Full Question & Answer Text (for Search Engines)
Question 1:
A 55-year-old male presents with a new-onset squeaking noise 3 years after a total hip arthroplasty. He is otherwise asymptomatic and radiographs show well-fixed components. What is the most likely biomechanical etiology of this phenomenon?
Options:
- Impingement of the neck on the rim causing edge loading
- Asymptomatic loosening of the femoral stem
- Corrosion at the head-neck junction (trunnionosis)
- Subclinical periprosthetic joint infection
- Catastrophic failure of a polyethylene liner
Correct Answer: Impingement of the neck on the rim causing edge loading
Explanation:
Ceramic-on-ceramic (CoC) bearing surfaces in total hip arthroplasty are known to occasionally produce a squeaking sound. The most common cause of squeaking in CoC articulations is edge loading, which often results from component malposition (e.g., steep cup inclination or excessive anteversion) leading to micro-separation, stripe wear, and loss of fluid film lubrication.
Question 2:
A 28-year-old male sustains a high-energy Pauwels type III femoral neck fracture. Compared to a Pauwels type I fracture, which of the following biomechanical forces is most significantly increased at the fracture site?
Options:
- Compressive forces
- Shear forces
- Tensile forces
- Rotational forces
- Torsional forces
Correct Answer: Shear forces
Explanation:
The Pauwels classification of femoral neck fractures is based on the angle of the fracture line relative to the horizontal plane. A type III fracture has an angle greater than 50 degrees, making it more vertically oriented. This vertical orientation significantly increases shear forces across the fracture site, leading to a higher risk of varus collapse, nonunion, and fixation failure.
Question 3:
A 6-week-old female is diagnosed with a completely dislocated left hip (Graf IV) and treated with a Pavlik harness. After 4 weeks of compliant wear, dynamic ultrasound shows the hip remains persistently dislocated. What is the most appropriate next step in management?
Options:
- Continue the Pavlik harness for an additional 4 weeks
- Transition to a rigid abduction orthosis (e.g., Ilfeld) or proceed to closed reduction and spica casting
- Perform an open reduction via a medial approach
- Perform a proximal femoral varus derotational osteotomy
- Observe and reassess at 6 months of age
Correct Answer: Transition to a rigid abduction orthosis (e.g., Ilfeld) or proceed to closed reduction and spica casting
Explanation:
According to established AAOS guidelines for Developmental Dysplasia of the Hip (DDH), failure of a Pavlik harness to reduce a dislocated hip after 3-4 weeks is an indication to discontinue the harness to prevent 'Pavlik harness disease' (acetabular damage/erosion). The appropriate next step is transitioning to a rigid abduction orthosis or proceeding directly to a closed reduction and spica casting in the operating room.
Question 4:
A 32-year-old carpenter sustains a laceration to the volar aspect of his index finger proximal phalanx, cutting the flexor digitorum profundus (FDP) and superficialis (FDS) tendons in Zone II. To permit an early active motion protocol safely, biomechanical studies suggest the core suture repair of the FDP tendon should consist of at least how many strands?
Options:
- 2 strands
- 4 strands
- 6 strands
- 8 strands
- Strand count is irrelevant if an epitendinous suture is used
Correct Answer: 4 strands
Explanation:
In flexor tendon repairs, biomechanical strength is directly proportional to the number of core suture strands crossing the repair site. Studies have demonstrated that a 2-strand repair is generally only strong enough for passive motion protocols. A minimum of a 4-strand core repair is required to withstand the forces generated during an early active motion protocol and reduce the risk of gap formation or rupture.
Question 5:
A 22-year-old collegiate soccer player requires ACL reconstruction. The surgeon opts for a bone-patellar tendon-bone (BTB) autograft. Compared to a 4-strand hamstring autograft, the BTB autograft has a higher incidence of which postoperative complication?
Options:
- Deep surgical site infection
- Graft rupture within 2 years
- Anterior knee pain and kneeling pain
- Hardware failure
- Hamstring weakness in deep flexion
Correct Answer: Anterior knee pain and kneeling pain
Explanation:
Both bone-patellar tendon-bone (BTB) and hamstring autografts provide excellent stability for ACL reconstruction. However, BTB autografts are historically and consistently associated with a higher incidence of donor site morbidity, specifically anterior knee pain and pain with kneeling. Hamstring grafts may result in a minor deficit in deep flexion strength but avoid extensor mechanism morbidity.
Question 6:
A 65-year-old male presents with bilateral leg pain that worsens with walking. The pain is relieved by sitting or leaning over a shopping cart. Which of the following clinical findings is most useful for confirming that his symptoms are neurogenic rather than vascular in origin?
Options:
- Pain onset occurring consistently after a fixed walking distance
- Decreased ankle-brachial index (< 0.8)
- Pain relief strictly isolated to standing stationary
- Presence of normal pedal pulses and an ankle-brachial index > 0.9
- Loss of hair over the anterior tibia and shiny skin
Correct Answer: Presence of normal pedal pulses and an ankle-brachial index > 0.9
Explanation:
The patient's presentation of relief with sitting or spinal flexion (shopping cart sign) is classic for neurogenic claudication due to lumbar spinal stenosis. Vascular claudication is typically relieved simply by resting/standing stationary and occurs at a set distance. The presence of normal pedal pulses and a normal ankle-brachial index (>0.9) objectively rules out vascular claudication, making it the best finding to differentiate the two.
Question 7:
A 15-year-old boy is diagnosed with high-grade intramedullary osteosarcoma of the distal femur. What is the single most important prognostic factor for his overall survival?
Options:
- Histologic subtype of the tumor
- Presence of metastatic disease at presentation
- Tumor size and volume at diagnosis
- Anatomic location of the primary tumor
- Alkaline phosphatase levels at diagnosis
Correct Answer: Presence of metastatic disease at presentation
Explanation:
In osteosarcoma, the single most important prognostic factor for survival is whether metastatic disease is present at the time of diagnosis. For patients presenting with localized disease, the percentage of tumor necrosis following neoadjuvant chemotherapy (>90% necrosis indicates a good response) becomes the most important prognostic factor.
Question 8:
A 40-year-old recreational athlete sustains an acute Achilles tendon rupture. When comparing non-operative management utilizing an early functional rehabilitation protocol against operative repair, recent high-level literature (e.g., Willits et al.) demonstrates which of the following?
Options:
- A significantly higher re-rupture rate in the non-operative group
- Similar re-rupture rates between both groups
- A significantly higher deep infection rate in the non-operative group
- Superior long-term functional outcomes favoring operative management
- A higher incidence of sural nerve injury in the non-operative group
Correct Answer: Similar re-rupture rates between both groups
Explanation:
Historically, non-operative management of Achilles tendon ruptures was associated with higher re-rupture rates. However, modern level I studies (e.g., Willits et al.) have demonstrated that when non-operative management is paired with an early functional rehabilitation protocol (early weight-bearing in an orthosis), the re-rupture rates and functional outcomes are statistically similar to those of operative repair, while completely avoiding surgical complications like infection or nerve injury.
Question 9:
During fracture healing via secondary intention, a soft callus is eventually replaced by hard callus, which consists of woven bone. Which of the following characteristics best describes woven bone when compared to mature lamellar bone?
Options:
- Highly organized, parallel collagen fibers
- Lower osteocyte cell density
- Slow, organized deposition rate
- Isotropic mechanical properties
- Anisotropic mechanical properties
Correct Answer: Isotropic mechanical properties
Explanation:
Woven bone is characterized by randomly oriented collagen fibers, a high cell density (more osteocytes), and rapid formation. Because the collagen fibers lack a specific directional orientation, woven bone has isotropic mechanical properties, meaning it exhibits equal mechanical strength in all directions. In contrast, lamellar bone is highly organized, slowly formed, and anisotropic (stronger in the direction of the loaded axis).
Question 10:
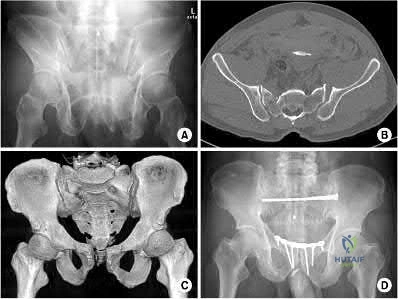
A 35-year-old male is brought to the trauma bay after a motorcycle accident. A pelvic radiograph shows a completely disrupted pubic symphysis and widened sacroiliac joints bilaterally (APC type III injury). He is hemodynamically unstable. What is the most common anatomical source of life-threatening hemorrhage in this injury pattern?
Options:
- Superior gluteal artery
- Presacral venous plexus and cancellous bone
- Internal pudendal artery
- External iliac artery
- Obturator artery
Correct Answer: Presacral venous plexus and cancellous bone
Explanation:
While arterial bleeding (commonly from the superior gluteal or internal pudendal arteries) can occur and is often addressed by angioembolization, the vast majority (approximately 80-90%) of life-threatening hemorrhage in blunt pelvic ring injuries arises from the presacral venous plexus and the fractured cancellous bony surfaces. Venous and bony bleeding are primarily managed by reducing pelvic volume (e.g., with a pelvic binder or external fixator).
Question 11:
A 12-year-old obese male presents with a mild, stable right slipped capital femoral epiphysis (SCFE). Which of the following conditions is an absolute indication for prophylactic in situ pinning of the contralateral asymptomatic hip?
Options:
- Age greater than 14 years at presentation
- Obesity (BMI > 95th percentile)
- Presence of an underlying endocrine disorder
- African American race
- Male sex
Correct Answer: Presence of an underlying endocrine disorder
Explanation:
The risk of developing a contralateral SCFE is approximately 20-40% overall. However, prophylactic pinning of the contralateral asymptomatic hip is strongly indicated in patients with underlying endocrinopathies (e.g., hypothyroidism, growth hormone deficiency), renal osteodystrophy, prior pelvic radiation therapy, or an unusually young age at presentation (<10 years), as their risk of bilateral involvement approaches 100%.
Question 12:
A 65-year-old female presents with a painful 'catch' and a palpable, audible pop in her knee when extending from 40 degrees of flexion to full extension. She is 1 year status-post a posterior-stabilized total knee arthroplasty. If non-operative management fails, what is the most appropriate surgical treatment?
Options:
- Revision of the femoral component to a cruciate-retaining design
- Arthroscopic excision of a fibrous nodule
- Isolated patellar resurfacing
- Lateral retinacular release
- Tibial tubercle osteotomy for patellar tracking
Correct Answer: Arthroscopic excision of a fibrous nodule
Explanation:
The patient's symptoms are classic for patellar clunk syndrome, a complication specific to posterior-stabilized (PS) total knee arthroplasty designs. It occurs when a fibrosynovial nodule develops on the deep surface of the distal quadriceps tendon and catches in the intercondylar box of the femoral component during extension. The treatment of choice after failed conservative management is arthroscopic or open excision of the nodule.
Question 13:
During an open carpal tunnel release, the surgeon carefully incises the transverse carpal ligament, mindful of the recurrent motor branch of the median nerve to the thenar muscles. According to anatomic studies (e.g., Lanz's classification), what is the most common path of the recurrent motor branch?
