Full Question & Answer Text (for Search Engines)
Question 1:
A 25-year-old male is brought to the emergency department after a high-speed motorcycle collision. He is hemodynamically unstable. A pelvic binder is appropriately placed. Radiographs reveal a rotationally unstable but vertically stable pelvic ring injury with symphyseal widening greater than 2.5 cm (APC-II pattern). Which of the following ligaments is predominantly disrupted at the sacroiliac joint in this specific injury pattern?
Options:
- Anterior sacroiliac ligament
- Posterior sacroiliac ligament
- Sacrotuberous ligament
- Sacrospinous ligament
- Iliofemoral ligament
Correct Answer: Anterior sacroiliac ligament
Explanation:
An Anteroposterior Compression Type II (APC-II) injury involves diastasis of the pubic symphysis > 2.5 cm, with disruption of the anterior sacroiliac, sacrotuberous, and sacrospinous ligaments. The posterior sacroiliac ligaments remain intact, maintaining vertical stability. Thus, at the sacroiliac joint, the anterior sacroiliac ligament is the one disrupted.
Question 2:
A 12-year-old obese boy presents with 3 weeks of vague knee pain and a new inability to bear weight on the right leg. On physical examination, the affected leg is resting in external rotation. What is the most significant clinical risk factor for the development of avascular necrosis (AVN) in this patient's condition?
Options:
- Duration of symptoms prior to presentation
- Degree of initial slip angle
- Unstable nature of the slip
- Patient's body mass index
- Concomitant endocrine disorder
Correct Answer: Unstable nature of the slip
Explanation:
The patient has a Slipped Capital Femoral Epiphysis (SCFE). The inability to bear weight, even with crutches, defines an 'unstable' SCFE according to Loder's classification. Unstable SCFE carries a significantly higher risk of avascular necrosis (nearly 47%) compared to stable SCFE (less than 10%).
Question 3:
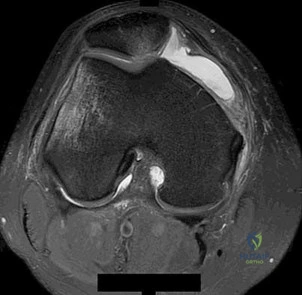
A 22-year-old female collegiate soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BTB) autograft. During the first year postoperatively, she complains of significant anterior knee pain. Which of the following is the most likely cause of her pain associated with this specific graft choice?
Options:
- Arthrofibrosis
- Cyclops lesion
- Harvest site morbidity
- Chondromalacia patellae
- Hardware irritation
Correct Answer: Harvest site morbidity
Explanation:
Anterior knee pain is the most common complication following ACL reconstruction with a bone-patellar tendon-bone (BTB) autograft. It is primarily related to harvest site morbidity at the patellar tendon donor site.
Question 4:
A 65-year-old active male underwent a total hip arthroplasty utilizing a ceramic-on-ceramic bearing surface. Two years later, he complains of an audible 'squeaking' sound from his hip during ambulation. Which of the following factors is most strongly associated with this complication?
Options:
- Femoral stem subsidence
- Acetabular component edge loading due to malposition
- Polyethylene wear debris
- Adverse local tissue reaction (ALTR)
- Recurrent subluxation
Correct Answer: Acetabular component edge loading due to malposition
Explanation:
Squeaking is a known complication specific to ceramic-on-ceramic total hip arthroplasties. It is strongly associated with component malposition, specifically increased acetabular anteversion and inclination, which leads to edge loading, loss of fluid lubrication, and micro-separation.
Question 5:
A 24-year-old man falls on an outstretched hand and sustains a proximal pole scaphoid fracture. Which of the following vascular supplies is most directly responsible for the high rate of nonunion and avascular necrosis in this specific fracture location?
Options:
- Volar carpal branch of the radial artery
- Dorsal carpal branch of the radial artery
- Superficial palmar arch
- Deep palmar arch
- Anterior interosseous artery
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The major blood supply to the scaphoid enters distally at the dorsal ridge via the dorsal carpal branch of the radial artery and flows retrogradely to the proximal pole. Fractures at the proximal pole disrupt this retrograde supply, leading to high rates of avascular necrosis and nonunion.
Question 6:
A 30-year-old construction worker sustains an axial load to a plantarflexed foot. Weight-bearing radiographs demonstrate a 3 mm diastasis between the base of the first and second metatarsals. Which of the following correctly describes the primary anatomy of the Lisfranc ligament?
Options:
- Connects the medial cuneiform to the base of the first metatarsal
- Connects the medial cuneiform to the base of the second metatarsal
- Connects the middle cuneiform to the base of the second metatarsal
- Connects the lateral cuneiform to the cuboid
- Connects the base of the first metatarsal to the base of the second metatarsal
Correct Answer: Connects the medial cuneiform to the base of the second metatarsal
Explanation:
The Lisfranc ligament is an oblique, strong intraosseous ligament that connects the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. It provides critical stability to the midfoot.
Question 7:
A 70-year-old man presents with deteriorating handwriting and difficulty buttoning his shirts. Physical examination demonstrates a positive inverted supinator reflex. What is the most likely level of spinal cord compression?
Options:
- C3-C4
- C4-C5
- C5-C6
- C6-C7
- C7-T1
Correct Answer: C5-C6
Explanation:
The inverted supinator reflex is elicited by tapping the brachioradialis tendon (innervated by C5-C6). A positive sign results in finger flexion (C8) rather than elbow flexion/supination, indicating a lower motor neuron lesion at C5-C6 and an upper motor neuron lesion below that level, thus localizing the compression to C5-C6.
Question 8:
A 15-year-old male presents with worsening pain in his distal femur. Radiographs reveal a destructive metaphyseal lesion with a 'sunburst' periosteal reaction and Codman's triangle. Which of the following is the most significant prognostic factor for overall survival in this patient?
Options:
- Histologic subtype
- Size of the initial tumor
- Percentage of tumor necrosis following neoadjuvant chemotherapy
- Alkaline phosphatase levels
- Location of the tumor
Correct Answer: Percentage of tumor necrosis following neoadjuvant chemotherapy
Explanation:
This patient has an osteosarcoma. The single most important prognostic factor for overall survival in osteosarcoma is the histological response (percentage of tumor necrosis) to neoadjuvant chemotherapy, with >90% necrosis indicating a good response.
Question 9:
Which of the following biomechanical conditions is required for primary (strain-free) bone healing to occur?
