Full Question & Answer Text (for Search Engines)
Question 1:
A 12-year-old obese male presents with left thigh pain and obligatory external rotation during hip flexion. What is the most widely accepted absolute indication for prophylactic in situ pinning of the asymptomatic contralateral hip in the setting of Slipped Capital Femoral Epiphysis (SCFE)?
Options:
- Modified Oxford bone age of 14
- Acute, unstable slip on the affected side
- Underlying endocrinopathy or renal osteodystrophy
- Patient weight greater than the 95th percentile
- Southwick slip angle greater than 50 degrees on the affected side
Correct Answer: Underlying endocrinopathy or renal osteodystrophy
Explanation:
While the decision to prophylactically pin the contralateral hip in SCFE is often debated, absolute indications generally include patients with a known endocrinopathy (such as hypothyroidism or growth hormone deficiency) or renal osteodystrophy, as they have a significantly higher risk of a sequential slip. Other relative indications include young age (e.g., modified Oxford bone age < 16) or an inability to follow up, but endocrine disorders represent the most universally accepted absolute indication.
Question 2:
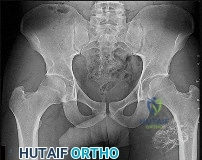
A 35-year-old male sustains an anteroposterior compression (APC) type II pelvic ring injury. During anterior ring fixation via an ilioinguinal approach, massive hemorrhage is encountered posterior to the superior pubic ramus. Which anomalous anatomical connection represents the classic 'corona mortis'?
Options:
- External iliac artery to internal pudendal artery
- External iliac artery or inferior epigastric artery to the obturator artery
- Internal iliac artery to superior gluteal artery
- Internal pudendal artery to inferior epigastric artery
- Internal pudendal artery to obturator artery
Correct Answer: External iliac artery or inferior epigastric artery to the obturator artery
Explanation:
The 'corona mortis' (crown of death) refers to a vascular anastomosis between the obturator and external iliac (or inferior epigastric) vascular systems. It is located posterior to the superior pubic ramus at a variable distance (average 5-6 cm) from the symphysis pubis and can cause life-threatening hemorrhage if inadvertently disrupted during anterior pelvic ring surgery (ilioinguinal or Stoppa approaches).
Question 3:
A 62-year-old male undergoes a C4-C6 posterior laminectomy and fusion for cervical spondylotic myelopathy. Postoperatively, he develops isolated deltoid and biceps weakness (3/5) but denies new sensory loss or leg weakness. What is the most likely etiology of this specific postoperative complication?
Options:
- Intraoperative spinal cord contusion
- Epidural hematoma
- Tethering of the nerve root due to posterior spinal cord shift
- Inadequate anterior decompression of the C6 nerve root
- Intraoperative prone positioning causing brachial plexopathy
Correct Answer: Tethering of the nerve root due to posterior spinal cord shift
Explanation:
The patient is experiencing a C5 palsy, a well-known complication after cervical decompressive surgery, particularly posterior laminectomy. The most widely accepted etiology is the tethering effect on the C5 nerve root caused by the posterior drift of the spinal cord following decompression. The C5 root has a relatively short and direct horizontal course, making it uniquely susceptible to traction injury when the cord migrates posteriorly.
Question 4:
A 40-year-old laborer complains of chronic radial-sided wrist pain. Radiographs demonstrate advanced arthrosis of the radioscaphoid joint and capitolunate joint, with a preserved radiolunate articulation. Based on these findings, which of the following is the most appropriate surgical treatment?
Options:
- Scaphoid open reduction internal fixation with vascularized bone graft
- Proximal row carpectomy (PRC)
- Scaphoid excision and four-corner fusion
- Radial styloidectomy and scaphoid fixation
- Total wrist arthrodesis
Correct Answer: Scaphoid excision and four-corner fusion
Explanation:
The clinical scenario describes Scaphoid Nonunion Advanced Collapse (SNAC) Stage III, characterized by arthrosis extending to the capitolunate joint but sparing the radiolunate joint. Proximal row carpectomy (PRC) is contraindicated in the presence of capitolunate arthrosis because the capitate must articulate with the lunate fossa of the radius. Therefore, scaphoid excision and four-corner fusion is the most appropriate motion-preserving salvage procedure.
Question 5:
A 19-year-old female undergoes MPFL reconstruction for recurrent patellar instability. To ensure proper isometry, the femoral attachment (Schöttle's point) must be accurately identified on a true lateral radiograph. Where is this point located?
