Full Question & Answer Text (for Search Engines)
Question 1:
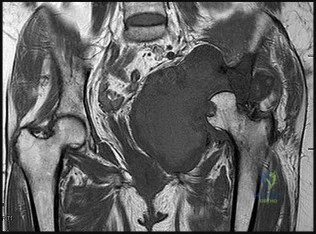
A 12-year-old obese male presents with left groin pain and an altered gait. Based on the presumed diagnosis of slipped capital femoral epiphysis (SCFE) shown in the representative radiograph, which of the following is the primary blood supply to the femoral head that is at highest risk for iatrogenic injury during percutaneous in situ pinning if the pin is placed in the posterosuperior quadrant?
Options:
- Anterior ascending branch of the lateral circumflex femoral artery
- Posterosuperior retinacular vessels from the medial circumflex femoral artery
- Foveal artery from the obturator artery
- Inferior gluteal artery branches
- Medial epiphyseal artery
Correct Answer: Posterosuperior retinacular vessels from the medial circumflex femoral artery
Explanation:
The primary blood supply to the capital femoral epiphysis in children over the age of 3 is the posterosuperior retinacular vessels (lateral epiphyseal artery), which are terminal branches of the medial circumflex femoral artery (MCFA). During in situ pinning for SCFE, placement of the pin in the posterosuperior quadrant of the femoral neck/head places these extracapsular vessels at extreme risk of injury, potentially leading to avascular necrosis (AVN). Pins should ideally be placed in the center-center position to minimize this risk.
Question 2:
A 45-year-old female sustains a knee injury following a motor vehicle collision. Assuming the representative image demonstrates a medial tibial plateau fracture with articular depression (Schatzker IV), what is the most likely mechanism of injury?
Options:
- Valgus force combined with an axial load
- Varus force combined with an axial load
- Hyperextension injury
- Direct anterior blow to a flexed knee
- Low-energy rotational twisting on a planted foot
Correct Answer: Varus force combined with an axial load
Explanation:
A Schatzker IV fracture involves the medial tibial plateau. The medial plateau is structurally denser and stronger than the lateral plateau, meaning fractures here typically require higher energy. The classic mechanism is a varus force combined with an axial load. In contrast, lateral plateau fractures (Schatzker I-III) are typically caused by a valgus force with an axial load. High-energy trauma to the medial plateau is also highly associated with injury to the peroneal nerve, popliteal artery, and ligamentous structures (like the ACL or LCL).
Question 3:
A 25-year-old male is involved in a high-speed motor vehicle collision. Radiographs demonstrate a traumatic spondylolisthesis of the axis (Hangman's fracture) with an oblique fracture line through the pars interarticularis, minimal translation, but extreme angulation (>11 degrees). The C2-C3 disc space appears disrupted posteriorly. According to the Levine-Edwards classification, what is the most appropriate initial management for this specific injury pattern (Type IIa)?
Options:
- Immediate application of heavy axial traction followed by a halo vest
- Halo vest applied with gentle compression and extension
- Halo vest applied in slight flexion
- Anterior cervical discectomy and fusion at C2-C3
- Posterior C1-C2 transarticular screw fixation
Correct Answer: Halo vest applied with gentle compression and extension
Explanation:
The scenario describes a Levine-Edwards Type IIa Hangman's fracture. This injury is caused by a flexion-distraction mechanism, leading to severe angulation with minimal initial translation. A critical point in management is that axial traction is STRICTLY CONTRAINDICATED, as it will exacerbate the distraction and worsen the deformity. The appropriate non-operative management involves the application of a halo vest under gentle compression and extension to reduce the angulation and stabilize the fracture.
Question 4:
A 14-year-old male presents with worsening night pain in his distal femur. The radiograph shows a mixed lytic/sclerotic lesion with a 'sunburst' periosteal reaction and Codman's triangle. A biopsy confirms conventional osteosarcoma. Which of the following genetic alterations is most classically associated with the pathogenesis of this tumor?
Options:
- t(11;22) translocation
- Mutations in the p53 and Rb tumor suppressor genes
- t(X;18) translocation
- Amplification of the c-myc oncogene
- t(2;13) translocation
Correct Answer: Mutations in the p53 and Rb tumor suppressor genes
Explanation:
Conventional osteosarcoma is highly associated with mutations in the p53 (associated with Li-Fraumeni syndrome) and Rb (retinoblastoma) tumor suppressor genes. Option A (t(11;22)) is characteristic of Ewing sarcoma (EWS-FLI1 fusion). Option C (t(X;18)) is seen in Synovial Sarcoma (SYT-SSX). Option E (t(2;13)) is associated with Alveolar Rhabdomyosarcoma (PAX3-FOXO1).
