OITE & ABOS Orthopedic Prep: Trauma, Lower & Upper Extremity | Part 246

Key Takeaway
This page offers Part 246 of an OITE & AAOS Orthopedic Board Review. It provides 100 high-yield, verified MCQs, specifically formatted for board exams. Designed for orthopedic residents and surgeons, this interactive quiz supports rigorous preparation for ABOS certification, covering key orthopedic topics.
About This Board Review Set
This is Part 246 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 246
This module focuses heavily on: Arthroplasty, Foot, Fracture, Knee, Wrist.
Sample Questions from This Set
Sample Question 1: Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full exte...
Sample Question 2: A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination r...
Sample Question 3: A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tendernes...
Sample Question 4: A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?...
Sample Question 5: A patient with a displaced and comminuted fracture of the radial head and neck also has pain and swelling about the ipsilateral distal radioulnar joint. Which treatment option may exacerbate the wrist disorder?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 2
A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination reveals swelling and tenderness over the tarsometatarsal joints. Radiographs show advanced arthrosis of the first and second tarsometatarsal joints. Management should now include
Explanation
REFERENCES: Sangeorzan BJ, Veith GR, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joints by arthrodesis. Foot Ankle 1990;10:193-200.
Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 3
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient’s pain?
Explanation
REFERENCES: Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Fehring TK: Revision TJA corrects flexion extension gap imbalance. Orthop Today 2002;22:44.
Question 4
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?
Explanation
REFERENCES: Bach BR, O’Brien SJ, Warren RF, et al: An unusual neurologic complication of the Bristow procedure. J Bone Joint Surg Am 1988;70:458-460.
McIlveen SJ, Duralde XA: Isolated nerve injuries about the shoulder, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 214-239.
Question 5
A patient with a displaced and comminuted fracture of the radial head and neck also has pain and swelling about the ipsilateral distal radioulnar joint. Which treatment option may exacerbate the wrist disorder?
Explanation
A. observation.
B. corticosteroid injection.
C. immediate surgical decompression.
D. tendon transfers.
Question 6
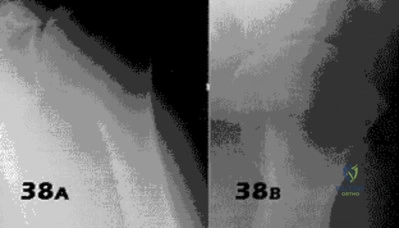
- Figures 38a & 38b show radiographs of a 40 year old man who underwent a Putti-Platt repair for recurrent dislocations at age 22. He reports increasing pain in the shoulder and limited motion for five years. Examination reveals 130 degrees of elevation and 15 degrees of external rotation. Non-surgical treatment has failed. Treatment should now consist of what?
Explanation
Late onset of pain (average 13 years) was noted following this procedure in a small number of patients. The pain is attributed to excessive G-H compressive forces due to limited external rotation. NSAIDS and PT are first line treatments. If these fail, the authors demonstrated good results with release of the anterior structures. Choices 3 & 4 would probably be reserved for patients older than 50 with more advanced signs of degenerative disease.
Question 7
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 8
A 7-year-old boy has a limp with pain and tenderness over the distal right femur. Radiographs are shown in Figures 5a and 5b. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Dormans, JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Easley ME, Kneisl JS: Pathologic fractures through nonossifying fibromas: Is prophylactic treatment warranted? J Pediatr Orthop 1997;17:808-813.
Question 9
A 56-year-old man who tripped and fell out of his golf cart onto his right shoulder 4 days ago now reports mild pain while chipping. Examination reveals mild bruising over the lateral clavicle but good shoulder range of motion and strength. A radiograph is shown in Figure 9. Appropriate treatment at this time should include which of the following?

Explanation
Question 10
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?
Explanation
REFERENCES: Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584.
Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Pochatko DJ, Schlehr FJ, Murphey MD, Hamilton JJ: Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot Ankle Int 1994;15:457-461.
Question 11
Myodesis of which muscle group is most important for optimal outcome after transfemoral amputation?

Explanation
Question 12
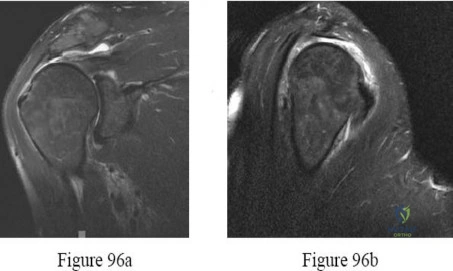
A 7-year-old girl has pain and a mass in the left scapula. A MRI scan and biopsy specimen are shown in Figures 30a and 30b. After staging studies, initial management should consist of
Explanation
REFERENCES: Grier HE: The Ewing family of tumors: Ewing’s sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am 1997;44:991-1004.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 13
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?
Explanation
REFERENCES: Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Smith DG, McFarland LV, Sangeorzan BJ, et al: Postoperative dressing and management strategies for transtibial amputations: A critical review. J Rehabil Res Dev 2003;40:213-224.
Question 14
Which wear mechanism is most likely responsible for the wear damage on the modular tibial insert retrieval shown in Figure 82?
Explanation
The figure shows the top side of a retrieved tibial liner. Pitting and delamination, which are associated with fatigue wear, are noted. Creep is deformation without wear. Adhesive and abrasive wear is associated with removal of material on the back side of modular tibial components.
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87
A bilateral cemented total knee arthroplasty (TKA) was performed on an otherwise healthy 63-year-old woman. The surgery and immediate postsurgical course were uneventful. Two days after surgery, while in physical therapy at the hospital, the patient’s oxygen saturation is noted at 92%.
Question 15
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 16
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 17
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 18
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy? Review Topic
Explanation
Question 19
A new composite material is being evaluated for potential use as a prosthetic ligament. In measuring the tensile strength of this material, why is it important to consider and accurately control the loading rate?
Explanation
Question 20
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 21
Which laboratory findings would most support a diagnosis of prosthetic joint infection (PJI) in a hip or knee arthroplasty performed 3 weeks ago?
Explanation
The diagnosis of acute PJI is associated with different criteria than the diagnosis of a chronic PJI. There is no agreed-upon threshold for ESR during the acute period (6 weeks) following total joint arthroplasty. The CRP threshold is higher during the acute period (100 mg/L vs 10 mg/L for a chronic infection). The threshold for synovial fluid analysis for an acute PJI is 10000 cells/µL and more than 90% PMN neutrophils vs 3000 cells/µL and more than 80% PMN neutrophils for a chronic infection.

Question 22
A 29-year-old obese patient is transferred from an outside facility for the management of a closed-head injury and the fracture shown in Figure A. He presents to the trauma bay as a transient responder to blood products, and undergoes urgent pre-surgical angiography embolization. Surgery is performed within 8 hours from the time of injury. The patient develops a deep wound infection 1 week post-operatively. Which of the following factors would be considered the MOST statistically significant predictor for post-operative infection in this patient.