Options:
- Anterior to the posterior femoral cortical line and distal to Blumensaat's line
- 1 mm anterior to the posterior femoral cortical line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to Blumensaat's line
- 1 mm posterior to the posterior femoral cortical line, 2.5 mm proximal to the posterior origin of the medial femoral condyle, and proximal to Blumensaat's line
- 2.5 mm anterior to the posterior femoral cortical line and exactly on Blumensaat's line
- Posterior to the posterior femoral cortical line and distal to Blumensaat's line
Correct Answer: 1 mm anterior to the posterior femoral cortical line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to Blumensaat's line
Explanation:
Schöttle's point is a radiographic landmark for the femoral origin of the medial patellofemoral ligament (MPFL). On a strict lateral radiograph, it is defined as 1 mm anterior to the posterior femoral cortical line, 2.5 mm distal to the posterior articular border of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat's line. Placing the graft at this point helps achieve near-isometric behavior.
Question 6:
A 50-year-old active male underwent a THA 3 years ago and now complains of an audible squeaking sound during hip flexion. Which of the following factors is most strongly associated with squeaking in ceramic-on-ceramic total hip arthroplasty?
Options:
- Use of a 28 mm femoral head
- Acetabular component anteversion of 15 degrees
- Component malposition leading to edge loading
- Body mass index > 40
- Use of a highly cross-linked polyethylene liner
Correct Answer: Component malposition leading to edge loading
Explanation:
Squeaking is a specific complication associated with hard-on-hard bearings, particularly ceramic-on-ceramic THA. The most significant biomechanical cause is edge loading, which occurs due to micro-separation, impingement, or component malposition (e.g., steep cup abduction angles or insufficient anteversion). This results in loss of fluid film lubrication and stripe wear, ultimately causing the squeak.
Question 7:
A 15-year-old male presents with knee pain, and biopsy confirms conventional high-grade osteosarcoma of the distal femur. Following neoadjuvant chemotherapy and wide resection, what histologic finding represents the most significant prognostic factor for long-term survival in localized disease?
Options:
- High mitotic index (>10 per HPF)
- Tumor necrosis rate < 90% following neoadjuvant chemotherapy
- Presence of chondroblastic elements
- Extension of tumor through the physis
- Presence of osteoid matrix throughout the tumor
Correct Answer: Tumor necrosis rate < 90% following neoadjuvant chemotherapy
Explanation:
In localized high-grade osteosarcoma, the degree of tumor necrosis after induction (neoadjuvant) chemotherapy is one of the most powerful prognostic indicators. A "good response" is typically defined as ≥ 90% necrosis (Huvos grade III or IV). A necrosis rate of less than 90% is an adverse prognostic factor for survival.
Question 8:
A 28-year-old male sustained a displaced talar neck fracture and underwent open reduction and internal fixation. Six weeks postoperatively, a subchondral radiolucent band is seen in the talar dome on the AP mortise radiograph. What does this radiographic finding indicate?
Options:
- Impending avascular necrosis of the talar body
- Nonunion of the fracture site
- Infection of the tibiotalar joint
- Intact vascularity to the talar body
- Early manifestation of post-traumatic subtalar arthritis
Correct Answer: Intact vascularity to the talar body
Explanation:
Hawkins sign is a subchondral radiolucent band seen in the talar dome 6 to 8 weeks after a talus fracture. It represents subchondral osteopenia secondary to disuse atrophy. Because bone resorption requires an active blood supply, the presence of a Hawkins sign is a highly reliable indicator that the talar body has intact vascularity and that avascular necrosis (AVN) is unlikely.
Question 9:
A 72-year-old female with cuff tear arthropathy undergoes a reverse total shoulder arthroplasty (rTSA) using a Grammont-style prosthesis. How does this classic implant design primarily alter the biomechanics of the shoulder to improve active elevation?
Options:
- Lateralizes the center of rotation to increase deltoid tension
- Medializes and distalizes the center of rotation to increase the deltoid moment arm
- Superiorly translates the center of rotation to recruit the intact lower subscapularis
- Medializes and proximalizes the center of rotation to decrease joint reactive forces
- Increases the offset of the humerus to restore the anatomical joint line
Correct Answer: Medializes and distalizes the center of rotation to increase the deltoid moment arm
Explanation:
The classic Grammont-style reverse total shoulder arthroplasty (rTSA) alters shoulder biomechanics by medializing and distalizing the center of rotation. This effectively lengthens the deltoid muscle (increasing its tension) and significantly increases its moment arm, allowing the deltoid to effectively elevate the arm in the absence of a functional rotator cuff.
Question 10:
A 45-year-old patient sustains a bicondylar tibial plateau fracture (Schatzker VI) with a displaced posteromedial fragment. When utilizing a posteromedial approach to buttress this fragment, the surgical dissection typically exploits the internervous/intermuscular interval between which two structures?
Options:
- Tibialis anterior and extensor hallucis longus
- Popliteus and soleus
- Lateral head of the gastrocnemius and biceps femoris
- Medial head of the gastrocnemius and the pes anserinus
- Flexor digitorum longus and tibialis posterior
Correct Answer: Medial head of the gastrocnemius and the pes anserinus
Explanation:
The posteromedial approach to the tibial plateau utilizes the interval between the medial head of the gastrocnemius (which is retracted posteriorly along with the neurovascular bundle) and the pes anserinus (which is retracted anteriorly). This provides direct access to the posteromedial metaphysis to place an anti-glide buttress plate.