Options:
- Absolute stability and compression
- Relative stability with callus formation
- Intramedullary fixation with a gap
- External fixation with dynamization
- Cast immobilization
Correct Answer: Absolute stability and compression
Explanation:
Primary bone healing (intramembranous ossification via cutting cones without callus formation) requires absolute stability (rigid fixation) and direct interfragmentary compression with no motion at the fracture site.
Question 10:
A 32-year-old male sustains a closed tibial shaft fracture. You suspect acute compartment syndrome. His diastolic blood pressure is 80 mmHg. What is the absolute minimum intracompartmental pressure reading that would typically mandate emergency fasciotomy based on the Delta-P concept?
Options:
- 20 mmHg
- 30 mmHg
- 40 mmHg
- 50 mmHg
- 60 mmHg
Correct Answer: 50 mmHg
Explanation:
The Delta-P is defined as Diastolic Blood Pressure minus Intracompartmental Pressure. A Delta-P of 30 mmHg or less is an absolute indication for fasciotomy. Therefore, 80 mmHg - Compartment Pressure <= 30 mmHg means the pressure must be at least 50 mmHg to mandate fasciotomy.
Question 11:
A 6-year-old girl falls off the monkey bars and sustains a displaced extension-type supracondylar humerus fracture. On examination, she is unable to make an 'A-OK' sign, instead demonstrating a pinch with the pulps of her index finger and thumb. Which nerve is most likely injured?
Options:
- Radial nerve
- Ulnar nerve
- Anterior interosseous nerve
- Posterior interosseous nerve
- Musculocutaneous nerve
Correct Answer: Anterior interosseous nerve
Explanation:
The anterior interosseous nerve (AIN), a branch of the median nerve, is the most commonly injured nerve in extension-type supracondylar humerus fractures. It innervates the flexor pollicis longus and flexor digitorum profundus to the index finger; an injury results in an inability to flex the IP joint of the thumb and DIP joint of the index finger (positive 'A-OK' or 'pinch' test).
Question 12:
A 68-year-old female with severe valgus osteoarthritis of the knee undergoes a total knee arthroplasty with an extensive lateral soft tissue release. Postoperatively, she exhibits a foot drop. Which structure is most likely compromised?
Options:
- Tibial nerve
- Deep peroneal nerve
- Superficial peroneal nerve
- Common peroneal nerve
- Sural nerve
Correct Answer: Common peroneal nerve
Explanation:
Correction of a severe valgus knee deformity during total knee arthroplasty puts the common peroneal nerve at risk for stretch injury or direct trauma, especially following extensive lateral releases or postoperative hematoma formation, leading to a classic foot drop.
Question 13:
A 21-year-old male suffers a traumatic anterior shoulder dislocation. An MRI reveals a Bankart lesion. What is the defining anatomical characteristic of a classic Bankart lesion?
Options:
- Avulsion of the anterior-inferior labrum with the anterior band of the inferior glenohumeral ligament
- Compression fracture of the posterolateral humeral head
- Superior labrum anterior to posterior tear extending to the biceps anchor
- Avulsion of the posterior-inferior labrum
- Capsular stretch without frank labral detachment
Correct Answer: Avulsion of the anterior-inferior labrum with the anterior band of the inferior glenohumeral ligament
Explanation:
A Bankart lesion is defined as an avulsion of the anterior-inferior capsulolabral complex from the glenoid rim. This specifically involves the anterior band of the inferior glenohumeral ligament (IGHL).
Question 14:
A laceration to the volar surface of the hand occurs between the distal palmar crease and the proximal interphalangeal joint. Both the flexor digitorum superficialis (FDS) and profundus (FDP) tendons are severed. This injury is located in which flexor tendon zone?
Options:
- Zone I
- Zone II
- Zone III
- Zone IV
- Zone V
Correct Answer: Zone II
Explanation:
Zone II (historically known as 'no man/'s land') extends from the A1 pulley (at the level of the distal palmar crease) to the insertion of the FDS tendon (middle phalanx). Injuries here involve both the FDS and FDP within the tight fibro-osseous sheath, making repair challenging due to adhesion formation.
Question 15:
A 45-year-old weekend warrior feels a sudden 'pop' in his heel while accelerating to play a tennis ball. On examination, squeezing the calf does not result in plantar flexion of the foot. This specific clinical maneuver (Simmonds-Thompson test) evaluates the integrity of which of the following structures?
Options:
- Posterior tibial tendon
- Peroneus brevis tendon
- Achilles tendon
- Plantaris tendon
- Flexor hallucis longus
Correct Answer: Achilles tendon
Explanation:
The Simmonds-Thompson test (calf squeeze test) is used to diagnose Achilles tendon ruptures. A positive test (absence of passive plantar flexion upon calf compression) indicates a complete rupture of the Achilles tendon.
Question 16:
A 72-year-old woman complains of bilateral leg pain and cramping that worsens with walking and standing upright, but is rapidly relieved when she leans forward over a shopping cart. Which of the following physical examination findings is most consistent with her likely diagnosis?
Options:
- Positive straight leg raise test
- Diminished distal pulses
- Normal lower extremity neurologic examination at rest
- Claudication distance remains constant regardless of posture
- Pitting edema of the lower extremities
Correct Answer: Normal lower extremity neurologic examination at rest
Explanation:
The patient's presentation of neurogenic claudication (shopping cart sign) is classic for lumbar spinal stenosis. Unlike vascular claudication, patients with neurogenic claudication often have completely normal physical and neurological examinations while seated or at rest.
Question 17:
An 11-year-old boy presents with a diaphyseal tumor of the femur. Radiographs show an 'onion-skin' periosteal reaction. A biopsy reveals small, round blue cells. Which of the following cytogenetic abnormalities is most pathognomonic for this tumor?
Options:
- t(9;22)
- t(11;22)
- t(X;18)
- t(12;16)
- t(2;13)
Correct Answer: t(11;22)
Explanation:
Ewing sarcoma classically presents in the diaphysis of long bones with an 'onion-skin' appearance. It is characterized by small, round blue cells and is most commonly associated with the t(11;22)(q24;q12) chromosomal translocation, resulting in the EWS-FLI1 fusion protein.
Question 18:
In the microstructure of articular cartilage, which zone is characterized by vertically aligned collagen fibers and is primarily responsible for resisting compressive forces?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified cartilage zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage has chondrocytes arranged in vertical columns with collagen fibers oriented perpendicular to the joint surface. This structural arrangement is optimal for resisting compressive loads.
