set
This is Part 101 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 101
This module focuses heavily on: Cartilage, Elbow, Tumor.
Sample Questions from This Set
Sample Question 1: A 23-year-old male reports a firm, immobile mass behind his tibia that creates pain when he walks long distances or uses stairs. He reports no night pain or constitutional symptoms. His WBC, LDH, and Alkaline phosphatase are normal. Radiogr...
Sample Question 2: Which of the following techniques is most commonly used to classify tissue type in soft-tissue tumors?...
Sample Question 3: -What is the most appropriate initial treatment for her condition?...
Sample Question 4: Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?...
Sample Question 5: A 43-year-old man who works as a plumber has a painful stiff elbow in his dominant arm. He notes that while he recalls no single event of injury, he thinks the many years of pulling wrenches and soldering pipes have resulted in his problem....
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
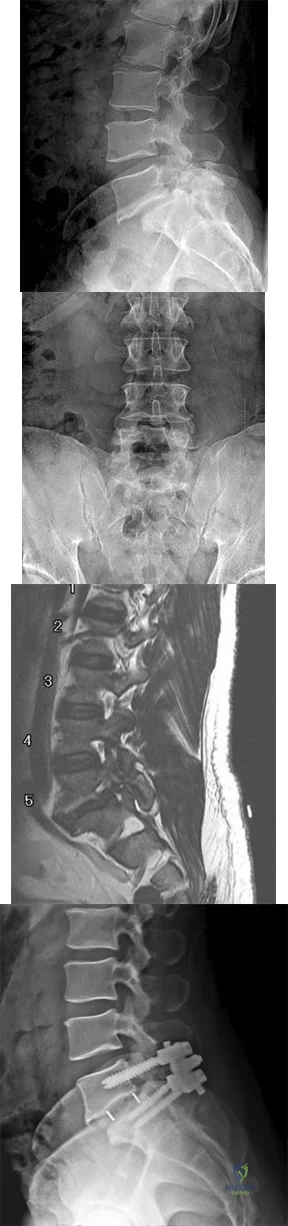
A 23-year-old male reports a firm, immobile mass behind his tibia that creates pain when he walks long distances or uses stairs. He reports no night pain or constitutional symptoms. His WBC, LDH, and Alkaline phosphatase are normal. Radiographs are shown in Figures A and B. A T1 MRI is shown in Figure C. What is the next most appropriate step in management?

Explanation
Osteochondromas are benign lesions, and therefore treatment is dictated by the severity of the symptoms they produce, the skeletal maturity of the patient, and concern for malignant transformation. If the symptoms are tolerable, excision is delayed until patient reaches skeletal maturity or for as long as possible due to increased risk of recurrence. In a more symptomatic skeletally immature patient, marginal excision is performed. Depending on the location, an additional concern for these patients is periarticular deformity or limb length inequality after removal. In skeletally mature patients, marginal excision is the treatment with very low risk of local recurrence. Concern for malignant transformation, found in less than 1% of patients, is an indication for wide resection.
Gitelis et al. discussed osteochondromas addressing general characteristics, presentation, and management options. Nonsurgical management is used in asymptomatic patients with no concern for malignant degeneration. Surgical excision is indicated in patients who have pain, interference with joint function, or impingement of the mass on neurovascular structures. These symptomatic tumors are usually treated with marginal resection, but there is the option of intralesional excision in skeletally mature patients. If there is concern for malignant degeneration, wide resection is performed for all patients.
Figure A and B are radiographs of an osteochondroma in which the cortex of the lesion and the underlying cortex are continuous. Figure C is a sagittal cut of a T1-weighted MRI image showing the high signal features of fatty marrow extending from the medullary canal of the tibia up into the bony stock of the pedunculated osteochondroma.
Incorrect Answers:
A 51-year-old female with known metastatic breast cancer presents with acute right thigh pain and inability to bear weight. A radiograph is shown in Figure A. A biopsy is performed that confirms metastatic breast cancer. What is the next step in management?
Local radiation therapy
Intramedullary nailing only
Intramedullary nailing and chemotherapy
Intramedullary nailing, radiation therapy to the tumor site, and chemotherapy
Intramedullary nailing, radiation therapy to the entire femur, and chemotherapy
This patient is presenting with biopsy proven metastatic breast cancer and a pathological fracture. The treatment in this situation is intramedullary nailing with postoperative radiation therapy to the entire femur and chemotherapy.
Due to the process of placing the intramedullary nail, the treating surgeon contaminates the ENTIRE femur with breast cancer. The surrounding area is already contaminated with tumor cells from the fracture, however. While the intramedullary nail will stabilize the pathological fracture, it does nothing to control the local progression of breast cancer in this patient's leg. Local radiotherapy will not only improve the local control of disease but it will palliate the patient's cancer related pain.
Weber et al review bone metastasis to the femur and propose valuable treatment pearls for clinical decision making and the biology which prevents cancer bearing bones to heal properly despite appropriate mechanical stabilization.
Swanson et al review the role of the orthopaedic surgeon in evaluating and treating metastatic bone disease, paying close attention to the necessity to obtain a tissue diagnosis in the event of presumed metastatic disease PRIOR to proceeding with any treatment plan.
All of the following locations are common sites for giant cell tumor of bone to occur EXCEPT?
Posterior elements of the spine
Distal femur
Sacrum
Distal radius
Proximal tibia
As reviewed by Robert Turcotte in the referenced article, the most common locations for giant cell tumor of bone to occur are about the distal femur/proximal tibia, distal radius, and the sacrum. The spine is an uncommon location for giant cell tumors, and when they occur, they usually occur in the vertebral body, not the posterior elements. In the axial skeleton, the sacrum is a common location for giant cell tumor of bone. Outside of the sacrum, giant
cell tumor of bone is characteristically an epiphyseal/metaphyseal lesion. As discussed in the in vitro study by Gortzak et al, treatment of giant cell tumor of bone includes aggressive intralesional curettage augmented with adjuvant treatment like hydrogen peroxide, argon beam, liquid nitrogen, or phenol. Due to the morbidity of the surgical treatment, and the less than perfect long term outcome, adjuvant therapy with an antibody against RANKL called denosumab is currently being investigated in multiple centers across North America as described by Thomas et al in their phase 2 study. Denosumab inhibits osteoclast mediated osteolysis and treatment is associated with improved bone stock and sclerosis of the GCT lesions. While denosumab doesn't obviate the need for surgical excision, the resulting surgical procedure is less extensive and early data may suggest a decreased risk of local recurrence.
While giant cell tumor of bone is a benign condition, there is a small chance for pulmonary seeding of giant cell metastases. This occurs in somewhere between 2-5% of patients with primary giant cells and occurs more often in patients with recurrent disease.
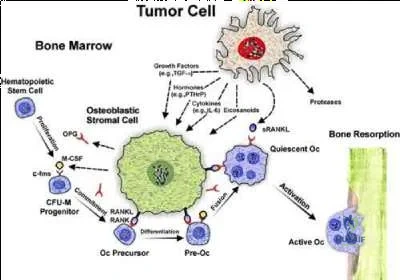
A 59-year-old female presents with a metastatic spinal tumor and has a lytic lesion in the T12 vertebral body. The process of bone resorption in her lytic lesion is mediated by
Direct resorption of bone by tumor cells
Neoangiogenesis of the vertebral body
Macrophage-mediated bony destruction
Tumor induced activation of osteoclasts
Necrosis of the vertebral body
Metastatic tumors are thought to induce osteolysis not by direct resorption of bone (remember only osteoclasts can destroy bone) but rather by releasing osteoclastogenic inflammatory cytokines.
Okeefe et al present a Level 5 review that states TNFa, RANKL, IL-1b, and IL-6 are osteoclastogenic inflammatory cytokins. Among these, RANKL is the most
notable and important cytokine. It binds to RANK, a surface receptor, and initiates osteoclastogenesis.
Goltzman presents a Level 5 review of the skeletal manifestations of malignancy. They report that by binding and neutralizing RANKL, osteoprotegrin (OPG) can diminish the production of functioning osteoclasts, and this factor has been shown to block bone resorption that is associated with malignancy.
Illustration A is a schematic representation of tumor-cell induced osteolysis.
Patients with which of the following conditions have the highest incidence of malignant tumor?
Single enchondroma
Single osteochondroma
Multiple hereditary exostosis
Ollier's disease
Maffucci's syndrome
Of all the listed cartilage lesions, patients with Maffucci's syndrome have the highest risk of malignant tumor - estimated to be 100% over the lifetime of the patient.
Single enchondromas and osteochondromas have a 1% risk of malignant transformation. Multiple hereditary exostosis patients have approximately a 10 % life time risk of malignant transformation. Ollier's disease is one of multiple enchondromas and carries a 30% risk of malignant transformation ( Illustration A) while Maffucci's syndrome is multiple enchondromas with hemangiomas (Illustration B). Maffucci's is also associated with a large number of other malignancies—particularly, pancreatic and hepatic adenocarcinoma, mesenchymal ovarian tumors, brain tumors such as glioma and astrocytoma, and various kinds of sarcomas.
While patients with enchondromas and osteochondromas do have a slight elevation in the risk for malignant transformation, it is not as great as those patients with Ollier's disease or Maffucci's syndrome. Distinguishing enchondromas from low grade chondrosarcomas can be done by looking at radiograph features such as the degree of endosteal scalloping on radiographs and the clinical presence of pain, both associated with low grade chondrosarcomas.
Ryzewicz et al review the diagnosis, pathology, and recommended treatment for patients with benign cartilage lesions. They recommend periodic follow-up even for the most benign lesions to track for malignant degeneration.