Question 11:
An infant is treated with serial casting for idiopathic clubfoot using the Ponseti method. During the manipulative correction of the adductus and varus deformities, the physician's thumb must apply counter-pressure to which specific osseous structure to serve as a fulcrum?
Options:
- Medial aspect of the navicular
- Lateral aspect of the calcaneocuboid joint
- Head of the talus
- Sustentaculum tali
- Lateral malleolus
Correct Answer: Head of the talus
Explanation:
In the Ponseti method, the key to successful manipulation is applying counter-pressure with the thumb on the lateral aspect of the head of the talus. Pressure on the calcaneocuboid joint or lateral malleolus blocks abduction of the calcaneus, preventing correction of the heel varus and forefoot adductus.
Question 12:
A 55-year-old male presents with severe right anterior thigh pain and weakness in knee extension. MRI shows a far lateral (extraforaminal) disc herniation at L3-L4. Which nerve root is primarily compressed in this scenario?
Options:
- Exiting L3 nerve root
- Traversing L4 nerve root
- Exiting L4 nerve root
- Traversing L5 nerve root
- Exiting L2 nerve root
Correct Answer: Exiting L3 nerve root
Explanation:
In the lumbar spine, a classic posterolateral paracentral disc herniation compresses the traversing nerve root (e.g., an L3-L4 paracentral disc hits the L4 root). However, a far lateral (extraforaminal) disc herniation compresses the exiting nerve root at that level. Therefore, a far lateral L3-L4 disc herniation compresses the exiting L3 nerve root, causing anterior thigh pain and quadriceps weakness.
Question 13:
A 30-year-old sustains a laceration to the volar aspect of his index finger in Zone II, requiring primary FDP repair. To safely allow an early active motion protocol without gap formation or rupture, biomechanical studies suggest a minimum of how many core strands crossing the repair site?
Options:
- 2 strands
- 4 strands
- 6 strands
- 8 strands
- Epitendinous repair alone is sufficient
Correct Answer: 4 strands
Explanation:
Early active motion protocols after flexor tendon repair reduce adhesions and improve outcomes but place higher stresses on the repair. Biomechanical studies have demonstrated that a 2-strand repair is generally insufficient to withstand the forces of active flexion without gap formation. A minimum of a 4-strand core repair, ideally augmented with an epitendinous repair, is recommended for early active mobilization.
Question 14:
A 45-year-old recreational athlete presents with anterior shoulder pain. MRI arthrogram demonstrates a Type II SLAP tear. In patients over the age of 40, comparing primary biceps tenodesis to arthroscopic SLAP repair, literature shows that primary tenodesis generally results in:
Options:
- Higher rates of postoperative stiffness
- Increased incidence of revision surgery
- Lower rates of return to sport
- Equivalent or superior patient-reported outcomes with lower complication rates
- Decreased glenohumeral stability in the abduced-externally rotated position
Correct Answer: Equivalent or superior patient-reported outcomes with lower complication rates
Explanation:
In patients over 40 years old with symptomatic SLAP tears, primary biceps tenodesis has been shown to yield equivalent or superior clinical outcomes, higher rates of return to activity, and significantly lower rates of reoperation and postoperative stiffness compared to arthroscopic SLAP repair. Therefore, tenodesis is often favored in this age group.
Question 15:
Following a standard primary Total Knee Arthroplasty (TKA), the surgeon notes lateral patellar maltracking during the trial reduction. Which of the following component malrotations is most likely responsible for causing lateral patellar maltracking?
Options:
- External rotation of the femoral component and external rotation of the tibial component
- Internal rotation of the femoral component and internal rotation of the tibial component
- External rotation of the femoral component and internal rotation of the tibial component
- Internal rotation of the femoral component and external rotation of the tibial component
- Excessive lateralization of the tibial tray
Correct Answer: Internal rotation of the femoral component and internal rotation of the tibial component
Explanation:
Lateral patellar maltracking in TKA is primarily caused by an increase in the Q-angle. Internal rotation of the femoral component medializes the trochlear groove relative to the extensor mechanism. Internal rotation of the tibial component medializes the tibial tubercle. Both errors functionally increase the Q-angle and lead to lateral patellar tracking or subluxation.
Question 16:
A 32-year-old female is diagnosed with a Giant Cell Tumor (GCT) of the proximal tibia. She is prescribed Denosumab as neoadjuvant therapy. What is the precise mechanism of action of Denosumab in treating GCT?