Explanation
Question 23
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
at risk.
REFERENCES: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 281-289.
Question 24
03 Figure 9 shows the radiograph of a patient who has anterior knee pain and range of motion from 0-of the tibial tubercle. Treatment should consist of

Explanation
The picture shows a laterally subluxed and a relatively-externally rotated patella on a femoral component. The question tells us that the femoral component is internally rotated and the tibial component is perfectly placed. If we know that the femoral component should be externally
rotated about 3 degrees, we know that in this patient, that’s where the problem is. So, we don’t have to do anything to the quads, tubercle or tibial component. We need to revise the femur. Besides, a lateral retinacular release may damage the lateral geniculates; since this patient most likely had a medial arthrotomy, this may devascularize the patella and lead to patellar AVN. A lateral retinacular release will not address the malpositioned components )
back to this question next question
Question 25
Figures 122a and 122b are the radiographs of a 79-year-old woman with a 2-year history of progressively worsening right hip pain. She had a right total hip arthroplasty 7 years prior. An infection workup is negative. She opts for revision surgery; the most appropriate surgical plan to address her femoral component is
Explanation
The patient’s radiographs show loosening of the cemented femoral stem and varus remodeling of the femur. An extended trochanteric osteotomy is necessary because attempting to extract the existing prosthesis and implant another prosthesis without an osteotomy is likely to cause a proximal femoral fracture. Also, an osteotomy would facilitate atraumatic removal of the stem and cement. Cementless fixation is likely to produce a more predictable long-term outcome than cemented fixation for the revision implant.
Question 26
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?
Explanation
after surgery.
REFERENCES: Fontes RA, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
Ozalay M, Ozkoc G, Akpinar S, et al: Necrotizing soft-tissue infection of a limb: Clinical presentation and factors related to mortality. Foot Ankle Int 2006;27:598-605.
Question 27
A 3-year-old boy has hip pain and refuses to walk. His right hip is tender with any range of motion. His temperature is 102.2 degrees F (39.0 degrees C). Laboratory studies reveal the following values: C-reactive protein level of 6.0, WBC count of 19,000/mm3 (normal 3,500 to 10,500/mm3), and an erythrocyte sedimentation rate of 45 mm/h (normal up to 20 mm/h). A hip sonogram demonstrates a large effusion in the right hip. What is the best treatment plan? Review Topic
Explanation
(SBQ13PE.61) Mutations in genes COL1A1/COL1A2 are responsible for the clinical manifestations of: Review Topic
Marfan's syndrome
Osteopetrosis
Osteogenesis imperfecta
Achondroplasia
Multiple Epiphyseal Dysplasia
Osteogenesis imperfecta is caused by mutations in type I collagen genes COL1A1 or COL1A2 in 85% of cases.
Pathological manifestions of osteogenesis imperfecta (OI) occur because of abnormal type 1collagen . Clinical manifestations include multiple fractures, blue sclera, and scoliosis. The genes responsible for normal collagen synthesis are COL1A1/COL1A2 and many mutations have been characterized which result in OI. Quantitative collagen defects result in a milder phenotype whereas qualitative collagen defects result in more severe clinical manifestations.
Zeitlin et al. reviewed osteogenesis imperfecta. They report that bone fragility in OI stems from decreased bone mass, disturbed organization of bone tissue, and altered bone geometry (size and shape). They found that cyclical intravenous pamidronate administration reduces bone pain and fracture incidence while increasing bone density and level of ambulation with minimal side effects.
Burnei et al. review the diagnosis and treatment of OI. They report that medical treatment with bisphosphonates, even in patients younger than age 2 years, have become widely accepted in the symptomatic treatment of OI. They report alendronate has proven to beneficially decrease fracture frequency while improving vertebral bone density and quality of life.
Illustration A shows the Sillence Classification of Osteogenesis Imperfecta. Incorrect Answers:
Question 28
A 40-year-old woman has had sciatic pain on the left side for the past 8 weeks. She reports that the pain radiates to her posterior thigh, lateral calf, and into the dorsum of her left foot. Neurologic examination shows weakness of the left extensor hallucis longus. Axial T 2 -weighted MRI scans through L4-L5 are shown in Figure 14. Management should consist of
Explanation
REFERENCES: Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Shah RV, Lutz GE: Lumbar intraspinal synovial cysts: Conservative management and review of the world’s literature. Spine J 2003;3:479-488.
Question 29
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?
Explanation
REFERENCE: Unidia-Kallio L, et al: Serum c-reactive protein, ESR and WBC in acute hematogenous osteomyelitis in children. Pediatrics 1994;93:59-62.
Question 30
3 degrees Celsius and heart rate of 105 bpm. A clinical photograph, results of synovial fluid analysis, and a polarizing microscopy image are seen in Figures A through C. Synovial fluid gram stain and cultures are pending. What is the most appropriate next step in management?
Explanation
While the incidence of superimposed gout and septic arthritis is low (~1.5%),
it is reported. In the presence of crystals on aspiration, one should not rule out the possibility of septic arthritis. If there are other risk factors for infection, or the synovial WBC count is high (greater than 50,000), then empiric antibiotics should be initiated immediately after cultures are obtained. If the patient has other evidence supporting septic arthritis (positive Gram stain, purulence), emergent I&D is indicated. Even if the initial suspicion is lower, if they have
not respond to antibiotics after 24-48 hours they should undergo I&D.
Shah et al. investigated 265 crystal-positive joint aspirates in a 7-year retrospective study. They found the incidence of concomitant septic arthritis and crystal disease was 1.5% (4 cases including 2 knees, 1 hip, 1 ankle). All 4 patients that had superimposed infection had a WBC of > 50,000. They concluded that the presence of crystals in the synovial fluid cannot
conclusively rule out a septic joint.
Schuind et al. described a case report of concomitant septic arthritis and gout of the wrist. They found that cultures were positive for Staphylococcus aureus while pathological examination revealed aggregated crystals of monosodium urate.
Figure A shows tense, erythematous swelling of the right knee. Figure B is a table showing synovial fluid analysis with elevated WBC and PMN cell count characteristic of septic arthritis. Figure C shows needle-shaped negatively birefringent crystals on polarizing microscopy. Illustration A shows the synovial fluid characteristics in different disease conditions.
Incorrect Answers:
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Lead to lower patient satisfaction rates
Lead to higher patient satisfaction rates
Lead to higher likelihood the patient will take legal action against surgeon
Lead to higher likelihood the patient will change physicians
Prevent any legal action
The surgeon has provided all the elements of good communication with the patient and family. His actions will lead to improved patient satisfaction, compared to nondisclosure and attempting to push or shirk responsibility.
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise:
an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose
non-disclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
The acquired immune response mediated by the interaction between the T cell receptor and major histocompatibility complex requires which of the following first steps?
Antigen phagocytosis by T cells
Antigen processing and presentation to T cells
Antigen recognition by natural killer T cells
Antigen proliferation by polymerase chain reaction
T cell disulfide bond cleavage and enzymatic processing
The process of antigen processing and presentation is the first step of the acquired immune response. This is performed by the so called antigen presentation cells (APC) of which B cells and dentritic cells are two examples. The APC breaks down the protein antigen in a multitude of enzymatic reactions and presents key peptide sequences via the major histocompatibility complex
(MHC) receptors. Once presented on the surface of the APC, the T-cell receptor recognizes the MHC/antigen complex leading to T-cell activation. At no point in this process are antigens phagocytosed by T cells. Natural killer T cells are involved in this sequence, but not for antigen processing and presentation. Polymerase chain reaction is a laboratory tool used to amplify nucleic acid. Finally, disulfide bond cleavage is a step involved in the APCs antigen processing reaction and does not occur in T cells.
All of the following are true regarding a physician responding to a formal written complaint by a patient EXCEPT:
Complaint should be taken seriously
Written response by the physician is required