Options:
- Extraligamentous, branching distal to the transverse carpal ligament and recurring to the thenar muscles
- Subligamentous, branching deep to the transverse carpal ligament
- Transligamentous, piercing directly through the transverse carpal ligament
- Branching from the ulnar aspect of the median nerve
- Passing dorsal to the flexor tendons before entering the thenar musculature
Correct Answer: Extraligamentous, branching distal to the transverse carpal ligament and recurring to the thenar muscles
Explanation:
According to Lanz's anatomic classification of the median nerve in the carpal tunnel, the extraligamentous variation is the most common (found in roughly 50-80% of cases). In this pattern, the recurrent motor branch arises distal to the transverse carpal ligament and recurves over its distal edge to innervate the thenar muscles. Transligamentous, subligamentous, and ulnar-sided branches are less common variants.
Question 14:
A 24-year-old rugby player has recurrent anterior shoulder instability with 25% anterior glenoid bone loss on a 3D CT scan. A Latarjet procedure is performed. What is the primary biomechanical stabilizing mechanism of this procedure when the shoulder is in the apprehension position (abduction/external rotation)?
Options:
- Bony augmentation of the glenoid arc by the coracoid graft
- Sling effect of the conjoined tendon against the inferior subscapularis and capsule
- Anatomic repair of the torn coracoacromial ligament
- Tensioning of the middle glenohumeral ligament (MGHL)
- Rerouting the long head of the biceps brachii
Correct Answer: Sling effect of the conjoined tendon against the inferior subscapularis and capsule
Explanation:
The Latarjet procedure involves transferring the coracoid process with the attached conjoined tendon to the anterior glenoid. While the bony block restores the glenoid arc (the 'bony effect'), biomechanical studies have demonstrated that the primary stabilizing mechanism in abduction and external rotation is the dynamic 'sling effect.' The conjoined tendon acts as a hammock against the inferior capsule and lower subscapularis, preventing anterior translation of the humeral head.
Question 15:
A 19-year-old Asian male presents with painless, unilateral, progressive weakness and atrophy of his right hand intrinsic muscles. Sensory exam is normal, and his lower extremities are unaffected. A dynamic flexion MRI of the cervical spine reveals anterior displacement of the posterior dural sac, compressing the lower cervical cord. What is the most likely diagnosis?
Options:
- Amyotrophic lateral sclerosis
- Cervical spondylotic myelopathy
- Syringomyelia
- Hirayama disease
- Parsonage-Turner syndrome
Correct Answer: Hirayama disease
Explanation:
The clinical picture of progressive unilateral distal upper extremity atrophy in a young male, coupled with dynamic flexion MRI showing forward displacement of the posterior dural sac causing cord compression, is pathognomonic for Hirayama disease (juvenile muscular atrophy of the distal upper extremity). The repeated dynamic compression leads to ischemia of the anterior horn cells in the lower cervical cord.
Question 16:
Tranexamic acid (TXA) is frequently administered during total joint arthroplasty to minimize perioperative blood loss. Which of the following describes the primary mechanism of action of tranexamic acid?
Options:
- Irreversible inhibition of cyclooxygenase enzymes
- Reversible competitive blockade of lysine binding sites on plasminogen
- Direct inhibition of Factor Xa in the coagulation cascade
- Allosteric activation of antithrombin III
- Inhibition of ADP-induced platelet aggregation
Correct Answer: Reversible competitive blockade of lysine binding sites on plasminogen
Explanation:
Tranexamic acid (TXA) is a synthetic analog of the amino acid lysine. It acts as an antifibrinolytic agent by reversibly and competitively binding to the lysine receptor sites on plasminogen. This prevents plasminogen from converting into the active enzyme plasmin, thereby inhibiting the degradation of fibrin clots.
Question 17:
A 32-year-old male sustains a closed tibia fracture and develops intense leg pain out of proportion to the injury. You suspect acute compartment syndrome. Which of the following pressure parameters is considered the most reliable threshold indication for performing a four-compartment fasciotomy?
Options:
- Absolute compartment pressure > 30 mmHg
- Absolute compartment pressure > 45 mmHg
- Diastolic blood pressure minus compartment pressure (Delta P) < 30 mmHg
- Mean arterial pressure minus compartment pressure (Delta P) < 40 mmHg
- Systolic blood pressure minus compartment pressure (Delta P) < 20 mmHg
Correct Answer: Diastolic blood pressure minus compartment pressure (Delta P) < 30 mmHg
Explanation:
The differential pressure (Delta P) is universally recognized as more reliable than absolute compartment pressure for diagnosing acute compartment syndrome. A Delta P is calculated by subtracting the intracompartmental pressure from the patient's diastolic blood pressure. A Delta P of less than 30 mmHg represents inadequate tissue perfusion pressure and is an absolute indication for emergency fasciotomy.
Question 18:
An infant with severe idiopathic clubfoot (talipes equinovarus) is managed with serial casting according to the Ponseti method. According to this treatment protocol, which component of the deformity is corrected last?
Options:
- Cavus
- Adductus
- Varus
- Equinus
- Supination
Correct Answer: Equinus
Explanation:
The Ponseti method follows a strict sequence of deformity correction summarized by the acronym CAVE: Cavus (elevating the first ray to match the forefoot supination), Adductus, Varus, and finally Equinus. The equinus contracture is addressed last, and in about 80% of cases, correction requires a percutaneous Achilles tenotomy prior to the final cast application.
Question 19:
A 45-year-old female presents with a painful bunion and clinically evident hypermobility of the first tarsometatarsal (TMT) joint. Weight-bearing radiographs demonstrate a hallux valgus angle of 40 degrees and an intermetatarsal angle (IMA) of 18 degrees. Which surgical procedure is most appropriate to comprehensively address her pathology?
Options:
- Distal chevron osteotomy
- Akin osteotomy
- Proximal opening wedge osteotomy alone
- First tarsometatarsal arthrodesis (Lapidus procedure)
- Keller resection arthroplasty
Correct Answer: First tarsometatarsal arthrodesis (Lapidus procedure)
Explanation:
The patient has a severe hallux valgus deformity (IMA > 15 degrees) combined with first TMT joint hypermobility. The Lapidus procedure (arthrodesis of the first tarsometatarsal joint) addresses both the severe metatarsus primus varus and the hypermobility of the first ray at its apex, making it the most appropriate and biomechanically sound choice for this specific clinical scenario.
Question 20:
A 30-year-old female is diagnosed with an expansile, lytic lesion in her distal femur that extends to the subchondral bone. Biopsy confirms a Giant Cell Tumor (GCT) of bone. She is treated preoperatively with denosumab. What is the molecular target of denosumab in the treatment of this tumor?
Options:
- The RANK receptor on the surface of osteoclast precursors
- Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL) secreted by neoplastic stromal cells
- Osteoprotegerin (OPG)
- Vascular Endothelial Growth Factor (VEGF)
- Matrix Metalloproteinases (MMPs)
Correct Answer: Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL) secreted by neoplastic stromal cells
Explanation:
In a Giant Cell Tumor of bone, the actual neoplastic cells are the mononuclear spindle-like stromal cells. These cells secrete excessive amounts of RANKL, which recruits and activates the reactive multinucleated giant cells (osteoclasts) that cause bone destruction. Denosumab is a monoclonal antibody that specifically targets and binds to RANKL, preventing it from interacting with the RANK receptor on osteoclast precursors, thereby halting bone lysis.
Question 21:
Which of the following is a major criterion for the diagnosis of Periprosthetic Joint Infection (PJI) according to the 2018 International Consensus Meeting (ICM)?
Options:
- Purulence in the affected joint
- Elevated synovial C-reactive protein (CRP)
- A single positive culture of a highly virulent organism
- Two positive periprosthetic cultures with phenotypically identical organisms
- Elevated synovial leukocyte esterase
Correct Answer: Two positive periprosthetic cultures with phenotypically identical organisms
Explanation:
According to the 2018 ICM criteria for PJI, there are two major criteria: 1) Two positive periprosthetic cultures with phenotypically identical organisms, and 2) A sinus tract communicating with the joint. The presence of either major criterion is diagnostic for PJI. The other options represent minor criteria or findings that contribute to the aggregate score but are not major criteria on their own.
Question 22:
A 24-year-old male presents with a slow-growing, painful soft tissue mass around the knee. Core needle biopsy reveals a biphasic tumor with both spindle cells and epithelial cells. What is the characteristic cytogenetic abnormality associated with this pathology?
Options:
- t(11;22)
- t(X;18)
- t(9;22)
- t(12;16)
- t(2;13)
Correct Answer: t(X;18)
Explanation:
The patient has a biphasic synovial sarcoma. Synovial sarcoma is uniquely characterized by the t(X;18)(p11;q11) translocation, which results in the SYT-SSX fusion gene. t(11;22) is characteristic of Ewing sarcoma, t(9;22) is associated with myxoid chondrosarcoma (and CML), t(12;16) is seen in myxoid liposarcoma, and t(2;13) is seen in alveolar rhabdomyosarcoma.
Question 23:
A 13-year-old obese boy undergoes in situ pinning for a stable slipped capital femoral epiphysis (SCFE). During the procedure, the screw is inadvertently placed in the anterosuperior quadrant of the femoral head. What is the most likely complication associated with this specific pin position?
Options:
- Chondrolysis
- Osteonecrosis
- Slip progression
- Femoral neck fracture
- Labral tear
Correct Answer: Osteonecrosis
Explanation:
The blood supply to the femoral head relies heavily on the lateral epiphyseal branches of the medial femoral circumflex artery, which enter the femoral head posterosuperiorly. Pin placement in the anterosuperior quadrant of the femoral head directly endangers this blood supply, significantly increasing the risk of iatrogenic osteonecrosis (avascular necrosis). The ideal screw position is in the center of the epiphysis.
Question 24:
When a constant magnitude of load is applied to a viscoelastic material over a prolonged period, the material undergoes increasing progressive deformation. This biomechanical property is known as:
Options:
- Stress relaxation
- Hysteresis
- Creep
- Fatigue failure
- Anisotropy
Correct Answer: Creep
Explanation:
Creep is defined as the progressive, time-dependent deformation of a viscoelastic material under a constant load. Stress relaxation is the decrease in stress (force) over time when the material is held at a constant deformation. Hysteresis is the energy lost (usually as heat) during the loading and unloading cycle.
Question 25:
A 45-year-old man sustains a high-energy knee injury in a motorcycle accident. Based on the Schatzker classification, a bicondylar tibial plateau fracture with complete dissociation of the metaphysis from the diaphysis is classified as:
Options:
- Schatzker III
- Schatzker IV
- Schatzker V
- Schatzker VI
- Schatzker II
Correct Answer: Schatzker VI
Explanation:
A Schatzker VI fracture is defined by complete metaphyseal-diaphyseal dissociation, often accompanied by severe soft tissue injury. Schatzker V is a bicondylar fracture but maintains continuity between the articular segment and the diaphysis. Schatzker I-III involve the lateral plateau, and IV involves the medial plateau.