Options:
- Binds to RANK receptor on osteoclasts, directly inhibiting their activation
- Binds to RANK Ligand (RANKL) expressed by the mononuclear stromal cells
- Inhibits vascular endothelial growth factor (VEGF), leading to tumor necrosis
- Binds directly to the multinucleated giant cells and induces apoptosis
- Inhibits farnesyl pyrophosphate synthase within osteoclasts
Correct Answer: Binds to RANK Ligand (RANKL) expressed by the mononuclear stromal cells
Explanation:
In Giant Cell Tumor of bone, the neoplastic cells are actually the mononuclear stromal cells, not the giant cells themselves. These stromal cells overexpress RANK Ligand (RANKL), which recruits and activates the reactive osteoclast-like multinucleated giant cells that cause bone destruction. Denosumab is a monoclonal antibody that binds to RANKL, preventing it from interacting with the RANK receptor on osteoclast precursors, thereby halting osteolysis.
Question 17:
Bone morphogenetic proteins (BMPs) play a critical role in osteoinduction and fracture healing. Upon BMP binding to its serine/threonine kinase cell surface receptors, which downstream intracellular signaling molecules are directly phosphorylated to translocate to the nucleus?
Options:
- JAK/STAT
- Smad 1, 5, and 8
- Smad 2 and 3
- Wnt/beta-catenin
- NF-kappaB
Correct Answer: Smad 1, 5, and 8
Explanation:
BMPs signal through serine/threonine kinase receptors. Upon binding, the receptors phosphorylate specific receptor-regulated Smad proteins. For BMPs, the specific intracellular mediators are Smad 1, Smad 5, and Smad 8. In contrast, TGF-beta primarily utilizes Smad 2 and Smad 3. The phosphorylated Smads then form a complex with Smad 4 to translocate into the nucleus and regulate gene expression.
Question 18:
A 38-year-old female sustains a coronal shear fracture of the capitellum and lateral trochlea. Operative fixation via an extensile lateral approach (Kocher interval) is planned. During distal extension of this approach, the surgeon must be careful to protect which nerve within the substance of the supinator muscle?
Options:
- Median nerve
- Anterior interosseous nerve
- Posterior interosseous nerve
- Superficial branch of the radial nerve
- Recurrent motor branch of the median nerve
Correct Answer: Posterior interosseous nerve
Explanation:
The Kocher approach exploits the interval between the extensor carpi ulnaris (ECU) and the anconeus. When extending this approach distally to expose the proximal radius and lateral elbow joint, the supinator muscle is elevated. The posterior interosseous nerve (PIN), a branch of the radial nerve, courses through the two heads of the supinator (arcade of Frohse) and is at significant risk of injury during distal dissection.
Question 19:
A 35-year-old female undergoes surgical release of the first dorsal extensor compartment for recalcitrant De Quervain's tenosynovitis. To prevent incomplete relief of symptoms, the surgeon must specifically look for and release a separate subsheath that frequently houses which of the following tendons?
Options:
- Extensor pollicis longus
- Abductor pollicis longus
- Extensor pollicis brevis
- Extensor carpi radialis longus
- Extensor indicis proprius
Correct Answer: Extensor pollicis brevis
Explanation:
De Quervain's tenosynovitis involves the first dorsal compartment, which contains the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons. Anatomical variations are common, and in a significant percentage of patients (up to 40%), the EPB is located within its own distinct subsheath. Failure to identify and release this EPB subsheath is the most common cause of persistent symptoms following surgery.
Question 20:
A 42-year-old male undergoes percutaneous repair of an acute Achilles tendon rupture. Postoperatively, he has numbness along the lateral aspect of his foot. The nerve most likely injured during this procedure typically crosses the lateral border of the Achilles tendon at what average distance proximal to the calcaneal insertion?
Options:
- 2 to 3 cm
- 5 to 7 cm
- 9 to 12 cm
- 15 to 18 cm
- 20 to 22 cm
Correct Answer: 9 to 12 cm
Explanation:
The sural nerve provides sensation to the posterolateral lower leg and the lateral aspect of the foot. It is at particular risk during percutaneous or minimally invasive Achilles tendon repairs. Anatomical studies show that the sural nerve typically crosses from medial to lateral across the lateral border of the Achilles tendon at an average distance of 9.8 to 10.5 cm proximal to its calcaneal insertion.
Question 21:
A 60-year-old male presents with progressively worsening clumsy hands and an unsteady, broad-based gait. Physical examination reveals a positive Hoffmann sign bilaterally and hyperreflexia in the lower extremities. Radiographs and MRI demonstrate Ossification of the Posterior Longitudinal Ligament (OPLL) extending continuously from C3 to C6. The 'K-line' (a line connecting the midpoints of the spinal canal at C2 and C7) is evaluated, and the OPLL mass crosses posteriorly to this line (K-line negative). Based on these imaging parameters, which of the following surgical approaches is most appropriate to adequately decompress the spinal cord?