Physician mandated to retain an attorney to address the formal complaint
Patient should be supplied with contact information for the institution's patient representative department
Law mandates that the physician respond to the formal complaint
It is important for the surgeon to know how to manage a formal complaint. An attorney is not required to assist on behalf of the physician when addressing a formal complaint. All complaints must be taken seriously and the physician is required by law to respond to all formal complaints in writing. Verbal
responses to formal, written complaints are not sufficient. If a patient is filing a formal complaint it is advisable that the patient be supplied with contact information for the institution's patient representative department.
What laboratory findings would you expect to find in a patient newly diagnosed with renal osteodystrophy?
Decreased PTH secretion, hypophosphatemia, and hypocalcemia
Increased PTH secretion, hyperphosphatemia, and hypocalcemia
Decreased PTH secretion, hypophosphatemia, and hypercalcemia
Increased PTH secretion, hyperphosphatemia, and hypercalcemia
Hypophosphatemia and hypocalcemia
Renal osteodystrophy is characterized by bone mineralization deficiency due to the electrolyte and endocrine abnormalities associated with chronic kidney disease. The pathogenesis of renal osteodystrophy is multifactorial. Hypocalcemia occurs due to the inability of the damaged kidney to convert vitamin D3 into its active form, calcitriol. The hypocalcemia and lack of phosphate excretion by the damaged kidney causes hyperparathyroidism and secondary hyperphosphatemia.
Loss of function in the 25(OH) vitamin D1-alpha hydroxylase gene causes which of the following diseases?
Hyperphosphatemia
Vitamin D resistant rickets
Hereditary Vitamin D dependant rickets type I
Hereditary Vitamin D dependant rickets type II
Hypophosphatemic rickets
Loss of function mutations in the 25 (OH) vitamin D hydroxylase gene cause hereditary vitamin D dependant rickets type I. Hereditary vitamin D dependant rickets type II is caused by a defect in intracellular receptor for 1,25-(OH)2- vitamin D3. Both forms of
hereditary vitamin D dependent rickets show decreased serum calcium/phosphorous, elevated alkaline phosphatase/PTH,
but type I has a decrease in the 1,25(OH)2 vitamin D and type II shows a increase in 1,25(OH)2 vitamin D. Vitamin D resistant rickets (Familial Hypophosphatemic Rickets) is caused by a large deletion in the PHEX gene and results in low serum phosphorous, elevated alkaline phosphatase, and normal calcium. Hyperphosphatemia can be caused by mutation in the GALNT3 gene and results in elevated serum phosphate and decreased PTH/calcium.
Kato et al. describe the molecular physiology of vitamin D metabolism and the recognized gene mutations associated with various clinical manifestations of mutations in vitamin D homeostasis.
Figure A is a radiograph taken after an open reduction and internal fixation of a periprosthetic distal femur fracture. With this type of hybrid locked plate fixation, what is the difference between screw A and screw B?
Screw A can assist in fracture reduction while screw B provides a fixed angle support
Screw A provides improved axial stiffness while screw B provides a fixed angle support
Screw A can be used to reduce the plate to bone while screw B can be used to lag fracture fragments together
Screw A provides a fixed angle support while screw B can be used to reduce the plate to the bone
Screw A can be used to lag fracture fragments together and screw B increases the plate bone frictional stability
Locking screws provide a fixed angle support and can improve fixation in osteoporotic bone while nonlocking screws can be used to reduce the plate to the bone, lag fracture fragments together and increase the plate bone frictional stability. "Hybrid" locked plate fixation utilizes both screw types in order to assist with difficult fracture fixation such as when there is a short metaphyseal segment and osteoporotic bone.
Zura et al discusses the biomechanical and biological advantages offered by locked plate fixation.
Using levels of evidence in research studies, which of the following represents a level II study?
Retrospective case control study
Prospective cohort study
Case report of 3 patients with the same disease
High-quality randomized prospective clinical trial
The opinion of a review panel at the annual AAOS meeting
Level II Evidence includes prospective cohort studies. There are 5 levels of evidence in clinical research. Level I includes randomized clinical trials. Level II includes prospective cohort studies. Level III includes case control studies AND retrospective cohort studies. Level IV includes case series. Level V evidence includes expert opinion, case reports, and personal observation. The cited reference by Bernstein et al is an excellent review of Evidence Based Medicine (EBM) and describes the 5 step process of making medical decisions based on the available, and often limited, evidence. These steps include: 1) Formulate answerable questions. 2) Gather the evidence. 3) Appraise the evidence. 4) Implement the evidence. 5) Evaluate the process. The reference by Spindler et al is another review article that discusses the different levels of evidence for different study types.
All of the following are true regarding the assessment of bone mineral density EXCEPT?
Bone mineral density loss is not apparent on standard radiographs until 30% to 40% of mineral is lost
Dual energy x-ray absorbtiometry (DEXA) is only able to measure mineralization of the axial skeleton
Single photon absorbtiometry allows for the analysis of bone mineralization in the appendicular skeleton alone
Quantitative computed tomography (QCT) is associated with 10 times the radiation of a DEXA scan
MRI allows for accurate discrimination of normal bone from osteopenic bones
without exposing the patient to ionizing radiation
Dual energy x-ray absorbtiometry (DEXA) scans allow for accurate assessment of bone mineralization in both the axial and appendicular skeleton.
Over the last decade, DEXA has become a safe, cost-effective and reliable method to quantify bone mineral density. The World Health Organization (WHO) has adopted DEXA derived BMD measurements to define normal bone, osteopenia, and osteoporosis in the adult and paediatric population. The typical DEXA analysis therefore reports a Z-score, which is the number of standard deviations (SDs) that a patient's BMD is above or below the mean value for persons of the patient's age and sex. The T score is the number of SDs the patient's BMD is either above or below the mean value for young patients of the same gender.
Tortolani et al. provide an overview of the techniques used to assess bone mineral density, the pathophysiology of osteopenia, and the evaluation and treatment options for the general pediatric population as well as for patients with specific pediatric disorders. The authors encouraged orthopaedic surgeons to understand the problems of osteopenia in both otherwise healthy children and children with chronic disorders.
Binkovitz & Henwood provide a review of DEXA technique and interpretation with emphasis on the considerations unique to pediatrics. They found that changes in bone size over time, as occurs in normal pediatric development, confound DXA interpretation. This is one of the major limitations in the use of pediatric DXA. However, attempts to correct for or to circumvent this limitation have been proposed and show promise in improving DXA interpretation and
our understanding of bone physiology.
T-score according to the World Health Organization (WHO): A T- score of -1.0 or above is normal bone density.
A T-score between -1.0 and -2.5 means you have low bone density or osteopenia.
A T-score of -2.5 or below is a diagnosis of osteoporosis.
Incorrect Answers:
A mother brings her 4-year-old daughter to your clinic for evaluation of knocked knees and short stature. On exam, the patient ambulates with a circumduction gait pattern and frequently falls. Plain radiographs are displayed in Figure A. Laboratory data is obtained and notable for calcium 9.1 mg/dL (RR 8.5-
Question 31
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520.
Question 32
A 40 year-old-man was involved in a motor vehicle accident and sustained the pelvic injury seen in Figures 24a and 24b. Definitive management of the injury should consist of reduction by
Explanation
REFERENCES: Tile M: Management of pelvic ring injuries, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 168-202.
Kabak S, Halici M, Tuncel M, et al: Functional outcome of open reduction and internal fixation for completely unstable pelvic ring fractures (type C): A report of 40 cases. J Orthop Trauma 2003;17:555-562.
Question 33
A B
Explanation
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
Question 34
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?
Explanation
REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.
Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.
Question 35
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively? Review Topic

Explanation
Question 36
A patient presenting with scapulothoracic dissocation and ipsilateral extremity neurologic injury is most likely to have which of the following outcomes?