A 44-year-old male reports a mass at his right iliac crest that bothers him when he wears a belt. He denies constitutional symptoms
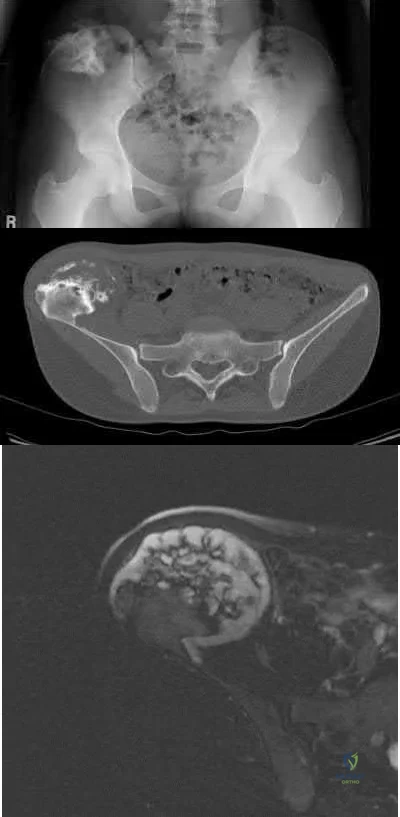
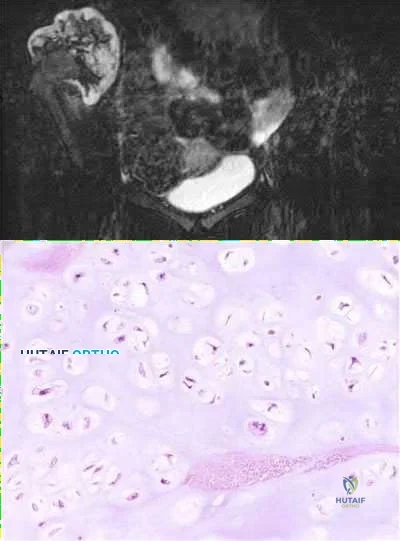
and has no bowel function disturbance. His ESR and CRP are normal. His chest CT is normal. Pelvis radiograph, CT, and MRI images are shown in Figures A-D. A biopsy is performed with histology shown in Figure E. What is the next most appropriate step in management?
Repeat CT scan in 3 months
Neoadjuvant radiation followed by marginal surgical resection followed by adjuvant chemotherapy 3 . Marginal surgical resection
Wide surgical resection
Neoadjuvant chemotherapy followed by marginal surgical resection followed by adjuvant chemotherapy
The history, imaging, and biopsy is consistent with chondrosarcoma and is appropriately treated with wide surgical resection. Chondrosarcoma is a malignant tumor of cartilaginous origin. It can be a primary lesion but may also develop from a preexisting cartilaginous lesion (e.g., osteochondroma, enchondroma). On plain radiographs, chondrosarcoma is typically visualized as a destructive, lytic lesion. Extension into surrounding soft tissues is frequently seen and delineated well on MRI. The characteristic chondroid matrix (rings
and arcs) can be seen on radiographs (70%), and better visualized by CT. The histology generally demonstrates enlarged, pleomorphic chondrocytes with multinucleated lacunae.
Level 4 evidence by Lee et al reviewed 227 patients with chondrosarcoma with an average follow-up of 6 years. They found that “patients who had had a resection with wide margins (margins extending outside the reactive zone) had a longer duration of survival than did those who had had a so-called marginal resection (margins extending outside the tumor but within the reactive zone) or an intralesional resection (margins within the lesion) (p < 0.04)."
Sixty Gy is a typical radiation dose for which of the following indications?
Prevention of post-operative heterotopic ossification
Neoadjuvant radiation therapy for a high-grade chondrosarcoma
Adjuvant radiation therapy for a high-grade osteosarcoma
Adjuvant radiation therapy for a soft-tissue sarcoma
Palliative therapy for a painful adenocarcinoma metastasis in the thoracic spine
Sixty Gy (or 6000 cGy) is a typical radiation dose for adjuvant radiation therapy for a soft-tissue sarcoma.
External beam radiotherapy plays a major role in the treatment of soft-tissue sarcomas following limb salvage surgery. Radiation doses can vary between 45 and 65 Gy. Any dose of XRT compromises wound healing, but especially those of 45 Gy (delayed healing) and 60 Gy (not expected to heal).
Incorrect Answers:
Question 2
Which of the following techniques is most commonly used to classify tissue type in soft-tissue tumors?
Explanation
Question 3
-What is the most appropriate initial treatment for her condition?
Explanation
This patient has a history most consistent with multidirectional instability. A lax capsule causes subluxation of the shoulder and strain on the rotator cuff and may result in pain and instability. The capsule is most closely associated with the cause of her problem. Initial treatment for multidirectional instability is physical therapy focusing on restoring balance to the shoulder with rotator cuff and scapular stabilization exercises. Nonsurgical therapy should be protracted and is the mainstay of treatment in this scenario. This patient has exhausted all nonsurgical measures and is now a candidate for surgical reconstruction. Capsular plication will best address the lax capsule and provide the best option for reducing her symptoms. The rotator cuff and biceps tendon may be secondarily strained but are not the primary sources of the problem. The brachial plexus does not address the etiology, but rather the symptoms that may occur as a result of instability of the shoulder joint.
Complete rest will not alleviate the patient's underlying condition because the shoulder girdle may still be weak and symptoms likely will return. A corticosteroid injection and arthroscopic surgery are too invasive as initial treatment for this condition. Arthroscopic rotator cuff repair, a biceps tenodesis, and superior labral anterior-posterior repair are unlikely to result in symptomatic improvement for this patient and are not associated with pathologic findings in the setting of multidirectional instability.
Question 4
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
REFERENCES: Sady SP, Wortman M, Blanke D: Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil 1982;63:261-263.
Tanigawa MC: Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys Ther 1972;52:725-735.
Wallin D, Ekblom B, Grahn R, Nordenberg T: Improvement of muscle flexibility: A comparison between two techniques. Am J Sports Med 1985;13:263-268.
Question 5
A 43-year-old man who works as a plumber has a painful stiff elbow in his dominant arm. He notes that while he recalls no single event of injury, he thinks the many years of pulling wrenches and soldering pipes have resulted in his problem. He reports that he has pain with any motion in bending his arm and can no longer straighten his elbow. Examination reveals generalized swelling of the elbow, both medial and lateral with a range of motion that lacks 45 degrees of extension and flexes only to 110 degrees. Pronation and supination are also limited to 45 degrees. Audible crepitus is perceived but there is no instability. Radiographs reveal advanced osteoarthritis at the radiocapitellar and ulnohumeral joints with complete loss of articular cartilage. What is the most appropriate initial treatment option? Review Topic
Explanation
must respect the physical demands of the patient while trying to preserve joint motion and function with tolerable symptoms. Osteophyte resection and capsular release have offered many patients significant improvement in their symptoms while allowing them to return to most activities. The osteophyte resection and releases can be done effectively by an open or arthroscopic approach. Whereas total elbow arthroplasty would likely result in better and more thorough pain relief, it would not tolerate the occupational demands of this individual. There is no role for physical therapy initially in the face of advanced, painful arthritis associated with long-standing fixed joint contractures. Elbow fusion results in severe loss of function and its indication is rare and usually considered in the face of unmanageable sepsis. Radial head resection may improve symptoms related to the radial capitellar arthritis but would not improve range of motion or end range impingement pain. Also, radial head resection should be avoided in heavy laborers with elbow arthritis because it would lead to increased loads across the arthritic ulnohumeral joint.
Question 6
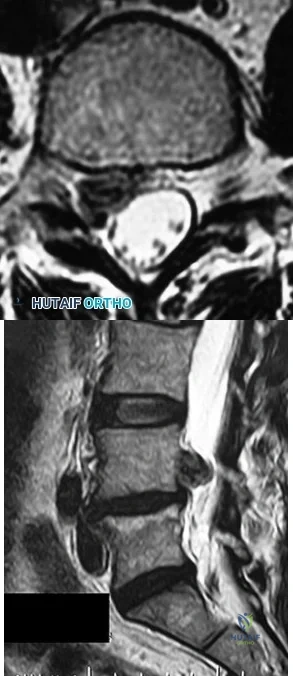
What are the most likely examination findings of the patient with the images shown in Figures 94a and 94b? A B
Explanation
The findings on MR imaging reveal a right-sided L4-L5 disk extrusion with cephalad migration of the disk fragment. The axial image shows marked displacement of the traversing right L5 nerve root. The physical findings noted in Response 4 above are typical of a right L5 sensory and motor radiculopathy that would be associated with this level of disk extrusion. Although an extrusion at this level can affect the exiting L4 nerve root resulting in an L4 radiculopathy as described in Response 1, the findings described in this response are contralateral to the disk herniation and not likely to be present. The other responses describe findings associated with left and right S1 radiculopathy, which more typically are associated with an L5-S1 disk herniation/extrusion
RECOMMENDED READINGS
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Haak MH. History and physical examination. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:43-55.
Question 7
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
Explanation
In a retrospective review of 137 patients treated surgically and 153 patients treated nonsurgically for adult scoliosis, Bess and associates found that surgical treatment for patients younger than 50 years of age was driven by increased coronal plane deformity, and surgical treatment for older patients was mandated by pain and disability. They also concluded that age, comorbidities, and sagittal balance did not influence treatment decisions.
RECOMMENDED READINGS
Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.View Abstract at PubMed
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
Question 8
- A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Explanation
Question 9
Which of the following findings is an indication for adjunctive use of high-dose steroids?
Explanation
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 319-328.
Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 10
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)? A B C D
Explanation
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. View Abstract at PubMed
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 14
Postoperative deep surgical site infection
Proximal junctional kyphosis
Pedicle screw cut-out
Pseudarthrosis
Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
Question 11
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
REFERENCES: Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 19-27.
Question 12
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 13
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
REFERENCES: Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598.
Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Shereff MJ, Cullivan WT, Johnson KA: Osteoid-osteoma of the foot. J Bone Joint Surg Am 1983;65:638-641.
Question 14
An 85-year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 1.0 mg/L (reference range 0.08 to 3.1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly difficult with activities of daily living and mobility.
Question 15
Figures 1 through 3 are the MRI scans of a 26-year-old man who injured his knee wrestling one day prior. He has a moderate effusion, medial knee pain and an inability to extend his knee actively or passively. What is the most appropriate definitive treatment option?
Explanation
Question 16
What is the most common complication following surgical fixation of a distal humeral fracture?
Explanation
REFERENCES: Sanders RA, Raney EM, Pipkin S: Operative treatment of bicondylar intra-articular fractures of the distal humerus. Orthopedics 1992;15:159-163.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 397-404.
Question 17
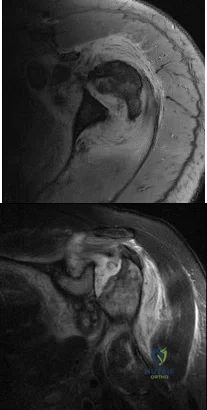
A 62-year-old woman has loss of function of her left shoulder and dull pain. She denies any history of trauma, and there were no previous surgical procedures. MRI scans are shown in Figures 42a and 42b. The etiology of this pathology is most likely confirmed by Review Topic
Explanation
Question 18
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Kamineni S, Hirahara H, Pomianowski S, et al: Partial posteromedial olecranon resection:
A kinematic study. J Bone Joint Surg Am 2003;85:1005-1011.
Question 19
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
Explanation
REFERENCE: Ruedi T, Murphy WM (eds): AO Principles of Fracture Management. New York, NY, Thieme, 2000, p 221.
Question 20
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings. Which of the following has been shown to decrease the risk of developing this complication?

Explanation
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to
lower infection rates). Most encouraged shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Question 21
What is the most common cause of early failure for patellofemoral arthroplasty?
Explanation
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.

Question 22
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them? Review Topic
Explanation
Question 23
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?
Explanation
kyphosis and stenosis. Because he is healthy, has responded well to previous surgery,
|and has a potentially correctable lesion, he is not a good candidate for an end-stage failed
back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient’s relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
REFERENCE: Eck JC, Humphreys SC, Hodges SD: Adjacent-segment degeneration after lumbar fusion: A review of clinical, biomechanical, and radiographic studies. Am J Orthop 1999;28:336-340.
Question 24
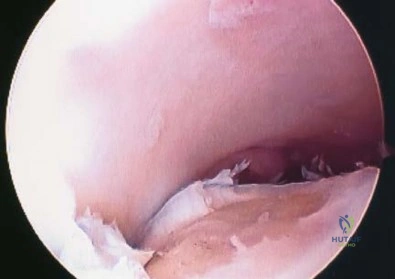
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 25
-Figures 3a and 3b are the clinical photographs of a 35-year-old man seen 3 months after repair of an acute Achilles tendon rupture. He has no constitutional symptoms and is unable to perform a single heelrise test. The most appropriate treatment is