Options:
- Posterior cervical laminoplasty
- Posterior cervical laminectomy and fusion
- Anterior cervical corpectomy and fusion
- Bilateral cervical foraminotomies
- C1-C2 posterior fusion
Correct Answer: Anterior cervical corpectomy and fusion
Explanation:
A K-line negative cervical spine indicates that the OPLL mass exceeds the line connecting the midpoints of the spinal canal from C2 to C7. In this scenario, posterior decompression (laminectomy or laminoplasty) will fail to achieve adequate indirect decompression because the spinal cord will not shift posteriorly enough to clear the anterior mass. Therefore, an anterior approach (corpectomy and fusion) or a combined anterior-posterior approach is indicated to directly resect the compressing OPLL.
Question 22:
During a primary total hip arthroplasty (THA), a multi-hole hemispherical acetabular component is used. The surgeon plans to place adjuvant screws for initial stability. Based on the Wasilewski quadrant system, placing a screw in the anterior-inferior quadrant places which of the following structures at highest risk of injury?
Options:
- Sciatic nerve
- Obturator nerve
- External iliac artery
- Superior gluteal nerve
- Internal pudendal artery
Correct Answer: Obturator nerve
Explanation:
According to the Wasilewski quadrant system (divided by a line from the ASIS through the center of the acetabulum and a perpendicular line), the posterior-superior quadrant is the safe zone for screw placement with the best bone stock. The anterior-superior quadrant places the external iliac artery and vein at risk. The anterior-inferior quadrant places the obturator nerve and vessels at risk. The posterior-inferior quadrant places the internal pudendal and inferior gluteal vessels at risk.
Question 23:
A 35-year-old male sustains an APC-III pelvic ring injury following a high-speed motorcycle collision. After initial hemodynamic stabilization, the surgeon elects to perform an open reduction and internal fixation of a widened sacroiliac (SI) joint via an anterior approach. During dissection and plate placement over the sacral ala, which neurological structure is at greatest risk of iatrogenic injury?
Options:
- L3 nerve root
- L4 nerve root
- L5 nerve root
- S1 nerve root
- Sciatic nerve
Correct Answer: L5 nerve root
Explanation:
During the anterior approach to the sacroiliac joint, the L5 nerve root is at significant risk. It courses directly over the sacral ala, typically approximately 2 cm medial to the SI joint, before joining the sacral plexus. Retraction or misplaced drills/screws in this region can easily injure the L5 root, leading to foot drop and sensory deficits.
Question 24:
A 24-year-old collegiate football player sustains a complete knee dislocation on the field. In the emergency department, the knee is successfully reduced. Pulses are palpable symmetrically, and the foot is well-perfused. An Ankle-Brachial Index (ABI) is calculated to be 0.85. What is the most appropriate next step in management?
Options:
- Discharge with urgent outpatient MRI
- Continued clinical observation with serial ABIs every 4 hours
- Immediate CT angiography of the lower extremity
- Immediate surgical exploration of the popliteal artery
- Application of a knee-spanning external fixator
Correct Answer: Immediate CT angiography of the lower extremity
Explanation:
In the setting of a knee dislocation, vascular assessment is critical due to the high risk of popliteal artery injury. Even if pulses are palpable, an ABI should be measured. An ABI > 0.9 can typically be observed with serial exams. An ABI < 0.9 (such as 0.85 in this case) warrants advanced vascular imaging, with CT angiography being the modern gold standard to identify an intimal tear or occlusion that could lead to delayed thrombosis.
Question 25:
A 48-year-old female presents with chronic, dull pain in her right proximal humerus that is worse at night. Radiographs demonstrate a well-circumscribed, lytic lesion with central 'popcorn' calcifications. MRI confirms a cartilaginous matrix, and cortical endosteal scalloping is present measuring 80% of the cortical thickness. What is the most appropriate definitive management?
Options:
- Intralesional curettage alone
- Intralesional curettage with phenol and polymethylmethacrylate (PMMA)
- Neoadjuvant chemotherapy followed by wide resection
- Wide surgical resection with negative margins
- Definitive radiation therapy
Correct Answer: Wide surgical resection with negative margins
Explanation:
The clinical presentation (pain at night) and radiographic findings (endosteal scalloping >2/3 of the cortical thickness, popcorn calcifications) are highly suspicious for a chondrosarcoma rather than a benign enchondroma. Low to intermediate-grade chondrosarcomas are managed with wide surgical resection, as they do not respond well to chemotherapy or radiation therapy.
Question 26:
A 42-year-old manual laborer presents with chronic radial-sided wrist pain 10 years after an untreated fall on an outstretched hand. Radiographs demonstrate a scaphoid nonunion advanced collapse (SNAC). Arthrosis is visible at both the radioscaphoid articulation and the capitolunate articulation, but the radiolunate joint is perfectly preserved (Stage III SNAC). Which of the following surgical procedures is strictly contraindicated in this patient?