Question 26:
A 50-year-old man presents with chronic neck pain radiating down his right arm. Neurological examination reveals marked weakness in elbow extension, wrist flexion, and finger extension. He also has decreased sensation over the dorsal aspect of the long finger. The triceps reflex is 1+. Which cervical nerve root is most likely compressed?
Options:
Correct Answer: C7
Explanation:
A C7 radiculopathy classically presents with motor weakness in the triceps (elbow extension), wrist flexors (flexor carpi radialis), and finger extensors. Patients often have a diminished triceps reflex and sensory changes over the long (middle) finger. C6 radiculopathy would affect wrist extensors and the brachioradialis reflex, with sensory changes in the thumb and index finger.
Question 27:
A 28-year-old carpenter sustains a deep laceration to his volar palm, exactly at the proximal edge of the A1 pulley, resulting in an inability to flex his digits. In which flexor tendon zone did this injury occur?
Options:
- Zone I
- Zone II
- Zone III
- Zone IV
- Zone V
Correct Answer: Zone II
Explanation:
Zone II (historically termed 'no man's land' by Bunnell due to historically poor surgical outcomes) extends from the proximal aspect of the A1 pulley to the insertion of the flexor digitorum superficialis (FDS) on the middle phalanx. Both FDS and FDP tendons run tightly together in the fibro-osseous sheath in this zone, making repair technically demanding.
Question 28:
Which of the following ligaments provides the primary and strongest stabilizing force to the Lisfranc joint complex in the midfoot?
Options:
- The dorsal ligament connecting the medial cuneiform and second metatarsal base
- The plantar ligament connecting the medial cuneiform and second metatarsal base
- The interosseous ligament connecting the medial cuneiform and second metatarsal base
- The dorsal ligament connecting the lateral cuneiform and third metatarsal
- The plantar ligament connecting the navicular and medial cuneiform
Correct Answer: The interosseous ligament connecting the medial cuneiform and second metatarsal base
Explanation:
The Lisfranc ligament is an interosseous ligament that courses from the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. It is the largest and strongest ligament of the complex and provides the primary stabilizing force. The dorsal ligaments are the weakest, making dorsal dislocation the most common direction of injury.
Question 29:
During arthroscopic evaluation of a 22-year-old baseball pitcher's shoulder, a superior labral anterior to posterior (SLAP) tear is identified. The labrum is visibly frayed, but the biceps anchor is completely intact and firmly attached to the superior glenoid tubercle without any detachment. What type of SLAP lesion is this?
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type I
Explanation:
Type I SLAP tears are characterized by fraying and degeneration of the superior labrum with an intact biceps anchor. Type II involves detachment of the superior labrum and biceps anchor from the glenoid. Type III is a bucket-handle tear of the labrum with an intact biceps anchor. Type IV is a bucket-handle tear that extends into the biceps tendon.
Question 30:
A 30-year-old male is admitted after suffering a closed tibial shaft fracture. Twelve hours later, he complains of severe pain out of proportion to his injury and pain with passive toe extension. Which of the following pressure measurements is the most reliable threshold indicating the need for an emergent fasciotomy?
Options:
- Absolute compartment pressure of 20 mmHg
- Absolute compartment pressure of 25 mmHg
- Delta pressure (Diastolic blood pressure minus compartment pressure) of less than 30 mmHg
- Delta pressure (Systolic blood pressure minus compartment pressure) of less than 45 mmHg
- Mean arterial pressure minus compartment pressure of less than 30 mmHg
Correct Answer: Delta pressure (Diastolic blood pressure minus compartment pressure) of less than 30 mmHg
Explanation:
The delta pressure (Δp) is calculated as the diastolic blood pressure minus the intracompartmental pressure. A Δp of less than 30 mmHg is considered highly specific for acute compartment syndrome and is a standard indication for emergent four-compartment fasciotomy of the leg. Absolute pressures are less reliable because tissue perfusion depends on the perfusion gradient.
Question 31:
In normal mature articular cartilage, which zone is characterized by having the highest concentration of proteoglycans, the lowest concentration of water, and collagen fibers arranged perpendicularly (vertically) to the joint surface?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage contains collagen fibers oriented perpendicular to the articular surface. It contains the highest concentration of proteoglycans and the lowest water content, making it critical for resisting compressive forces. The superficial zone has water content highest, collagen parallel to surface, and lowest proteoglycan content.
Question 32:
During a total hip arthroplasty, the surgeon decides to use a high-offset femoral stem, which effectively lateralizes the greater trochanter. What is the expected biomechanical effect of this modification?
Options:
- Decrease the abductor moment arm and increase joint reaction force
- Increase the abductor moment arm and decrease joint reaction force
- Decrease the abductor moment arm and decrease joint reaction force
- Increase the abductor moment arm and increase joint reaction force
- Increase the center of rotation and decrease the bending moment on the stem
Correct Answer: Increase the abductor moment arm and decrease joint reaction force
Explanation:
Increasing the femoral offset lateralizes the greater trochanter and the insertion of the hip abductors. This increases the abductor moment arm (lever arm). As a result, less force is required from the abductor muscles to maintain a level pelvis during single-leg stance, which in turn decreases the overall joint reaction force across the hip joint.
Question 33:
A 35-year-old manual laborer presents with chronic dorsal wrist pain and decreased grip strength. Radiographs demonstrate sclerosis and early collapse of the lunate, accompanied by ulnar minus (negative) variance. Which of the following is the most appropriate initial surgical management for this early-stage (Stage II or IIIA) Kienbock's disease?
Options:
- Proximal row carpectomy
- Total wrist arthrodesis
- Radial shortening osteotomy
- Lunate excision and silastic replacement
- Ulnar shortening osteotomy
Correct Answer: Radial shortening osteotomy
Explanation:
In early stages of Kienbock's disease (avascular necrosis of the lunate) where the lunate has not severely collapsed or fragmented (Stage I, II, or IIIA) and there is negative ulnar variance, joint leveling procedures are indicated. A radial shortening osteotomy (or ulnar lengthening) shifts load off the radiolunate joint onto the ulnocarpal joint, allowing lunate revascularization. Proximal row carpectomy or arthrodesis are salvage procedures for advanced disease (Stage IIIB/IV).
Question 34:
A 6-month-old female is diagnosed with Developmental Dysplasia of the Hip (DDH). An anterior-posterior radiograph of the pelvis is evaluated. Which of the following radiographic parameters specifically indicates superior (proximal) displacement of the femoral head?
Options:
- A broken Shenton's line
- The femoral head ossific nucleus lies medial to Perkin's line
- The femoral head ossific nucleus lies inferior to Hilgenreiner's line
- An acetabular index of 20 degrees
- A center-edge angle of Wiberg of 35 degrees
Correct Answer: A broken Shenton's line
Explanation:
Shenton's line is a continuous curve formed by the medial border of the femoral neck and the superior border of the obturator foramen. A break in this line indicates proximal (superior) displacement of the femur relative to the pelvis. Normal position requires the ossific nucleus to be medial to Perkin's line (evaluates lateral displacement) and inferior to Hilgenreiner's line.
Question 35:
Which variant of osteosarcoma is characteristically located on the surface of the bone, frequently involves the posterior cortex of the distal femur, features a heavily ossified broad base on imaging, and generally carries an excellent prognosis with wide surgical resection alone?
Options:
- Parosteal osteosarcoma
- Periosteal osteosarcoma
- High-grade surface osteosarcoma
- Telangiectatic osteosarcoma
- Intramedullary osteosarcoma
Correct Answer: Parosteal osteosarcoma
Explanation:
Parosteal osteosarcoma is a low-grade surface tumor classically located at the posterior aspect of the distal femur. It presents as a dense, heavily ossified mass on a broad base. Due to its low-grade nature, it has the best prognosis among osteosarcoma subtypes, and wide surgical resection is typically curative without neoadjuvant chemotherapy. Periosteal osteosarcoma is intermediate-grade, often diaphyseal, with prominent chondroblastic features.
Question 36:
A 25-year-old male sustains a severe flexion-distraction injury resulting in a burst fracture of T4 with complete paralysis and loss of sensation below the nipples. He presents to the trauma bay with a blood pressure of 80/40 mmHg and a heart rate of 50 beats per minute. His extremities are warm and flushed. This specific clinical presentation is most consistent with:
Options:
- Hemorrhagic shock
- Spinal shock
- Neurogenic shock
- Cardiogenic shock
- Septic shock
Correct Answer: Neurogenic shock
Explanation:
Neurogenic shock is a distributive shock caused by a loss of sympathetic tone following a high thoracic (T6 and above) or cervical spinal cord injury. It presents with the classic triad of hypotension, bradycardia, and warm, flushed extremities (peripheral vasodilation). Spinal shock, distinct from neurogenic shock, refers to the temporary loss of all spinal reflexes below the level of injury (e.g., absent bulbocavernosus reflex) immediately following spinal cord injury.
Question 37:
Which of the following statements most accurately describes the mechanism and requirements of primary (direct) bone healing?
Options:
- It occurs via endochondral ossification and a robust cartilage intermediate.
- It requires absolute stability and occurs via cutting cones crossing the fracture site.
- It relies on controlled micromotion to stimulate abundant bridging callus formation.
- It proceeds primarily through intramembranous ossification mediated solely by the periosteum.
- It is the typical mode of healing seen with intramedullary nailing of comminuted diaphyseal fractures.
Correct Answer: It requires absolute stability and occurs via cutting cones crossing the fracture site.
Explanation:
Primary (direct) bone healing occurs without a cartilage intermediate and without the formation of a visible callus. It requires absolute stability (rigid fixation with no micromotion, such as with compression plating) and intimate bone contact. The mechanism involves osteoclastic cutting cones that cross the fracture line, immediately followed by osteoblasts laying down new osteons (Haversian remodeling).
Question 38:
In Anterior Cruciate Ligament (ACL) reconstruction, graft choice depends on multiple factors including initial graft strength. Which of the following commonly utilized autografts possesses the highest initial ultimate tensile load?
Options:
- Bone-patellar tendon-bone (10 mm)
- Quadrupled hamstring (semitendinosus and gracilis)
- Quadriceps tendon (10 mm without bone block)
- Single-strand semitendinosus
- Patellar tendon (8 mm)
Correct Answer: Quadrupled hamstring (semitendinosus and gracilis)
Explanation:
A quadrupled hamstring autograft (semitendinosus and gracilis) has the highest initial ultimate tensile load of the common grafts, averaging approximately 4000-4100 N. This is stronger than a standard 10 mm bone-patellar tendon-bone (BPTB) graft (~2900 N) and significantly stronger than the native ACL, which has an ultimate tensile load of approximately 2160 N.
Question 39:
A 55-year-old poorly controlled diabetic patient presents with a warm, swollen, erythematous right foot. Radiographs show periarticular osteopenia and early joint subluxation in the midfoot. Differentiating acute Charcot neuroarthropathy from osteomyelitis is critical. Which of the following advanced diagnostic modalities offers the highest specificity for distinguishing true infection from Charcot arthropathy?