Explanation
Question 26
Figures below depict the AP and lateral radiographs obtained from a 64-year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 27
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?
Explanation
REFERENCES: Ghalambor N, Warner JJP: Arthroscopic capsular release: Evolution of the technique and its applications. Tech Shoulder Elbow Surg 2000;1:52-60.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 28
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 29
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 30
An otherwise healthy 16-year-old dancer reports a 1-month history of leg pain. AP and lateral radiographs of the distal femur are shown in Figures 67a and 67b. What is the next most appropriate step in management?
Explanation
REFERENCES: Gebhardt MC, Ready JE, Mankin HJ: Tumors about the knee in children. Clin Orthop Relat Res 1990;255:86-110.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 31
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient? Review Topic
Explanation
Question 32
Benign Ethnic Neutropenia is more common in males.
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14- year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
The perioperative use of which medication has been shown to increase the risk of post-operative infection following orthopaedic procedures in patients with rheumatoid arthritis (RA)?
Naproxen
Leflunomide
Sulfasalazine
Etanercept
Aspirin
Of the medications listed, only etanercept has been shown to increase the risk of post- operative infection following orthopaedic procedures in patients with RA.
Etanercept is a TNF-alpha antagonist with a short half-life that is administered once or twice weekly in patients with RA. Since TNF-alpha plays a central role in the pathogenesis of RA and is instrumental in causing joint destruction, the inhibition of this molecule has shown excellent results in controlling disease. The most powered study on TNF-alpha inhibitor use in the perioperative period following an orthopaedic procedures demonstrated a significant increase in
post-operative infection.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Giles et al. review 91 patients with rheumatoid arthritis who underwent an orthopaedic procedure. They found TNF-alpha inhibitor therapy to be significantly associated with the development of a serious postoperative infection (p=.041)
Perhala et al. review 61 patients with RA who were treated with methotrexate during the perioperative period surrounding a total joint arthroplasty. They
failed to find a significant increase in complications in this patient group, stating the perioperative use of methotrexate does not affect wound healing or increase the likelihood of periprosthetic infection.
Illustration A shows the site of action of TNA-alpha inhibitors in the RA pathway.
Incorrect Answers:
Communication breakdown is the leading cause of which of the following?
Delayed diagnoses
Medication errors
Surgical site infections
1 and 2
All of the above
Communication failures are the leading cause of wrong side surgeries, medication errors and diagnostic delays.
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
treatment, medication errors and wrong side surgery
Which of the following is true regarding osteoprotegerin (OPG)?
It is secreted by osteoclasts
It increases bone resorption
Binds to prostoglandin E2 before stimulating osteoclasts
Osteoprotegerin knock-out mice develop osteopetrosis
Binds to and sequesters RANKL
Osteoprotegerin is a decoy receptor for RANKL. Binding to RANKL causes decreased production of osteoclasts by inhibiting the differentiation of osteoclast precursors.
Bone resporption/remodeling is a complex process regulated by a large variety of molecules. Molecules that have shown to inhibit osteoclasts include OPG, calcitonin, estrogen, TGF-B, and IL-10. Corticosteroids have been shown to decrease production of OPG, thereby enhancing osteoclast formation and longevity. Prolia, or denosumab, is a newly approved drug used to treat osteoporosis and has a mechanism of action similar to osteoprotegerin
(inhibits binding of RANKL to RANK).
Boyle et al. review osteoclast differentiation and activation. The authors state that targeted disruption of OPG causes increased osteoclastogenesis and/or activation resulting in osteopenia.
Illustration A shows how OPG binds to RANKL inhibiting the stimulation of osteoclasts.
Incorrect Answers:
A 55-year-old woman has T-score -2.0 at the femoral neck. According to the World Health Organization Fracture Risk Assessment Tool (FRAX), she has a ten- year probability of sustaining a hip fracture of 1.5% and a ten-year probability of sustaining a major osteoporotic fracture of 8.9%. Which of the following statements is true regarding her antiresorptive therapy management?
Antiresorptive therapy should be started based on her T-score
Antiresorptive therapy should be started based on her risk of hip fracture alone
Antiresorptive therapy should be started based on her risk of major osteoporotic fracture alone
Antiresorptive therapy should not be started
Antiresorptive therapy should be started based on her risks of both hip fracture and major osteoporotic fracture
This patient has osteopenia. Assessment by FRAX shows that ten-year risk of hip fracture is less than 3% and her ten-year risk of major osteoporosis- related fracture is less than 20%. Therefore, antiresorptive therapy is not indicated at this time.
According to the 2008 National Osteoporosis Foundation guidelines, pharmacologic treatment for osteoporosis should be considered if patients are
postmenopausal women or men greater than 50 years old AND meet one of the following criteria: (1) they have a prior hip or vertebral fracture, (2) they have a T score -2.5 or less at the femoral neck or spine, (3) they have a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%.
FRAX (World Health Organization Fracture Risk Assessment Tool) calculates
year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. reviewed the assessment of fracture risk. Besides FRAX score and T-score, they discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Ekman et al. reviewed the role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. The surgeon should consider prescribing appropriate medications, physical therapy, assessing fall risk and preventing falls and changing lifestyle factors (exercise, smoking and alcohol).
Illustration A shows the FRAX online tool (http://www.shef.ac.uk/FRAX/tool.aspx?country= =9).Illustration B shows the clinical risk factors considered in FRAX calculation.
Incorrect Answers:
A 32-year-old runner sustains a trimalleolar left ankle fracture. She undergoes open reduction and internal fixation and is kept non- weightbearing after surgery. At 2 months, what changes will occur in the articular cartilage of both her knees as a result of her current weightbearing regimen?
Cartilage thickening in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
Cartilage thinning in both knees
Cartilage thinning in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
Cartilage thinning in the left (ipsilateral) knee and increased cartilage thickness in the right (contralateral) knee
Increased cartilage thickness in both knees
After a period of off-loading, the off-loaded limb will experience cartilage thinning. The contralateral limb will not demonstrate any cartilage changes.
Physiologic loading of cartilage increases proteoglycan synthesis and cell proliferation and is chondroprotective. Joint immobilization leads to cartilage thinning, tissue softening, and reduced proteoglycan content, leading to cartilage erosion. Joint overuse leads to cartilage damage (in vitro only).
Hinterwimmer et al. examined cartilage atrophy after partial load bearing
using quantitative MRI. They found cartilage thinning in all knee compartments (greatest thinning, medial tibia; least thinning, patella). There was no change in cartilage morphology in the contralateral knee.
Sun reviewed the relationship between mechanical loading and cartilage degeneration. In OA, cartilage breakdown occurs at the articular surface, and is then fueled by synovial proteases and cytokines. In RA, synovial cells and macrophages are the source of degradative enzymes and incite cartilage destruction.
Milward-Sadler et al. examined mRNA levels following mechanical stimulation in normal and osteoarthritic chondrocytes. Normal chondrocytes showed increased aggrecan mRNA and decreased matrix metalloproteinase 3 (MMP-3) mRNA after stimulation. This
chondroprotective response was absent in osteoarthritic chondrocytes.
Illustration A shows pro- and anti-inflammatory mechanisms of mechanical loading on chondrocytes. Underloading and overloading induce cartilage damage through pathways involving the upregulation of MMPs and ADAMTSs (ADAMTS, a disintegrin and metalloproteinase with thrombospondin motifs, or aggrecanase). Physiological loading blocks these increases.
Incorrect Answers:
A morbidly obese 40-year-old man is scheduled to undergo hemilaminectomy for resection of an painful osteoid osteoma of the T6 lamina. He is positioned prone on a Jackson table and localization is performed with intraoperative fluoroscopy prior to the start of the case. At close to the end of the case, intraoperative frozen section reveals only normal bone fragment from the resected lamina. A probe is placed and a cross-table lateral radiograph reveals that the T7 lamina was resected instead of T6. At this point, the surgeon should
do all of the following EXCEPT
Complete the surgery
Abort the case and obtain further imaging
Apologize to the patient and family
Formally document the error in the operative report
Inform the patient and family immediately after the operation
Fluoroscopic localization of the correct thoracic vertebra can be difficult in the obese
patient. Upon detection of wrong level surgery, he should not abort the case. Rather, he should perform the desired procedure at the correct site, and advise the patient and family upon completion.
Adverse events are inevitable. The correct action following wrong-site surgery is to perform the desired procedure at the correct site followed by frank and honest communication with the patient/family. Open, honest communication favorably affects patient behavior, health outcomes, patient satisfaction, and often reduces the incidence of medical professional liability actions. The
discussion should include a disclosure of known facts and an explanation as to the likely cause, as well as ongoing treatment, follow up care, and prognosis.
The AAOS Information Statement about Wrong Site Surgery identifies 3 treatment steps following discovery of an error during surgery under general anesthesia: Return the patient to his preoperative condition, perform the correct procedure at the correct site, and advise the patient and family of what occurred and the likely consequences, if any, of the wrong- site surgery.
The AAOS Information Statement on Communicating Adverse Events states that the surgeon has an ethical and professional obligation to disclose the error to the patient and/or family. Disclosure should include what happened, why it happened, health implications, and what measures are being instituted to prevent recurrences.
Incorrect Answers:
All of the following are Standards of Professionalism relating to interactions with industry for practicing orthopaedic surgeons EXCEPT:
Decline gifts from industry with a market value over $100 (unless they are medical textbooks or patient educational materials)
Disclose to the patient any financial arrangements with industry that relates to the patient's treatment
Accept no direct financial inducements from industry for utilizing a particular implant
Disclose any relationship with industry to colleagues who may be influenced by your work
Decline to participate in industry sponsored non-CME courses or
conferences
The AAOS has adopted the Standards of Professionalism (SOP). These SOP’s establish mandatory, minimum levels of acceptable conduct for fellows and members of the AAOS to engage in relationships with industry. There are 17 standards with relation to industry. Answer choice 5 is not a SOP as surgeons are allowed to participate in or consult in meetings that are conducive to the effective exchange of information. The SOP also stipulate that tuition, travel, and modest hospitality (including meals and receptions) are allowed to attend an industry-sponsored non-CME course.
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
Single factor analysis of variance
Chi-square test
Student t-test
Mann-Whitney rank sum test
Wilcoxon rank sum test
In the study provided, we need to determine whether distributions of categorical variables differ from one another. The appropriate study is the chi- square test.
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi- square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in terms of measures of dispersion, such as range, standard deviation, and percentiles.
Illustration A shows an algorithm for determining which test to use for varying data. Incorrect Answers:
distributed.
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating?
A locked plate construct (locked screws) or hybrid construct (locked and non- locked screws) is necessary.
Periosteal stripping is performed through two incisions proximal and distal to the fracture.
Bridge plating is performed following direct reduction of the fracture.
AO Type A diaphyseal fractures are best treated with this technique.
Bridge plating with a long working length creates a flexible, axially stable construct.
In bridged plating, only the most proximal and distal screw holes are filled. This creates a flexible, axially stable construct.
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18- 43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
periosteal blood supply is critical.
Which of the following components of bone is most responsible for compressive strength?
Type I collagen
Osteocalcin
Proteoglycans
Osteonectin
Osteopontin
Proteoglycans, in addition to calcium hydroxyapatite [Ca10(PO4)6(OH)2], are most responsible for providing compressive strength.
Bone is composed of both organic and inorganic components. Inorganic components include calcium hydroxyapatite and osteocalcium phosphate. Organic components include collagen, proteoglycans, matrix proteins, cytokines and growth factors. While Type I collagen is responsible for providing the tensile strength of bone, proteoglycans and calcium hydroxyapatite [Ca10(PO4)6(OH)2] are most responsible for providing compressive strength. Proteoglycans contain a core protein with various
numbers of covalently attached side chains of glycosaminoglycans. In addition to providing compressive strength, they are also responsible for binding growth factors and inhibiting mineralization.
Knothe et al. review the osteocyte. They discuss that osteocytes are the most abundant
cells in bone, are actively involved in maintaining the bony matrix, and may act as mechanosensors.
Illustration A shows a proteoglycan aggregate, which can form when individual molecules link onto a chain of hyaluronic acid.
Incorrect Answers:
A prospective, randomized controlled trial of 150 patients undergoing total hip arthroplasty is performed to test whether repair of the capsule during a posterior approach reduces post-operative dislocations in the first three months. The study found no difference in dislocation rate if the capsule was repaired versus not repaired (p =
.34). Subsequently, a multicenter follow-up study of 2000 patients showed that repairing the capsule led to a decreased dislocation rate
in the first three months (p = .03). Assuming the second study reflects reality, which of the following errors occurred in the first study?
Observer bias
Type-II error
Alpha error
Type-I error
Confounding error
In this situation, the null hypothesis was accepted when it should have been rejected.
This is a type-II error.
A study can have two types of errors. Type-I errors, or alpha errors, occur when the null hypothesis is rejected when it should have been accepted. The alpha level refers to the probability of a type-I error. By convention, the alpha level of significance is set at 0.05, which means that we accept the finding of a significant association if there is less than a one in twenty chance that the observed association was due to chance alone. Type-II errors, or beta errors, occur when the null hypothesis is accepted when it should be rejected. This
often occurs when studies are underpowered. In the example above, the null hypothesis is that repair of the capsule does not reduce dislocations within the first three months. Since the first study did not show a statistically significant difference, the null hypothesis was accepted. Since a more powered study showed that repair of the capsule does reduce dislocations, the null hypothesis should have been rejected in the initial study (if it was adequately powered).
Fosgate et al. review the importance of sample size calculations when performing research. They state that sample size ensures statistical significance if the subsequent data collection is perfectly consistent with the assumptions made for the sample size calculation (assuming power was set as
50% or greater).
Illustration A shows the difference between type-I and type-II errors. Video V is a lecture discussing statistical definition review of PPV, NPV, sensitivity and specificity.
Incorrect Answers:
that properly constructed studies attempt to avoid.
Which of the following is a potential cause of fretting corrosion?
The micromotion at the femoral head-neck junction in a modular total hip replacement
A stainless-steel cerclage wire is in contact with a titanium-alloy femoral stem
Friction between polyethylene liner and femoral head leading to osteolysis
The formation of pits within a stainless-steel plate and the subsequent release of metal ions
The formation of an adherent oxide coating on titanium implants
Micromotion at the femoral head-neck junction can lead to fretting corrosion, one of the most common causes of failure of a modular implant.
Modular components give surgeons excellent intraoperative flexibility, but are susceptible to various types of corrosion. While titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer leading to fretting corrosion, defined as micromotion at contact sites under load. This may eventually lead to a painful synovitis that necessitates a revision procedure.
Srinivasan et al. review modularity in total hip arthroplasty. Amongst other things, they discuss the modularity of the femoral head/neck junction, describing the morse taper interlocking system that provides both axial and rotational stability.
Illustration A shows an example of corrosion at the head/neck junction of a total hip arthroplasty.
Incorrect Answers:
Which of the following situations is most likely to decrease sentinel event errors?
Physician and nurse training is lengthened by 20%
Resident hours are decreased to 55 hours per week
An environment is created where all members of the healthcare team feel empowered to express their concerns and beliefs
Holding individuals responsible for errors in clinical judgement
Physicians and nurses are assigned to a smaller number of patients
Creating an environment where all members of the healthcare team feel empowered to express their beliefs increases communication, the key element in decreasing sentinel events.
Research has shown that 70% of sentinel event errors are caused by improper communication. Specific ways to improve communication include effective clinical handover between shifts and breaking down the "hierarchy" so that all members of the team can discuss their expectations and concerns. Barriers to effective communication include distractions, cultural differences, power distance relationships, time pressures, and lack of organization.
Leonard et al. describe specific clinical experiences in the application of surgical briefings, properties of high reliability perinatal care, the value of critical event training and simulation, and benefits of a standardised communication process in the care of patients transferred from hospitals to skilled nursing facilities. They recommend embedding standardized tools and behaviors to bridge differences in communications styles between clinicians.
Incorrect Answers:
Which of the following side effects is most strongly associated with the use of NSAIDs?
Hepatic dysfunction
Renal impairment
Prolonged QTc
Seizures
Hematuria
All NSAIDs have the potential to cause serious renal impairment.
NSAIDs work by inhibiting the cyclooxygenase pathway (COX), which is comprised of the COX-1 and COX-2 pathways. The COX-1 pathway is involved in prostaglandin E2– mediated gastric mucosal protection and thromboxane effects on coagulation, while the COX-2 pathway is mainly involved with the modulation of pain and fever without effect on platelet function. While selective COX-2 inhibitors have a decreased side effect profile, all NSAIDS
have the potential to cause renal impairment and their use should be limited in patients with underlying renal disease.
Horlocker et al. review multimodal pain management in the perioperative setting of a total joint arthroplasty. Specifically, they note that NSAIDs should be used cautiously in patients with underlying renal dysfunction who are to undergo a procedure with major blood loss.
Griffin et al. reviewed 1,799 patients hospitalized for acute renal failure. They found that NSAIDs increased the risk of renal failure by 58% and that NSAID use resulted in 25 excess hospital admissions per 10,000 years of use.
Illustration A shows the COX pathways and their inhibition by NSAIDs. Incorrect Answers:
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
Glucosamine
Cholecalciferol
Levothyroxine
Teriparatide
Bisphosphonates
Bisphosphonate therapy combined with invasive dental work increases the risk for development osteonecrosis of the jaw.
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non- vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive
dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding
bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age
>60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?
Longer duration of anticoagulation due to increased risk of DVT
Avoiding anticoagulation medications due to increased risk of bleeding
Require higher dosages of post-operative analgesia
Longer period of non-weight bearing on surgical limb
Avoiding opioids due to higher risk of unrecognized allergies
Female patients with natural red-hair may require higher dosages of post- operative analgesia compared to other hair types.
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non- functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Which of the following medications used for thromboprophylaxis following orthoapedic surgery is a direct inhibitor of factor Xa?
Dextran
Rivaroxaban (Xarelto)
Coumadin
Fondaparinux (Arixtra)
Aspirin
Rivaroxaban (Xarelto), an oral anticoagulant, is a direct inhibitor of factor Xa.
Rivaroxaban (Xarelto) is a member of a new class of oral, direct (antithrombin- independent) factor Xa inhibitors, which restrict thrombin generation both in vitro and in vivo. Inhibition of Factor Xa interrupts the intrinsic and extrinsic pathway of the blood coagulation cascade, inhibiting both thrombin formation and development of thrombi.
Eriksson et al. compare rivaroxaban to enoxaparin for the prevention of symptomatic venous embolism following total hip arthroplasty. Major venous thromboembolism occurred in 4 of 1686 patients (0.2%) in the rivaroxaban group and in 33 of 1678 patients (2.0%) in the enoxaparin group. Additionally, major bleeding events were similar between the two groups.
Illustration A shows the mechanisms of action of various agents used for thromboprophylaxis.
Incorrect Answers:
as Protein C and Protein S.
The origin of bovine derived grafts is particularly important to which of the following religious groups?
Christianity
Islam
Hinduism
Buddhism
Judaism
The origin of bovine-derived surgical implants should be discussed in further detail with patients ascribing to Hinduism.
Patients come from a variety of religious backgrounds. Depending on a patient’s religion, the origin of surgical implants may have implications for their use. In Hinduism, bovine animals are considered sacred. Use of cow by- products is considered purifying in nature. Subsequently, the origin of bovine derived implants should be discussed with patients ascribing to Hinduism.
Easterbrook et al. evaluated the utility of porcine and bovine surgical implants amongst those of Jewish, Muslim and Hindu faiths. Hindu religious leaders, who were surveyed, did not approve of the use of bovine surgical implants.
Enoch et al. evaluated the acceptability of biological products amongst various religious groups. The Hindu religious leaders were found to not have an objection to the use of biological implants derived from cows.
Illustration A shows a clinical photo of a fetal bovine derived dermal substitute. Incorrect Answers:
Immunological testing of anti-cyclic citrullinated peptide antibodies (anti- CCP) is most commonly used for the diagnosis and prognosis of which immunological condition?
Ankylosis spondylitis
Rheumatoid arthritis
Psoriatic arthritis
Systemic lupus erythematosus
Reiter's syndrome
Anti-cyclic citrullinated peptide antibodies (anti-CCP) are commonly used as a marker for the diagnosis and prognosis of rheumatoid arthritis (RA).
Immunological studies are commonly performed to investigate cases of suspected rheumatoid arthritis. Rheumatoid factor has historically been used as a primary marker for RA. However, in more recent years, the use of anti- CCP antibodies has shown to be as sensitive as, and more specific than, rheumatoid factor (RF) in early and fully established disease. In general, anti-
CCP assays equate to a sensitivity of 50-75% and a specificity of 90-95%. High levels of anti-CCP have been shown to be indicative of a more erosive disease process and may be detected before the onset of arthritis.
Gardner and Kadel reviewed the laboratory studies most commonly used in rhuematologic diseases. Standard ordering for clinically suspected RA include Rf, anti- CCP, ESR/CRP as well as other markers of autoimmune diseases such as antinuclear antibodies, anticardiolipin antibodies and lupus anticoagulant, HLA-B27, and uric acid levels.
Illustration A shows the sensitivity and specificity of anti-CCP vs. RF in a variety of autoimmune diseases.
Incorrect Answers:
Vitamin C has been shown to decrease the likelihood of which of the following complications following surgery on the foot and ankle in non-diabetic patients?
Nonunion
Complex Regional Pain Syndrome, type II
Malunion
Complex Regional Pain Syndrome, type I
Wound infection
Vitamin C has been shown to decrease the likelihood of developing complex regional pain syndrome (CRPS), type 1, when given post-operatively to patients undergoing foot and ankle and wrist surgery.
CRPS is a frequent post-operative complication, with rates varying from 10-
37%. Type I CRPS does not have an identifiable nerve lesion, while type II has an identifiable nerve lesion. Multiple studies have shown that vitamin C decreases rates of CRPS following distal radius fractures, and more recently, the same has been shown following foot and ankle surgery. While the exact mechanism of CRPS is unknown, vitamin C has been shown to reduce lipid peroxidation, scavenge hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability. All of these characteristics of vitamin C may play a role in modulating the pain pathway.
Zollinger et al. perform a double-blind, prospective, multicenter trial where
416 patients with 427 wrist fractures were randomly allocated to treatment with placebo or treatment with 200, 500, or 1500 mg of vitamin C daily for fifty days. The prevalence of complex regional pain syndrome was 2.4% in the vitamin C group and 10.1% in the placebo group.
Besse et al. compare two groups of patients undergoing surgery on the foot and ankle to determine the effect of vitamin C on the development of CRPS, type I. CRPS type I occurred in 18 cases (9.6%) in the group not given vitamin C, and 4 cases (1.7%) in the group given vitamin C.
Illustration A shows an example of a limb affected by CRPS. Note the increased swelling, a common physical exam finding in patients afflicted with the disease.
Incorrect Answers:
A 25-year-old Spanish speaking male presents to the emergency department 6 hours after sustaining the injury seen in Figure A. He is grossly intoxicated and screaming in pain. Physical examination reveals a closed injury with overlying muscular compartments that are extremely firm to palpation. After sedating the patient, measurements of the intracompartmental pressures were all found to be
>75mmHg. His wife is Spanish speaking and expected to arrive to the hospital in 2-3 hours with a relative to help with translation. No medical translator is
available. You attempt to outline the risk and benefits of surgery to the patient, but the he repeatedly interrupts you and yells out ,"No surgery!". An English-Spanish speaking friend is with the patient and says that he has known the patient for over 2 years and will help with any decision making. What would be the next most appropriate step in the management of this patient?
Delay surgery to monitor the patient for impending compartment syndrome
Proceed with surgery with urgent fasciotomy after documenting the necessity of treatment without consent
Delay the surgery until the wife arrives and able to give informed consent with the aid of a translator
Proceed with surgery for urgent fasciotomy after obtaining informed consent from the patients friend
Respect the patients autonomy and reassess the patient in the morning when he demonstrates capacity to accurately comprehend the proposed treatment
This patient is presenting with compartment syndrome of the right tibia. In a situation of required surgery for limb threatening injury without available legal consent the surgeon should confirm and document the necessity of care with a fellow colleague.
Physicians are responsible for whether a patient is able to reasonably understand their medical condition and the nature of any proposed medical procedure, including the risks, benefits, and available alternatives. If the patient lacks this capacity, disclosure imposed by the doctrine of informed
consent are excused because irreparable harm that may result from the physician’s hesitation to provide treatment. Detailed documentation is also important. In addition, the attending physician should contact the Risk Management Dept at the hospital for support prior to surgical intervention or have a medical translator involved to ensure information is being translated properly.
Katz et al. reviewed the medical decision making process of Hispanic people. They showed that Hispanic people are more likely to permit their physician to take the predominant role in making health decisions compared to Non- Hispanic people.
Figure A shows a comminuted tibia and fibula fracture. Incorrect Answers
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?
The child is a victim of neglect
The child had no symptoms of pain
He was allowed to return to school wearing the cast
Concerns of cost
Follow-up instructions were not effectively communicated
The most likely reason the child did not attend the recommended orthopaedic follow-up visit was a language barrier preventing effective communication of the intended follow-up instructions.
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to
follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter.
Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
A 25-year-old female presents to the emergency room within increasing left shoulder pain after walking into a door 5 months ago. She previously sustained a femoral fracture 2 years ago after tripping on a rug. Relevant skeletal survey radiographs and tissue biopsy results are shown in Figures A through D. Laboratory investigations show normal glomerular filtration rate and creatinine clearance. Dual energy x-ray absorptiometry (DEXA) scan shows T-score of -1.4 and
-1.2 at the hip and lumbar spine, respectively. Which of the following laboratory values in Figure E most likely reflects this patient's condition?
A
B
C
D
E
This patient has primary hyperparathyroidism. Laboratory investigations are likely to show elevated serum intact parathyroid hormone (PTH), alkaline phosphatase (ALP) and ionized serum calcium, and low serum phosphate.
Primary hyperparathyroidism is most commonly caused by a single adenoma (80-90%). Besides the signs and symptoms of hypercalcemia, patients present
with calcification of menisci and articular cartilage, erosions in hand bones, "salt and pepper skull", and brown tumors (osteoclastomas), which appear as lytic regions expanding the cortex and causing pathological fractures, so named because of hemosiderin deposition.
Singhal et al. reviewed primary hyperparathyroidism. They advocate routine serum calcium levels for patients with pathologic fractures. If this is elevated, total and ionized calcium and intact PTH levels should be obtained. They feel that surgery for orthopaedic stabilization and parathyroidectomy should be performed simultaneously for better outcome.
Mankin et al. reviewed metabolic bone disease. They suggest that patients with mild disease with normal calcium levels do not require treatment. For patients with high calcium levels, treatment should include maintenance of fluid balance, localization and removal of the adenoma, bony stabilization, and medications (calcitonin, estrogen, bisphosphonates, and calcimimetics such as cinacalcet).
Figure A is an AP radiograph showing a lytic expansile lesion with pathological fracture in metadiaphyseal region of left humerus with similar lesion in the
fifth posterior rib. Figure B is an AP radiograph showing a lytic expansile lesion in the third metacarpal of the right hand and the fifth metacarpal of the left hand. Figure C is a low power micrograph of a brown tumor demonstrating a central zone of bone resorption, and filling with fibroblastic tissue, with a peripheral rim of osteoid production. Figure D is a high power micrograph of a brown tumor. In areas of bone resorption, there are numerous osteoclast-like giant cells amidst a fibrous stroma. This is unlike a true giant cell tumor, which lacks a fibrogenic stroma.
Incorrect Answers:
and impaired 1,25-dihydroxyvitamin D production by the diseased kidneys. This patient has normal renal function. Answer 3: Elevated PTH, ALP, serum calcium and phosphate occur in tertiary hyperparathyroidism. This again occurs in chronic renal disease after prolonged chronic secondary hyperparathyroidism or after renal transplantation, where the parathyroid glands become autonomous and PTH levels do not normalize. This patient has normal renal function.
elevated.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 33
A 10-year-old boy who has had progressive low back and right buttock pain for the past 3 days is now unable to bear weight on the right side secondary to pain. He has a temperature of 101.3 degrees F (38.5 degrees C). Examination reveals full hip range of motion; but he reports pain on the right side with external rotation. Pain is elicited with compression of the iliac wings and with direct palpation of the right sacroiliac (SI) joint. An MRI scan of the pelvis shows no abscess, but there is inflammation of the SI joint. Management should consist of
Explanation
REFERENCES: Morrissey RT: Bone and Joint Sepsis in Pediatric Orthopaedics. Philadelphia, PA, JB Lippincott, 1990.
Beaupre A, Carroll N: The three syndromes of iliac osteomyelitis in children. J Bone Joint Surg Am 1979;61:1087-1092.
Reilly JP, Gross RH, Emans JB, Yngve DA: Disorders of the sacro-iliac joint in children. J Bone Joint Surg Am 1988;70:31-40.
Question 34
A 12-year-old girl who is 3 months postmenarchal undergoes full-time brace treatment for scoliosis. The posteroanterior radiograph (Figure A ) taken at that time reveals a right thoracic curve measures 28 degrees, and the left lumbar curve measures 23 degrees. At age 15, after 3 years of bracing, a repeat posteroanterior radiograph is obtained, now revealing a right thoracic curve measuring 11 degrees and the left lumbar curve measuring 19 degree, and Risser 4. Which statement best represents the indicated course of action in this patient? Review Topic