Question 19:
A 30-year-old male sustains a high-energy vertical shear fracture of the femoral neck (Pauwels Type III). What biomechanical force predominantly contributes to the high risk of nonunion and loss of fixation in this specific fracture pattern?
Options:
- Compressive forces
- Tensile forces
- Shear forces
- Torsional forces
- Bending forces
Correct Answer: Shear forces
Explanation:
Pauwels Type III femoral neck fractures have a fracture line angle >50 degrees relative to the horizontal. This vertical orientation subjects the fracture site to high shear forces rather than compressive forces, drastically increasing the risk of varus collapse and nonunion.
Question 20:
An infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). At the two-week follow-up, the mother notes the infant has stopped kicking with the affected leg. On examination, active knee extension is absent, though passive motion is full. Which of the following complications has most likely occurred?
Options:
- Avascular necrosis of the femoral head
- Obturator nerve palsy
- Femoral nerve palsy
- Sciatic nerve palsy
- Superior gluteal nerve palsy
Correct Answer: Femoral nerve palsy
Explanation:
Femoral nerve palsy is a known complication of the Pavlik harness if the hip is hyperflexed (usually > 120 degrees). It presents as decreased active knee extension and quadriceps firing. It is usually reversible upon decreasing the amount of hip flexion.
Question 21:
A 35-year-old male sustains a severe crushing injury to his pelvis. Examination reveals a large, fluctuant swelling over the greater trochanter with ecchymosis. Aspiration of the lesion yields serosanguinous fluid with fat globules. Which of the following is the most appropriate definitive management for a large, chronic lesion of this type?
Options:
- Immediate open debridement and primary closure
- Percutaneous aspiration
- Open debridement and delayed closure or secondary intention
- Observation
- Sclerotherapy
Correct Answer: Open debridement and delayed closure or secondary intention
Explanation:
A Morel-Lavallée lesion is a closed degloving injury. Chronic lesions with a mature capsule often require open debridement, capsulectomy, and either delayed closure, use of dead-space management, or secondary intention, as simple aspiration has a high recurrence rate.
Question 22:
A 65-year-old female presents with a painful total knee arthroplasty 2 years post-operatively. Synovial fluid analysis shows a WBC count of 3,500 cells/µL with 75% PMNs. The alpha-defensin immunoassay is positive. What is the primary cellular source of alpha-defensin in this context?
Options:
- Synovial fibroblasts
- Macrophages
- Neutrophils
- T-lymphocytes
- Osteoblasts
Correct Answer: Neutrophils
Explanation:
Alpha-defensin is an antimicrobial peptide released primarily by neutrophils in response to infection. It serves as a highly sensitive and specific biomarker for periprosthetic joint infection.
Question 23:
A 45-year-old male presents with chronic wrist pain. Radiographs demonstrate scapholunate advanced collapse (SLAC). In a Stage II SLAC wrist, the degenerative changes involve which of the following articulations?
Options:
- Radial styloid and scaphoid alone
- Entire radioscaphoid joint
- Radioscaphoid and capitolunate joints
- Capitolunate and lunotriquetral joints
- Radiolunate joint
Correct Answer: Entire radioscaphoid joint
Explanation:
SLAC wrist progression: Stage I involves the radial styloid-scaphoid articulation. Stage II involves the entire radioscaphoid facet. Stage III involves the capitolunate joint. The radiolunate joint is characteristically spared.
Question 24:
A 25-year-old male presents after an MVA with neck pain and right C6 radiculopathy. Radiographs show a unilateral facet dislocation at C5-C6. MRI confirms no herniated disc. He is awake and cooperative but unable to undergo closed reduction. What is the next best step in management?
Options:
- Anterior cervical discectomy and fusion (ACDF)
- Posterior cervical fusion alone
- Anterior and posterior cervical fusion
- Halo vest application
- Laminectomy
Correct Answer: Anterior cervical discectomy and fusion (ACDF)
Explanation:
For a unilateral facet dislocation in an awake patient who fails closed reduction (or if closed reduction is not feasible), an anterior approach (ACDF) is generally preferred as it allows for direct visualization and removal of any disc material prior to reduction, minimizing the risk of neurologic deterioration, and provides excellent biomechanical stability.
Question 25:
A 13-year-old obese male presents with left thigh pain and a limp. He walks with an externally rotated leg. Radiographs reveal a severe slipped capital femoral epiphysis (SCFE) with a slip angle of 60 degrees. What is the most significant risk associated with performing an acute anatomical reduction prior to pinning?
Options:
- Chondrolysis
- Avascular necrosis of the femoral head
- Femoroacetabular impingement
- Subtrochanteric fracture
- Leg length discrepancy
Correct Answer: Avascular necrosis of the femoral head
Explanation:
Acute anatomical reduction of a SCFE is highly associated with stretching or kinking of the retinacular vessels, leading to avascular necrosis (AVN) of the femoral head. Therefore, in-situ pinning is the gold standard for stable slips, though unstable slips may require gentle reduction or open procedures (e.g., modified Dunn).
Question 26:
When comparing the tibial inlay technique to the transtibial tunnel technique for posterior cruciate ligament (PCL) reconstruction, the tibial inlay technique has the theoretical biomechanical advantage of decreasing what phenomenon?
Options:
- Graft stretch-out
- The "killer turn" effect
- Arthrofibrosis
- Tunnel widening
- Anterior tibial translation
Correct Answer: The "killer turn" effect
Explanation:
The transtibial tunnel technique for PCL reconstruction forces the graft to make an acute angle at the posterior aperture of the tibial tunnel, known as the "killer turn," which can lead to graft abrasion and attenuation. The tibial inlay technique avoids this acute angle.
Question 27:
A 55-year-old active male underwent a total hip arthroplasty using a ceramic-on-ceramic bearing. He presents 2 years post-operatively complaining of a squeaking noise from the hip during walking. Which of the following component malpositions is most commonly associated with this phenomenon?
Options:
- Acetabular component retroversion
- Femoral component retroversion
- Acetabular component edge loading due to excessive inclination
- Excessive femoral offset
- Insufficient acetabular version
Correct Answer: Acetabular component edge loading due to excessive inclination
Explanation:
Squeaking in ceramic-on-ceramic THA is often associated with edge loading, which typically results from acetabular component malposition, specifically excessive inclination and/or version issues causing loss of fluid film lubrication and subsequent stripe wear.