Options:
- Erythrocyte sedimentation rate (ESR) alone
- Triple-phase technetium-99m bone scan
- MRI without intravenous gadolinium
- Technetium-99m hexamethylpropyleneamine oxime (HMPAO) scan alone
- Indium-111 labeled leukocyte (WBC) scan combined with technetium-99m sulfur colloid marrow scan
Correct Answer: Indium-111 labeled leukocyte (WBC) scan combined with technetium-99m sulfur colloid marrow scan
Explanation:
Differentiating Charcot from osteomyelitis is difficult because both show hyperperfusion and bony changes. A combined Indium-111 WBC scan and Tc-99m sulfur colloid bone marrow scan is highly specific. In Charcot arthropathy, there is increased bone turnover and marrow expansion, leading to matched uptake on both scans. In osteomyelitis, the infection suppresses the normal marrow, leading to mismatched uptake (increased WBC uptake, decreased marrow uptake).
Question 40:
The recurrent motor branch of the median nerve provides critical motor innervation to the thenar eminence. Which of the following muscles is typically NOT innervated by the recurrent motor branch of the median nerve?
Options:
- Abductor pollicis brevis
- Opponens pollicis
- Superficial head of the flexor pollicis brevis
- Deep head of the flexor pollicis brevis
- None of the above; all are innervated by the recurrent median nerve.
Correct Answer: Deep head of the flexor pollicis brevis
Explanation:
The thenar muscles include the abductor pollicis brevis (APB), opponens pollicis (OP), and flexor pollicis brevis (FPB). The recurrent motor branch of the median nerve innervates the APB, OP, and the superficial head of the FPB. The deep head of the FPB is typically innervated by the deep branch of the ulnar nerve (though dual innervation can occur). The adductor pollicis is also innervated by the ulnar nerve.
Question 41:
Which zone of articular cartilage has the highest concentration of proteoglycans, the lowest water content, and collagen fibers oriented perpendicular to the joint surface?
Options:
- Superficial (tangential) zone
- Transitional (middle) zone
- Deep (radial) zone
- Calcified zone
- Subchondral bone plate
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone contains the highest concentration of proteoglycans and the lowest water content. The collagen fibers are thick and oriented perpendicularly to the articular surface to resist compressive loads. The superficial zone has fibers parallel to the surface to resist shear forces.
Question 42:
A revision total hip arthroplasty is performed for a fractured modular neck. Examination of the taper junction reveals black debris and pitting. What is the primary initiating mechanism of corrosion at the modular taper junction of a titanium stem and cobalt-chrome head?
Options:
- Galvanic corrosion
- Crevice corrosion
- Fretting corrosion
- Pitting corrosion
- Intergranular corrosion
Correct Answer: Fretting corrosion
Explanation:
Fretting corrosion (mechanically assisted crevice corrosion) is the primary initiating mode of failure at modular junctions in total joint arthroplasty. Micro-motion mechanically disrupts the protective passivation (oxide) layer, which then allows crevice and galvanic corrosion to occur.
Question 43:
In the Ponseti method for the treatment of idiopathic clubfoot, which of the following represents the correct sequence of deformity correction?
Options:
- Cavus, Adductus, Varus, Equinus
- Cavus, Equinus, Varus, Adductus
- Varus, Adductus, Cavus, Equinus
- Equinus, Varus, Adductus, Cavus
- Adductus, Varus, Equinus, Cavus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The correct sequence of correction in the Ponseti method follows the acronym CAVE: Cavus (corrected by elevating the first ray), Adductus, Varus, and finally Equinus (which often requires a percutaneous tendoachilles lengthening).
Question 44:
When applying a circumferential pelvic binder for a hemodynamically unstable APC-III pelvic ring injury, what is the optimal anatomic landmark for placement to maximize reduction and minimize complications?
Options:
- Iliac crests
- Anterior superior iliac spines
- Greater trochanters
- Symphysis pubis
- Subtrochanteric line
Correct Answer: Greater trochanters
Explanation:
Pelvic binders should be centered directly over the greater trochanters to effectively close the pelvic ring, generate appropriate compressive vectors, and avoid excessive pressure on the abdomen or inadequate reduction seen with higher placements (e.g., over the iliac crests).
Question 45:
Diffuse idiopathic skeletal hyperostosis (DISH) is characterized by flowing ossification along the anterolateral aspect of the spine. According to Resnick's classical diagnostic criteria, how many contiguous vertebral bodies must be involved?
Options:
Correct Answer: 4
Explanation:
Resnick's criteria for DISH include: flowing ossification of at least 4 contiguous vertebral bodies (bridging 3 intervertebral disc spaces), preservation of disc height, and the absence of apophyseal joint ankylosis or sacroiliac erosion.
Question 46:
A 28-year-old male presents with a slowly enlarging, painful soft tissue mass in his plantar foot. Biopsy reveals a biphasic spindle cell neoplasm with epithelial components. Which of the following chromosomal translocations is most characteristic of this tumor?
Options:
- t(11;22)
- t(X;18)
- t(12;16)
- t(9;22)
- t(2;13)
Correct Answer: t(X;18)
Explanation:
The clinical picture and biphasic histology describe Synovial Sarcoma. This tumor is characterized by the t(X;18)(p11;q11) translocation, resulting in the SYT-SSX fusion gene. t(11;22) is seen in Ewing sarcoma, and t(12;16) is characteristic of myxoid liposarcoma.
Question 47:
Biomechanically, a complete radial tear of the posterior horn of the medial meniscus root alters knee kinematics most similarly to which of the following conditions?
Options:
- Total meniscectomy
- 50% partial meniscectomy
- ACL deficiency
- PCL deficiency
- Isolated MCL tear
Correct Answer: Total meniscectomy
Explanation:
Complete meniscal root tears or complete radial tears disrupt the circumferential hoop stresses of the meniscus. This results in functional meniscal extrusion under axial load, biomechanically mimicking a total meniscectomy and dramatically increasing peak tibiofemoral contact pressures.
Question 48:
A 55-year-old diabetic patient presents with a swollen, erythematous, and warm foot. Radiographs demonstrate periarticular osteopenia, osseous debris, and fragmentation of the midfoot. According to the Eichenholtz classification of Charcot arthropathy, what is the most appropriate initial treatment?
Options:
- Arthrodesis with rigid internal fixation
- Total contact casting and non-weight bearing
- Accommodative shoe wear and orthotics
- Exostectomy of the medial column
- Intravenous antibiotics for 6 weeks
Correct Answer: Total contact casting and non-weight bearing
Explanation:
The patient is in Eichenholtz Stage I (Developmental/Fragmentation), characterized by erythema, swelling, debris, and fragmentation. The standard of care is immediate immobilization and offloading using total contact casting (TCC) until the acute inflammatory phase resolves and coalescence (Stage II) begins.
Question 49:
A 35-year-old male presents with chronic wrist pain. Radiographs reveal a scaphoid nonunion with radioscaphoid arthritis. The capitolunate and radiolunate joints are radiographically preserved. What stage of Scaphoid Nonunion Advanced Collapse (SNAC) is this, and what is the most appropriate surgical treatment?
Options:
- Stage I: Radial styloidectomy and scaphoid fixation
- Stage II: Proximal row carpectomy or four-corner fusion
- Stage III: Total wrist arthrodesis
- Stage IV: Total wrist arthroplasty
- Stage II: Scaphoid fixation with vascularized bone graft
Correct Answer: Stage II: Proximal row carpectomy or four-corner fusion
Explanation:
This is SNAC Stage II. Stage I involves arthritis isolated to the radial styloid. Stage II involves the entire radioscaphoid joint. Stage III involves the capitolunate joint. The radiolunate joint is typically spared. Stage II is appropriately treated with proximal row carpectomy (PRC) or 4-corner fusion.
Question 50:
Bone morphogenetic proteins (BMPs) initiate intracellular signaling primarily by binding to transmembrane serine/threonine kinase receptors that directly phosphorylate and activate which of the following downstream mediators?
Options:
- Wnt/beta-catenin complex
- Smad proteins
- JAK/STAT pathway
- RANK/RANKL complex
- Notch receptors
Correct Answer: Smad proteins
Explanation:
BMPs bind to types I and II serine/threonine kinase receptors. Upon activation, they phosphorylate receptor-regulated Smads (R-Smads 1, 5, and 8), which then bind to the common-partner Smad (Co-Smad 4) to translocate to the nucleus and regulate the transcription of osteogenic target genes.
Question 51:
A 4-week-old infant with developmental dysplasia of the hip is treated with a Pavlik harness. During a follow-up visit, the parents report the infant is not kicking the treated leg. Examination shows decreased active knee extension but normal passive motion and hip flexion. What is the most likely cause of this clinical presentation?
Options:
- Avascular necrosis of the femoral head
- Femoral nerve palsy
- Obturator nerve palsy
- Sciatic nerve palsy
- Tibial nerve palsy
Correct Answer: Femoral nerve palsy
Explanation:
Femoral nerve palsy is a known complication of Pavlik harness treatment due to excessive hyperflexion of the hip, leading to nerve compression. It presents as decreased active knee extension (quadriceps weakness). Management requires temporary discontinuation or adjustment of the harness.
Question 52:
According to current guidelines for a Type III open tibia fracture heavily contaminated with soil from an agricultural farm injury, what is the most appropriate initial empiric systemic antibiotic coverage?
Options:
- First-generation cephalosporin alone
- First-generation cephalosporin and an aminoglycoside
- First-generation cephalosporin, an aminoglycoside, and high-dose penicillin
- Fluoroquinolone alone
- Carbapenem monotherapy
Correct Answer: First-generation cephalosporin, an aminoglycoside, and high-dose penicillin
Explanation:
For severe open fractures (Type III) with farm or heavily contaminated soil exposure, high-dose penicillin is added specifically for anaerobic coverage (e.g., Clostridium species) to prevent gas gangrene, along with a 1st-generation cephalosporin (Gram-positive coverage) and an aminoglycoside (Gram-negative coverage).
Question 53:
In a posterior-stabilized (PS) total knee arthroplasty, the cam-and-post mechanism is designed primarily to replicate the function of which native knee structure to facilitate femoral rollback during flexion?
Options:
- Anterior cruciate ligament
- Posterior cruciate ligament
- Medial collateral ligament
- Lateral collateral ligament
- Popliteus tendon
Correct Answer: Posterior cruciate ligament
Explanation:
The cam and post mechanism in a PS TKA engages during deep flexion to substitute for the resected Posterior Cruciate Ligament (PCL). This forces the femur to translate posteriorly on the tibia (femoral rollback), improving maximal flexion and preventing anterior subluxation of the femur.
Question 54:
In patients with cervical spondylotic myelopathy undergoing non-operative management, which of the following MRI findings is considered a poor prognostic indicator for neurological recovery?
Options:
- Duration of symptoms less than 6 months
- Cross-sectional area of the spinal cord < 40 mm2
- Presence of unilateral upper extremity radiculopathy
- Patient age under 50 years
- Maintenance of lordotic sagittal alignment
Correct Answer: Cross-sectional area of the spinal cord < 40 mm2
Explanation:
A spinal cord cross-sectional area of < 40 mm2 (transverse area), presence of myelomalacia (T2 hyperintensity/T1 hypointensity in the cord), duration of symptoms > 6 months, and severe clinical deficit (Nurick > 3) are established poor prognostic indicators for conservative management of cervical myelopathy.