Explanation
Curves <25° can be treated with observation, while flexible curves from 25° to 45° in skeletally immature patients (Risser 0, 1, 2) should be treated with bracing. Bracing success is most commonly defined as <5° curve progression and failure is 6° or more curve progression at orthotic discontinuation (skeletal maturity), absolute progression to >45° either before or at skeletal maturity, or discontinuation in favor of surgery. Skeletal maturity is defined Risser sign 4, <1cm change in height over 2 visits 6 months apart, 2 years postmenarchal.
Richards et al. attempted to define parameters for future AIS bracing studies. Outcome measures should include patients with (1) <5° curve progression vs >6° progression at maturity, (2) curves exceeding 45° at maturity, or those who have had surgery recommendation/undergone.
Negrini et al. performed a Cochrane systematic review. Basing conclusions on 2
studies, they found that (1) a brace treated curve progression (74% success) better than observation (34% success) and electrical stimulation (33% success), and (2) a rigid brace is more successful than an elastic one (SpineCor) at curbing curve progression.
A
is
a
standing
PA
radiograph
showing.
Incorrect
Question 35
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Pettine KA, Morrey BF: Osteochondral fractures of the talus: A long-term follow-up. J Bone Joint Surg Br 1987;69:89-92.
Question 36
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
REFERENCES: Lloyd-Roberts GC, Bucknill TM: Anterior dislocation of the radial head in children-etiology: Natural history and management. J Bone Joint Surg Am 1977;58:402.
Hamilton W, Parks JC II: Isolated dislocation of the radial head without fracture of the ulna. Clin Orthop Relat Res 1973;97:94-96.
Question 37
A 34-year-old man presents to clinic with 4 months of right elbow pain. He began going to the gym and playing squash about 3 months ago. On exam, he is tender over the lateral aspect of the elbow and has pain with resisted wrist extension. Which of the following choices lists the correct compartment of the muscle typically involved in this disease and then lists its antagonist muscle? Review Topic
Explanation
Lateral epicondylitis is an overuse injury, typically secondary to repetitive pronation and supination motion in extension, that leads to inflammation of the ECRB origin at the elbow. Histological analysis typically shows vascular hyperplasia and disorganized collagen. Clinically, patients will have pain over the lateral elbow exacerbated by resisted wrist extension. ECRB, the most commonly involved muscle origin, is innervated by the deep branch of the radial nerve and inserts on the base of the 3rd metacarpal. As it is radial wrist extensor, its antagonist is the ulnar sided wrist flexor.
Brummel et al. reviewed the clinical presentation and management options for lateral epicondylitis. They report acute symptoms in younger patients and chronic symptoms in older patients. NSAIDs, extensor stretching and activity modification are the mainstay of nonsurgical treatment.
Bunata et al. studies 85 cadavar elbows to determine anatomic factors contributing to tennis elbow. They found that the ECRB undersurface rubs against the lateral capitellium in elbow extension leading to tendinosis.
Illustration A is cross-sectional diagram of the forearm with muscle bellies labeled. Notice the location of ECRB in the mobile wad. Illustration B is a coronal T2 MRI showing fluid signal and undersurface tearing near the extensor origin as can be seen in lateral epicondylitis.
Incorrect Answers:
1-4: The ECRB is in the mobile wad and its antagonist is flexor carpi ulnaris. All other answers are incorrect.
Question 38
Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?