Explanation
The referenced study by Althausen et al found that outcomes from this injury were: a flail extremity in 52%, early amputation in 21%, and death in 10%.
The other referenced study by Ebraheim et al found that 12/15 patients had a complete brachial plexus injury and that none recovered any function (the other 3 patients died in the acute period).
Question 37
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 38
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?
Explanation
REFERENCE: Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 39
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, p1550.
Benzel EC (ed): Spine Surgery Techniques, Complication Avoidance and Management. New York, NY, Churchill Livingstone, 1999, p 190.
Question 40
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 41
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?
Explanation
REFERENCES: Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: A user-friendly technique. Foot Ankle 1992;13:367-377.
Mann RA: Hallux rigidus. Instr Course Lect 1990;39:15-21.
Question 42
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 43
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 44
When performing a posterior cruciate-substituting total knee revision, trial components are inserted. The knee comes to full extension but is tight in flexion. The surgeon should consider
Explanation
In this scenario, the extension gap is normal and the flexion gap is tight. Increasing the flexion gap without changing the extension gap can be performed by downsizing the femoral component or adding posterior slope to the tibia resection. Flexing the femoral component tightens the flexion gap. Decreasing the tibial component thickness loosens the flexion and extension gaps. Resecting more distal femur only loosens the extension gap.

CLINICAL SITUATION FOR QUESTIONS 4 THROUGH 7
Figure 4 is the radiograph of a 73-year-old woman who returns for her annual follow-up 14 years after undergoing total hip arthroplasty. She denies pain and has no discomfort upon examination.
Question 45
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?

Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 46
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
Explanation
Question 47
The flexor hallucis longus tendon is at greatest risk of injury with a lateral-to-medial drill or screw during fixation of what structure?