Question 55:
A patient sustains a deep laceration over the volar aspect of the proximal phalanx of the index finger. Surgical exploration reveals complete transection of both the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP). What flexor tendon zone is this injury located in?
Options:
- Zone I
- Zone II
- Zone III
- Zone IV
- Zone V
Correct Answer: Zone II
Explanation:
Zone II (historically called 'no man's land') extends from the A1 pulley (distal palmar crease) to the insertion of the FDS on the middle phalanx. It contains both the FDS and FDP tendons within the narrow fibro-osseous sheath.
Question 56:
A 22-year-old collegiate baseball pitcher presents with deep shoulder pain, decreased velocity, and a positive O'Brien's test. MRI arthrogram reveals a Type II SLAP lesion. What anatomic feature specifically distinguishes a Type II SLAP tear from a Type I tear?
Options:
- Fraying of the superior labrum with an intact biceps anchor
- Detachment of the superior labrum and biceps anchor from the superior glenoid
- A bucket-handle tear of the labrum with an intact biceps anchor
- A bucket-handle tear of the labrum extending into the biceps tendon
- A labral tear extending into the middle glenohumeral ligament
Correct Answer: Detachment of the superior labrum and biceps anchor from the superior glenoid
Explanation:
Snyder classification of SLAP tears: Type I is fraying of the labrum with an intact anchor. Type II is detachment of the superior labrum and biceps anchor from the superior glenoid. Type III is a bucket-handle tear with an intact anchor. Type IV is a bucket-handle tear extending into the biceps tendon.
Question 57:
According to Perren's strain theory of bone healing, the type of tissue that forms in a fracture gap is dictated by the mechanical strain environment. What is the maximum tissue strain limit that allows for the formation of lamellar bone?
Options:
- < 2%
- 2% - 10%
- 10% - 30%
- 30% - 50%
- > 50%
Correct Answer: < 2%
Explanation:
Perren's strain theory states that lamellar bone can only form in low strain environments (< 2% strain). Woven bone tolerates up to 10% strain, fibrocartilage tolerates 10-30%, and granulation tissue can tolerate up to 100% strain before failing.
Question 58:
A 14-year-old boy is undergoing neo-adjuvant chemotherapy for an osteosarcoma of the distal femur. His regimen includes Doxorubicin, Cisplatin, and high-dose Methotrexate. Which of the following is a classic dose-limiting toxicity specifically associated with Doxorubicin?
Options:
- Hemorrhagic cystitis
- Ototoxicity
- Dilated cardiomyopathy
- Peripheral neuropathy
- Pulmonary fibrosis
Correct Answer: Dilated cardiomyopathy
Explanation:
Doxorubicin (Adriamycin) is heavily associated with cumulative, dose-dependent cardiotoxicity, specifically dilated cardiomyopathy. Cisplatin is classically associated with ototoxicity and nephrotoxicity. Ifosfamide is associated with hemorrhagic cystitis. Bleomycin is associated with pulmonary fibrosis.
Question 59:
A 30-year-old male with a comminuted tibial shaft fracture complains of escalating leg pain out of proportion to the injury. His blood pressure is 110/80 mmHg. Intracompartmental pressure testing is performed. Which of the following measured thresholds is the most reliable criterion for performing an emergency fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Absolute compartment pressure > 30 mmHg
- Delta P (Diastolic BP minus Compartment Pressure) < 30 mmHg
- Delta P (Mean Arterial Pressure minus Compartment Pressure) < 40 mmHg
- Delta P (Systolic BP minus Compartment Pressure) < 50 mmHg
Correct Answer: Delta P (Diastolic BP minus Compartment Pressure) < 30 mmHg
Explanation:
The Delta P concept (Diastolic Blood Pressure minus Compartment Pressure < 30 mmHg) is the most reliable and universally accepted threshold for diagnosing acute compartment syndrome. It accounts for the perfusion pressure of the limb, reducing unnecessary fasciotomies in hypotensive patients.
Question 60:
A 60-year-old female presents with medial ankle pain and a progressive flatfoot deformity. Examination reveals flexible hindfoot valgus and an inability to perform a single-leg heel rise. Radiographs demonstrate no arthritic changes in the subtalar or talonavicular joints. According to the Johnson and Strom classification, what stage of posterior tibial tendon dysfunction does this represent?
Options:
- Stage I
- Stage II
- Stage III
- Stage IV
- Stage V
Correct Answer: Stage II
Explanation:
Stage II posterior tibial tendon dysfunction (PTTD) is characterized by a flexible flatfoot deformity, an inability to perform a single-leg heel rise, and the absence of degenerative joint changes. Stage I has normal alignment and preserved heel rise. Stage III is a rigid deformity with hindfoot arthritis. Stage IV involves lateral ankle instability and deltoid ligament compromise.
Question 61:
An orthopaedic surgeon is treating a newborn with idiopathic clubfoot (congenital talipes equinovarus) using the Ponseti method. The first manipulation involves correcting the cavus deformity. Which of the following describes the correct anatomic manipulation to achieve this step?
Options:
- Pronating the forefoot to align with the hindfoot
- Supinating the forefoot and elevating the first ray to align with the hindfoot
- Plantarflexing the first ray while abducting the midfoot
- Simultaneous dorsiflexion of the midfoot and hindfoot
- Eversion of the calcaneus while supinating the forefoot
Correct Answer: Supinating the forefoot and elevating the first ray to align with the hindfoot
Explanation:
The first step of the Ponseti method is to correct the cavus deformity. This is achieved by supinating the forefoot (elevating the first ray) so that the forefoot is aligned with the varus hindfoot. Once the cavus is corrected and the foot is supinated, the entire foot is gradually abducted around the lateral aspect of the head of the talus to correct the adductus and varus deformities. The equinus is corrected last, typically requiring a percutaneous Achilles tenotomy.
Question 62:
When utilizing a posteromedial approach to the proximal tibia for the fixation of a complex tibial plateau fracture, the surgical interval is developed between which of the following structures?
Options:
- Medial head of the gastrocnemius and the soleus
- Semimembranosus and the medial collateral ligament
- Medial head of the gastrocnemius and the pes anserinus
- Tibialis posterior and the flexor digitorum longus
- Tibialis anterior and the medial tibial crest
Correct Answer: Medial head of the gastrocnemius and the pes anserinus
Explanation:
The posteromedial approach to the proximal tibia involves an internervous interval (though practically an intermuscular interval) between the medial head of the gastrocnemius (innervated by the tibial nerve) posteriorly and the pes anserinus (sartorius, gracilis, semitendinosus) anteriorly. Retracting the pes anteriorly and the medial gastrocnemius posteriorly protects the neurovascular bundle and provides excellent exposure to posteromedial tibial plateau fragments.
Question 63:
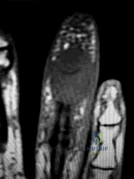
A 62-year-old female presents with a painful mass over the dorsal aspect of her right index finger distal interphalangeal (DIP) joint, accompanied by a longitudinal groove in her nail plate. She undergoes surgical excision of the lesion. To minimize the highest risk of recurrence, which of the following must be performed during the procedure?
Options:
- Wide excision of the overlying skin with a rotation flap
- Marginal excision of the associated distal phalanx osteophyte
- Arthrodesis of the DIP joint
- Complete resection of the extensor tendon insertion
- Cauterization of the nail matrix
Correct Answer: Marginal excision of the associated distal phalanx osteophyte
Explanation:
The clinical scenario and image refer to a mucous cyst of the DIP joint, which is a ganglion cyst associated with underlying osteoarthritis (Heberden's nodes). The highest rate of recurrence of a mucous cyst occurs if the surgeon fails to identify and debride the underlying marginal osteophyte from the DIP joint. Excision of the cyst stalk and meticulous osteophyte debridement reduces the recurrence rate to less than 5%.
Question 64:
A collegiate football player sustains a valgus injury to the knee, resulting in a complete tear of the medial collateral ligament (MCL). During surgical reconstruction, accurate identification of the superficial MCL footprints is critical. The distal insertion of the superficial MCL is correctly located:
Options:
- Immediately deep to the medial meniscus
- Approximately 1.5 cm distal to the joint line on the anteromedial tibia
- Approximately 4 to 5 cm distal to the joint line, deep to the pes anserinus
- Directly on the adductor tubercle of the distal femur
- On the medial aspect of the patellar tendon insertion
Correct Answer: Approximately 4 to 5 cm distal to the joint line, deep to the pes anserinus
Explanation:
The superficial medial collateral ligament (sMCL) has its proximal footprint on the posterior aspect of the medial femoral epicondyle. Its distal footprint is located on the medial aspect of the proximal tibia, approximately 4.5 cm (range 4 to 5 cm) distal to the joint line, and lies deep to the pes anserinus. It is the primary restraint to valgus stress at 30 degrees of knee flexion.
Question 65:
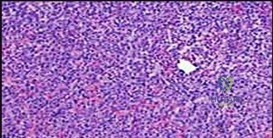
A 15-year-old male presents with chronic knee pain. Radiographs reveal an eccentric, lytic lesion confined to the epiphysis of the proximal tibia. A biopsy is performed. Histological evaluation demonstrates mononuclear cells with grooved nuclei ('coffee bean' appearance) and areas of pericellular 'chicken-wire' calcification. What is the most likely diagnosis?
Options:
- Giant Cell Tumor
- Clear Cell Chondrosarcoma
- Chondroblastoma
- Aneurysmal Bone Cyst
- Osteoblastoma
Correct Answer: Chondroblastoma
Explanation:
The diagnosis is Chondroblastoma, a benign but locally aggressive cartilaginous bone tumor that characteristically arises in the epiphysis or apophysis of long bones in skeletally immature or young adult patients. Histological hallmarks include mononuclear chondroblasts with grooved or clefted nuclei ('coffee bean' nuclei), multinucleated osteoclast-like giant cells, and fine lattice-like 'chicken-wire' pericellular calcifications.
Question 66:
An 82-year-old male with a history of severe osteoporosis presents after a ground-level fall. Imaging reveals a displaced Type II odontoid fracture. He has significant neck pain but is neurologically intact. To optimize union rates and minimize morbidity and mortality, which of the following is the most appropriate surgical management?
Options:
- Anterior odontoid screw fixation
- Application of a halo vest
- Cervical collar application and strict bed rest
- Posterior C1-C2 instrumented fusion
- Occipitocervical fusion
Correct Answer: Posterior C1-C2 instrumented fusion
Explanation:
In an elderly patient (e.g., >80 years old) with a displaced Type II odontoid fracture, posterior C1-C2 instrumented fusion provides the highest rate of fracture union and has lower morbidity compared to alternative surgical methods like an anterior odontoid screw (which relies on good bone quality, often poor in this demographic, and poses a higher risk of hardware failure or dysphagia). Halo vest immobilization in the elderly is associated with high nonunion rates and severe morbidity/mortality (pin site infection, pneumonia, cardiac arrest) and is generally avoided.