Question 5:
A 55-year-old diabetic patient presents with a swollen, erythematous, and warm foot. Assuming radiographs initially revealed midfoot fragmentation and subluxation, and follow-up radiographs 4 months later demonstrate absorption of fine bone debris and early fusion of large fragments. According to the Eichenholtz classification of Charcot arthropathy, which stage does this represent?
Options:
- Stage 0 (Inflammatory)
- Stage I (Development/Fragmentation)
- Stage II (Coalescence)
- Stage III (Remodeling/Consolidation)
- Stage IV (Chronic Deformity)
Correct Answer: Stage II (Coalescence)
Explanation:
The Eichenholtz classification describes the natural history of Charcot neuroarthropathy. Stage 0 is the inflammatory phase (erythema, edema, warmth, normal radiographs or mild osteopenia). Stage I (Fragmentation) is characterized by joint subluxation, debris formation, and fragmentation. Stage II (Coalescence) is marked by the absorption of fine debris, early sclerosis, and fusion of larger fragments as the acute inflammation subsides. Stage III (Consolidation/Remodeling) shows remodeling of the bone ends, decreased sclerosis, and a stable (though often deformed) joint.
Question 6:
In the context of modularity in total hip arthroplasty (THA), which of the following is the primary mechanism of failure associated with trunnionosis at the head-neck junction?
Options:
- Galvanic corrosion due to dissimilar metals in a static environment
- Mechanically assisted crevice corrosion and fretting
- Pitting corrosion from high chloride physiological fluids
- Intergranular corrosion at grain boundaries
- Stress corrosion cracking from cyclic loading only
Correct Answer: Mechanically assisted crevice corrosion and fretting
Explanation:
Trunnionosis refers to wear and corrosion at the modular head-neck junction of a THA. The primary mechanism is mechanically assisted crevice corrosion (MACC), which involves a combination of fretting (micromotion between the surfaces) that disrupts the passive oxide layer, and crevice corrosion (a localized drop in pH and oxygen depletion in the crevice) once the bulk material is exposed. While galvanic corrosion can contribute when mixed metals are used (e.g., CoCr head on Ti stem), fretting and MACC are the predominant driving factors.
Question 7:
A 6-week-old female is placed in a Pavlik harness for developmental dysplasia of the hip (DDH). At her 2-week follow-up, the mother notes the child is no longer kicking her right leg. On physical exam, there is an absence of active knee extension on the right side. What is the most appropriate next step in management?
Options:
- Immediate MRI of the lumbar spine to rule out tethered cord
- Discontinue the harness completely and apply a rigid hip spica cast
- Adjust the anterior straps to decrease the amount of hip flexion
- Adjust the posterior straps to decrease the amount of hip abduction
- Continue the harness unmodified and refer to pediatric neurology
Correct Answer: Adjust the anterior straps to decrease the amount of hip flexion
Explanation:
The infant is presenting with a femoral nerve palsy, which is the most common nerve palsy associated with the Pavlik harness. It is caused by hyperflexion of the hips, which compresses the femoral nerve against the inguinal ligament. The appropriate management is to adjust the anterior straps to decrease hip flexion, allowing the nerve to recover. Complete discontinuation is usually not necessary unless the palsy fails to resolve after adjustment. Posterior straps control abduction; hyperabduction can lead to avascular necrosis (AVN), not typically femoral nerve palsy.
Question 8:
A 22-year-old male sustains a proximal pole scaphoid fracture. Which of the following best describes the predominant arterial supply to the scaphoid that makes this specific fracture pattern highly prone to avascular necrosis (AVN) and nonunion?