Options:
- Proximal row carpectomy (PRC)
- Four-corner arthrodesis
- Total wrist arthrodesis
- Scaphoid excision and capitolunate fusion
- Denervation of the wrist
Correct Answer: Proximal row carpectomy (PRC)
Explanation:
A Proximal Row Carpectomy (PRC) relies on a preserved, healthy articulation between the proximal pole of the capitate and the lunate fossa of the radius. In Stage III SNAC (or SLAC) wrist, capitolunate arthritis is present, meaning the capitate cartilage is compromised. Therefore, PRC is contraindicated. A four-corner fusion (which fuses the capitate, lunate, hamate, and triquetrum) is the preferred motion-preserving salvage procedure for Stage III disease.
Question 27:
During operative fixation of a traumatic Lisfranc injury, the surgeon places the traditional 'home run screw' to recreate the primary restraint of the tarsometatarsal articulation. What is the correct anatomical trajectory for this screw?
Options:
- From the base of the first metatarsal into the intermediate cuneiform
- From the medial cuneiform into the base of the second metatarsal
- From the intermediate cuneiform into the base of the first metatarsal
- From the base of the second metatarsal into the medial cuneiform
- From the medial cuneiform into the base of the third metatarsal
Correct Answer: From the medial cuneiform into the base of the second metatarsal
Explanation:
The Lisfranc ligament is the strongest interosseous ligament in the tarsometatarsal joint complex, functioning as the primary stabilizer. It originates from the lateral surface of the medial cuneiform and inserts into the medial surface of the base of the second metatarsal. The 'home run screw' is placed from medial to lateral, starting at the medial cuneiform and aiming into the base of the second metatarsal to anatomically recreate this restraint.
Question 28:
Articular cartilage is functionally divided into multiple distinct structural zones. Which of the following accurately describes the composition of the deep zone of articular cartilage compared to the other zones?
Options:
- Highest concentration of proteoglycans and lowest concentration of water
- Highest concentration of water and lowest concentration of proteoglycans
- Highest concentration of collagen and highest concentration of water
- Lowest concentration of collagen and highest concentration of proteoglycans
- Equal concentrations of water and proteoglycans
Correct Answer: Highest concentration of proteoglycans and lowest concentration of water
Explanation:
The deep (radial) zone of articular cartilage is characterized by the highest concentration of proteoglycans and the lowest water content. The collagen fibers (mostly Type II) are arranged perpendicular to the joint surface to resist compressive forces. Conversely, the superficial (tangential) zone has the highest water content, lowest proteoglycan content, and collagen fibers oriented parallel to the joint surface to resist shear forces.
Question 29:
A 32-year-old male falls from a ladder and sustains a Hawkins Type III fracture of the talar neck. By definition, a Hawkins Type III injury involves a talar neck fracture accompanied by which of the following patterns of dislocation?
Options:
- Subluxation of the subtalar joint only
- Dislocation of the tibiotalar joint only
- Dislocation of both the subtalar and tibiotalar joints
- Dislocation of the subtalar, tibiotalar, and talonavicular joints
- Extrusion of the talar body with an intact talonavicular joint
Correct Answer: Dislocation of both the subtalar and tibiotalar joints
Explanation:
The Hawkins classification describes talar neck fractures: Type I is nondisplaced; Type II involves subtalar subluxation or dislocation; Type III involves dislocation of both the subtalar and tibiotalar (ankle) joints (the talar body extrudes posteromedially); Type IV (added by Canale) involves dislocation of the subtalar, tibiotalar, and talonavicular joints. The risk of avascular necrosis (AVN) increases substantially with each grade, approaching 100% in Type III/IV if not reduced urgently.
Question 30:
A surgeon is performing a percutaneous trigger finger release of the index finger. The A1 pulley is being transected. If the cutting instrument strays too far radially during the release, which structure is at greatest risk of iatrogenic injury?
Options:
- Ulnar digital nerve of the index finger
- Radial digital nerve of the index finger
- Ulnar digital artery of the index finger
- Flexor digitorum superficialis tendon
- Proper palmar digital nerve to the thumb
Correct Answer: Radial digital nerve of the index finger
Explanation:
During an A1 pulley release of the index finger, the radial digital nerve is at exceptional risk because it courses obliquely over the flexor sheath near the MP joint crease, crossing closer to the midline than in other digits. Similarly, the radial digital nerve of the thumb is at risk during thumb trigger release for the same anatomical reason.
Question 31:
A 2-month-old female is diagnosed with Developmental Dysplasia of the Hip (DDH). Ultrasound confirms a dislocated but reducible left hip. The orthopedist elects to initiate treatment with a Pavlik harness rather than rigid spica casting. What is the primary physiological advantage of using a Pavlik harness in this scenario?
