Full Question & Answer Text (for Search Engines)
Question 1:
A 5-year-old boy presents to the emergency department after falling from monkey bars. He sustained a displaced extension-type supracondylar humerus fracture. Examination reveals an inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which of the following nerves is most likely injured?
Options:
- Anterior interosseous nerve
- Posterior interosseous nerve
- Ulnar nerve
- Radial nerve
- Musculocutaneous nerve
Correct Answer: Anterior interosseous nerve
Explanation:
The anterior interosseous nerve (AIN) is a branch of the median nerve and is the most commonly injured nerve in extension-type supracondylar humerus fractures. Injury to the AIN results in the inability to form an 'OK' sign due to weakness of the flexor pollicis longus and the flexor digitorum profundus to the index finger.
Question 2:
A 75-year-old woman sustains a displaced femoral neck fracture after a mechanical fall. Which of the following is the predominant blood supply to the femoral head that is at risk of disruption in this injury?
Options:
- Artery of the ligamentum teres
- Inferior gluteal artery
- Deep branch of the medial femoral circumflex artery
- Lateral femoral circumflex artery
- Profunda femoris artery
Correct Answer: Deep branch of the medial femoral circumflex artery
Explanation:
The predominant blood supply to the adult femoral head is provided by the lateral epiphyseal artery, which is the terminal branch of the medial femoral circumflex artery (MFCA). This runs along the posterosuperior aspect of the femoral neck and is frequently disrupted in displaced femoral neck fractures, leading to a high risk of avascular necrosis.
Question 3:
A 15-year-old boy presents with progressive knee pain and swelling for two months. Radiographs demonstrate a metaphyseal lesion in the distal femur with a 'sunburst' periosteal reaction and Codman's triangle. A biopsy confirms a high-grade primary bone sarcoma. Which of the following genetic alterations is most closely associated with this condition?
Options:
- t(11;22) translocation
- Mutation of the EXT1 gene
- Inactivation of the RB1 and TP53 tumor suppressor genes
- t(X;18) translocation
- GNAS1 mutation
Correct Answer: Inactivation of the RB1 and TP53 tumor suppressor genes
Explanation:
The clinical presentation and imaging are classic for osteosarcoma. Osteosarcoma is strongly associated with mutations or inactivations of tumor suppressor genes, particularly RB1 (Retinoblastoma gene) and TP53 (Li-Fraumeni syndrome). t(11;22) is seen in Ewing sarcoma. t(X;18) is seen in synovial sarcoma. EXT1 is associated with multiple hereditary exostoses. GNAS1 is associated with fibrous dysplasia.
Question 4:
A 68-year-old man presents with bilateral leg pain and cramping that worsens with walking and prolonged standing, but improves when he leans forward over a shopping cart or sits down. What is the most likely pathophysiologic mechanism for his symptom relief with flexion?
Options:
- Decreased metabolic demand on the lower extremity musculature
- Unbuckling of the ligamentum flavum leading to increased canal volume
- Increased tension on the dural sac
- Spasm of the paraspinal musculature
- Relief of arterial claudication
Correct Answer: Unbuckling of the ligamentum flavum leading to increased canal volume
Explanation:
The patient's symptoms are classic for neurogenic claudication secondary to lumbar spinal stenosis. Lumbar flexion relieves symptoms by unbuckling the ligamentum flavum, which increases the cross-sectional area of the spinal canal and neural foramina, thereby temporarily relieving compression on the neural elements.
Question 5:
A 40-year-old recreational basketball player feels a sudden 'pop' in his posterior ankle while jumping. On examination, he has a positive Thompson test. If non-operative management is chosen, what is the most appropriate initial immobilization position?
Options:
- Short leg cast in maximum dorsiflexion
- Short leg cast in neutral position
- Short leg cast in 20 degrees of plantarflexion
- Long leg cast in knee flexion and ankle dorsiflexion
- Rigid walking boot with immediate full weight-bearing in neutral
Correct Answer: Short leg cast in 20 degrees of plantarflexion
Explanation:
The patient has an acute Achilles tendon rupture. Non-operative management typically begins with immobilization in a resting equinus position (usually about 20-30 degrees of plantarflexion) to approximate the torn tendon ends. This position is progressively adjusted towards neutral over a period of weeks using a cast or a functional orthosis with heel wedges.