Question 28:
A 14-year-old female presents with pain in her proximal humerus. Radiographs show an eccentric, expansile, lytic lesion with thin cortices. MRI demonstrates fluid-fluid levels. A biopsy confirms an aneurysmal bone cyst (ABC). What is the genetic translocation most commonly associated with primary ABCs?
Options:
- t(11;22) (q24;q12)
- t(16;17) (q22;p13)
- t(X;18) (p11;q11)
- t(12;16) (q13;p11)
- t(2;13) (q35;q14)
Correct Answer: t(16;17) (q22;p13)
Explanation:
Primary aneurysmal bone cysts are neoplasms characterized by a rearrangement of the USP6 gene on chromosome 17p13. The most common translocation is t(16;17)(q22;p13) which fuses the promoter region of CDH11 to USP6.
Question 29:
A 60-year-old female undergoes volar locked plating for a displaced distal radius fracture. Eight weeks post-operatively, she returns complaining of the sudden inability to actively flex the interphalangeal joint of her thumb. Which of the following surgical errors most likely led to this complication?
Options:
- Plate placed distal to the watershed line
- Dorsal screw penetration
- Unrecognized scapholunate ligament tear
- Failure to repair the pronator quadratus
- Over-distraction of the radiocarpal joint
Correct Answer: Plate placed distal to the watershed line
Explanation:
Flexor pollicis longus (FPL) tendon rupture is a known complication of volar plating of the distal radius. It is typically caused by placement of the plate distal to the watershed line, allowing the FPL tendon to rub against the prominent distal edge of the plate.
Question 30:
An athlete sustains a hyperplantarflexion injury to the midfoot. Radiographs demonstrate widening of the space between the medial and middle cuneiforms. The primary stabilizing ligament of the Lisfranc joint complex attaches to which two bones?
Options:
- Medial cuneiform and second metatarsal base
- Middle cuneiform and second metatarsal base
- Lateral cuneiform and third metatarsal base
- Cuboid and fourth metatarsal base
- Medial cuneiform and first metatarsal base
Correct Answer: Medial cuneiform and second metatarsal base
Explanation:
The Lisfranc ligament is an interosseous ligament that runs from the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. It is the strongest and most crucial stabilizing ligament of the tarsometatarsal complex.
Question 31:
A rugby player sustains a closed injury to his right ring finger while grabbing an opponent's jersey. He is unable to actively flex the DIP joint. Imaging shows an avulsion fracture of the distal phalanx base retracted to the level of the PIP joint. According to the Leddy and Packer classification, what type of injury is this?
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type II
Explanation:
Leddy and Packer classification of FDP avulsion (Jersey finger): Type I - retracted to palm; Type II - retracted to the PIP joint level (held by the vinculum longum); Type III - large bony fragment avulsed and caught at the A4 pulley; Type IV - osseous fragment with concurrent tendon avulsion from the fragment.
Question 32:
An 18-year-old gymnast complains of chronic lower back pain. Lateral radiographs demonstrate a pars interarticularis defect at L5 with an anterior translation of the L5 vertebral body over S1 by 60%. What is the appropriate Meyerding grade for this slip?
Options:
- Grade I
- Grade II
- Grade III
- Grade IV
- Spondyloptosis
Correct Answer: Grade III
Explanation:
The Meyerding classification system grades the severity of spondylolisthesis based on the percentage of forward translation: Grade I (0-25%), Grade II (26-50%), Grade III (51-75%), Grade IV (76-100%), and Grade V (>100%, Spondyloptosis). 60% falls into Grade III.
Question 33:
When managing a congenital talipes equinovarus (clubfoot) using the Ponseti method, the first step in the casting sequence aims to correct which deformity?
Options:
- Equinus
- Cavus
- Varus
- Adductus
- Forefoot pronation
Correct Answer: Cavus
Explanation:
The Ponseti method corrects the deformities of clubfoot in a specific sequence (CAVE). The first step is the correction of Cavus by elevating the first ray to align the forefoot with the hindfoot, supinating the forefoot.
Question 34:
A 28-year-old overhead throwing athlete undergoes arthroscopy for a suspected SLAP tear. The surgeon notes fraying of the superior labrum but the biceps anchor is intact and firmly attached to the glenoid. According to the Snyder classification, this represents:
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type I
Explanation:
Snyder classification of SLAP tears: Type I involves fraying and degeneration of the superior labrum with an intact biceps anchor. Type II involves detachment of the superior labrum and biceps anchor from the glenoid. Type III involves a bucket-handle tear of the superior labrum with an intact biceps anchor. Type IV involves a bucket-handle tear that extends into the biceps tendon.
Question 35:
During normal knee flexion, the phenomenon of femoral rollback is primarily facilitated by which of the following structures?
Options:
- Anterior cruciate ligament (ACL)
- Posterior cruciate ligament (PCL)
- Medial collateral ligament (MCL)
- Lateral collateral ligament (LCL)
- Popliteus tendon
Correct Answer: Posterior cruciate ligament (PCL)
Explanation:
Femoral rollback is the posterior translation of the femur on the tibia during knee flexion, which allows for increased flexion before impingement occurs. This is primarily guided and facilitated by the tension in the posterior cruciate ligament (PCL). In PCL-restituting or substituting TKAs, maintaining this mechanism is critical.
Question 36:
A 30-year-old female presents with knee pain. Radiographs reveal an eccentric, lytic lesion in the distal femoral epiphysis extending to the subchondral bone. Biopsy confirms a giant cell tumor. She is treated with denosumab preoperatively. What is the mechanism of action of denosumab?
Options:
- Inhibition of VEGF
- Monoclonal antibody against RANKL
- Direct cytotoxicity to osteoclasts
- Antagonist of the PTH receptor
- Inhibition of sclerostin
Correct Answer: Monoclonal antibody against RANKL
Explanation:
Denosumab is a fully human monoclonal antibody that binds to and inhibits RANK Ligand (RANKL). This prevents RANKL from activating RANK on the surface of osteoclasts and their precursors, thereby decreasing bone resorption and causing sclerosis in giant cell tumors.
Question 37:
A 32-year-old male sustains a severe inversion injury resulting in a displaced fracture of the talar neck with subluxation of the subtalar joint, while the tibiotalar joint remains congruous. According to the Hawkins classification, what type of injury is this and what is the approximate rate of avascular necrosis (AVN)?