Explanation
Question 48
intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
Explanation
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is
positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
Ig antibodies at the neuromuscular (NM) junction
Decreased release of acetylcholine at the NM junction
Decrease in myelin sheath of axonal nerves with loss of NM junction
Absence of dystrophin with excess calcium at sarcolemma
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
Analysis of variance (ANOVA)
Regression analysis
Student t test
Mann-Whitney U test
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
Which of the following is the mechanism of action of aspirin?
Inhibition of vitamin K-dependent carboxylation
Inhibition of factor Xa through antithrombin binding
Binding of cyclooxygenase (COX)-1 and COX-2
Direct thrombin inhibition
Glycoprotein IIIb agonist binding
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Intermediate doses (650 mg to 4 g/day) inhibit COX-1 and COX-2, blocking prostaglandin (PG) production, and have analgesic and antipyretic effects. Illustration A shows the mechanism of action of aspirin.
InCORRECT Answers: 1,2,4,5: Aspirin does not have any of these mechanisms of action.
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Crossover design trial
Parallel design trial
Cohort study
Case series
In a parallel design trial, participants are randomized to 2 or more groups, each of which receives a different treatment or intervention. For example, Group A receives the drug and Group B receives the placebo. This type of
design allows for comparison between groups. In a crossover design clinical trial, both groups receive both interventions over a defined time period. For example, Groups A and B both receive the drug as well as the placebo. This allows for within-participant comparisons. In a cohort study, patient groups are followed over time on the basis of having or not having received an exposure. Cohort studies are not randomized. In a case series, patients often receive a particular treatment and the outcomes are then examined.
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Increase calcium and vitamin D intake
Avoid all nonsteroidal anti-inflammatory drugs (NSAIDs)
Maintain smoking cessation
Engage in early physical therapy to strengthen the trunk musculature
Smoking is the biggest risk factor for nonunion and should be strictly avoided. NSAIDs interfere with bone healing, but not as strongly as smoking. Early mobilization would potentially stress the construct, inducing movement that leads to nonunion. Without history of calcium and vitamin D deficiency, increasing intake would not decrease the risk of nonunion.
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
occurs earlier.
occurs later.
is prolonged.
is shortened.
Compared to similar autograft, allograft tissue demonstrates a prolonged inflammatory response, slower rate of biological incorporation and remodeling, and a higher proportion of large-diameter collagen fibrils. Native ACL inserts
into bone through a transition of 4 distinct zones: tendon, unmineralized fibrocartilage, mineralized fibrocartilage, and bone. This transition is not reproduced with tendon grafts, which instead heal with interposed fibrovascular scar at the graft-tunnel interface. The scar rapidly remodels to form perpendicular fibers resembling Sharpey fibers and, eventually, mature bone growth into the outer portion of the graft. The intra- articular portion of allograft undergoes an initial phase of necrosis followed by repopulation by host synovial cells into the acellular collagen scaffold.
Revascularization and maturation complete the ligamentization of graft tissue.
A researcher decides she wants to look at the current total number of patients who have methicillin-resistant Staphylococcus aureus (MRSA) infections in a hospital on 1 particular day. What is the researcher measuring?
Correlation coefficient of MRSA
Prevalence of MRSA
Incidence of MRSA
Relative risk of MRSA
The prevalence of a disease is a measure of the number of cases of a disease at or during a specific time point or time period. In this case, the researcher wants to know the prevalence of disease on a given day. Incidence measures new cases of a disease or event per unit of time. Correlation coefficient is a measure of how 2 things correlate with one another, while relative risk is a statistical outcome that is often used in case-control or cohort studies to provide a measure of the risk of a particular disease occurring when a certain exposure has already occurred.
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
protein C and S.
vitamin K.
von Willebrand factor.
factor VIII.
Hemophilia A is an X-linked recessive deficiency of factor VIII that can lead to significant bleeding problems including recurrent spontaneous hemarthroses that can lead to synovitis and joint destruction. von Willebrand disease is a lack of von Willebrand factor that leads to decreased platelet aggregation; more commonly patients have mucosal bleeding and not hemarthroses. Vitamin K deficiency is not hereditary; it is typically attributable to inadequate dietary intake, malabsorption, and loss of storage sites from hepatocellular disease. Protein C and S deficiencies are autosomal-dominant diseases that lead to thrombosis, not bleeding, as protein C and S shut off thrombin formation.
What is the recommended optimal timing of presurgical antibiotic administration to prevent infection in patients undergoing total joint replacement surgery?
Within 1 hour before incision
Within 2 hours before incision
Immediately after incision
Within 1 hour after incision
The current recommendation for antibiotic prophylaxis for major orthopaedic surgical procedures is to administer intravenous antibiotics within 1 hour of surgical incision. Redosing of antibiotics should occur 3 to 4 hours after the initial dose for procedures that extend beyond 3 to 4 hours. Little evidence supports postsurgical antibiotic use beyond 24 hours. As you move beyond 1 hour from time of administration of antibiotics, risk for infection increases and rates of bacterial cell death decline. It is not acceptable to
administer presurgical antibiotics after incision.
Bacterial resistance to antibiotics in biofilm is an example of
avoidance.
decreased susceptibility.
inactivation.
mutation. CORRECT answer: 1
Three basic mechanisms of antibiotic resistance have been identified: avoidance, decreased susceptibility, and inactivation. Biofilm formation is a classic example of avoidance, whereby the biofilm creates a physical barrier to the antibiotic. Bacteria can decrease their susceptibility to antibiotics by mutating the antibiotic target or generating a mechanism to inactivate the antibiotic. Biofilm formation develops when a sufficient mass of bacteria forms on a surface. The cell-to-cell signaling becomes sufficient to activate transcription of genes needed for biofilm formation in a process known as quorum sensing. Once the bacteria produce a mature biofilm, they enter a greatly reduced or stationary phase of growth. Lastly, high-shear
environments seem to stimulate biofilm production.
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Promotes reabsorption of phosphate in the renal tubules
Interferes with osteoclast maturation
Interferes with intestinal absorption of calcium
Upregulates osteoblast formation
Calcitonin is a hormone that reduces serum calcium concentration by directly interfering with osteoclast maturation via receptors. Calcitonin inhibits phosphate reabsorption and decreases calcium reabsorption in the kidneys. By attenuating cartilage breakdown and stimulating cartilage formation via inhibitory pathways of matrix metalloproteinases, calcitonin also has a
chondro-protective effect on articular cartilage. Calcitonin has no major effects on intestinal absorption of calcium, but may aid in small-bowel secretion of sodium, potassium, chloride, and water. Calcitonin also has no receptor effect on osteoblasts.
A cartilage water content increase is the hallmark of which
osteoarthritis stage?
Prearthritis
Early
Late
Terminal
The first stage of osteoarthritis is marked by an increase in water content secondary to disruption of the matrix framework. This is followed by an increase in chondrocyte anabolic and catabolic activity in response to tissue damage. Wnt-induced signal protein 1 increases chondrocyte protease expression. Failure to restore tissue balance ultimately leads to continued destruction and osteoarthritis. One hallmark of osteoarthritic cartilage is a reduced repair mechanism attributable to decreased chondrocyte response to growth factor stimulation (transforming growth factor-alpha and insulin-like growth factor-1).
Mitochondrial dysfunction and increased production of reactive oxygen species may promote cell senescence, a progressive slowing of cellular activity. Microscopic evidence of cartilage degeneration begins with fibrillation of the superficial and transition zones, followed by disruption of the tidemark by subchondral blood vessels and eventual subchondral bone remodeling. This process ultimately leads to cartilage degradation with decreased water content in the late and terminal phases of osteoarthritis.
What is the plasma half-life of warfarin?
1 to 2 hours
4 to 6 hours
12 to 18 hours
36 to 42 hours
Warfarin, which is dosed daily, can take 72 to 96 hours to reach therapeutic levels. It has a plasma half-life of 36 to 42 hours. Low-molecular heparins have a plasma half-life of 4 to 5 hours, and fondaparinux has a half-life of 17 to 21 hours. Warfarin will not affect the International Normalized Ratio (INR) until 2 to 3 days after it is given. Patients on chronic warfarin therapy should
have treatment stopped 3 to 5 days before elective surgery to allow the INR to normalize.
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has Factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Type of surgery, age, and BMI
Type of surgery, hypercholesterolemia, and age
Age, BMI, and hypercholesterolemia
BMI, type of surgery, and hypercholesterolemia
Risk stratification is one of the most critical clinical evaluations before undergoing total joint arthroplasty. Many factors have been identified to increase risk for venous thromboembolism (VTE). The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormonal replacement therapy.
Hypercholesterolemia is not a risk factor for thromboembolic disease.
DNA replication occurs during which phase of the cell cycle?
M
S
R
G1
G2
The cell cycle consists of four distinct phases: initial growth (G1), DNA replication/synthesis (S), a gap (G2), and mitosis (M) (see illustration).
The G1 and G2 phases of the cell cycle represent the “gaps” or growth phases in the cell cycle that occur between DNA synthesis and mitosis. G0 cells are in a stable state and have not entered the cell cycle. During the S phase, the DNA is synthesized and replicated. During the M phase or mitosis, all genetic material divides into two daughter cells.
The cells are diploid (2N) in the G0 and G1 phases. The cells become tetraploid (4N) at the end of S and for the entire G2 phases. There is no R phase in the cell cycle.
What antithrombotic agent is a selective factor I0a inhibitor?
Warfarin
Low-molecular-weight heparin
Rivaroxaban
Aspirin
Rivaroxaban is a selective factor I0a inhibitor. Aspirin is a cyclooxygenase inhibitor. Low-molecular-weight heparin is a nonspecific anticoagulant. Warfarin is a vitamin K antagonist and reduces production of clotting factors II, VII, IX, and X.
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic
disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee
Arthroplasty, include
use of mechanical prophylaxis (eg, pneumatic calf compressors) while in the hospital.
oral warfarin with a goal INR between 2.0 and 3.0.
low-dose warfarin for 3 weeks postsurgically beginning 48 hours after surgery.
no prophylaxis because this patient already is partially anticoagulated secondary to her liver disease.
The 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty, recommends the use of mechanical prophylaxis for patients at increased risk
for bleeding (including those with liver disease or hemophilia). This recommendation is the consensus of the workgroup that established these guidelines because there was insufficient evidence to justify a stronger recommendation in this clinical scenario. The other responses use no prophylaxis or pharmacological prophylaxis. Pharmacological prophylaxis is not recommended in patients who are at increased risk for bleeding.
The pharmacokinetics of which deep venous thrombosis (DVT) prophylactic agent are affected by liver function and dietary intake?
Dalteparin
Warfarin
Fondaparinux
Enoxaparin
Warfarin is an oral vitamin K antagonist that is rapidly absorbed from the gastrointestinal tract. It accumulates in the liver, where it is metabolized and excreted. The pharmacokinetics of warfarin can be affected by certain drugs or disease states that influence liver function. Fondaparinux is a synthetic factor Xa inhibitor that is eliminated through the kidneys. Both Dalteparin and Enoxaparin are low-molecular-weight heparins that activate antithrombin and inhibit factors Xa and IIa. Like Fondaparinux, they are eliminated through the kidneys and should be used with caution in patients with kidney disease.
What infection-control measure has been shown to have the most notable impact in reducing surgical-site infections?
Intravenous antibiotic administration within 1 hour of surgical incision
Screening and decolonization of patients colonized with methicillin-resistant
<em>Staphylococcus aureus</em>
Horizontal laminar flow
Use of enclosed body exhaust suits
Timely administration of prophylactic antibiotics is the most important factor shown to decrease surgical-site infections. The use of horizontal laminar flow and body exhaust suits has not been shown to significantly affect infection rates.
The resistance to pullout of a screw in osteoporotic bone is increased by all of the following EXCEPT?
Placement parallel to the trabecular pattern
Purchase in cortical bone
Use of a fixed angle (locking screw construct)
Tapping prior to screw placement
Augmentation with polymethylmethacrylate
Of the options listed, tapping prior to screw placement is the only variable that does not increase the pullout strength of a screw in osteoporotic bone.
Cornell reviews internal fixation in osteoporotic bone. According to this article, the quality of the bone is the primary determinant of the holding power of an individual screw. Other factors that increase the pullout strength include fixation in cortical bone (cortical bone has greater mineral density and, therefore, greater resistance to screw pullout than trabecular bone), screws placed parallel to the trabecular pattern, and screw fixation augmented with PMMA. The addition of a locking plate will also increase the resistance to failure by creating a fixed angle construct. Tapping prior to placement of the screw has not been shown to increase resistance to pullout, on the contrary studies have shown
this decreases resistance to pullout.
Turner et al examined the holding strength of small and large diameter screws in healthy bovine and diseased human bone. They found the screw diameter, trabecular orientation of the bone, and mineral content of the bone all affect the holding strength. A larger diameter screw, parallel placement to the trabecular pattern, and purchase in bone with a higher density all increase the holding strength.
Gigantism affects which region of the growth plate labeled in Figure A?
A
B
C
D
E
Gigantism, like achondroplasia, affects the proliferative zone (Region C of Figure A) of the growth plate. In Figure A, Region A is the epiphysis, Region B is the resting zone, Region D is the hypertrophic zone, and Region E is the metaphysis. Illustration A is another depiction of the physis which is labeled. Gigantism is typically caused by a pituitary adenoma which over secretes growth hormone. Its effect on the proliferative zone results in bone overgrowth and excessive height and limb length. Acromegaly may also be
caused by a pituitary adenoma that over secretes growth hormone, but has its effect once the physis has closed.
Plain radiographs do not provide an accurate assessment of bone mineral density (BMD) until what percentage of mineral has been lost?
Question 49
Rupture of the structure shown in the axial cross and the sagittal sections in Figures 100a and 100b causes weakness in