Question 6:
A 35-year-old mechanic presents with a swollen, painful index finger 3 days after sustaining a puncture wound. The finger is held in a flexed posture, is uniformly swollen, tender along the volar aspect, and exquisitely painful with passive extension. What is the most appropriate next step in management?
Options:
- Oral antibiotics and buddy taping
- Immediate bedside incision and drainage in the emergency department
- Surgical irrigation and debridement of the flexor tendon sheath and intravenous antibiotics
- Corticosteroid injection into the flexor sheath
- Splinting in extension and close observation
Correct Answer: Surgical irrigation and debridement of the flexor tendon sheath and intravenous antibiotics
Explanation:
The patient presents with all four Kanavel signs (fusiform swelling, flexed posture, tenderness along the flexor tendon sheath, and pain on passive extension), indicating pyogenic flexor tenosynovitis. This is a surgical emergency requiring prompt formal surgical irrigation and debridement of the flexor tendon sheath in the operating room, along with broad-spectrum intravenous antibiotics.
Question 7:
A 6-week-old female infant is evaluated for developmental dysplasia of the hip (DDH). Ultrasound is performed, and an alpha angle of 45 degrees is noted on the right hip. She is prescribed a Pavlik harness. Which of the following complications is most likely to occur if the harness is placed in excessive hip flexion (greater than 120 degrees)?
Options:
- Femoral nerve palsy
- Sciatic nerve palsy
- Avascular necrosis of the femoral head
- Obturator nerve palsy
- Inferior hip dislocation
Correct Answer: Femoral nerve palsy
Explanation:
In the use of a Pavlik harness for DDH, excessive hip flexion (typically > 120 degrees) is known to cause femoral nerve palsy due to compression of the nerve against the inguinal ligament. Excessive abduction is associated with avascular necrosis of the femoral head.
Question 8:
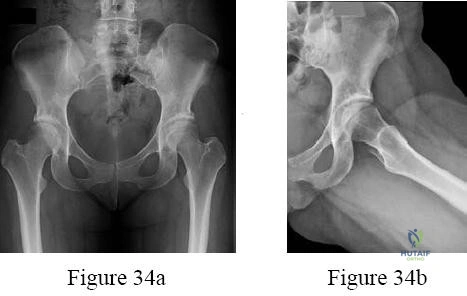
A 13-year-old overweight boy presents with a 3-week history of right groin and knee pain. He walks with a limp. On examination, when his right hip is flexed, it obligatorily externally rotates. Radiographs show a slip of the proximal femoral epiphysis. Which radiographic line is used to diagnose this condition?
Options:
- Shenton's line
- Hilgenreiner's line
- Klein's line
- Perkin's line
- Ward's triangle
Correct Answer: Klein's line
Explanation:
The clinical scenario describes Slipped Capital Femoral Epiphysis (SCFE). Klein's line is drawn along the superior edge of the femoral neck on an AP pelvic radiograph. In a normal hip, this line should intersect a portion of the lateral capital femoral epiphysis. In SCFE, the line passes superior to the epiphysis or intersects less of it compared to the contralateral normal side (Trethowan's sign).
Question 9:
A 22-year-old female soccer player sustains a twisting injury to her left knee. An AP radiograph demonstrates a small vertical avulsion fracture of the lateral tibial plateau, distal to the joint line. This fracture is considered pathognomonic for an injury to which of the following structures?
Options:
- Posterior cruciate ligament
- Anterior cruciate ligament
- Medial collateral ligament
- Lateral meniscus
- Popliteus tendon
Correct Answer: Anterior cruciate ligament
Explanation:
The radiograph describes a Segond fracture, which is an avulsion fracture of the anterolateral aspect of the proximal tibia. It is typically associated with avulsion of the anterolateral ligament (ALL) or lateral capsular attachments and is highly predictive (pathognomonic) of an anterior cruciate ligament (ACL) tear.