Options:
- Type I, 0-10%
- Type II, 20-50%
- Type III, 80-100%
- Type IV, 100%
- Type II, 80-100%
Correct Answer: Type II, 20-50%
Explanation:
Hawkins Classification of talar neck fractures: Type I is nondisplaced (0-10% AVN). Type II involves displacement with subtalar subluxation/dislocation (20-50% AVN). Type III involves displacement with both subtalar and tibiotalar dislocation (nearly 100% AVN). Type IV adds talonavicular subluxation/dislocation.
Question 38:
A 55-year-old male with poorly controlled diabetes mellitus presents with a swollen, erythematous, and warm left foot. Radiographs demonstrate periarticular fragmentation, subluxation, and bony debris at the midfoot. According to the Eichenholtz classification, this presentation is most consistent with which stage?
Options:
- Stage 0
- Stage I (Development)
- Stage II (Coalescence)
- Stage III (Reconstruction)
- Stage IV (Resolution)
Correct Answer: Stage I (Development)
Explanation:
The Eichenholtz classification of Charcot arthropathy: Stage 0 (pre-fragmentation) - erythema, edema, normal radiographs. Stage I (Development/Fragmentation) - severe edema, erythema, bony fragmentation, joint subluxation/dislocation, debris. Stage II (Coalescence) - decreased edema, absorption of fine debris, early fusion. Stage III (Reconstruction) - remodeling and consolidation of bone.
Question 39:
Following rigid internal fixation of a diaphyseal fracture with absolute stability, primary bone healing occurs without callus formation. This process is mediated primarily by:
Options:
- Endochondral ossification
- Intramembranous ossification
- Cutting cones crossing the fracture gap
- Fibrocartilage template conversion
- Chondrocyte hypertrophy
Correct Answer: Cutting cones crossing the fracture gap
Explanation:
Absolute stability (e.g., compression plating) eliminates micro-motion at the fracture site, leading to primary bone healing. This occurs via direct Haversian remodeling where osteoclasts create "cutting cones" that cross the fracture site, followed by osteoblasts laying down new osteons, without a cartilaginous intermediate or visible callus.
Question 40:
A 42-year-old pregnant female presents with numbness and tingling in her right thumb, index, and long fingers. EMG/NCS is obtained. Which of the following is the earliest and most sensitive nerve conduction study finding in carpal tunnel syndrome?
Options:
- Increased distal motor latency
- Decreased motor nerve conduction velocity
- Increased distal sensory latency
- Fibrillation potentials in the abductor pollicis brevis
- Decreased sensory nerve action potential amplitude
Correct Answer: Increased distal sensory latency
Explanation:
In carpal tunnel syndrome (median nerve compression), the sensory fibers are typically affected before the motor fibers. Therefore, a delay in the sensory nerve conduction (increased distal sensory latency) is generally the earliest and most sensitive electrodiagnostic finding.
Question 41:
A 45-year-old manual laborer presents with chronic right wrist pain. He recalls a severe sprain 10 years ago that was untreated. Radiographs demonstrate an established scaphoid nonunion with arthritic changes at the radioscaphoid and capitolunate joints, but preservation of the radiolunate articulation. Based on the expected stage of this disease process, which of the following is the most appropriate surgical treatment?
Options:
- Open reduction internal fixation of the scaphoid with vascularized bone graft
- Radial styloidectomy alone
- Proximal row carpectomy (PRC)
- Total wrist arthroplasty
- Scaphotrapeziotrapezoid (STT) fusion
Correct Answer: Proximal row carpectomy (PRC)
Explanation:
This patient has Scaphoid Nonunion Advanced Collapse (SNAC) Stage III, defined by arthritis at both the radioscaphoid joint and the midcarpal (capitolunate) joint, with a preserved radiolunate joint. Open reduction and internal fixation is no longer indicated once degenerative changes have occurred. Radial styloidectomy is insufficient for Stage III. The standard salvage procedures for SNAC Stage III (and SLAC Stage III) are either a proximal row carpectomy (PRC) or a scaphoid excision with a four-corner fusion. The radiolunate fossa is typically spared in both SLAC and SNAC wrists because the lunate maintains a concentric articulation with the radius.
Question 42:
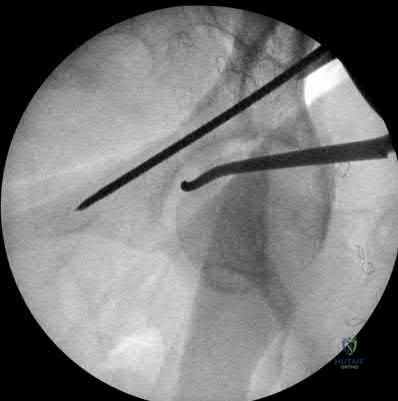
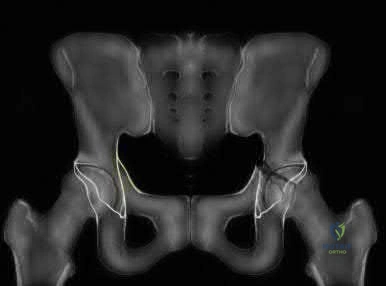
A 32-year-old male is brought to the trauma bay following a high-speed motorcycle collision. He is hemodynamically unstable. An anteroposterior radiograph of the pelvis demonstrates a 'symphysis pubis diastasis of 4 cm and disruption of the anterior sacroiliac ligaments with intact posterior ligaments' (an APC II injury). During surgical exploration to control hemorrhage, brisk arterial bleeding is encountered posterior to the superior pubic ramus. This vessel is most likely an anastomosis between which two vascular distributions?
Options:
- Internal pudendal and superior gluteal arteries
- Inferior epigastric (or external iliac) and obturator arteries
- Superior mesenteric and inferior mesenteric arteries
- Internal iliac and median sacral arteries
- Femoral and superficial circumflex iliac arteries
Correct Answer: Inferior epigastric (or external iliac) and obturator arteries
Explanation:
The vessel described is the 'corona mortis' (crown of death). It is an anatomic variant anastomosis between the external iliac or inferior epigastric system and the obturator artery (internal iliac system). It traverses over the superior pubic ramus at an average distance of 4 to 5 cm from the pubic symphysis. Disruption of this vascular connection during high-energy pelvic trauma, particularly anterior ring injuries, can lead to severe, life-threatening hemorrhage.
Question 43:
An 8-year-old child presents with a limp and poorly localized knee pain. Radiographs confirm a unilateral slipped capital femoral epiphysis (SCFE). Given the patient's age, an endocrine workup is indicated. Which of the following is the most common underlying endocrine abnormality associated with SCFE in this patient population?