Explanation
Question 39
Figures 43a and 43b show the T 1 - and T 2 -weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
REFERENCES: Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 40
Figures 50a and 50b show the standing clinical photographs of a 12-year-old boy who has had increasing pain in the left foot for the past 9 months. He reports that the pain is activity related, aching in nature, and localized to the medial aspect of the midfoot and hindfoot. History reveals that he sustained a puncture wound located superior and posterior to the medial malleolus from a plate glass window 18 months ago. Examination reveals no restriction of ankle or subtalar motion, normal neurovascular status, no masses, and a well-healed 1.5-cm laceration posterior to the superior aspect of the medial malleolus. Inversion strength of the foot is decreased to grade 3/5. Radiographs of the foot show no bony abnormalities. Treatment should consist of
Explanation
REFERENCES: Mosca VS: Flexible flatfoot and skewfoot, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 355-376.
Myerson MS: Adult acquired flatfoot deformity: Treatment of dysfunction of the posterior tibial tendon, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1997, pp 393-405.
Question 41
From which artery does the princeps pollicis artery branch?
Explanation
The princeps pollicis artery can be located on the palmar aspect of the adductor pollicis and emerges into the subcutaneous tissue at the thumb metacarpophalangeal flexion crease. It branches from the radial artery just distal to the location of the deep palmar arch.
RECOMMENDED READINGS
Coleman SS, Anson B: Arterial patterns in the hand based on a study of 650 specimens. Surg Gynec Obstet 1961;4:409-424.
Ames EL, Bissonnette M, Acland R, Lister G, Firrell J. Arterial anatomy of the thumb. 78 J Hand Surg Br. 1993 Aug;18(4):427-36. PubMed PMID: 8409651. View Abstract at PubMed
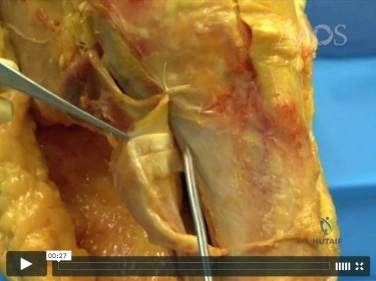
Question 42
Which of the following is considered a disadvantage of knee disarticulation when compared with transfemoral amputation?
Explanation
disarticulation versus transfemoral amputation is the degree of trauma involving the soft tissue around the knee, as increased tissue trauma may lead to painful residual limbs and eventually the need for revision amputation at a higher level. If the residual limb of the knee disarticulation is unable to accommodate the distal-end weight bearing of the socket, then patients with a knee disarticulation may experience decreased levels of function compared with patients undergoing transfemoral amputation.
Question 43
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 44
A 35-year-old woman is involved in a head-on collision while driving. Initial radiographs are shown in Figures 8a and 8b. Injury to what vessel increases the risk for osteonecrosis of the injured bone?

Explanation
Question 45
Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?
Explanation
REFERENCES: Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.
Myerson MS, Schon LC, McGuigan FX, et al: Results of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int
2000;21:297-306.
Question 46
Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in
Explanation
REFERENCES: Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194.
Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Edwards SG, Whittle AP, Wood GW: Nonoperative treatment of ipsilateral fractures of the scapular and clavicle. J Bone Joint Surg Am 2000;82:774-779.
Question 47
Patients who sustain bilateral femoral shaft fractures when compared to unilateral femur fractures have higher rates of the following EXCEPT:

Explanation
Question 48
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 49
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 50
Figure 18 is the radiograph of a 52-year-old woman who has leg length inequality and chronic activity-related buttock discomfort. This has been a life-long problem, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step vs. oblique cut, or strut grafts.
Question 51
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 52
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of
Explanation
REFERENCES: Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 53
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 54
A 36-year-old nurse has had redness, pain, and small vesicles on the pulp of her middle finger for the past 3 days. Management should consist of
Explanation
REFERENCES: Fowler JR: Viral Infections. Hand Clin 1989;5:613-627.
Jebsen PL: Infections of the fingertip: Paronychias and felons. Hand Clin 1998;14:547-555.
Question 55
- To maximally resist apex anterior angulation in the tibia, the pins of a unilateral external fixator should be oriented in which of the following planes?
Explanation
Question 56
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182.
Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293.
Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 57
A 55-year-old male sustained the injury in Figure A. His injury was complicated by an acute compartment syndrome. He underwent external fixation of his extremity and four compartment fasciotomy. When should the treatment shown in Figure B be performed to minimize the risk of infection?

Explanation
Question 58
The patient does not improve with 1 year of rehabilitation exercises. MR arthrography reveals a normal glenoid labrum and rotator cuff. Surgical treatment should consist of
Explanation
This patient has multidirectional instability (MDI). Symptoms are typically of insidious onset with nonspecific sports-related pain during the second or third decade of life. The etiology of MDI involves a patulous inferior capsular complex, but, in isolation, this lesion may not produce symptoms. Patients with MDI have abnormal patterns of rotator cuff muscle activity that is not restored with nonsurgical treatment. Symptomatic patients with MDI also demonstrate increased rates of abnormal scapular kinematics. The prevalence of MDI is higher among overhead athletes. The sulcus sign is an examination finding that produces a visible dimple inferior to the lateral border of the acromion with application of inferior traction on the arm. Generalized hyperlaxity or a connective tissue disorder may be present. Physical therapy for strengthening of the rotator cuff and scapular stabilizers remains the recommended initial treatment. Rehabilitation should continue for at least 6 months (and possibly much longer). Motivated patients frequently report diminished pain and improved stability with strengthening exercises. If nonsurgical measures fail to provide adequate relief, arthroscopic capsular plication is a viable treatment option, with high rates of return to play among properly selected patients. Thermal capsulorrhaphy has a high failure rate and poses potential for serious complications, including chondrolysis and thermal injury to the axillary nerve. Closure of the rotator interval has not been definitively shown to enhance stability or improve outcomes for patients with MDI.

Question 59
What significant structure is most at risk during a posterior approach of the Achilles tendon near its musculotendinous junction?
Explanation
REFERENCES: Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 60
A 40-year-old woman who is an avid tennis player reports the insidious onset of progressive left shoulder pain for the past 2 months. Examination reveals full range of motion with a positive impingement sign. Strength in the supraspinatus and infraspinatus muscles is normal, although stress testing is painful. An earlier subacromial cortisone injection provided good, but only temporary relief. An AP radiograph of the left shoulder is shown in Figure 10. Management should now consist of
Explanation
REFERENCES: Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg 1998;7:30-37.
Ark JW, Flock TJ, Flatow EL, Bigliani LU: Arthroscopic treatment of calcific tendinitis of the shoulder. Arthroscopy 1992;8:183-188.
Question 61
A 23-year-old male is an unrestrained driver in a motor vehicle accident and sustains an unstable pelvic ring fracture. During fluoroscopic-aided fixation, a lateral sacral view is required for proper placement of which of the following fixation methods?

Explanation
Routt et al (1997) examined the sacral slope and sacral alar anatomy in cadavers and a series of patients. They determined that the pelvic outlet and lateral sacral plain films provide the best plain radiographic view of the sacral ala. They recommended routine usage of these views intraoperatively to guide screw placement.
Routt et al (2000) reported on the early complications of percutaneous placement of iliosacral screws for treatment of posterior pelvic ring disruptions. While technically challenging, this technique leads to less blood loss and lower rates of infection compared to traditional open techniques.
Barei et al described methods of anterior and posterior pelvic ring disruptions. They determined that successful placement depends on accurate closed reduction, excellent intraoperative fluoroscopic imaging, and detailed preoperative planning. Early treatment decreased hemorrhage, provides patient comfort, and allows early mobilization.
Question 62
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 63
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 64
A 67-year-old woman has had pain in the area of the metatarsal heads and toes bilaterally for the past 18 months. She describes a diffuse discomfort and a constant burning sensation. She notes that the area feels swollen. Examination reveals that her pulses are normal, and there is no frank swelling or focal tenderness. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121.
Gorson KC, Ropper AH: Idiopathic distal small fiber neuropathy. Acta Neurol Scand 1995;92:376-382.
Question 65
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.
Question 66
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 67
A 16-year-old swimmer has right shoulder pain with activity. She describes the continued sensation that her shoulder is “loose.” She has been in physical therapy for 7 months to work on strengthening the muscles around her shoulder and scapula. She denies being able to voluntarily dislocate her shoulder. Upon examination, you can feel the humeral head slide over the glenoid rim both anteriorly and posteriorly with the load and shift test. She has a grade III sulcus sign. What is the most appropriate next step?
Explanation
Nonsurgical treatment with activity modification and physical therapy is generally considered the first-line approach for young athletes with multidirectional instability (MDI) of the shoulder. Physical therapy focuses on exercises to strengthen the scapular stabilizers and rotator cuff muscles and restore scapulohumeral rhythm. Although a definitive length of time
to assess physical therapy failure is not known, many surgeons believe that a patient with MDI should undergo at least 6 months of physical therapy and activity modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.

CLINICAL SITUATION FOR QUESTIONS 21 THROUGH 25
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow.
Question 68
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Dubousset J: Congenital kyphosis and lordosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 245-258.
Question 69
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. J Sports Med 1998;26:41-45.
Question 70
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?
Explanation
REFERENCES: Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 362-363.
Question 71
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 72
Figures 132a and 132b are the lateral and anteroposterior radiographs of a 15-year-old boy with a 6-month history of recurrent, activity-related posterior elbow pain when pitching. Two separate 6-week periods of rest have failed to provide relief. What is the next best step to enable him to return to play? Review Topic

Explanation
cessation from throwing followed by appropriate physiotherapy, surgical management with cannulated screw fixation is appropriate and has been demonstrated to have favorable success rates. Hinged-elbow bracing will not facilitate healing or return to play. Long-arm casting is likely to result in stiffness and would not be unreasonable for a short duration at the onset of symptoms, but is less likely to be helpful at this point. Plate fixation is not indicated for treatment of this injury.
Question 73
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 74
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 75
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Explanation
REFERENCE: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 76
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 77
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 78
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 79
Treatment of this fracture should consist of
Explanation
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
Question 80
When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides
Explanation
REFERENCES: Aglietti P, Baldini A, Buzzi R, et al: Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: A prospective randomized study. J Arthroplasty 2005;20:145-153.
Sorrells RB: The rotating platform mobile bearing TKA. Orthopedics 1996;19:793-796.
Dennis DA, Komistek RD: Kinematics of mobile-bearing total knee arthroplasty. Instr Course Lect 2005;54:207-220.
Question 81
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?
Explanation
REFERENCES: Haddad SL: Disorders of tendons: Peroneal tendon dysfunction, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 812-817.
MacDonald BD, Wertheimer SJ: Bilateral os peroneum fractures: Comparison of conservative and surgical treatment and outcomes. J Foot Ankle Surg 1997;36:220-225.
Question 82
Figures 7a through 7d are the images of a 31-year-old obese woman who has a long history of low-back pain and intermittent bilateral lower extremity pain. Five days ago her symptoms increased markedly and she was given pain medications upon presentation to her primary care physician. Three days ago she noticed that her bed was wet upon awakening; she also had numbness and tingling in her peroneal area and lower extremities and weakness in her lower extremities. She is brought to your office in a wheelchair. Her examination reveals diminished sensation to light touch in the L4 to S4 dermatomes and 0-1/5 strength in all muscle groups in her bilateral lower extremities with the exception of her hip flexors, hip adductors, and quadriceps, which are 5/5 in strength. She has decreased sphincter tone on rectal examination. You recommend immediate decompressive laminectomy. What is the likelihood she will regain bladder function after surgery? A B C D

Explanation
This patient has congenital and acquired spinal stenosis with multilevel disk protrusions that have both chronic (calcified) and acute components, resulting is multilevel cauda equina compression and acute cauda equina syndrome of more than 48 hours duration. Most studies indicate that patients who undergo decompression within 48 hours of symptom onset have a better prognosis for neurologic recovery than those who undergo decompression after 48 hours. Among patients with urinary incontinence, 1 study indicated that 43% remained incontinent at follow-up visits, but this study included a mix of early and late surgical patients. In another series of 44 patients with acute cauda equina syndrome, chronic bowel and bladder dysfunction were issues for 63% of those for whom surgery was delayed for more than 48 hours after symptom onset.
RECOMMENDED READINGS
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
Question 83
Arthrodesis
Explanation
with OA or RA. Certainly in patients who have glenoid bone deficiency precluding placement of a glenoid component…" as is apparent in this radiograph.
Question 84
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 85
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm 3 , with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
REFERENCE: Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 86
An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a 3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?
Explanation
REFERENCES: Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.
Pinney SJ, Lin SS: Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int 2006;27:66-75.
Question 87
Figure A is a pelvic radiograph of a healthy 20-month old girl with a limb leg discrepancy. A hip arthrogram under general anesthesia reveals concentric reduction of the left hip ONLY when the hip is positioned in 70 to 80 degrees of abduction. The next best step in treatment would be: Review Topic

Explanation
capsulorrhaphy, +/- femoral osteotomy +/- pelvic osteotomy
In children older than 18 months, open reduction is the preferred treatment for hip dysplasia. Open reduction is also considered when concentric closed reduction cannot be achieved or when excessive abduction (>60 degrees) is required to maintain reduction (due to increasing risk of avascular necrosis). The goal of open reduction is to remove the blocks to reduction and to increase stability by preforming soft-tissue or bone procedures.
Wenger et al. reviewed the surgical treatment of DDH. They say that the impediment to congruent reduction are the iliopsoas muscle, joint capsule, ligamentum teres, pulvinar, labrum, and transverse acetabular ligament. The most commonly used approaches are anterior and medial/anteromedial to the hip.
Gholve et al. reviewed DDH and the factors that contribute to secondary procedures. In their study, neither age nor unilateral vs bilateral dislocation had a direct influence on the outcome or the need for secondary procedures. The variable that significantly influenced the need for a secondary procedure was the concomitant use of a femoral osteotomy during initial surgical treatment. Of the 27 patients who did not have concurrent femoral osteotomy at index surgery, 19/27 (73%) required a secondary procedure (P<0.001).
Figure A shows an AP pelvic radiograph of an infant. Focusing on the left hip, there is lateral and superior subluxation of the femoral head, with the femoral head lateral to Perkin's line. The medial joint space is increased. The acetabular index is increased
>30 degrees. Shenton's line is disrupted. These are all features of DDH.
Incorrect Answers:
Question 88
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
Explanation
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non-vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age >60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Question 89
8 (Normal ratio = 0.8 - 1.2). The most common symptoms associated with patella baja include anterior impingement, knee pain, and knee stiffness.
Explanation

OrthoCash 2020
A 88-year-old female fell onto her right hip sustaining the fracture shown in Figure A. Past medical history is significant for mild dementia and moderate coronary artery disease. At baseline, she ambulates with a walker. There are concerns about her ability to maintain weight-bearing precautions following surgery. Which of the following is most appropriate for management of the femoral side?