Explanation
The structure identified is the distal biceps tendon. Rupture of this tendon causes weakness in both flexion and supination. The biceps tendon does not affect extension or pronation.
RECOMMENDED READINGS
Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. PubMed PMID: 3972865. View Abstract at PubMed
Mazzocca AD, Spang JT, Arciero RA. Distal biceps rupture. Orthop Clin North Am. 2008 Apr;39(2):237-49, vii. doi: 10.1016/j.ocl.2008.01.001. Review. PubMed PMID: 18374814. View Abstract at PubMed
Question 50
Figures below depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?

Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 51
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 52
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
Explanation
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 53
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 54
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 55
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals

Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 56
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
REFERENCES: Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998,
pp 421-454.
Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 57
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Explanation
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 58
A 22-year-old man sustained a shoulder dislocation while playing collegiate football at age 18. Since that time, he has dislocated the shoulder three more times despite physical therapy. His last dislocation occurred 4 weeks ago while sleeping. What is the most appropriate management for this patient? Review Topic
Explanation
Question 59
Which of the following is an FDA approved adjunctive treatment for an acute open tibia fracture being treated with an intramedullary nail?
Explanation
Open tibial shaft fractures can present many treatment challenges. Although its use remains somewhat controversial, rhBMP-2 has been shown to have many positive effects when used to treat acute open tibia fractures. These benefits include accelerated early fracture healing, decreased rates of hardware failure, decreased need for subsequent bone grafting procedures, and decreased infection rates. rhBMP-2 does have FDA approval specifically for use in open tibia fractures being treated with an intramedullary nail.
Alt et al. present a comparison of patients with Grade III open tibia fractures treated
with un-reamed nails with or without rhBMP-2. They found significant decreases in need for secondary interventions such as bone grafting or nail exchange. Mean time to fracture healing was less in the rhBMP-2 group, but this difference was not statistically significant.
Govender et al. present a prospective randomized study of 450 patients with open tibia fractures treated with an intramedullary nail with or without rhBMP-2. They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Wei et al. provide a meta analysis regarding use of rhBMP-2 in open tibia fractures. Due to decreased rates of secondary interventions they estimated a net savings of
$6,000 per case when rh-BMP2 was used. They found no significant difference in rates of infection, postoperative pain, hardware failure, or fracture healing at 20 weeks.
Incorrect answers:
Question 60
-What leads to muscle hypertrophy?
Explanation

Question 61
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management? Review Topic

Explanation
Question 62
A 14-year-old boy is involved in a motor vehicle accident and sustains the injury shown in Figures 18a and 18b. What is the most likely diagnosis? Review Topic

Explanation
Question 63
Figures 47a and 47b show the CT scans of a patient who reports persistent pain in the sinus tarsi following a fall. The avulsion fracture fragment remains attached to what ligament?
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, p 192.
Robbins MI, Wilson MG, Sella EJ: MR imaging of anterosuperior calcaneal process fractures. Am J Roentgenol 1999;172:475-479.
Question 64
Which of the following studies has the highest sensitivity and specificity in diagnosis of osteonecrosis of the femoral head?
Explanation
REFERENCES: Steinberg ME: Early diagnosis, evaluation, and staging of osteonecrosis, in Jackson DW (ed): Instructional Course Lectures 43. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 513-518.
Glickstein MF, Burk DL Jr, Schiebler ML, et al: Avascular necrosis versus other diseases of the hip: Sensitivity of MR imaging. Radiology 1988;169:213-215.
Question 65
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
REFERENCES: Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Elliot DC: An evaluation of the end points of resuscitation. J Am Coll Surg 1998;187:536-547.
Question 66
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 67
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 68
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, Kojimoto H, Shimomura Y: Lumbar disc herniation in children. J Pediatr Orthop 1990;10:394-396.
Question 69
-A 75-year-old woman fell at home and sustained the injury seen in Figures 249a through 249c. What is the most appropriate treatment option?
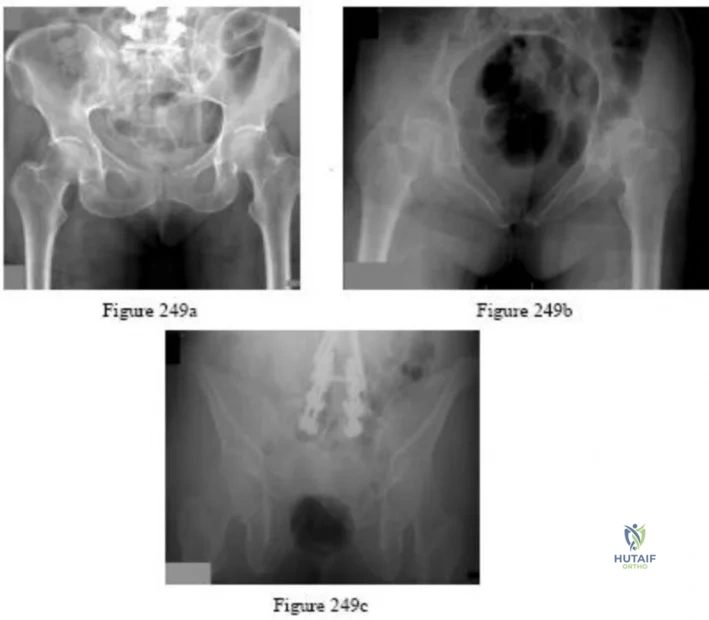
Explanation