Question 67:
A 65-year-old male presents with new-onset groin pain and a palpable mass 6 years following a primary Metal-on-Polyethylene (MoP) total hip arthroplasty (THA). A MARS MRI demonstrates a solid and cystic soft-tissue mass. Laboratory testing reveals elevated serum Cobalt levels (>10 ppb) with relatively normal Chromium levels. Infection is ruled out. What is the most likely underlying mechanism for his presentation?
Options:
- Adverse local tissue reaction due to bearing surface wear
- Mechanically assisted crevice corrosion at the head-neck taper
- Polyethylene-induced osteolysis
- Aseptic loosening of the femoral stem
- Ceramic liner fracture
Correct Answer: Mechanically assisted crevice corrosion at the head-neck taper
Explanation:
The clinical scenario describes trunnionosis, or mechanically assisted crevice corrosion (MACC), occurring at the modular head-neck junction (trunnion) of the femoral stem. In a Metal-on-Polyethylene (MoP) THA, elevated cobalt levels in the presence of normal chromium levels strongly suggest corrosion at a modular junction (typically a CoCr head on a titanium stem), not bearing surface wear. This process can lead to an adverse local tissue reaction (ALTR/ALVAL) and pseudotumor formation.
Question 68:
A 24-year-old female sustains a purely ligamentous Lisfranc injury following a fall from a horse. The first and second metatarsals are significantly widened on weight-bearing radiographs. What surgical intervention has been shown in prospective randomized trials to provide superior functional outcomes and lower reoperation rates for this specific injury pattern compared to ORIF?
Options:
- Closed reduction and percutaneous K-wire fixation
- Open reduction and internal fixation with cortical screws
- Primary arthrodesis of the involved tarsometatarsal joints
- Dorsal bridge plating without joint preparation
- Suture-button suspension arthroplasty
Correct Answer: Primary arthrodesis of the involved tarsometatarsal joints
Explanation:
For purely ligamentous Lisfranc injuries, multiple randomized controlled trials (such as by Ly and Coetzee) have demonstrated that primary arthrodesis of the first, second, and third tarsometatarsal joints yields superior short- and mid-term functional outcomes and significantly lower rates of planned and unplanned reoperations (such as hardware removal or salvage fusion) when compared to open reduction and internal fixation (ORIF). Bony fracture-dislocations of the Lisfranc joint may still be treated well with ORIF.
Question 69:
According to Perren's strain theory of bone healing, the interfragmentary strain threshold determines the type of tissue that forms within a fracture gap. Primary (direct) bone healing without callus formation occurs when the interfragmentary strain is maintained below what percentage?
Options:
Correct Answer: 2%
Explanation:
Perren's strain theory dictates that tissues cannot form if the local strain exceeds their tolerance. Granulation tissue tolerates up to 100% strain, fibrous connective tissue up to 17%, and fibrocartilage between 2% and 10%. Lamellar bone can only form directly (primary bone healing via cutting cones) when the interfragmentary strain is strictly below 2%, which is typically achieved with rigid absolute stability (e.g., compression plating).
Question 70:
A 3-year-old female presents with progressive genu varum. Radiographs reveal beaking and fragmentation of the medial proximal tibial metaphysis consistent with infantile Blount's disease. Pathoanatomically, this disease is primarily caused by disordered endochondral ossification of which specific portion of the proximal tibial physis?
Options:
- Posteromedial aspect
- Anteromedial aspect
- Posterolateral aspect
- Anterolateral aspect
- Central physeal aspect
Correct Answer: Posteromedial aspect
Explanation:
Blount's disease (tibia vara) is characterized by disordered endochondral ossification and growth suppression primarily at the posteromedial aspect of the proximal tibial physis. This asymmetric growth restriction leads to the classic clinical deformity of multiplanar varus, internal tibial torsion, and procurvatum.
Question 71:
A 35-year-old manual laborer presents with progressive wrist pain. Radiographs reveal sclerosis and collapse of the lunate without a fixed scaphoid ring sign or carpal instability (Lichtman Stage IIIA Kienböck's disease). Measurement of the radioulnar relationship demonstrates 3 mm of ulnar negative variance. Which of the following is the most appropriate surgical treatment?
Options:
- Proximal row carpectomy
- Radial shortening osteotomy
- Total wrist arthrodesis
- Lunate excision and silastic replacement
- Scaphoid-trapezium-trapezoid (STT) fusion
Correct Answer: Radial shortening osteotomy
Explanation:
In Lichtman Stage IIIA Kienböck's disease, there is lunate collapse but carpal height and alignment (scaphoid) are maintained. For a patient with Stage IIIA disease and ulnar negative variance, a joint-leveling procedure such as a radial shortening osteotomy is the most appropriate and biomechanically sound intervention, as it decreases load transmission through the radiolunate fossa. Proximal row carpectomy or STT fusion are typically reserved for more advanced stages (IIIB or IV).
Question 72:
An 85-year-old female with severe rheumatoid arthritis and osteoporosis sustains a highly comminuted, intra-articular distal humerus fracture (AO/OTA 13-C3) after a mechanical fall. She lives independently and uses a walker. Which surgical intervention provides the most predictable pain relief and allows for immediate postoperative weight-bearing through the upper extremity for mobility?
Options:
- Open reduction and internal fixation with dual orthogonal locking plates
- Hinged external fixation
- Total elbow arthroplasty
- Olecranon osteotomy and tension band wiring
- Distal humerus hemiarthroplasty
Correct Answer: Total elbow arthroplasty
Explanation:
In an elderly, osteoporotic patient (especially with a history of inflammatory arthritis like RA) who sustains a highly comminuted intra-articular distal humerus fracture, Total Elbow Arthroplasty (TEA) provides superior outcomes compared to ORIF. It offers more predictable pain relief, earlier return of function, and allows the patient to bear weight immediately (within standard TEA limits, though essential for immediate walker use) without the high risk of hardware failure or nonunion associated with osteoporotic bone.
Question 73:
A 62-year-old male with multiple myeloma presents with thigh pain. Radiographs demonstrate an osseous lesion. When calculating the Mirels' score to determine the indication for prophylactic internal fixation, which of the following clinical or radiographic findings assigns the maximum of 3 points for its respective category?
Options:
- A purely blastic lesion
- A lesion involving the upper extremity
- Pain described as mild with weight-bearing
- A lesion diameter occupying greater than 2/3 of the bone cortex
- A lesion located in the diaphyseal shaft
Correct Answer: A lesion diameter occupying greater than 2/3 of the bone cortex
Explanation:
The Mirels' classification evaluates four parameters to predict impending pathologic fracture: Site (Upper extremity=1, Lower extremity=2, Peritrochanteric=3), Pain (Mild=1, Moderate=2, Functional/Severe=3), Lesion character (Blastic=1, Mixed=2, Lytic=3), and Lesion size (<1/3 cortex=1, 1/3 to 2/3 cortex=2, >2/3 cortex=3). A score of 9 or greater indicates impending fracture requiring prophylactic fixation. Therefore, a lesion >2/3 of the cortex scores 3 points.
Question 74:
A 70-year-old male presents with bilateral leg pain and fatigue when walking short distances. Which of the following features most strongly suggests a diagnosis of neurogenic claudication secondary to lumbar spinal stenosis rather than vascular claudication?
Options:
- Pain is rapidly relieved simply by standing completely still
- Symptoms are exacerbated by pushing a shopping cart
- Symptoms are reliably reproduced after walking a precise distance each time
- Pain is improved when walking uphill and exacerbated walking downhill
- The presence of diminished pedal pulses and distal hair loss
Correct Answer: Pain is improved when walking uphill and exacerbated walking downhill
Explanation:
Neurogenic claudication is hallmarked by exacerbation of symptoms with lumbar extension and relief with lumbar flexion. Walking uphill flexes the lumbar spine, enlarging the spinal canal and foramina, thereby relieving symptoms. Walking downhill forces the spine into extension, exacerbating symptoms. In contrast, vascular claudication is distance-dependent, relieved merely by resting (standing still), and presents with signs of poor perfusion (diminished pulses).
Question 75:
A 19-year-old collegiate swimmer presents with bilateral shoulder pain and a sensation of instability in multiple directions. Physical examination reveals a positive sulcus sign and generalized ligamentous laxity. If surgical intervention is ultimately indicated after exhaustive physical therapy, the procedure must address the primary patholaxity, which is characterized by:
Options:
- An avulsion of the anterior labrum from the glenoid rim
- An increased volume and redundancy of the inferior capsular pouch
- A complete tear of the superior glenohumeral ligament
- An engaging Hill-Sachs lesion
- A congenital hypoplasia of the glenoid
Correct Answer: An increased volume and redundancy of the inferior capsular pouch
Explanation:
The patient has multidirectional instability (MDI) of the shoulder, characterized by symptomatic instability in more than one direction (anterior, posterior, inferior). The hallmark pathoanatomy of MDI is a patulous (redundant/increased volume) inferior capsule. If a prolonged course of physical therapy (focusing on rotator cuff and periscapular stabilization) fails, the surgical treatment of choice is an inferior capsular shift to reduce capsular volume.
Question 76:
During a cruciate-retaining (CR) total knee arthroplasty (TKA), the surgeon evaluates the kinematics of the implant after trial components are placed. If the posterior cruciate ligament (PCL) is excessively tight, which of the following kinematic abnormalities is most likely to be observed?
Options:
- Excessive femoral rollback causing tightness in deep flexion and anterior tibial lift-off
- Anterior translation of the femur on the tibia during deep flexion
- A symmetric extension gap but a highly asymmetric flexion gap
- Hyperextension of the knee joint with posterior sag
- Patellar clunk syndrome during terminal extension
Correct Answer: Excessive femoral rollback causing tightness in deep flexion and anterior tibial lift-off
Explanation:
In a CR TKA, an intact and appropriately balanced PCL acts to induce femoral rollback during knee flexion. If the PCL is excessively tight, it will pull the femur posteriorly too early and forcefully during flexion, leading to excessive femoral rollback. This effectively decreases the flexion gap (making it tight in deep flexion) and can cause the anterior aspect of the tibial tray to lift off. It does not cause anterior femoral translation (which would happen if the PCL were deficient).
Question 77:
A 55-year-old male with long-standing, poorly controlled diabetes presents with a swollen, erythematous, and warm left foot without open wounds or signs of systemic sepsis. Radiographs demonstrate significant soft tissue edema, osteopenia, and early periarticular fragmentation at the midfoot. According to the Eichenholtz classification, what is the most appropriate initial treatment for this stage of his condition?
Options:
- Total contact casting and strict non-weight-bearing
- Immediate midfoot arthrodesis with robust internal fixation
- Intravenous antibiotics and surgical debridement
- Prescription of custom accommodative orthotic footwear
- Excision of the fragmented bone (exostectomy)
Correct Answer: Total contact casting and strict non-weight-bearing
Explanation:
The patient is presenting with acute Eichenholtz Stage I (developmental/fragmentation stage) Charcot arthropathy, characterized by a red, hot, swollen foot, osteopenia, subluxation, and bony fragmentation. The standard of care for acute Stage I Charcot is immediate offloading and immobilization using a total contact cast (TCC). Surgery is generally contraindicated in the acute inflammatory phase due to poor bone stock and high failure rates.