Options:
- Volar carpal branch of the radial artery entering distally
- Dorsal carpal branch of the radial artery entering distally and flowing retrograde
- Volar carpal branch of the ulnar artery entering proximally
- Dorsal carpal branch of the ulnar artery entering distally
- Interosseous artery branches entering directly into the proximal pole
Correct Answer: Dorsal carpal branch of the radial artery entering distally and flowing retrograde
Explanation:
The scaphoid is primarily supplied by the dorsal carpal branch of the radial artery (supplying 70-80% of the bone, including the proximal pole). These vessels enter the scaphoid distally at the dorsal ridge and flow in a retrograde fashion toward the proximal pole. Because of this retrograde blood supply, fractures at the proximal pole disrupt the vascularity to the proximal fragment, leading to high rates of AVN and nonunion.
Question 9:
During a total knee arthroplasty (TKA) for a severe varus deformity, the surgeon resects the distal femur and proximal tibia. With spacer blocks inserted, the knee remains tight medially in both flexion and extension. To balance the gaps symmetrically, which structure should be released next?
Options:
- Posterior cruciate ligament
- Popliteus tendon
- Lateral collateral ligament
- Deep medial collateral ligament and posteromedial capsule
- Iliotibial band
Correct Answer: Deep medial collateral ligament and posteromedial capsule
Explanation:
In a varus knee undergoing TKA, a tight medial gap in both flexion and extension indicates a symmetric medial soft tissue contracture. The standard medial release sequence typically begins with the deep medial collateral ligament (MCL) and the posteromedial capsule. If the gap remains tight, further releases may include the superficial MCL (often off the tibia, maintaining the periosteal sleeve) and the pes anserinus. Releasing the lateral structures (LCL, IT band, popliteus) would worsen the varus imbalance.
Question 10:
A 30-year-old male presents in hypotensive shock following a motorcycle crash. Pelvic radiographs and CT demonstrate an anteroposterior compression type III (APC-III) injury according to the Young-Burgess classification. Which of the following ligamentous complexes are completely disrupted in this specific injury pattern?
Options:
- Symphysis pubis only
- Symphysis pubis, sacrotuberous, and sacrospinous ligaments
- Symphysis pubis, sacrotuberous, sacrospinous, and anterior sacroiliac ligaments
- Symphysis pubis, sacrotuberous, sacrospinous, anterior and posterior sacroiliac ligaments
- Posterior sacroiliac ligaments and iliolumbar ligaments only
Correct Answer: Symphysis pubis, sacrotuberous, sacrospinous, anterior and posterior sacroiliac ligaments
Explanation:
The Young-Burgess classification for APC injuries relies on progressive disruption of the pelvic ring from anterior to posterior. APC-I involves pubic diastasis <2.5 cm with intact posterior ligaments. APC-II involves diastasis >2.5 cm with disruption of the anterior sacroiliac (SI), sacrotuberous, and sacrospinous ligaments, but intact posterior SI ligaments (rotationally unstable, vertically stable). APC-III involves complete disruption of both the anterior and posterior SI ligaments, resulting in a globally (rotationally and vertically) unstable hemipelvis.
Question 11:
Which of the following statements most accurately describes the vascular anatomy and healing potential of the meniscus?
Options:
- The inner third is highly vascularized by the middle genicular artery
- The medial meniscus receives a significantly more robust blood supply than the lateral meniscus
- The blood supply penetrates from the peripheral capsule via the medial and lateral inferior genicular arteries
- Vascularity progressively increases with age, improving healing potential in older adults
- The popliteal artery provides direct terminal branches to the anterior horns of both menisci
Correct Answer: The blood supply penetrates from the peripheral capsule via the medial and lateral inferior genicular arteries
Explanation:
The blood supply to the menisci originates from the medial, lateral, and middle genicular arteries (predominantly the inferior genicular arteries). The vessels form a perimeniscal capillary plexus within the synovial and capsular tissues. Only the peripheral 10% to 30% of the menisci (the 'red-red' zone) is vascularized in adults, making this zone capable of healing after repair. The inner portions ('white-white' zone) are avascular and rely on diffusion from synovial fluid. Vascularity actually decreases with age.
Question 12:
In healthy hyaline articular cartilage, which of the following macromolecular components is primarily responsible for providing the tissue with its compressive strength and stiffness?
Options:
- Type II collagen
- Aggrecan
- Type I collagen
- Fibronectin
- Elastin
Correct Answer: Aggrecan
Explanation:
Aggrecan, a large proteoglycan, is the primary source of compressive strength in articular cartilage. It contains numerous negatively charged glycosaminoglycans (GAGs), such as chondroitin sulfate and keratan sulfate, which repel each other and attract water via the Donnan osmotic effect. This creates a swelling pressure that resists compressive loads. In contrast, the Type II collagen network provides the tensile strength and restrains the swelling pressure of the proteoglycans.