Question 70
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 965-981.
Question 71
A morbidly obese 80-year-old woman presents with back pain for 2 months. Sagittal T2-weighted, sagittal T1-weighted, coronal short tau inversion recovery (STIR) images are shown in Figures A through C, respectively. Which of the following statements is true of her diagnosis? Review Topic

Explanation
The MR signs suggestive of a benign, osteoporotic VCF include band-like low T1 signal, fluid sign, retropulsion of a vertebral bone fragment. Acute fractures show low signal on T1-weighted and high signal on T2-weighted and STIR images. The MR signs suggestive of malignant VCF include complete replacement of normal marrow signal, convex posterior vertebral border, pedicle involvement, focal paraspinal mass and epidural mass.
Kim et al. performed a literature review on management of the osteoporotic spine. They concluded that nonsurgical management should focus on pain control and maximizing function. Surgery remains controversial and should be reserved for those who fail nonoperative management. Surgical options include vertebroplasty, balloon tamp reduction, and decompression and instrumented fusion with structural graft and multiple fixation points.
Spivak et al. discussed percutaneous treatment of VCF. They recommend vertebroplasty for patients with unremitting pain and little deformity as it is less costly and does not require general anesthesia. They recommend kyphoplasty for cases with
greater vertebral collapse, especially subacute fractures where partial healing may hinder postural fracture reduction.
Figure A is a T2-weighted sagittal MR image showing a fluid-filled cleft ("fluid sign"). Figure B is a T1-weighted sagittal MR image showing loss of intensity (black) consistent with vertebral body edema. Figure C is a coronal STIR image showing the fluid-filled vertebral body cleft. An incidental renal cyst is noted. Illustration A shows different patterns of band-like signal abnormality on T1-weighted imaging. The black region represents low signal intensity (edema). Illustration B is a sagittal STIR image showing the MR fluid sign. Illustration C shows the band like signal abnormality on T1-weighted imaging. Illustration D shows metastatic disease with complete replacement of normal marrow intensity and diffuse convexity of the posterior vertebral border.
Incorrect
Question 72
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
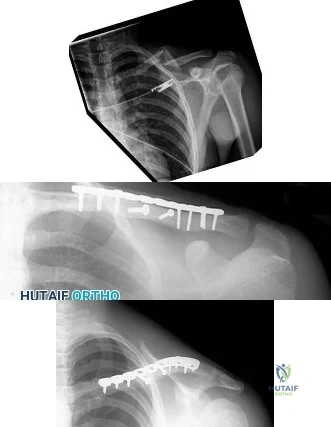
Explanation
Question 73
A 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
Question 74
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 75
Which of the following best characterizes the injury shown in Figure 53? Review Topic

Explanation
Question 76
Figure 48 shows a current lateral radiograph of a 23-year-old man who sustained a closed femoral diaphyseal fracture 5 months ago. Treatment consisted of placement of a retrograde femoral nail for the femoral fracture. The patient now reports a sudden onset of pain in the midthigh and cannot bear weight on his leg. Management should consist of

Explanation
In Webb, et al. one hundred five consecutive patients with a diagnosis of delayed union (61 patients) or nonunion (44 patients) of the femoral shaft from February 1968 to November 1983 were managed by intramedullary reaming and nailing. The procedure was accomplished by closed techniques in 82 of the cases. Adequate follow-up study was obtained in 101 patients; all but four showed clinical and radiologic union at an average of 20 weeks following the procedure, with an overall union rate of 96%. The four patients whose fractures failed to consolidate with this treatment had repeat procedures with placement of thicker nails, and all subsequently healed.
The fracture pictured for this question is an oblique, distal 1/3 diaphyseal femur fracture with a butterfly fragment, an axially and rotationally unstable fracture configuration. The clinical history and x-ray are consistent with delayed union, therefore response #4 is the only sensible management option.
Question 77
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 78
Figures 48a and 48b are the axial and sagittal T1-weighted MR images of the L4-5 disc level of a 38-year-old man. He is symptomatic from the pathology shown. A surgeon would expect the neurological findings to include

Explanation
The pathology shown in the MR images is a right-sided far lateral herniated nucleus pulposus at L4-5, which, if symptomatic, would cause a radiculopathy of the exiting root, L4. A more common posterolateral herniation at L4-5 would cause irritation of the traversing root, L5. The L4 root has a sensory distribution over the anterior thigh that extends along the anterior shin but does not tend to reach the toes. The motor distribution is to the quadriceps and anterior tibialis muscles, with the predominant reflex effect being the patella reflex. The L5 root has a sensory distribution to the first dorsal web space of the foot, motor distribution to the EHL, and no specific reflex.
RECOMMENDED READINGS
Standaert CJ, Herring SA, Sinclair JD. The patient history and physical examination: Cervical, thoracic, and lumbar. In: Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, eds. Rothman-Simeone The Spine. Vol 1. 5th ed. Philadelphia, PA: Saunders Elsevier; 2006:171-186.
Bono CM, Wisneski R, Garfin SR: Lumbar disc herniations. In: Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, eds. Rothman-Simeone The Spine. Vol 1. 5th ed. Philadelphia, PA: Saunders Elsevier; 2006:967-991.
Question 79
Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On the contralateral side, he reports pain and restricted ankle range of motion. Management should consist of

Explanation
Question 80
Figure 22 reveals what anatomic variant of the lumbar spine?
Explanation
REFERENCES: Brault JS, Smith J, Currier BL: Partial lumbosacral transitional vertebra resection for contralateral facetogenic pain. Spine 2001;26:226-229.
Quinlan JF, Duke D, Eustace S: Bertolotti’s syndrome: A cause of back pain in young people.
J Bone Joint Surg Br 2006;88:1183-1186.
Whelan MA, Feldman F: The variant lumbar pedicle. Neuroradiology 1982;22:235-242.
Question 81
The newborn foot deformity seen in Figures 64a and 64b should initially treated with Review Topic

Explanation
Question 82
Figures 1 and 2 are the MRI scans of a 57-year-old man who dislocated his left shoulder after a fall while playing tennis. On examination, he had full passive shoulder range of motion, but he was unable to actively elevate his injured shoulder. Sensation was intact to light touch over the lateral shoulder. What is the most likely etiology of his shoulder weakness?
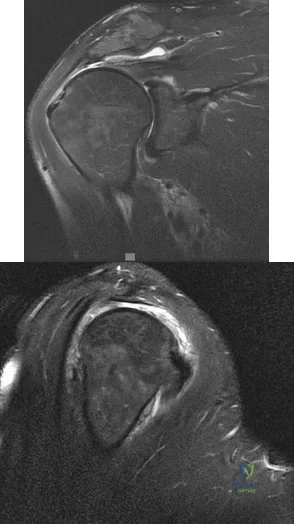
Explanation
Question 83
Figures 18a through 18c show injuries sustained by a 22-year-old woman after falling 45 feet while mountain climbing. After being airlifted to the nearest trauma center, her arterial blood gas was 7.21, pO2 84, pCO2 48, and delta base -11 mmol/L. Her Hgb is 8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?