Question 78:
The microanatomy of adult articular cartilage is divided into specific structural zones. Which of the following statements accurately characterizes the superficial (tangential) zone of articular cartilage?
Options:
- It contains the highest concentration of water and collagen fibers oriented parallel to the joint surface.
- It contains the highest concentration of proteoglycans and chondrocytes that are organized into vertical columns.
- It is separated from the deeper cartilage by the tidemark and contains no viable chondrocytes.
- It primarily consists of Type X collagen and resists compressive forces more than shear forces.
- It is the thickest zone and its collagen fibers are oriented perpendicularly to the subchondral bone.
Correct Answer: It contains the highest concentration of water and collagen fibers oriented parallel to the joint surface.
Explanation:
The superficial (tangential) zone makes up 10-20% of articular cartilage thickness. It has the highest water content (up to 80%), the lowest proteoglycan content, and features flat chondrocytes with Type II collagen fibers oriented parallel to the joint surface to resist shear stress. The deep zone has the highest proteoglycan content, lowest water content, and collagen fibers arranged vertically to resist compression.
Question 79:
A 35-year-old male is brought to the trauma bay following a high-speed motorcycle collision. He is hemodynamically unstable with a blood pressure of 75/40 mmHg. An anteroposterior pelvic radiograph reveals an APC-III pelvic ring injury (diastasis of the pubic symphysis > 2.5 cm and disruption of the sacroiliac joints). A circumferential pelvic sheet or binder is indicated. To be maximally effective in reducing the pelvic volume and stabilizing the venous plexus, the binder must be centered over which anatomical landmark?
Options:
- The anterior superior iliac spines
- The greater trochanters
- The iliac crests
- The umbilicus
- The proximal femur shafts
Correct Answer: The greater trochanters
Explanation:
To effectively reduce pelvic volume in open-book (APC) pelvic ring injuries, a pelvic binder or sheet must be centered squarely over the greater trochanters of the femurs. Placement over the iliac crests is a common error that can actually force the pelvis into further outward rotation or fail to adequately close the posterior pelvic ring, exacerbating hemorrhage.
Question 80:
In the surgical repair of flexor tendon lacerations within Zone II of the hand, maintaining initial tensile strength is critical to permit early active motion protocols. The initial tensile strength of a flexor tendon repair is most directly proportional to which of the following factors?
Options:
- The caliber of the epitendinous suture
- The number of core suture strands crossing the repair site
- The location of the knot (internal vs. external)
- The preservation of the A3 and A5 pulleys
- The strict adherence to a passive-only rehabilitation protocol
Correct Answer: The number of core suture strands crossing the repair site
Explanation:
The initial strength of a flexor tendon repair is directly proportional to the number of core suture strands crossing the repair site. A 4-strand or 6-strand repair provides significantly more tensile strength than a classic 2-strand repair (e.g., modified Kessler), which is necessary to safely support early active motion protocols. While epitendinous sutures reduce gapping and add some strength, the core strands are the primary structural determinant.
Question 81:
A surgeon performs a primary posterior-stabilized total knee arthroplasty (TKA). During trialing, the knee is perfectly balanced in full extension, but the trial components are overly tight in flexion, limiting motion to 85 degrees. The joint line is appropriately restored. What is the most appropriate next step to correct this specific imbalance?
Options:
- Resect more distal femur
- Decrease the anterior-posterior size of the femoral component
- Release the posterior capsule
- Recut the proximal tibia to increase resection thickness
- Increase the anterior-posterior size of the femoral component
Correct Answer: Decrease the anterior-posterior size of the femoral component
Explanation:
A knee that is balanced in extension but tight in flexion indicates an isolated flexion gap issue. The most appropriate way to increase the flexion gap without affecting the extension gap is to decrease the anterior-posterior size of the femoral component, which decreases the posterior condylar offset. Resecting more distal femur or recutting the proximal tibia would inappropriately widen the extension gap.
Question 82:
An 11-year-old boy presents with a painful, swollen thigh. Imaging reveals a permeative diaphyseal lesion with an 'onion-skin' periosteal reaction. A biopsy confirms Ewing sarcoma. Which of the following cytogenetic abnormalities is most characteristically associated with this tumor?
Options:
- t(11;22)(q24;q12)
- t(9;22)(q34;q11)
- t(X;18)(p11;q11)
- t(2;13)(q35;q14)
- t(12;16)(q13;p11)
Correct Answer: t(11;22)(q24;q12)
Explanation:
Ewing sarcoma is classically associated with the t(11;22)(q24;q12) chromosomal translocation, resulting in the EWS-FLI1 fusion protein in about 85% of cases. t(9;22) is seen in chronic myelogenous leukemia (Philadelphia chromosome). t(X;18) is associated with synovial sarcoma. t(2;13) is seen in alveolar rhabdomyosarcoma. t(12;16) is associated with myxoid liposarcoma.
Question 83:
A 45-year-old woman complains of pain, tingling, and numbness over the dorsal radial aspect of her hand, which is exacerbated by wearing tight jewelry. She has a strongly positive Tinel's sign over the radial aspect of her mid-to-distal forearm. What nerve is most likely compressed, and between which two muscles does it typically emerge from the deep fascia?
Options:
- Superficial radial nerve, between brachioradialis and extensor carpi radialis longus
- Posterior interosseous nerve, between supinator and extensor digitorum communis
- Superficial radial nerve, between flexor carpi radialis and brachioradialis
- Posterior interosseous nerve, between brachioradialis and extensor carpi radialis brevis
- Lateral antebrachial cutaneous nerve, between biceps and brachialis
Correct Answer: Superficial radial nerve, between brachioradialis and extensor carpi radialis longus
Explanation:
Wartenberg's syndrome is a compressive neuropathy of the superficial sensory branch of the radial nerve. The nerve typically emerges from the deep fascia in the distal third of the forearm between the brachioradialis and the extensor carpi radialis longus (ECRL) tendons. Tight items around the wrist, such as watches or bracelets, often exacerbate the symptoms.
Question 84:
A 12-year-old boy presents with left thigh pain and an antalgic gait. Radiographs confirm a mild left slipped capital femoral epiphysis (SCFE). He is subsequently evaluated for potential contralateral disease. Which of the following is considered the strongest absolute indication for prophylactic in-situ pinning of the contralateral right hip?
Options:
- Open triradiate cartilage
- Underlying endocrine disorder
- Body mass index > 95th percentile
- Initial slip angle > 50 degrees
- Male gender
Correct Answer: Underlying endocrine disorder
Explanation:
Prophylactic pinning of the contralateral hip in patients with SCFE is highly recommended and considered essentially an absolute indication for patients with endocrine or metabolic disorders (e.g., hypothyroidism, renal osteodystrophy, panhypopituitarism) due to the exceedingly high risk of bilateral involvement, approaching 100% in these conditions. Young age (<10 years) and open triradiate cartilage are relative indications.
Question 85:
A 24-year-old collegiate football lineman sustains a severe hyperplantarflexion injury to his midfoot. He complains of inability to bear weight. Physical examination notes significant midfoot swelling and plantar ecchymosis. Weight-bearing radiographs show 3 mm of widening between the base of the first and second metatarsals. The injured ligament pathognomonic for this condition connects which of the following osseous structures?
Options:
- Base of the 1st metatarsal to the base of the 2nd metatarsal
- Medial cuneiform to the base of the 2nd metatarsal
- Medial cuneiform to the intermediate cuneiform
- Intermediate cuneiform to the base of the 2nd metatarsal
- Lateral cuneiform to the cuboid
Correct Answer: Medial cuneiform to the base of the 2nd metatarsal
Explanation:
The Lisfranc ligament is a stout, strong interosseous ligament that connects the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. There is no direct transverse ligamentous connection between the bases of the first and second metatarsals, making this region reliant on the Lisfranc ligament for stability.
Question 86:
A 65-year-old female presents with progressive neurogenic claudication and lower back pain. Imaging shows an L4-L5 grade I degenerative spondylolisthesis with severe central canal stenosis. After failing 6 months of comprehensive conservative treatment, she considers operative intervention. According to the Spine Patient Outcomes Research Trial (SPORT), which of the following statements regarding surgical versus nonoperative treatment at 4-year follow-up is correct?
Options:
- Nonoperative treatment yields superior results in pain reduction compared to surgery.
- Surgical treatment provides significantly greater improvement in pain and function compared to nonoperative treatment.
- Both groups demonstrate equal long-term improvement in functional outcomes.
- Surgical treatment is associated with a significantly higher rate of long-term mortality.
- Epidural steroid injections provide equivalent long-term relief to surgical decompression.
Correct Answer: Surgical treatment provides significantly greater improvement in pain and function compared to nonoperative treatment.
Explanation:
The Spine Patient Outcomes Research Trial (SPORT) demonstrated that for patients with degenerative spondylolisthesis and symptomatic spinal stenosis, surgical treatment (decompression with or without fusion) maintained significantly greater improvement in pain and function compared to nonoperative treatment at 4-year follow-up. This benefit persisted in long-term 8-year follow-up data.
Question 87:
Articular cartilage is a highly specialized tissue organized into four distinct zones to handle complex mechanical loads. Which zone typically contains the highest concentration of proteoglycans, the lowest concentration of water, and collagen fibrils arranged perpendicularly to the articular surface?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified cartilage zone
- Subchondral bone plate
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage is characterized by the highest concentration of proteoglycans, the lowest concentration of water, and thick collagen fibrils oriented perpendicularly to the subchondral bone, which provides the highest resistance to compressive forces. The superficial zone has the highest water content and collagen arranged parallel to the surface for shear resistance.
Question 88:
A 26-year-old recreational skier sustains a twisting knee injury. On physical examination, the physician notes a positive dial test (increased external rotation of the tibia relative to the femur) at 30 degrees of knee flexion, but the test normalizes and is symmetric to the contralateral uninjured side at 90 degrees of flexion. Which of the following structures is most likely injured?
Options:
- Anterior cruciate ligament (ACL)
- Posterior cruciate ligament (PCL)
- Posterolateral corner (PLC)
- Both the PCL and the PLC
- Medial collateral ligament (MCL)
Correct Answer: Posterolateral corner (PLC)
Explanation:
A positive dial test (increased external rotation of the tibia >10 degrees compared to the normal side) at 30 degrees of flexion that normalizes at 90 degrees of flexion indicates an isolated injury to the posterolateral corner (PLC). If the dial test is positive at both 30 degrees and 90 degrees of flexion, it indicates a combined injury involving both the PLC and the PCL.
Question 89:
A 14-year-old boy presents with acute ankle pain after an external rotation injury while playing soccer. Radiographs reveal a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. What is the primary deforming force (ligamentous attachment) responsible for producing this specific fracture pattern?
Options:
- Anterior talofibular ligament (ATFL)
- Calcaneofibular ligament (CFL)
- Anterior inferior tibiofibular ligament (AITFL)
- Posterior inferior tibiofibular ligament (PITFL)
- Deltoid ligament
Correct Answer: Anterior inferior tibiofibular ligament (AITFL)
Explanation:
A juvenile Tillaux fracture is a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. It occurs due to avulsion by the strong anterior inferior tibiofibular ligament (AITFL) during an external rotation injury. This pattern occurs in adolescents because the distal tibial physis closes asynchronously: central, then medial, and finally anterolateral, leaving the anterolateral portion vulnerable to avulsion.