Options:
- Hyperparathyroidism
- Hypothyroidism
- Growth hormone deficiency
- Panhypopituitarism
- Testosterone deficiency
Correct Answer: Hypothyroidism
Explanation:
While idiopathic SCFE typically occurs during the adolescent growth spurt (ages 10-14 for girls, 12-16 for boys), patients who present 'out of age range' (< 10 years or > 16 years) or whose weight is less than the 50th percentile have a high association with endocrine disorders. Hypothyroidism is the most commonly associated endocrine disorder in patients with SCFE. Other causes include panhypopituitarism, growth hormone supplementation, and renal osteodystrophy.
Question 44:
A 24-year-old male presents with a slowly growing, painful mass in the anterior compartment of his left leg. Radiographs show an eccentric, multi-loculated, 'soap-bubble' osteolytic lesion in the diaphysis of the tibia. A biopsy is performed. Histological analysis reveals nests of epithelial-appearing cells in a fibrous stroma. Immunohistochemistry is strongly positive for cytokeratin. What is the most likely diagnosis?
Options:
- Osteofibrous dysplasia
- Ewing sarcoma
- Adamantinoma
- Chondromyxoid fibroma
- Synovial sarcoma
Correct Answer: Adamantinoma
Explanation:
Adamantinoma is a rare, low-grade malignant bone tumor that almost exclusively occurs in the diaphysis of the tibia. Radiographically, it appears as a multi-loculated 'soap-bubble' lesion. Histologically, it is biphasic with both epithelial cells and osteofibrous stroma. The definitive diagnostic marker is its strong immunohistochemical positivity for cytokeratins. Osteofibrous dysplasia occurs in the same location and demographic but lacks the cytokeratin-positive epithelial cells and is a benign lesion.
Question 45:
In the biomechanical design of a pedicle screw, which of the following modifications most effectively increases the screw's pullout strength in osteoporotic bone?
Options:
- Decreasing the thread density (pitch length)
- Increasing the major (outer) diameter of the screw
- Increasing the minor (inner core) diameter while maintaining the major diameter
- Using a partially threaded rather than fully threaded screw
- Decreasing the length of thread engagement
Correct Answer: Increasing the major (outer) diameter of the screw
Explanation:
Pullout strength of a screw is primarily determined by the major (outer) diameter of the screw, the length of thread engagement, thread shape, and bone density. The equation for pullout strength shows it is directly proportional to the major diameter. Increasing the minor (core) diameter without changing the major diameter actually decreases the volume of bone trapped between the threads, thereby decreasing pullout strength. Decreasing the pitch length (which increases the thread density, meaning more threads per inch) also increases pullout strength, but increasing the major diameter is the most powerful design modification to improve pullout strength.
Question 46:
During arthroscopy for an acute anterior cruciate ligament (ACL) tear, a systematic evaluation of the knee is performed. The surgeon places the arthroscope through the intercondylar notch into the posteromedial compartment. A longitudinal tear is observed at the meniscocapsular junction of the posterior horn of the medial meniscus. What is the term for this specific lesion?
Options:
- RAMP lesion
- Root tear
- Bucket-handle tear
- Wrisberg rip
- Radial tear
Correct Answer: RAMP lesion
Explanation:
A RAMP lesion is a longitudinal tear of the peripheral attachment (meniscocapsular junction) of the posterior horn of the medial meniscus. It is highly associated with acute ACL ruptures (occurring in up to 24% of cases). Because it is located in the blind spot of the knee, it is frequently missed if the posteromedial compartment is not systematically inspected through the intercondylar notch or via a posteromedial portal.
Question 47:
During a primary total knee arthroplasty using a measured resection technique, the surgeon utilizes trial components and finds that the knee is symmetric and balanced in full extension, but perfectly symmetric and overly tight in 90 degrees of flexion. Which of the following adjustments is the most appropriate to balance the knee?
Options:
- Recut the proximal tibia with more posterior slope
- Increase the size of the polyethylene insert
- Downsize the femoral component
- Release the posterior cruciate ligament (PCL)
- Recut the distal femur to take more bone
Correct Answer: Downsize the femoral component
Explanation:
When a knee is balanced in extension but tight in flexion, the flexion gap must be increased without altering the extension gap. The flexion gap is determined by the posterior femoral condyles and the proximal tibia. Recutting the tibia (or changing the poly) would affect both gaps. Downsizing the femoral component (which decreases the anteroposterior dimension of the femur by taking more posterior bone with an anterior referencing system) selectively increases the size of the flexion gap, balancing the knee.
Question 48:
A 28-year-old female presents to the emergency department after a motor vehicle collision. She is awake, alert, and cooperative. She complains of severe neck pain. Neurological examination is completely intact. Lateral cervical spine radiographs show an anterior translation of C5 on C6 of approximately 60% of the vertebral body width, with dislocated facets bilaterally. What is the most appropriate next step in management?
Options:
- Immediate urgent MRI to evaluate for disc herniation prior to any reduction
- Awake closed reduction using cranial tongs and progressive weight traction
- Immediate anterior cervical discectomy and fusion (ACDF)
- Immediate posterior cervical fusion
- Placement of a hard cervical collar and discharge with outpatient follow-up
Correct Answer: Awake closed reduction using cranial tongs and progressive weight traction
Explanation:
In an awake, alert, and cooperative patient with a bilateral facet dislocation and no (or stable) neurological deficits, the standard of care is to attempt a prompt awake closed reduction using progressive cranial tong traction. MRI prior to reduction is generally reserved for patients who have altered mental status, cannot cooperate with serial neurological exams during closed reduction, or have failed closed reduction. An awake reduction allows the physician to monitor the patient for neurologic deterioration (indicating a potential disc herniation being dragged into the canal), at which point traction would be reversed and an MRI obtained.
Question 49:
A 55-year-old male with long-standing, poorly controlled type 2 diabetes presents with a red, hot, swollen right foot. He denies any recent trauma, fevers, or systemic illness. Laboratory studies reveal a normal white blood cell count, ESR of 25 mm/h, and CRP of 1.0 mg/L. Radiographs demonstrate soft tissue swelling, profound joint subluxation at the tarsometatarsal joints, and bony fragmentation without focal osteopenia. What is the most appropriate initial treatment?