Explanation
prolonged, invasive surgery. Upper extremity fractures are best managed acutely with splints in this clinical setting. Definitive fracture fixation should be delayed until the patient is adequately resuscitated.
Question 84
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50? Review Topic
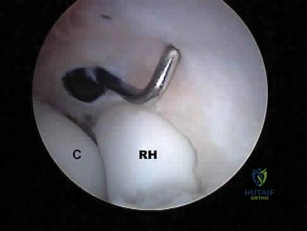
Explanation
Question 85
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 86
Figure 20 shows the clinical photograph of a man who has had diabetes mellitus controlled with oral medication for the past 10 years. He wears soft-soled shoes and only uses leather-soled shoes for important business meetings. Examination reveals palpable dorsalis pedis and posterior tibial pulses, although they are somewhat diminished. He is insensate to pressure with the Semmes-Weinstein 5.07 monofilament. The ulcer heals after treatment with a full contact cast. What is the best course of action at this time?
Explanation
REFERENCES: Pinzur MS, Kernan-Schroeder D, Emmanuele NV, et al: Development of a nurse-provided health system strategy for diabetic foot care. Foot Ank Int 2001;22:744-746.
Pinzur MS, Shields N, Goelitz B, et al: American Orthopaedic Foot & Ankle Society shoe survey of diabetic patients. Foot & Ankle Int 1999;20:703-707.
Reiber GE, Smith DG, Wallace CM, et al: Effect of therapeutic footwear on foot reulceration in patients with diabetes: A randomized controlled trial. JAMA 2002;287:2552-2558.
Question 87
A 45-year-old man underwent unipolar hemiarthroplasty reconstruction using cementless fixation for nontraumatic osteonecrosis of the femoral head 5 years ago. He now reports buttock and groin pain that is associated with loading activities. What is the most likely cause of his pain?
Explanation
REFERENCES: Steinberg ME, Corces A, Fallon M: Acetabular involvement in osteonecrosis of the femoral head. J Bone Joint Surg Am 1999;81:60-65.
Dalldorf PG, Banas MP, Hicks DG, Pelligrini VD Jr: Rate of degeneration of human acetabular cartilage after hemiarthroplasty. J Bone Joint Surg Am 1995;77:877-882.
Question 88
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 89
Which of the following best describes the relationship of the anterior tibial artery and dorsalis pedis artery to the extensor hallucis longus (EHL) tendon as they progress from the level of the ankle to the dorsum of the foot?
Explanation
REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 90
Varus malalignment after a talar neck fracture with medial comminution causes a decrease in what motion?

Explanation
Herscovici et al review the appropriate management of complex ankle and hindfoot injuries in this instructional course lecture.
Daniels et al performed a cadaveric study where they osteotomized the talar neck and then studied ankle motion with and without removal of a medially based wedge of bone. They found that subtalar eversion was specifically decreased.
Sanders et al found that secondary reconstructive procedures following talar neck fractures were most commonly performed to treat subtalar arthritis or misalignment.
Question 91
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?
Explanation
REFERENCES: Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
Lubowitz JH, Elson WS, Guttmann D: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86-92.
Question 92
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
Question 93
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Explanation
Question 94
Nonossifying fibroma
Explanation
Early osteomyelitis and septic arthritis appear as normal bony anatomy on radiographs, with perhaps only soft-tissue swelling seen. Radiographic changes with metaphyseal erosion appear in a delayed fashion, often after 7 or more days in indolent infections, but may present earlier in association with virulent infections such as methicillin-resistant Staphylococcus aureus. Osteoid osteoma has a radiolucent small nidus that may be difficult to see on radiograph; however, chronic cases cause marked cortical hypertrophy. Unicameral bone cysts are expansile metaphyseal lesions that are never wider than the physis. They are symmetric, well circumscribed, and can have cortical thinning. When fractures through the cyst are
present, the fallen leaf sign is visible as cortical fragments fall to the bottom of the cyst. Nonossifying fibromas are eccentric metaphyseal lesions with scalloped borders.
Question 95
Osteoarthritic cartilage is characterized by decreased
Explanation
Chondrocytes in OA are much more metabolically active than those of normal cartilage. Studies reveal measuring the levels of utilization on sulfate and H-glucosamine informing components of cartilage matrix. The amount of DNA also rises in OA cartilage most noticeable at the articular chondrocyte.
The synthesis of hyaluronate increases. Recent data suggests 1) hyaluronate that is synthesized is abnormal and, hence, does not allow aggregation; or 2) The excess synthesis is a response to a rapid degradation of synthesized product. This is in light of the fact that synthesis increases, yet concentration of hyaluronate decreases.
The correct answer is that proteoglycan content decreases. The synthesis of proteoglycan increases in OA, but due to the increased rate of breakdown of proteoglycan there is a net result of lowered proteoglycan content.
Question 96
Figure 47 shows the radiograph of a 2-day-old girl who has been referred for swelling and limited use of the right upper extremity. The second of twins, the infant was breech and delivered with forceps at age 38 weeks, weighing 5.37 lb. Difficulty in moving the arm was noted shortly after birth. Examination shows no active motion of the shoulder, elbow, or wrist. Active finger flexion and extension are present. The elbow is mildly swollen, and passive motion shows lack of full extension of 20°, lack of full flexion of 15°, and no restriction of pronation or supination. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH, Wilkins KE: Fractures involving the entire distal humeral physis, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, vol 3, pp 790-801.
Dias JJ, Lamont AC, Jones JM: Ultrasonic diagnosis of neonatal separation of the distal humeral epiphysis. J Bone Joint Surg Br 1988;70:825-828.
Gruel CR, Sullivan JA: Transcondylar fractures of the distal humerus, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 199-209.
Question 97
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
Explanation
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
distal femoral varus osteotomy.
osteoarticular transplant to the lateral femoral condyle.
unicondylar arthroplasty.
high tibial osteotomy.
Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
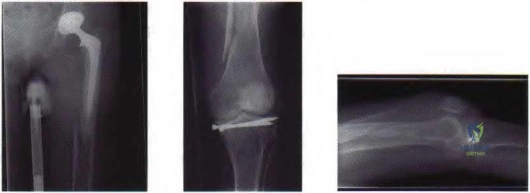
Figure 25a Figure 25b Figure 25c
Question 98
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. The injured structure is composed of an

Explanation
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 99
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
Explanation
Cauda equina syndrome is a lower-motor neuron deficit. Hyperreflexia, clonus, and other upper-motor neuron findings would not be seen. Saddle anesthesia, motor weakness, and neurogenic bladder are elements critical to the diagnosis of cauda equina syndrome.
RECOMMENDED READINGS
Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. View Abstract at PubMed
Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
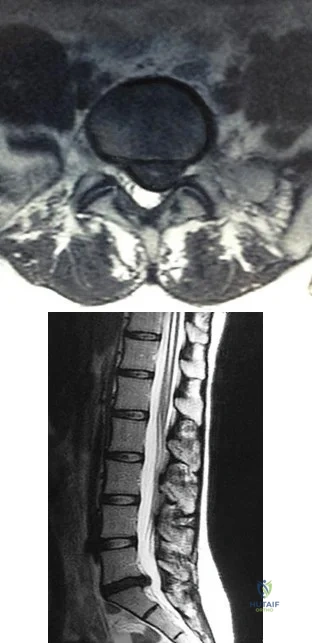
A B
Question 100
Figures 129a through 129b are the radiographs and MRI and CT scans of the lumbar spine of a 10-yearold premenarchal girl who has back pain and scoliosis. What is the most likely etiology of her scoliosis?

Explanation