Question 90:
Following a traumatic laceration and subsequent zone II flexor tendon repair in the index finger, preservation or reconstruction of the pulley system is mandatory for optimal biomechanics. Which of the following sets of annular pulleys are considered the most mechanically critical to prevent bowstringing and flexion contractures?
Options:
- A1 and A3
- A2 and A4
- A3 and A5
- A1, A3, and A5
- C1, C2, and C3
Correct Answer: A2 and A4
Explanation:
The A2 and A4 pulleys are the most mechanically critical annular pulleys in the flexor tendon sheath. They arise directly from the periosteum of the proximal and middle phalanges, respectively. Loss of these two pulleys leads to significant bowstringing of the flexor tendons, decreased excursion efficiency, reduced grip strength, and progressive flexion contractures.
Question 91:
A massive structural cortical allograft is utilized to reconstruct a large segmental bone defect following tumor resection. The biological process by which the living host bone gradually resorbs the necrotic allograft bone via osteoclastic activity, immediately followed by new osteoblastic bone formation on the remaining allograft scaffold, is termed:
Options:
- Osteoinduction
- Osteogenesis
- Creeping substitution
- Endochondral ossification
- Intramembranous ossification
Correct Answer: Creeping substitution
Explanation:
Creeping substitution is the classical process by which a non-vascularized cortical bone graft is incorporated. It involves the simultaneous resorption of the graft by host osteoclasts and the laying down of new host bone by osteoblasts along the haversian canals. Osteoinduction refers to the stimulation of phenotypic conversion of progenitor cells into osteoblasts. Osteoconduction provides a physical scaffold.
Question 92:
A 72-year-old female is undergoing a primary total hip arthroplasty via a posterior approach. During trial reduction, the hip is found to be highly unstable, dislocating posteriorly when the leg is placed in flexion, adduction, and internal rotation. The surgeon determines the acetabular and femoral components are oriented in perfect native version and inclination, but there is significant soft tissue laxity. The femoral head trial is currently a standard neck (+0). Which of the following component adjustments would most appropriately address this instability?
Options:
- Increase the femoral head length (e.g., to +4 or +8)
- Decrease the femoral head length (e.g., to -4)
- Decrease acetabular anteversion
- Decrease femoral anteversion
- Use an elevated rim liner positioned posteroinferiorly
Correct Answer: Increase the femoral head length (e.g., to +4 or +8)
Explanation:
In the setting of a posterior approach THA with posterior instability due to soft-tissue laxity (and correctly positioned components), increasing the femoral offset and leg length by using a longer offset head (e.g., +4 or +8) increases myofascial tissue tension, particularly of the abductors and external rotators, thereby stabilizing the hip joint. Decreasing anteversion or head length would worsen posterior instability.
Question 93:
A 55-year-old male with long-standing, poorly controlled type II diabetes presents with a diffusely swollen, erythematous, and warm right foot that is insensate to monofilament testing. Radiographs demonstrate florid fragmentation of the tarsal bones, joint subluxations, and significant periarticular osseous debris. According to the Eichenholtz classification of Charcot arthropathy, what stage does this represent?
Options:
- Stage 0 (Inflammatory)
- Stage I (Developmental/Fragmentation)
- Stage II (Coalescence)
- Stage III (Reconstruction/Consolidation)
- Stage IV (Chronic)
Correct Answer: Stage I (Developmental/Fragmentation)
Explanation:
The Eichenholtz classification details the natural history of Charcot neuroarthropathy. Stage I (Developmental/Fragmentation) is clinically characterized by a red, hot, swollen foot. Radiographs classically show joint space narrowing, fragmentation, subluxation/dislocation, and bony debris. Stage 0 is the clinical pre-fragmentation phase (normal x-rays). Stage II involves absorption of debris and early fusion. Stage III involves remodeling and a stable, albeit deformed, joint.
Question 94:
A 6-year-old boy is diagnosed with Legg-Calvé-Perthes disease. The treating orthopedist relies on the Herring Lateral Pillar classification to determine the child's prognosis and guide treatment. Which of the following accurately describes a Herring Lateral Pillar Group B hip?
Options:
- No involvement of the lateral pillar, maintaining 100% height
- > 50% maintenance of normal lateral pillar height
- < 50% maintenance of normal lateral pillar height
- Complete 100% collapse of the lateral pillar
- Central pillar collapse with perfectly intact lateral and medial pillars
Correct Answer: > 50% maintenance of normal lateral pillar height
Explanation:
The Herring Lateral Pillar Classification evaluates the height of the lateral aspect of the capital femoral epiphysis. Group A: No involvement of the lateral pillar. Group B: >50% of the lateral pillar height is maintained. Group C: <50% of the lateral pillar height is maintained. A Group B/C classification was later added for borderline cases where the pillar is approximately 50% of normal height or poorly ossified. Prognosis significantly worsens from A to C.
Question 95:
A 30-year-old jackhammer operator presents with worsening dorsal wrist pain and weakened grip strength. Advanced imaging and radiographs reveal sclerosis and early fragmentation of the lunate bone. However, measurements confirm the overall carpal height is maintained, and there is no fixed palmar rotation of the scaphoid. What Lichtman stage of Kienböck's disease does this represent?
Options:
- Stage I
- Stage II
- Stage IIIA
- Stage IIIB
- Stage IV
Correct Answer: Stage IIIA
Explanation:
Lichtman Classification of Kienböck's disease: Stage I shows a normal radiograph but abnormal MRI. Stage II shows lunate sclerosis without collapse. Stage IIIA shows lunate collapse and fragmentation, but normal carpal height and normal scaphoid alignment. Stage IIIB shows lunate collapse with decreased carpal height and fixed palmar rotation of the scaphoid. Stage IV involves generalized secondary radiocarpal or midcarpal osteoarthritis.
Question 96:
A 55-year-old male with a history of intravenous drug use presents with severe, progressive midthoracic back pain, a temperature of 39.0°C, and rapidly progressive bilateral lower extremity weakness over the past 24 hours. MRI with gadolinium reveals a large anterior epidural abscess causing severe spinal cord compression at T8. What is the most appropriate and definitive next step in management?
Options:
- Immediate administration of intravenous antibiotics and close neurological observation
- CT-guided needle aspiration for culture prior to definitive antibiotic therapy
- Anterior corpectomy, abscess evacuation, spinal cord decompression, and stabilization
- Posterior laminectomy alone for decompression
- Epidural steroid injection followed by bracing
Correct Answer: Anterior corpectomy, abscess evacuation, spinal cord decompression, and stabilization
Explanation:
An anterior spinal epidural abscess causing acute, progressive neurological deficit requires urgent surgical decompression. In the thoracic spine, where the pathology is anterior to the spinal cord, an anterior approach (such as an anterior corpectomy and fusion) is preferred. A posterior laminectomy alone is relatively contraindicated as it fails to address the anterior pathology adequately, can further destabilize the spine, and risks causing or worsening kyphosis, which can stretch and damage the already compromised spinal cord.
Question 97:
A 35-year-old female presents with persistent knee pain. Radiographs demonstrate an eccentric, purely lytic lesion in the distal femur that extends directly to the subchondral bone without a distinct sclerotic margin. Core needle biopsy confirms a Giant Cell Tumor of bone. The formation of the multinucleated giant cells characteristic of this tumor is mediated by a specific signaling pathway. Which of the following systemic medications specifically targets and inhibits this pathway?
Options:
- Imatinib
- Denosumab
- Bisphosphonates
- Doxorubicin
- Methotrexate
Correct Answer: Denosumab
Explanation:
Giant cell tumors of bone consist of neoplastic mononuclear stromal cells that express RANKL. RANKL recruits osteoclast precursors and stimulates their differentiation into multinucleated, bone-resorbing giant cells via the RANK receptor. Denosumab is a human monoclonal antibody that specifically binds and inhibits RANKL, effectively halting osteoclastogenesis, reducing tumor size, and allowing for intralesional ossification. It is often used as a neoadjuvant or primary treatment for unresectable cases.
Question 98:
A 40-year-old roofer falls 15 feet from a ladder, landing directly on his heels. He sustains a closed, displaced intra-articular fracture of the calcaneus. When evaluating his lateral radiograph, which of the following geometric changes is most classically associated with the typical deformity pattern of this injury?
Options:
- Increased Böhler's angle
- Decreased angle of Gissane
- Decreased Böhler's angle
- Increased calcaneal pitch
- Plantarflexion of the talar head
Correct Answer: Decreased Böhler's angle
Explanation:
On a normal lateral radiograph of the foot, Böhler's angle is typically between 20° and 40°. In a displaced intra-articular calcaneus fracture, the posterior facet is commonly driven downward (depressed) into the cancellous body of the calcaneus, resulting in a flattening of the calcaneus and a severely decreased or even negative Böhler's angle. The angle of Gissane (normally 100° to 130°) is typically increased, not decreased, due to strut collapse.
Question 99:
A 28-year-old competitive weightlifter feels a sudden, sharp 'tearing' sensation in his anterior axilla while performing heavy bench presses. This is followed by immediate weakness, swelling, and extensive ecchymosis. Physical examination reveals a loss of the normal anterior axillary fold contour and pronounced weakness in internal rotation and adduction. Which specific portion of the pectoralis major muscle complex is most commonly ruptured in this classic mechanism of injury?
Options:
- Clavicular head at the musculotendinous junction
- Sternal head at or near the humeral insertion
- Clavicular head at the clavicular origin
- Sternal head at the sternal origin
- Abdominal head at the musculotendinous junction
Correct Answer: Sternal head at or near the humeral insertion
Explanation:
Pectoralis major ruptures almost exclusively occur in young, active males during eccentric contraction activities, most notoriously the bench press. The sternal (sternocostal) head undergoes maximal stretch and tension when the arm is extended and externally rotated, making it mechanically the most vulnerable to rupture. The injury most commonly occurs at the humeral insertion (tendon avulsion) or at the musculotendinous junction of the sternal head. The clavicular head is often spared.
Question 100:
A 25-year-old cyclist goes over his handlebars and lands heavily on his left shoulder. Radiographs confirm a displaced midshaft clavicle fracture. While the decision for surgery often involves shared decision-making, which of the following scenarios is universally considered an absolute, unquestionable indication for immediate open reduction and internal fixation of a clavicle fracture?
Options:
- 1.5 cm of overall fracture shortening
- 100% superior displacement of the proximal fragment
- Severe comminution with a z-fragment
- Open fracture with exposed bone
- The patient is a high-demand professional athlete
Correct Answer: Open fracture with exposed bone
Explanation:
Absolute indications for operative management of a clavicle fracture include open fractures, fractures with associated progressive neurovascular injury, skin tenting that threatens to necrose and progress to an open fracture, and 'floating shoulder' (ipsilateral displaced clavicle and scapular neck fractures). High degrees of displacement, shortening >2 cm, comminution, and the patient's athletic or occupational demands are considered relative indications for surgery.