Options:
- Intravenous antibiotics and surgical debridement
- Oral antibiotics and non-weight bearing
- Immediate open reduction and internal fixation of the midfoot
- Total contact casting and strict non-weight bearing
- Primary below-knee amputation
Correct Answer: Total contact casting and strict non-weight bearing
Explanation:
This patient presents with Stage I (Developmental/Fragmentation phase) Charcot arthropathy, characterized by a red, hot, swollen foot, joint laxity, and radiographic fragmentation and debris. Normal inflammatory markers and lack of systemic signs help distinguish this from acute osteomyelitis or septic arthritis. The gold standard initial treatment for an acute Charcot neuroarthropathy is immobilization and offloading, typically achieved via a total contact cast, until the active inflammatory phase subsides and the bones begin to consolidate (Stage II/III).
Question 50:
In the anatomy of the flexor tendon sheath of the digits, preservation of certain structures is critical to prevent bowstringing of the flexor tendons. During an extensive tenolysis procedure of the index finger, which two annular pulleys are the most critical to preserve?
Options:
- A1 and A3
- A2 and A4
- A3 and A5
- A1 and A5
- A2 and A3
Correct Answer: A2 and A4
Explanation:
The flexor tendon sheath contains a series of thickened bands known as annular (A) and cruciate (C) pulleys. The A2 and A4 pulleys are the major mechanical pulleys that hold the flexor tendons close to the phalanges, preventing bowstringing during active flexion. The A2 pulley is located over the proximal phalanx, and the A4 pulley is over the middle phalanx. They are biomechanically the most critical.
Question 51:
Fracture healing can occur via endochondral or intramembranous ossification. Intramembranous ossification occurs without a cartilaginous intermediate and is primarily seen in flat bones and during rigid plate fixation (primary bone healing). Which of the following transcription factors is the critical master regulator that directs multipotent mesenchymal stem cells down the osteoblastic lineage during intramembranous bone formation?
Options:
- SOX9
- MyoD
- RUNX2 (Cbfa1)
- PPAR-gamma
- HIF-1 alpha
Correct Answer: RUNX2 (Cbfa1)
Explanation:
RUNX2 (also known as Cbfa1) is the master transcription factor required for osteoblast differentiation and is absolutely essential for both intramembranous and endochondral bone formation. Mice lacking RUNX2 are devoid of osteoblasts and completely lack bone. SOX9 is the master regulator for chondrocyte differentiation. PPAR-gamma regulates adipocyte differentiation. MyoD regulates myoblast differentiation.
Question 52:
An infant is diagnosed with severe, rigid idiopathic congenital talipes equinovarus (clubfoot). Treatment using the Ponseti method is initiated. According to the specific sequence of the Ponseti method, what is the required primary manipulation in the first casting to correct the multi-planar deformity?
Options:
- Elevate the first ray to supinate the forefoot
- Pronate the forefoot to stretch the plantar fascia
- Abduct the midfoot with counter-pressure on the calcaneocuboid joint
- Dorsiflex the ankle to stretch the Achilles tendon
- Evert the calcaneus to correct hindfoot varus
Correct Answer: Elevate the first ray to supinate the forefoot
Explanation:
The mnemonic for Ponseti casting is CAVE (Cavus, Adductus, Varus, Equinus). The very first step must be correction of the cavus deformity. The cavus in a clubfoot is caused by a pronated forefoot relative to the hindfoot. To correct this, the first ray is elevated, which supinates the forefoot so that it is in the same plane as the hindfoot. Once the cavus is corrected, the entire foot can be abducted (with counter-pressure over the lateral aspect of the talar head, NOT the calcaneocuboid joint) to simultaneously correct adductus and varus. Equinus is addressed last, often requiring a percutaneous Achilles tenotomy.
Question 53:
A 34-year-old male sustains a closed talar neck fracture following a fall from height. He undergoes urgent open reduction and internal fixation. At his 8-week postoperative follow-up, an anteroposterior radiograph of the ankle demonstrates a linear subchondral radiolucent band in the dome of the talus. What does this radiographic finding indicate regarding the prognosis of his injury?
Options:
- Early onset of post-traumatic osteoarthritis
- Imminent collapse of the talar dome
- High likelihood of nonunion
- Presence of adequate vascularity and low risk of avascular necrosis
- Establishment of deep bone infection
Correct Answer: Presence of adequate vascularity and low risk of avascular necrosis
Explanation:
The finding described is the 'Hawkins sign'. It is a subchondral radiolucent band (osteopenia) in the talar dome that typically appears 6 to 8 weeks after injury. Because bone resorption requires an intact blood supply, the presence of the Hawkins sign is a highly reliable indicator of preserved vascularity to the talar body, forecasting a low risk of avascular necrosis (AVN). Conversely, the absence of this sign (retention of subchondral radiodensity while the surrounding bone becomes osteopenic) suggests AVN.
Question 54:
A 65-year-old female with known multiple myeloma presents with escalating back pain. Radiographs reveal diffuse osteopenia and multiple 'punched-out' lytic lesions in her vertebral bodies. The profound osteolysis seen in multiple myeloma is primarily driven by an imbalance in bone remodeling. Which of the following factors is directly secreted by myeloma cells to upregulate osteoclast activity via the RANK/RANKL pathway?
Options:
- Osteoprotegerin (OPG)
- Transforming growth factor-beta (TGF-beta)
- Macrophage inflammatory protein-1 alpha (MIP-1 alpha)
- Bone morphogenetic protein-2 (BMP-2)
- Parathyroid hormone (PTH)
Correct Answer: Macrophage inflammatory protein-1 alpha (MIP-1 alpha)
Explanation:
Multiple myeloma bone lesions are characterized by uncoupled bone remodeling: increased osteoclast activity and markedly decreased osteoblast activity. Myeloma cells directly secrete several osteoclast activating factors, prominently Macrophage Inflammatory Protein-1 alpha (MIP-1 alpha) and RANK Ligand (RANKL). They also suppress osteoblastogenesis via Dickkopf-1 (DKK-1) and sclerostin. Osteoprotegerin (OPG) acts as a decoy receptor for RANKL and inhibits osteoclast activity; its levels are typically decreased in myeloma.
Question 55:
A 70-year-old patient returns to the emergency department three weeks following an uncomplicated primary total hip arthroplasty (posterior approach) with complaints of sudden severe hip pain. Radiographs demonstrate a posterior dislocation of the femoral component. Closed reduction is successful. In evaluating the cause of this early instability, which of the following component malpositions is the most common etiology for posterior dislocation in THA?