Options:
- Lower risk of femoral nerve palsy
- Decreased risk of avascular necrosis of the femoral head
- Superior correction of acetabular version
- Faster rate of concentric reduction
- Prevention of residual pelvic obliquity
Correct Answer: Decreased risk of avascular necrosis of the femoral head
Explanation:
The primary advantage of the Pavlik harness over rigid immobilization (like a spica cast) in an infant is a significantly decreased risk of avascular necrosis (AVN) of the femoral head. The harness maintains the hip in the 'safe zone' of Ramsey (flexion and limited, non-forced abduction) while allowing active motion. Rigid casting, especially in excessive abduction (frog-leg position), forces the medial circumflex femoral artery against the labrum, leading to ischemia and AVN.
Question 32:
A 19-year-old female presents to the trauma bay after a motor vehicle collision. She was a back-seat passenger wearing only a lap belt. Radiographs and CT demonstrate a flexion-distraction injury (Chance fracture) through the L2 vertebral body, pedicles, and spinous process. Neurological examination is intact. Due to the mechanism of injury, which of the following associated injuries must be most highly suspected and investigated?
Options:
- Traumatic aortic rupture
- Bilateral renal lacerations
- Diaphragmatic tear
- Intra-abdominal visceral injury
- Pelvic ring disruption
Correct Answer: Intra-abdominal visceral injury
Explanation:
Chance fractures are osseous or ligamentous flexion-distraction injuries of the spine, classic for lap-belt-only mechanisms in motor vehicle collisions. The fulcrum of flexion is located anteriorly at the abdominal wall. As a result, the spine undergoes distraction posteriorly, and the intra-abdominal contents are violently compressed. There is a very high association (up to 50%) of intra-abdominal visceral injuries, most commonly involving the hollow viscus (small bowel) or mesentery.
Question 33:
During a primary Total Knee Arthroplasty (TKA) for a patient with a severe varus deformity, the surgeon evaluates the gaps and notes that the medial side is tight in both flexion and extension. To correctly balance the knee, the surgeon must perform a medial release. According to the standard stepwise sequence, which of the following structures should be released first?
Options:
- Deep medial collateral ligament (MCL)
- Superficial medial collateral ligament (MCL)
- Semimembranosus tendon
- Pes anserinus
- Medial head of the gastrocnemius
Correct Answer: Deep medial collateral ligament (MCL)
Explanation:
The classic sequential medial release for a fixed varus deformity in TKA progresses from deep to superficial and anterior to posterior. The first structure released is the deep MCL (meniscofemoral and meniscotibial ligaments) via excision of the medial meniscus and release from the proximal tibia. If further release is needed, the posteromedial capsule, followed by the semimembranosus, superficial MCL, and finally the pes anserinus are progressively elevated or released.
Question 34:
A 26-year-old overhead athlete undergoes shoulder arthroscopy for chronic pain. A Type II Superior Labrum Anterior to Posterior (SLAP) tear is identified. The surgeon places a suture anchor at the 12 o'clock position on the superior glenoid rim. If the drill or anchor is placed too deeply and medially into the glenoid neck, which neurological structure is at greatest risk of injury?
Options:
- Axillary nerve
- Musculocutaneous nerve
- Suprascapular nerve
- Spinal accessory nerve
- Lateral pectoral nerve
Correct Answer: Suprascapular nerve
Explanation:
The suprascapular nerve courses through the suprascapular notch and then through the spinoglenoid notch at the base of the coracoid process, passing approximately 1 to 2 cm medial to the superior glenoid rim. When placing suture anchors at the 12 o'clock position for a SLAP repair, drilling too deeply or angling too medially puts the suprascapular nerve at high risk of iatrogenic injury.
Question 35:
Recombinant human bone morphogenetic protein-2 (rhBMP-2) is utilized in orthopedic surgery for its potent osteoinductive properties. Upon binding to its specific transmembrane serine/threonine kinase receptors, rhBMP-2 induces bone formation via phosphorylation of which of the following intracellular signaling molecules?
Options:
- Smad 2 and 3
- Smad 1, 5, and 8
- JAK and STAT
- Beta-catenin
- NF-kappaB
Correct Answer: Smad 1, 5, and 8
Explanation:
Bone Morphogenetic Proteins (BMPs), part of the TGF-beta superfamily, initiate intracellular signaling by binding to Type I and Type II serine/threonine kinase receptors. BMP signaling specifically causes the phosphorylation of receptor-regulated Smads 1, 5, and 8. These bind to the co-Smad (Smad 4) and translocate to the nucleus to induce osteogenic gene transcription (like Runx2). In contrast, TGF-beta signals primarily through Smad 2 and 3.
Question 36:
A 68-year-old female undergoes open reduction and internal fixation of a 3-part proximal humerus fracture using a locking plate. Three months postoperatively, radiographs demonstrate a varus collapse of the humeral head and subsequent 'cut-out' of the proximal locking screws into the glenohumeral joint. Which of the following technical errors during the index procedure is the most significant risk factor for this complication?