Revision total hip replacement with a proximally coated femoral stem
Open reduction, internal fixation with plate and cerclage wires
Proximal femoral replacement with megaprosthesis
Impaction bone grafting
Cortical strut allograft with cerclage wiring Corrent answer: 3
The radiograph shows a Vancouver B3 periprosthetic fracture with poor proximal femoral bone stock. Given her age, co-morbidities, and dementia, the appropriate management of her condition would be a proximal femoral replacement with megaprosthesis. This can allow for immediate weightbearing in the post-operative period.
Vancouver B3 periprosthetic fractures are fractures around or just below the tip of a loose stem with poor proximal femoral bone stock. Options for management of this fracture include a fully coated stem, a fluted tapered stem, a proximal femoral replacement with megaprosthesis, allograft-prosthesis composite, and impaction bone grafting. In elderly patients with comorbidities and an inability to maintain the strict weight-bearing precautions that impaction bone grafting and allograft prosthetic replacements require, proximal femoral replacement with a megaprosthesis is the best option.
Duncan et al. were the originators of the Vancouver classification system for
periprosthetic fractures. Type A fractures are peritrochanteric, type B fracture are around the stem tip, and type C fractures are well below the stem tip.
Parvizi et al. review the indications for proximal femoral replacements with megaprostheses. They conclude it is a reasonable option for elderly patients with massive proximal femoral bone loss. The most frequent complications are aseptic loosening and dislocation.
Klein et al. identified 23 patients who underwent proximal femoral replacement for a Vancouver type-B3 periprosthetic fracture. At a follow-up of 3 years, 22 of 23 patients were walking with minimal pain. The most frequent complications were persistent drainage (2), dislocation (2), refracture (1) and acetabular cage failure (1).
Figure A shows a Vancouver B3 periprosthetic fracture with loose stem and poor proximal bone stock. Illustration A shows an example of a proximal femoral replacement. Illustration B shows a radiograph of a proximal femoral replacement used for a failed total hip replacement with massive bone loss. Illustration C shows the Vancouver classification (A, B1, B2, B3, C)
Incorrect Answers:

OrthoCash 2020
A minimal-incision technique with an incision no more than 10 centimeters has which of the following advantages compared to a standard incision for a total hip replacement?
lower post-operative visual analogue pain score
less transfusion requirement
shorter length of stay
better cosmetic result
less pain medication requirement Corrent answer: 4
Ogonda et al randomized patients to standard (16cm) versus MIS incision (<10 cm). They found no significant difference with respect to postoperative hematocrit, blood transfusion requirements, pain scores, or analgesic use.
There were also no differences in early walking ability or length of hospital stay and no differences in component alignment.
OrthoCash 2020
What is an advantage of utilizing a 36-mm instead of a 28-mm femoral head in the setting of a revision total hip arthroplasty?
Compensating for abductor deficiency
Decreasing volumetric wear
Decreasing trunion stress
Delaying neck-socket impingement
Compensating for vertical cup placement Corrent answer: 4
Increasing femoral head size delays neck-socket impingement, enhancing stability by increasing the excursion distance prior to dislocation.
The optimal bearing in total hip arthroplasty (THA) should allow for the best stability and function while preserving implant longevity. Greater motion, stability, and patient satisfaction have been correlated with larger femoral head sizes. Stability is associated with an increased displacement distance in larger diameter heads prior to a dislocation event (increased jump distance) combined with a greater impingement-free range of motion. Although larger femoral head sizes are associated with greater volumetric wear and trunion stress (and possible taper corrosion), newer bearings such as ceramic-on-ceramic may help mitigate these factors.
Kung et al. examined the effect of femoral head size and abductor integrity on dislocation events after revision THA. They separated 230 patients who underwent revision THA into 4 groups: (1) intact abductors mechanism + 28-mm femoral head, (2) absent abductor mechanism + 28-mm femoral head,
(3) intact abductor mechanism + 36-mm femoral head, and (4) absent abductor mechanism + 36-mm femoral head. They found that in patients with intact abductor mechanisms, the 36-mm femoral head was associated with a lower dislocation rate with 6-month minimum follow-up; femoral head size did not reduce dislocation events in patients with deficient abductor mechanisms.
Burroughs et al. performed an in-vitro study evaluating the range of motion and stability in THA with 28-44-mm femoral head sizes. They found that
femoral heads >32-mm provided for greater ROM and decreased component impingement. For these reasons, the authors conclude that large femoral heads may be beneficial in revision THA.
Illustration 1 demonstrates the increased jump distance when utilizing a larger diameter femoral head. Illustration 2 demonstrates a greater impingement-free range of motion with a larger femoral head.
Incorrect Answers:
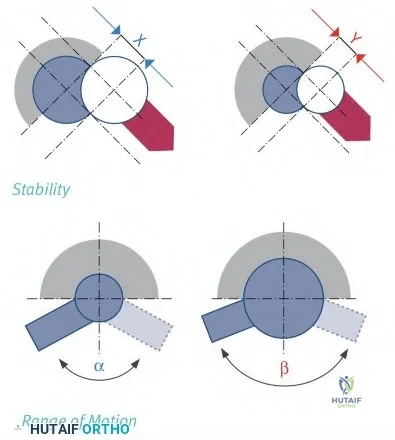
OrthoCash 2020
A 65-year-old male is now 6 weeks status post an uncomplicated total knee arthroplasty. Figures A and B represent his x-rays at today's visit. His primary complaint is knee stiffness. His current passive range of motion is 0-80 degrees, compared to 120 degrees
preoperatively, and he has failed to improve with physical therapy. He is otherwise afebrile, has no incisional erythema or pain, and CRP is within normal limits. Manipulation under anesthesia (MUA) will provide the largest improvement in flexion if performed before which of the following:

Before 6 weeks
Before 12 weeks
Before 26 weeks
Before 34 weeks
Outcomes after MUA are equivalent if performed within 1 year of surgery Corrent answer: 2
Manipulation under anesthesia (MUA) yields the greatest gain in flexion and improvement in overall range of motion if performed within 12 weeks postoperatively.
Post-operative knee stiffness (flexion < 90 degrees) occurs in 1.3%-12% of patients who undergo TKA. The preoperative risk factors for stiffness include decreased preoperative range of motion, age, diabetes mellitus, and socioeconomic status. Surgical factors can also contribute, including
overstuffing the patellofemoral joint, tight flexion/extension gaps, and excessive tightening of the extensor mechanism. If left untreated, loss of flexion negatively impacts functional outcomes, patient satisfaction, and ability to perform activities of daily living. MUA is considered the initial management for patients with flexion less than 90 degrees.
Issa et al. studied the optimal timing of MUA. They found that patients undergoing MUA before 12 weeks had a significantly higher mean gain in flexion (36.5° versus 17°), higher final range of motion (119° versus 95°), and higher Knee Society objective (89 versus 84 points) and function scores (88 versus 83 points) than those who had late manipulation under anesthesia (after 12 weeks). There was no statistically significant difference between MUA before 6 weeks vs MUA before 12 weeks.
Desai et al. similarly demonstrated that maximum flexion gains were achieved when MUA was performed between 12-14 weeks post-operatively. They also demonstrated that there is no benefit to multiple manipulations, with no observed flexion gain after the initial intervention.
Incorrect Answers:
OrthoCash 2020
A 51-year-old male presents with worsening left hip pain over the past 8 months. The patient reports hip surgery 5 years prior as seen in Figures A and B. His CRP level is within normal limits, ESR is at the upper limit of normal, and automated cell count following a hip aspiration yields a WBC of 15,000/µL (rr, 4500-11000µL) and 85% PMNs. Metal ion testing reveals elevated serum cobalt and chromium levels. What is the next best step?

Manual cell count of synovial fluid
stage revision arthroplasty
Acetabular cup revision with bone grafting
Femoral revision with cerclage wire placement
Hip arthrodesis
The patient has had a metal-on-metal (MoM) hip resurfacing with osteolysis. It is likely his WBC count is falsely elevated secondary to metal debris and corrosion. The next best step is a manual cell count to evaluate for metal debris, clots, fragmented cells, or other defects preventing accurate automated cell count.
Diagnosis of infection in the setting of MoM bearing surface can be difficult given very similar presentations. Typical workup includes CRP, ESR, synovial fluid WBC, and differential. Metal debris and corrosion reactions can confound the synovial fluid analysis leading to falsely elevated WBC counts in cases of aseptic failure. Prosthetic joint infection (PJI) and metallosis can occur concurrently so aggressive diagnostic testing is important for surgical decision making. Manual cell count of synovial fluid samples can identify metal debris and avoid false positives from automated cell testing. Supplementary tests, such as MARS MRI, metal ion levels, manual cell count, and repeat aspiration, can help guide appropriate management in these scenarios.
Yi et al. investigated ESR, CRP, synovial WBC and differential in diagnosing PJI in the setting of MoM hips or non-MoM hips undergoing revision for corrosion
or full thickness wear. They found that synovial fluid WBC count can be confounded by inaccurate automated cell counts secondary to foreign material and degenerating cells. They conclude that diagnosis of PJI in the setting of failed MoM bearings or corrosion is difficult due to falsely positive synovial fluid WBC.
Carrothers et al. evaluated the prevalence of complications of hip resurfacing arthroplasty. They found the most common complication was fracture of the femoral neck, followed by loosening of the acetabular component, femoral head collapse, loosening of a femoral component, infection, aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL), loosening of both components, and malposition of the acetabular component. They conclude that knowledge of complications following hip resurfacing is important to help select patients and counsel them on risks prior to surgery.
Figures A and B show a metal-on-metal hip resurfacing with supra-acetabular osteolysis.
Incorrect Answers:
OrthoCash 2020
An 87-year-old female presents with longstanding knee pain. The structures identified in Figure A are formed through the pathologic activation of endochrondral ossification. The pathway involved in this process involves which of the following signaling molecules?

Indian hedgehog (Ihh)
Peroxisome proliferator-activated receptor gamma (PPARG)
Receptor activator of nuclear factor kappa-ligand (RANKL)
Osteoprotegerin (OPG)
Sclerostin
Osteoarthritis and formation of osteophytes are felt to be mediated by the differentiation of quiescent chondrocytes through the Indian hedgehog signaling pathway.
Indian hedgehog (Ihh) is an important mediator of chondrocyte and osteoblast differentiation in prenatal endochondral bone formation. Adult articular cartilage without osteoarthritis does not have active Ihh signaling. However, Ihh and its downstream signaling proteins have been found to be unregulated in osteoarthritic joints. Ihh may play an important role in activating endochondral ossification leading to some of the clinical features of osteoarthritis (osteophytes and subchondral cysts). Modulation of Ihh has therapeutic potential in the treatment of osteoarthritis.
Maeda et al. studied mice with Ihh genes ablated from postnatal chondrocytes.
They found a loss of columnar structure, premature vascular invasion, and formation of ectopic hypertrophic chondrocytes in the growth plate. They concluded that Ihh is essential for maintained trabecular bone, skeletal growth, and articular cartilage.
Wang et al. reviewed the molecular mechanisms associated with cartilage degeneration in osteoarthritis. The study found that upregulation of the Ihh signaling molecules leads to the development of osteoarthritis, similar to that found in injury-induced controls. Additionally, they found that inhibiting the Ihh pathway reduces the severity of injury-induced osteoarthritis in mouse models.
Figure A shows a knee with varus deformity and severe medial sided arthritis with femoral and tibial sided osteophytes(red arrows).
Incorrect Answers:
OrthoCash 2020
Figure 1 is the AP pelvis radiograph of a 55-year-old male with known hip dysplasia and chronic right hip pain. He has no prior surgical history and is otherwise healthy. Your initial plan is to reconstruct his hip center at the site of his true acetabulum. Your preoperative template demonstrates that your acetabular component will have 40° of abduction, 15° of anteversion. However, there will be 25% uncoverage at the superolateral margin. What is the most appropriate next step to ensure adequate cup fixation?

Increase the abduction angle to 60 degrees for better coverage
Medialize the acetabular component beyond the medial wall for improved coverage
Elevate the hip center in search of better bone stock
Accept 25% uncoverage and proceed with total hip arthroplasty as templated
Use cement augments to improve superolateral coverage of the acetabular component
The most appropriate next step is to proceed with total hip arthroplasty (THA) as templated. Less than 30% of uncoverage is acceptable and has not been associated with increased rates of aseptic loosening.
Dysplasia of the hip broadly refers to abnormal development of the hip that leads to poor acetabular coverage of the femoral head. The characteristic pelvic deformities of dysplasia include a retroverted acetabulum with bone loss at the superolateral margin. As a result, there is often insufficient bone stock to provide complete coverage of the acetabular component when placed at the true hip center. Insufficient coverage (<60-70%) can lead to a lack of initial stability and early failure. If the pre-operative template suggests extreme superolateral bone loss, the surgeon must then consider alternative methods of achieving satisfactory fixation, including downsizing the acetabular component size, medializing or elevating the hip center, or use of trabecular metal augments or cement augmentation for better coverage.
Haddad et al. discuss pre-operative considerations when performing primary total hip arthroplasty on dysplastic hips. The literature review suggests that
less than 30% uncoverage does not increase the risk of aseptic loosening.
Paavilainen et al. studied the short-term outcomes on 100 cementless total hip replacements in severely dysplastic hips. They describe the importance of exposing the proximal aspect of the pubic and ischial bones since the pelvic wall is usually hypoplastic, and the use of augmentation when the superolateral rim was deficient. Overall, their outcomes with cementless total hip replacements were equivalent to cemented prostheses.
Figure A is an AP pelvis radiograph demonstrating a dysplastic right hip. Illustration A is a T1-weighted coronal MRI of a hip. Hip dysplasia can be assessed using the center-edge angle, the angle formed between a vertical line through the center of the femoral head and a line connecting the center of the femoral head with the lateral edge of the acetabulum. Less than 20° is one marker of hip dysplasia. Illustration B demonstrates the concept of joint reactive forces. Joint reactive force is minimized when the moment arm of body weight and abductor tensioning are balanced. Anatomic changes that reduce abductor tension such as elevating the hip center, decreasing femoral head size, and increased valgus neck angle increase the joint reactive force.
Incorrect Answers:
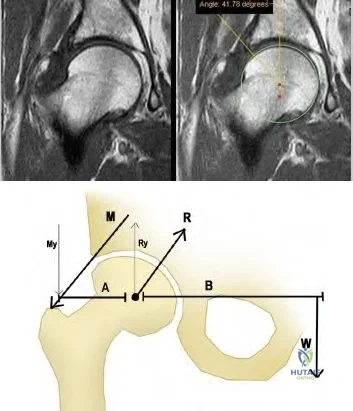
OrthoCash 2020
A 65-year-old man presents to your clinic with chronic, progressive knee pain. Figure A is an x-ray of his right knee. He would like to pursue non-surgical treatment options. The AAOS clinical practice guidelines on the treatment of symptomatic knee arthritis support which of the following with "strong evidence"?