Options:
- Acetabular component retroversion
- Acetabular component excessive abduction
- Femoral component excessive anteversion
- Excessive offset reconstruction
- Acetabular component excessive anteversion
Correct Answer: Acetabular component retroversion
Explanation:
Instability following THA is multifactorial. However, when component malposition is the primary driver of a posterior dislocation, acetabular retroversion (insufficient anteversion) is the most frequent culprit. Normal acetabular anteversion target is 15-20 degrees. Retroversion impinges the anterior neck during internal rotation/flexion, levering the head out posteriorly. Excessive abduction leads to superior escape/instability. Excessive anteversion usually leads to anterior dislocation.
Question 56:
A 19-year-old collegiate swimmer presents with bilateral shoulder pain. She reports a sensation that her shoulders are constantly 'slipping out' of place, especially during the pull phase of her stroke. Physical examination demonstrates generalized ligamentous laxity, a positive sulcus sign bilaterally, and positive apprehension tests anteriorly and posteriorly. Scapular dyskinesia is prominent. What is the most appropriate initial management?
Options:
- Arthroscopic labral repair (SLAP repair)
- Physical therapy focusing on periscapular stabilization and rotator cuff strengthening
- Open inferior capsular shift
- Arthroscopic plication of the anterior capsule
- Latarjet procedure
Correct Answer: Physical therapy focusing on periscapular stabilization and rotator cuff strengthening
Explanation:
This patient has classic symptoms of Multidirectional Instability (MDI) of the shoulder, often associated with generalized ligamentous laxity (Ehlers-Danlos, Marfan, or simply physiological hyperlaxity) and confirmed by a positive sulcus sign. The cornerstone of initial treatment for MDI is a prolonged, dedicated physical therapy program (minimum 3-6 months) focusing on strengthening the dynamic stabilizers of the shoulder (periscapular muscles and rotator cuff). Surgical stabilization (e.g., open or arthroscopic inferior capsular shift) is strictly reserved for patients who fail extensive conservative management.
Question 57:
A patient sustained a C6 burst fracture in a diving accident. On initial neurological examination in the ICU, he demonstrates active wrist extension against gravity (Grade 3/5) but no active triceps or hand intrinsic function. He has no voluntary anal contraction, but he has preserved sensation to pinprick in the perianal area (S4-S5). Additionally, he has trace voluntary movement of his right great toe (Grade 1/5). According to the ASIA Impairment Scale (AIS), how should this patient be classified?
Options:
- AIS A
- AIS B
- AIS C
- AIS D
- AIS E
Correct Answer: AIS C
Explanation:
The ASIA Impairment Scale classifies spinal cord injuries. The presence of ANY sacral sparing (perianal sensation or voluntary anal contraction) means the injury is incomplete (eliminating AIS A). Because there is motor function preserved more than 3 levels below the motor level (trace toe movement), the patient is motor incomplete. To differentiate between AIS C and AIS D, one evaluates the muscle grades below the neurological level: in AIS C, less than half of key muscle functions below the neurological level have a muscle grade of ≥ 3. In AIS D, at least half have a grade of ≥ 3. Since this patient only has trace (Grade 1) distal motor function, he is AIS C.
Question 58:
Osteochondral lesions (OCDs) of the talus frequently occur following ankle sprains. Based on classic descriptions of these injuries, what is the typical morphology and mechanism for an anterolateral talar dome lesion?
Options:
- Shallow, wafer-shaped, and caused by inversion and dorsiflexion
- Deep, cup-shaped, and caused by inversion and plantarflexion
- Shallow, wafer-shaped, and typically non-traumatic/insidious in origin
- Deep, cup-shaped, and caused by eversion and external rotation
- Usually bilaterally symmetric and asymptomatic
Correct Answer: Shallow, wafer-shaped, and caused by inversion and dorsiflexion
Explanation:
The mnemonic 'DIAL a PIMP' is classically used for talar dome lesions. DIAL = Dorsiflexion, Inversion -> AnteroLateral. PIMP = Plantarflexion, Inversion -> PosterioMedial. Anterolateral lesions are typically traumatic, shallow, wafer-shaped, and more likely to displace. Posteromedial lesions are often deeper, cup-shaped, less likely to displace, and may not have a clear history of trauma.
Question 59:
A 60-year-old female underwent volar locked plating of a comminuted distal radius fracture 4 months ago. She now presents complaining of the sudden inability to bend the tip of her thumb. She reports hearing a 'pop' in her wrist yesterday while opening a jar. Which of the following technical errors during the initial surgery is the most likely cause of her current presentation?
Options:
- Use of screws that were too long penetrating the dorsal cortex
- Failure to repair the pronator quadratus during closure
- Placement of the volar plate anterior to the watershed line
- Over-distraction of the fracture resulting in median nerve ischemia
- Inadequate reduction of the dorsal tilt
Correct Answer: Placement of the volar plate anterior to the watershed line
Explanation:
The sudden inability to flex the interphalangeal joint of the thumb months after a volar distal radius plate placement is classic for an iatrogenic rupture of the Flexor Pollicis Longus (FPL) tendon. This occurs due to mechanical attrition of the tendon against the hardware. The most critical risk factor for FPL rupture is placing the volar plate too far distally, specifically anterior to the 'watershed line' (a transverse ridge on the volar margin of the distal radius), which allows the plate to prominently impinge on the flexor tendons.
Question 60:
A 22-year-old male suffers a highly comminuted tibia-fibula fracture. Within hours, he develops extreme leg pain out of proportion to the injury, pain with passive stretch of the toes, and a tense, woody swelling of the leg. Compartment syndrome is suspected. If the anterior compartment is predominantly involved, which of the following sensory deficits is most likely to be found on examination?
Options:
- Numbness over the plantar aspect of the foot
- Numbness in the first web space of the dorsum of the foot
- Numbness over the lateral aspect of the foot
- Numbness over the medial malleolus
- Numbness over the posterior calf
Correct Answer: Numbness in the first web space of the dorsum of the foot
Explanation:
The anterior compartment of the lower leg contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius muscles, along with the deep peroneal nerve and anterior tibial artery. Increased pressure in this compartment will compress the deep peroneal nerve, leading to sensory deficits in its isolated cutaneous distribution: the dorsal first web space of the foot. The superficial peroneal nerve (lateral compartment) provides sensation to the rest of the dorsum of the foot. The tibial nerve (posterior compartment) innervates the plantar foot.