Options:
- Failure to repair the subscapularis tendon
- Use of a deltopectoral rather than a deltoid-splitting approach
- Failure to place the plate exactly 2 cm distal to the greater tuberosity
- Lack of medial calcar support restoration
- Placement of more than four proximal locking screws
Correct Answer: Lack of medial calcar support restoration
Explanation:
The most critical biomechanical factor in preventing varus collapse and secondary screw cut-out in proximal humerus fracture plating is the restoration of medial calcar support. This is achieved by anatomically reducing the medial cortex and, critically, by placing the inferior-most locking screws (calcar screws) accurately into the inferomedial quadrant of the humeral head. If severe comminution exists, structural allograft strut augmentation may be required.
Question 37:
A 3-year-old boy is brought to the clinic for progressive bowing of his left leg. Radiographs demonstrate a sharp varus deformity localized to the proximal tibial metaphysis with medial beaking. The metaphyseal-diaphyseal angle (MDA) of Drennan is measured at 18 degrees. What is the most appropriate initial management for this patient?
Options:
- Knee-ankle-foot orthosis (KAFO) bracing
- Observation with repeat radiographs in 6 months
- Guided growth via medial proximal tibial hemiepiphysiodesis
- High tibial osteotomy with rigid internal fixation
- Administration of bisphosphonates
Correct Answer: Knee-ankle-foot orthosis (KAFO) bracing
Explanation:
This child has infantile Blount's disease (tibia vara). While physiologic bowing is common in toddlers, a metaphyseal-diaphyseal angle (MDA) > 16 degrees strongly suggests true infantile Blount's disease rather than physiologic bowing (which typically has an MDA < 10 degrees). For a child under the age of 4 with a high MDA, the initial recommended treatment is KAFO bracing to unweight the medial compartment. Surgery is reserved for older children or failure of conservative management.
Question 38:
A 38-year-old avid cyclist presents with a two-month history of numbness and tingling isolated to his right ring and small fingers. Physical examination reveals weakness in interossei abduction and adduction. Wrist flexion and extension strength are normal. Tinel's sign is positive over Guyon's canal at the wrist. Which of the following anatomic structures forms the floor of Guyon's canal?
Options:
- Volar carpal ligament
- Transverse carpal ligament (flexor retinaculum) and pisohamate ligament
- Pisiform and the hook of the hamate
- Palmar aponeurosis
- Extensor retinaculum
Correct Answer: Transverse carpal ligament (flexor retinaculum) and pisohamate ligament
Explanation:
Guyon's canal (the ulnar tunnel) contains the ulnar nerve and artery. Its boundaries are critical for understanding compression syndromes (like 'cyclist's palsy'). The roof is formed by the volar carpal ligament (and palmaris brevis). The ulnar border is the pisiform, and the radial border is the hook of the hamate. The floor is formed by the transverse carpal ligament (flexor retinaculum) and the pisohamate ligament.
Question 39:
A 12-year-old obese male undergoes in-situ percutaneous screw fixation for a unilateral Slipped Capital Femoral Epiphysis (SCFE). Prophylactic pinning of the contralateral, asymptomatic hip is considered. Which of the following patient profiles is the strongest indication for prophylactic contralateral pinning?
Options:
- Male sex and a body mass index (BMI) > 95th percentile
- Age of 14 years at initial presentation
- A known underlying diagnosis of hypothyroidism
- A severe (Grade III) slip on the affected side
- Closed triradiate cartilages bilaterally
Correct Answer: A known underlying diagnosis of hypothyroidism
Explanation:
The risk of developing a contralateral SCFE is significant (around 20-30%, higher in certain populations). Strong indications for prophylactic pinning of the contralateral hip include patients with underlying endocrinopathies (e.g., hypothyroidism, renal osteodystrophy, growth hormone deficiency), patients presenting at an unusually young age (males < 10, females < 9), and patients who are unreliable for follow-up. Obesity alone, while a risk factor for the primary slip, is not an absolute indication for prophylactic pinning.
Question 40:
A 58-year-old male with long-standing, poorly controlled type II diabetes presents with a unilaterally swollen, red, and warm left foot. He denies any constitutional symptoms, and his white blood cell count is normal. Radiographs reveal fragmentation and early subluxation at the tarsometatarsal joint. Skin is intact with no ulceration. What is the most appropriate initial management?
Options:
- Total contact casting and strict non-weight bearing
- Urgent open reduction and internal fixation of the midfoot
- Administration of broad-spectrum intravenous antibiotics
- Below-knee amputation
- Immediate prescription of custom-molded orthotic shoes
Correct Answer: Total contact casting and strict non-weight bearing
Explanation:
The patient's presentation is classic for acute (Eichenholtz Stage 1 - Development/Fragmentation) Charcot neuroarthropathy. The hallmark is a red, hot, swollen foot in a patient with peripheral neuropathy, often mimicking infection. Because there is no ulcer or systemic sign of infection, osteomyelitis is less likely, and antibiotics are not indicated. The gold standard initial management to arrest the progressive bony destruction and deformity is immobilization via a Total Contact Cast (TCC) and offloading.