NSAIDs; tramadol
Weight loss; arthroscopic debridement
Weight loss; intra-articular steroid injections
Valgus-offloading brace; glucosamine chondroitin injections
Tramadol; acupuncture
The AAOS clinical practice guidelines (CPG) summary "strongly" recommends tramadol or NSAIDs for the treatment of symptomatic knee osteoarthritis.
Symptomatic knee osteoarthritis is widespread, with an incidence of 240 people per 100,000. Symptoms are often progressive, though addressing the modifiable risk factors of muscle weakness, large BMI, and repetitive loading can help with pain control. Definitive management is total knee arthroplasty, however, non-operative interventions are often successful in delaying surgery, particularly in younger patients.
The AAOS Clinical Practice Guideline Summary performed a systematic review of the available literature to propose evidence-based guidelines for the management of symptomatic knee osteoarthritis. The current guidelines show strong support for the engagement in physical activity (such as guided physical therapy), non-steroidal anti-inflammatory drugs, and Tramadol for the management of symptomatic osteoarthritis. The Clinical Guidelines provided “strong” evidence against acupuncture, glucosamine and chondroitin, hyaluronic acid, and arthroscopy with lavage or debridement.
Fishman et al. performed a double-blind, randomized study of 552 patients studying the efficacy of Tramadol vs placebo in the management of arthritic knee pain. Tramadol demonstrated a statistically significant improvement in knee pain over placebo as reported by the Patient Global Rating of Pain Relief Scale.
Incorrect Answers:
OrthoCash 2020
An 82-year-old healthy male presents to the ED with right leg pain and inability to bear weight after a fall from standing. He has a history
of revision right total knee arthroplasty performed 5 years ago and was doing well until his fall this morning. On exam, he is able to actively extend his knee, though limited by pain, and is neurovascularly intact. Figures A-B are radiographs of his distal femur. What is the most appropriate treatment?

Retrograde intramedullary nail
Revision total knee arthroplasty with a stemmed femoral component
Nonoperative management with application of a long leg cast
Open reduction and internal fixation with a lateral plate
Antegrade intramedullary nail Corrent answer: 4
Open reduction and internal fixation with a lateral plate is the most appropriate treatment for this supracondylar periprosthetic femur fracture above a well-fixed total knee arthroplasty (TKA).
Supracondylar periprosthetic femur fractures are defined as fractures within 15cm of the joint line or within 5cm of the proximal end of the implant in the case of a stemmed component. Risk factors include rheumatoid arthritis, neurologic disorders, steroid use, anterior cortical notching of the femoral
component and revision TKA. Nonoperative management usually requires long-term immobilization, which can result in significant loss of knee range of motion (ROM). Therefore, surgical treatment is often preferred. An acceptable outcome is > 90° of knee ROM, fracture shortening < 2cm, varus/valgus malalignment < 5°, and flexion/extension malalignment < 10°.
Su et al. performed a literature review of the management of periprosthetic femur fractures above a TKA. First, it is crucial to determine the stability of the femoral component. An unstable femoral component requires either revision TKA or distal femoral replacement, depending on the quality of the distal femoral bone stock. A fracture with a stable femoral component can be well fixed with a buttress plate or retrograde intramedullary nail. In a series of 12 patients undergoing fracture fixation with lateral plate, all patients healed and returned to pre-fracture ambulatory status.
Zehntner et al. studied the surgical outcomes of buttress plating in 6 supracondylar femur fractures above TKA. There was no nonunion, loss of fixation or infection. Knee ROM averaged 97°, and all patients were ambulating postoperatively.
Figures A and B represent AP and lateral radiographs of a supracondylar periprosthetic femur fracture above a stemmed TKA. Illustrations C and D represent AP and lateral radiographs of a supracondylar periprosthetic femur fracture above a stemmed TKA status post repair with lateral plate.
Incorrect Answers:

OrthoCash 2020
A 60-year-old woman presents for follow-up two weeks after right total knee arthroplasty. She complains of significant anterior knee pain after fall from standing onto a flexed knee. On physical exam, her passive range of motion is 0-120 degrees and she is stable to varus and valgus stress. She is able to achieve full extension with active range of motion, though she is experiencing severe pain. Lateral radiograph of the knee is provided in Figure A. What is the most appropriate next step?

Non-operative management with long leg cast
Closed treatment with immediate active range of motion
Removal of patellar component with early active range of motion
Open reduction and internal fixation of patella with wire or screw fixation
Extensor mechanism repair with Achilles allograft and revision of the patella Corrent answer: 1
The appropriate treatment for a transverse periprosthetic patella fracture with an intact extensor mechanism is closed treatment and immobilization in a long leg cast.
Periprosthetic patella fracture after total knee arthroplasty is rare (incidence of 0.68%-5.2%) and is overwhelmingly secondary to a traumatic mechanism.
Risk factors include excessive patella resection, use of cementless components, and elevated BMI. Broadly, the treatment algorithm for periprosthetic patella fracture depends on the stability of the implant and the involvement of the extensor mechanism. Ortiquerra and Berry classified periprosthetic patella fractures as intact extensor mechanism with well a fixed implant (Type I), extensor mechanism disruption with either a loose or stable implant (Type II), or intact extensor mechanism with a loose implant (Type III). Generally, fractures associated with component loosening or extensor mechanism injuries (Type II & Type III) require revision surgery and often yield poor results. Type I fractures are successfully managed non-operatively.
Nam et al. reviewed the management of extensor mechanism complications in
total knee arthroplasty. They report excellent results in Type I peri-prosthetic patella fractures managed non-operatively, with only 1 failure in 37 patients. They propose a treatment algorithm based upon fracture pattern (transverse vs vertical), component fixation, and extensor mechanism integrity. Type I injuries with transverse fractures should be immobilized in long leg casts, whereas Type I injuries with vertical fractures are more stable and can benefit from early active range of motion.
Cottino el al. similarly review the outcomes of peri-prosthetic patella fractures. They report a 50% complication rate and a 20-40% re-operation rate for type II and type III injuries, even with anatomic reductions.
Figure A is a lateral radiograph of the knee that demonstrates a transverse peri-prosthetic patella fracture without component loosening. There is no obvious extensor mechanism injury and the prompt indicates extension is intact. Illustration A represents the peri-prosthetic patella fracture treatment algorithm as proposed by Nam et al. Illustration B represents the Ortiquerra and Berry peri-prosthetic patella fracture classification.
Incorrect Answers:
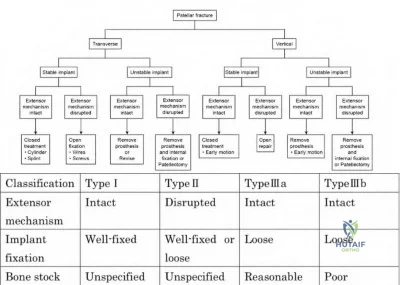
OrthoCash 2020
A 68-year-old healthy male with a history of a right total hip arthroplasty 8 years prior presents with one year of right hip pain and several months of inability to bear weight. An AP pelvis radiograph is shown in Figure A. ESR is 8 mm/hr and CRP is 1 mg/L. What is the best treatment option?
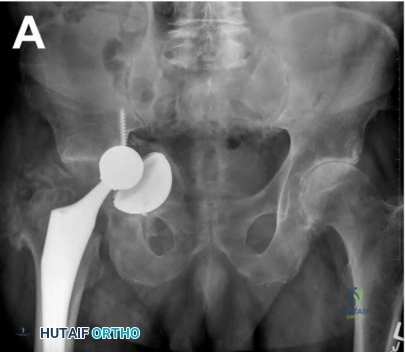
Cemented acetabular cup with morselized bone graft
Two stage revision with antibiotic spacer
Cup-cage construct with or without morselized bone graft
Definitive removal of hardware/Girdlestone procedure
Anterior and posterior column plates with hemispherical uncemented cup Corrent answer: 3
Cup-cage constructs have demonstrated excellent outcomes in patients with pelvic discontinuity and Gross type V acetabular defects.
When treating chronic pelvic discontinuities, four general principles need to be addressed: 1) restoration of the acetabulum by reconnecting the ischium to the ilium, 2) optimizing contact of bleeding bone to component surfaces with ingrowth potential, 3) grafting osseous deficiencies, 4) obtaining a mechanically stable reconstruction to protect components until ingrowth is achieved. There are several different classifications of acetabular bone loss, though the Gross classification is unique in that it not only grades the degree of bone loss but also provides reconstructive options that may be considered (Illustration A & B). Due to the segmental bone loss associated with Gross
Types IV and V defects, cup-cage constructs are used to bridge segmental defects or areas of discontinuity.
DeBoer et al. studied the long-term outcomes of 28 patients with pelvic discontinuity treated with custom triflange acetabular prostheses. They reported no instances of broken screws, implant migration, or component revision at 10 years. Complications included one partial sciatic nerve palsy and five patients with dislocation.
Makinen et al. reviewed the role of cages in revision arthroplasty. In Gross Type V defects, cages provide mechanical stability to protect the acetabular cup until ingrowth is achieved. They report two case series following cup-cage reconstructions for pelvic discontinuity, demonstrating 88% survival at 44.6 months and 87.2% survival at 82 months. The survivorship of cage only constructs was 49.9% at seven years.
Figure A demonstrates a failed right total hip arthroplasty with associated chronic pelvic discontinuity. Illustration A demonstrates the Gross classification for acetabular bone defects. Illustration B demonstrates the suggested reconstructive options for defects classified according to the Gross classification system.
Incorrect Answers:
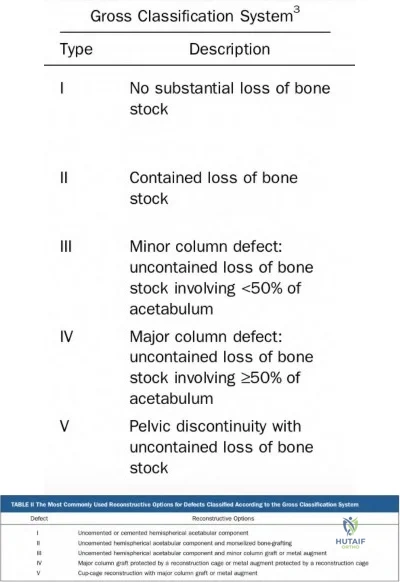
OrthoCash 2020
A 60-year-old male presents with significant left knee pain and end-stage osteoarthritis. He failed non-operative management and is requesting a total knee arthroplasty (TKA). His past medical history is significant for a left distal femur fracture that occurred when he was struck by a car 30 years prior. A standing, full-length radiograph of his left lower extremity is shown in Figure A. His femoral coronal plane deformity measures 28 degrees. When proceeding with a TKA, what must be done to address this patient's coronal deformity?

Soft tissue balancing and intra-articular bone cuts
Distal femoral medial closing-wedge osteotomy
Distal femoral lateral closing-wedge osteotomy
High tibial osteotomy
Hinged TKA
Coronal plane deformities of the femur >20 degrees require an extra-articular femoral osteotomy to achieve proper mechanical alignment when performing a TKA.
Coronal and sagittal plane deformities of the femur less than 20 degrees can usually be addressed with intra-articular bone cuts and soft tissue balancing. Attempting to correct deformities greater than this without an extra-articular osteotomy can compromise ligamentous stability. This highlights the importance of careful pre-operative templating/planning and obtaining full-length, standing radiographs when clinically warranted. Although correcting severe deformities with staged or concomitant extra-articular osteotomies can be challenging, they are often successful when properly executed.
Lonner et al. provided a retrospective case series and review article addressing
severe extra-articular deformities with simultaneous femoral osteotomy and TKA in patients with osteoarthritis. In their 10-patient series, they were successful in restoring coronal alignment within two degrees of anatomic in all patients. They suggest securing the femoral osteotomy site with a plate or locked intramedullary nail, depending on the osteotomy site.
Rajgopal et al. presented a case series of TKA in 36 knees in the setting of extra-articular deformities. In this series, they treated all patients with intraarticular bone resection and soft-tissue balancing to address their deformities. Femoral-coronal, sagittal, and tibial-coronal deformities successfully treated included 11-18 degrees, 0-15 degrees, and 12-24 degrees, respectively.
Figure A is a standing, full-length radiograph of the left lower extremity demonstrating a significant coronal plane deformity resulting from a previous distal femur fracture malunion. Illustration A is a left knee radiograph demonstrating an extra-articular distal femoral osteotomy with placement of a fluted, press-fit stem. Illustration B is the same patient at 3-year follow-up demonstrating a fully healed osteotomy and maintained hardware alignment.
Incorrect Answers:

OrthoCash 2020
A 76-year-old female presents with right hip pain 6 years after total hip arthroplasty. She denies constitutional symptoms at this time. On physical examination, her incision is well healed. Current radiographs are shown in Figures A and B. In addition to a complete blood count (CBC), C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR), an alpha-defensin immunoassay is ordered. What does the alpha-defensin immunoassay test for?