Question 13:
A 65-year-old male with a history of neurogenic claudication undergoes a posterior lumbar decompressive laminectomy. Hypertrophy of which of the following anatomical structures is most directly responsible for the dorsal compression of the thecal sac in central lumbar spinal stenosis?
Options:
- Posterior longitudinal ligament
- Anterior longitudinal ligament
- Ligamentum flavum
- Interspinous ligament
- Supraspinous ligament
Correct Answer: Ligamentum flavum
Explanation:
Central lumbar spinal stenosis is typically caused by a combination of disc bulging anteriorly, facet joint hypertrophy laterally, and hypertrophy/buckling of the ligamentum flavum posteriorly. The ligamentum flavum forms the dorsal margin of the spinal canal and its hypertrophy is the primary dorsal contributor to canal narrowing. The posterior longitudinal ligament is ventral to the thecal sac.
Question 14:
Following a primary Zone II flexor tendon repair, which of the following biological processes characterizes the 'proliferation' phase of tendon healing (typically peaking between 1 to 4 weeks post-repair)?
Options:
- Inflammatory cell infiltration, hematoma formation, and minimal tensile strength
- Maximum weakness of the repair site due to phagocytosis of necrotic tissue
- Increased collagen synthesis primarily orchestrated by epitenon and endotenon fibroblasts
- Remodeling of disorganized Type III collagen into longitudinally oriented Type I collagen
- Complete resolution of tissue edema with normalization of the extracellular matrix
Correct Answer: Increased collagen synthesis primarily orchestrated by epitenon and endotenon fibroblasts
Explanation:
Tendon healing occurs in three phases: inflammatory (days 1-7), proliferative (days 7-21/28), and remodeling (weeks to months). During the proliferative phase, fibroblasts (from the epitenon and endotenon) migrate to the repair site and synthesize abundant Type III collagen, increasing the mass and strength of the repair. The inflammatory phase is characterized by hematoma and macrophage activity (where the tendon is weakest), and the remodeling phase is characterized by the conversion of Type III to Type I collagen and cross-linking.
Question 15:
A 30-year-old female is diagnosed with a biopsy-proven giant cell tumor of the distal radius. Due to the extent of the lesion, she is treated with denosumab preoperatively. What is the precise mechanism of action of this pharmacological agent?
Options:
- It directly binds to and inhibits the RANK receptor on the surface of osteoclasts
- It binds to and inhibits the RANKL protein, preventing osteoclast formation and activation
- It induces targeted apoptosis of the neoplastic stromal cells through the p53 pathway
- It blocks the VEGF pathway to decrease tumor neoangiogenesis
- It acts as a synthetic analog of osteoprotegerin (OPG) produced by osteoblasts
Correct Answer: It binds to and inhibits the RANKL protein, preventing osteoclast formation and activation
Explanation:
Denosumab is a fully human monoclonal antibody that binds to Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL). Giant cell tumors of bone consist of neoplastic mononuclear stromal cells that overexpress RANKL, which in turn recruits and hyperactivates multinucleated giant cells (osteoclast-like cells) expressing the RANK receptor. By binding RANKL, denosumab prevents it from interacting with RANK on osteoclasts, severely halting bone resorption and leading to ossification of the tumor matrix.
Question 16:
According to the Seddon classification of nerve injuries, a peripheral nerve injury that involves complete disruption of the axon and myelin sheath, but preservation of the surrounding connective tissue framework (endoneurium, perineurium, and epineurium) is termed:
Options:
- Neuropraxia
- Axonotmesis
- Neurotmesis
- Wallerian degeneration
- Neuroma-in-continuity
Correct Answer: Axonotmesis
Explanation:
In the Seddon classification: Neuropraxia is a local conduction block with intact axons (demyelination); recovery is fast and complete. Axonotmesis involves disruption of the axon and myelin sheath, resulting in distal Wallerian degeneration, but the connective tissue tubes (endoneurium, perineurium, epineurium) remain intact. This guides the regenerating axons, allowing for spontaneous recovery at ~1 mm/day. Neurotmesis is a complete transection of the nerve including the connective tissue framework, requiring surgical repair for any functional recovery.