The presence of an intra-articular, antimicrobial peptide
The presence of an antimicrobial peptide within serum
The presence of an intra-articular, pro-inflammatory marker
The presence of an intra-articular, pro-inflammatory cytokine
The presence of intra-articular leukocytosis Corrent answer: 1
A synovial alpha-defensin immunoassay tests for the presence of an intraarticular, antimicrobial peptide.
When there is suspicion of a periprosthetic infection, laboratory workup should
include CRP and ESR. If suspicion remains after laboratory examination, an aspiration of the joint should be performed for cell count and culture. A fairly recent test developed to aid in the diagnosis of PJI is the synovial alpha-defensin immunoassay. Defensins are antimicrobial peptides that are active against many bacteria, fungi, and enveloped viruses. Alpha-defensin is an antimicrobial peptide which is abundant in neutrophils and macrophages. It is present in the natural local tissue response to infection. In the setting periprosthetic joint infection (PJI) the levels of intra-articular alpha-defensin increase substantially and may reach levels that can be detected by an immunoassay. Alpha-defensin may be more prone to false positive results in adverse local tissue reaction caused by a metal-on-metal arthroplasty.
Bonanzinga et al. performed a prospective study to determine the reliability of the alpha-defensin immunoassay for diagnosing PJI. They aspirated hips and knees in all patients presenting with pain in both primary and revision arthroplasties. They found the sensitivity of the alpha-defensin immunoassay was 97%, the specificity was 97%, the positive predictive value was 88%, and the negative predictive value was 99% (95% CI, 96%–99%). They conclude that alpha-defensin appears to be a reliable test.
Shinsky et al. performed a study to evaluate the utility of commonly available tests for determining the presence of PJI in patients undergoing revision total hip arthroplasty. 235 consecutive total hip arthroplasties undergoing revision were evaluated. They found that no hip in a patient with a preoperative ESR of
<30 mm/hr and a CRP of <10 mg/dL was infected. They also conclude that a synovial fluid cell count of >3000 white blood cells/mL was the most predictive perioperative testing modality when ESR and CRP were elevated as well.
Figures A and B are AP and lateral radiographs of the right hip, respectively, demonstrating a region of periarticular erosions around the proximal femoral stem.
Incorrect Answers:
OrthoCash 2020
A 72-year-old male presents to your clinic with a 6-month history of left groin pain without preceding trauma. He previously underwent an uneventful left total hip arthroplasty 15-years prior at an outside institution. He has been ambulating with a cane for the last month due to pain. A left hip radiograph is obtained and presented in Figure A. Less than 4 centimeters of intact diaphyseal bone remains distal to the isthmus. An infection work-up is negative. Of the choices provided, what is the most appropriate management option at this time?

Continued observation
Placement of a femoral cortical strut allograft and cerclage wires
Femoral revision with impaction grafting and a cementless femoral stem
Femoral revision with a metaphyseal-engaging tapered stem
Femoral revision with a modular fluted tapered stem Corrent answer: 5
This patient has a Paprosky type-IIIB femoral defect (less than 4cm diaphyseal bone available for distal fixation) that can be revised with a modular fluted tapered stem
Femoral revision with a modular fluted tapered stem is the preferred method
in the treatment of Paprosky type-IIIB femoral defects. Proximal femoral replacement, allograft prosthetic composite, resection arthroplasty, and impaction grafting may also be considered in the treatment of Paprosky type-IIIB and IV femoral defects. Impaction grafting involves creating a neomedullary canal by impacting cancellous bone chips into the femoral canal followed by cementation of the final femoral component.
Valle et al. present a review article describing the Paprosky classification of femoral defects as well as treatment options. They differentiate a type-IIIA and IIIB defect as having >4 and <4 centimeters of intact diaphyseal bone available for distal fixation, respectively.
Hartman et al. describe management strategies for femoral fixation in the setting of revision total hip arthroplasty. They review classification systems of femoral bone loss and provide an overview of various treatment options. The authors feel that type-II and IIIA defects can be effectively treated with cylindrical, extensively porous-coated implants, whereas IIIB defects can usually be treated with a modular fluted tapered stem.
Figure A show a total hip arthroplasty with less than 4cm of diaphyseal bone available for distal fixation with extensive metaphyseal and diaphyseal bone loss. Illustration A shows a diagram of the Paprosky classification for femoral bone loss.
Incorrect Answers:
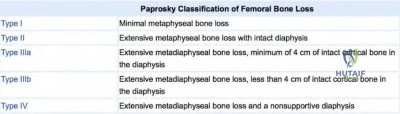
OrthoCash 2020
An 85-year-old woman sustains a ground level fall. Her THA was done 25 years ago. She was previously ambulatory but with a significant limp. With regard to the femur specifically, what is the Vancouver classification and preferred treatment option?

Vancouver C, revision to proximal femoral replacement
Vancouver B1, ORIF with impaction grafting
Vancouver AG, ORIF
Vancouver B3, revision to proximal femoral replacement
Vancouver B2, ORIF with femoral strut allograft augmentation Corrent answer: 4
The periprosthetic femoral fracture should be classified as Vancouver B3 given the location around the femoral stem with very poor proximal femoral bone stock, thus making reconstruction of this bone unrealistic. The best treatment options for a B3 fracture would be revision of the stem to a proximal femoral replacement or proximal femoral allograft composite.
The Vancouver periprosthetic classification system is one of the most useful classifications in orthopaedics as it can reliably guide treatment. Vancouver B1 or C type fractures confer a well-fixed stem and so ORIF would be the
treatment of choice. B2 and B3 fractures signify a loose femoral stem and so revision is necessary while B3 fractures have very poor proximal bone quality making any reliance on metaphyseal proximal bone for fixation or reconstruction futile.
Klein et al. retrospectively reviewed 21 patients (mean age 79) with Vancouver B3 fractures treated with a proximal femoral replacement. At most recent follow-up, 20/21 patients were ambulatory with no or minimal pain.
They note a relatively high complication rate (2 recurrent dislocators, 1 repeat fracture, 1 acetabular complication, 2 infections treated with I&D). However, given the circumstances and morbidity of non-operative management, they still recommend a proximal femoral replacement for this complicated patient group.
Savvidou et al. offer a good review of proximal femoral replacement both for periprosthetic fracture and also revision THA with significant proximal bone loss. They emphasize the complications such as dislocation and aseptic loosening and offer recommendations for minimizing them such as a large femoral head, soft tissue repair, and preservation/repair of abductors.
Figure A demonstrates a cemented total hip arthroplasty with significant osteolytic changes about both the femoral and acetabular components with multiple fractures around the grossly loose femoral stem. Taken from Klein et. al.
Illustration A demonstrates an example of a proximal femoral replacement. Taken from Savvidou et al.
Incorrect Answers:

OrthoCash 2020
Which of the following liner types have been associated with early acetabular component loosening?
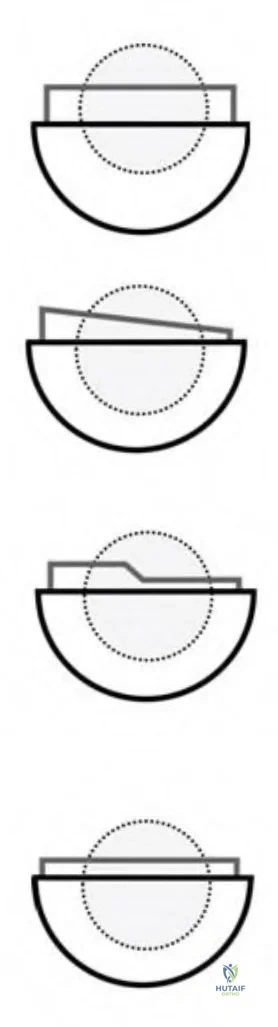
Figures B and C Corrent answer: 1
Figure A is an illustration of a lateralized or offset acetabular liner which has been shown to have a higher rate of loosening with primary and revision total hip arthroplasty (THA).
Extended offset polyethylene liners allow restoration of soft tissue tension by adding 4 to 10 mm of additional offset to the acetabular side. They translate the center of hip rotation laterally which will increase offset in the horizontal plane and add a few millimeters of additional limb lengthening in the vertical plane. The lateral translation of the center of rotation has been found to increase joint reaction forces and polyethylene wear. Additionally, this results
in an eccentric loading pattern and leads to increased torsional forces at the liner-shell interface and the bone-implant interface. This may cause motion at the interface resulting in failure of ingrowth and early loosening.
Glori performed a study to determine if torsion on an offset acetabular component may increase the risk of fixation failure. He found that a 70 kg person walking normally on a well-positioned 10-mm offset component will produce more torsion compared to a 4-mm offset component. Vertical cup placement was also found to increase torsion. He concludes that these torsional moments are comparable to moments shown to cause failure of the initial interference fit of cementless acetabular components in vitro. He suggests that after using an offset cementless acetabular component, one should initially limit weight bearing to minimize the risk of failure.
Archibeck et. al reviewed 1919 patients with primary THA and 346 with revision THA to evaluate acetabular component loosening. A 7-mm offset acetabular liner was used in 120 of the primary and 100 of the revision THAs. The aseptic loosening rate in the primary THA group was 0.12% in the standard offset and 4.2% in the extended offset groups at a minimum of 2 years follow-up. The aseptic loosening rate in the revision group was 1.7% in the standard and 7% in the extended offset groups at a mean of 4 years follow-up. They conclude that offset acetabular liners have a high failure rate in primary and revision THA.
Figure A is an illustration depicting an offset acetabular component. Figure B is an illustration depicting an oblique acetabular component or a face-changing liner. Figure C is an illustration depicting an elevated rim acetabular component or a lipped liner. Figure D is an illustration depicting a standard offset component.
Incorrect Answers:
OrthoCash 2020
During a revision hip surgery, which of the following muscles labeled in Figure 1 can be transferred in the setting of an abductor deficiency?
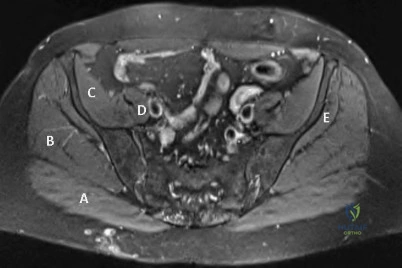
Question 90
Figures 1 and 2 are the MRI scans of a 35-year-old right-hand dominant man who has right elbow pain after trying to lift a large television at home. An examination reveals ecchymosis, an abnormal hook test, and altered biceps muscle contour. What treatment is most likely to result in a satisfactory and predictable outcome?
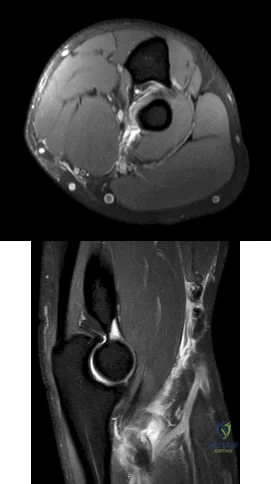
Explanation
Question 91
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
Question 92
A 43-year-old soccer player who had knee pain following a twisting injury underwent an arthroscopic meniscectomy 6 months ago. He continues to report posterior knee pain. Examination reveals soft-tissue fullness and tenderness just above the popliteal fossa, trace knee effusion, full range of knee motion, no instability, and negative meniscal signs. Radiographs show some mild medial joint space narrowing but no other bony changes. What is the next most appropriate step in management?
Explanation
11 patients. The authors noted that oncologic surgical treatment was affected in 15 of the
25 patients. The most frequent causes of erroneous diagnosis were initial poor quality radiographs and an unquestioned original diagnosis despite persistent symptoms. Persistent symptoms warrant further diagnostic studies, not additional treatment such as physical therapy, corticosteroid injection, or an unloader brace. Although a bone scan may be helpful in this case and confirm arthrosis of the medial compartment, the suspicion of a soft-tissue mass makes MRI the imaging modality of choice.
REFERENCES: Muscolo DL, Ayerza MA, Makino A, et al: Tumors about the knee misdiagnosed as athletic injuries. J Bone Joint Surg Am 2003;85:1209-1214.
Lewis MM, Reilly JF: Sports tumors. Am J Sports Med 1987;15:362-365.
Question 93
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Moskowitz A, Trommanhauser S: Surgical and clinical results of scoliosis surgery using Zielke instrumentation. Spine 1993;18:2444-2451.
Question 94
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled “A” in Figure 45?
Explanation
REFERENCES: Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Sobel M, Levy ME, Bohne WH: Congenital variations of the peroneus quartus muscle: An anatomic study. Foot Ankle 1990;11:81-89.
Question 95
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b? Review Topic

Explanation
Question 96
Figure 36 shows the radiograph of a 14-year-old boy who has been treated in the past for Perthes’ disease with an abduction brace. He now has hip pain that limits his activity, and nonsteroidal anti-inflammatory drugs have failed to provide relief. What is the most appropriate treatment?
Explanation
REFERENCES: Daly K, Bruce C, Catterall A: Lateral shelf acetabuloplasty in Perthes’ disease: A review of the end of growth. J Bone Joint Surg Br 1999;81:380-384.
Yoo WJ, Choi IH, Chung CY, et al: Valgus femoral osteotomy for hinge abduction in Perthes disease: Decision-making and outcomes. J Bone Joint Surg Br 2004;86:726-730.
Question 97
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a “foot” fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
REFERENCES: Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 98
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
REFERENCES: Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS: DeQuervain’s syndrome: Surgical and anatomical studies of the fibro-osseous canal. Orthopedics 1991;14:545-549.
Question 99
0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Explanation
Question 100
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?
Explanation
REFERENCES: Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula.
Foot Ankle Int 2006;27:907-912.
Pinzur MS, Pinto MA, Schon LC, et al: Controversies in amputation surgery. Instr Course Lect 2003;52:445-451.