Question 17:
A 25-year-old male suffers a highly comminuted, closed tibial shaft fracture. Two hours later, he complains of severe leg pain out of proportion to the injury, worsening with passive stretch of the toes. Which of the following absolute or differential pressure readings is the most widely accepted and evidence-based threshold for diagnosing acute compartment syndrome and proceeding with fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Absolute compartment pressure > 45 mmHg
- Diastolic blood pressure minus compartment pressure < 30 mmHg
- Mean arterial pressure minus compartment pressure < 40 mmHg
- Systolic blood pressure minus compartment pressure < 30 mmHg
Correct Answer: Diastolic blood pressure minus compartment pressure < 30 mmHg
Explanation:
The threshold for diagnosing acute compartment syndrome is generally based on the differential pressure (Delta P), calculated as the Diastolic Blood Pressure minus the Absolute Compartment Pressure. A Delta P of less than 30 mmHg indicates that perfusion to the capillary beds is critically impaired, leading to muscle and nerve ischemia. Absolute pressures alone are less reliable because systemic blood pressure variations significantly affect tissue perfusion thresholds.
Question 18:
A 6-year-old boy presents with a painless limp. Radiographs show sclerosis and early fragmentation of the capital femoral epiphysis, consistent with Legg-Calvé-Perthes disease. According to Catterall, which of the following is considered a radiographic 'head at risk' sign?
Options:
- Medial subluxation of the femoral head
- Vertical orientation of the proximal femoral physis
- A V-shaped radiolucent defect in the lateral portion of the epiphysis and adjacent metaphysis (Gage sign)
- Sclerosis of the acetabular dome
- Varus angulation of the femoral neck greater than 15 degrees
Correct Answer: A V-shaped radiolucent defect in the lateral portion of the epiphysis and adjacent metaphysis (Gage sign)
Explanation:
Catterall described five clinical and radiographic 'head at risk' signs for Legg-Calvé-Perthes disease that correlate with a worse prognosis and higher risk of femoral head deformation. These include: 1) Gage's sign (a V-shaped radiolucent defect in the lateral epiphysis/metaphysis), 2) Calcification lateral to the epiphysis, 3) Lateral (not medial) subluxation of the femoral head, 4) A horizontal (not vertical) growth plate, and 5) Metaphyseal cysts.
Question 19:
A 35-year-old female sustains a twisting injury to her ankle. Radiographs reveal a transverse fracture of the medial malleolus and a spiral fracture of the proximal third of the fibula (Maisonneuve fracture). For this specific fracture pattern to occur, which of the following ligamentous structures MUST be completely disrupted?
Options:
- Anterior talofibular ligament
- Calcaneofibular ligament
- Syndesmotic ligament complex and interosseous membrane
- Spring ligament
- Cervical ligament
Correct Answer: Syndesmotic ligament complex and interosseous membrane
Explanation:
A Maisonneuve fracture is a pronounced variation of a pronation-external rotation (PER) injury. The mechanism involves external rotation of the talus, which either avulses the medial malleolus or ruptures the deltoid ligament, then disrupts the anterior inferior tibiofibular ligament, tears up the interosseous membrane all the way to the proximal fibula, and exits as a high fibular fracture. Therefore, the syndesmotic complex and the interosseous membrane up to the level of the fracture are intrinsically disrupted.
Question 20:
Which of the following surgical approaches for total hip arthroplasty (THA) uniquely utilizes a true internervous and intermuscular plane, dissecting superficially between the tensor fasciae latae and the sartorius, and deeply between the gluteus medius and the rectus femoris?
Options:
- Direct anterior approach (Smith-Petersen)
- Anterolateral approach (Watson-Jones)
- Direct lateral approach (Hardinge)
- Posterior approach (Moore/Southern)
- Posterolateral approach
Correct Answer: Direct anterior approach (Smith-Petersen)
Explanation:
The direct anterior (Smith-Petersen) approach exploits a true internervous plane. Superficially, the plane is between the sartorius (femoral nerve) and the tensor fasciae latae (superior gluteal nerve). Deeply, the plane is between the rectus femoris (femoral nerve) and the gluteus medius/minimus (superior gluteal nerve). The anterolateral (Watson-Jones) plane is between the TFL and gluteus medius (both superior gluteal nerve, thus not internervous). The direct lateral approach splits the gluteus medius and vastus lateralis.