Question 10:
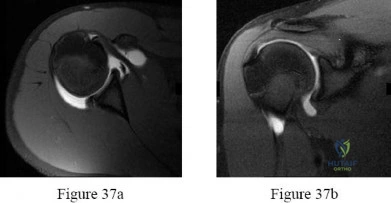
A 55-year-old carpenter presents with right shoulder pain and weakness after attempting to lift a heavy tool box. On physical examination, he demonstrates a positive drop-arm test and profound weakness with active abduction in the scapular plane. An MRI confirms a massive, retracted tear of the supraspinatus and infraspinatus tendons. Fatty infiltration of these muscles is graded. Which classification system is most commonly used to grade fatty infiltration of the rotator cuff muscles on imaging?
Options:
- Patte classification
- Goutallier classification
- Snyder classification
- Hamada classification
- Seebauer classification
Correct Answer: Goutallier classification
Explanation:
The Goutallier classification is used to quantify the amount of fatty infiltration of the rotator cuff muscles, originally described on CT but now widely adapted for MRI. High grades of fatty infiltration (Goutallier 3 and 4) are associated with poor functional outcomes and higher re-tear rates following surgical repair.
Question 11:
A 45-year-old construction worker falls from a 15-foot scaffold and sustains a highly comminuted, intra-articular distal tibia (Pilon) fracture. Severe soft tissue swelling and fracture blisters are present on presentation. What is the most appropriate initial management for this injury?
Options:
- Immediate open reduction and internal fixation with dual plating
- Application of a spanning external fixator and delayed internal fixation
- Percutaneous screw fixation of the articular surface followed by early range of motion
- Primary ankle arthrodesis
- Closed reduction and long leg cast application
Correct Answer: Application of a spanning external fixator and delayed internal fixation
Explanation:
High-energy Pilon fractures are often associated with significant soft tissue compromise. The standard of care is a staged protocol: initial application of a spanning external fixator (with or without fibular fixation) to stabilize the fracture and allow the soft tissues to recover (until the 'wrinkle sign' appears), followed by delayed definitive open reduction and internal fixation (ORIF) typically 10-21 days later. This minimizes the risk of catastrophic wound complications.
Question 12:
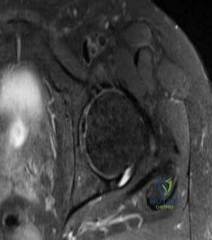
A 30-year-old woman presents with worsening knee pain. Radiographs reveal an eccentric, lytic, expansile lesion located in the epiphysis of the proximal tibia, extending to the subchondral bone. There is no sclerotic margin. Histology demonstrates mononuclear cells and numerous uniformly distributed osteoclast-like multinucleated giant cells. Which of the following is the most effective targeted medical therapy for advanced, unresectable cases of this tumor?
Options:
- Imatinib
- Denosumab
- Methotrexate
- Doxorubicin
- Rituximab
Correct Answer: Denosumab
Explanation:
The clinical and radiographic presentation is classic for a Giant Cell Tumor of Bone (GCTB). The neoplastic mononuclear cells in GCTB express high levels of RANKL, which recruits and activates the osteoclast-like giant cells, leading to massive bone destruction. Denosumab, a monoclonal antibody against RANKL, is highly effective in treating GCTB and is used for unresectable or recurrent lesions, or as a neoadjuvant therapy.
Question 13:
A 25-year-old male is involved in a high-speed motorcycle accident. Pelvic radiographs demonstrate symphysis pubis diastasis of 3.5 cm and widening of the anterior sacroiliac joints bilaterally. The posterior sacroiliac ligaments are determined to be intact. According to the Young-Burgess classification, what type of pelvic ring injury does this patient have?
Options:
- Lateral Compression Type I (LC-I)
- Lateral Compression Type II (LC-II)
- Anteroposterior Compression Type II (APC-II)
- Anteroposterior Compression Type III (APC-III)
- Vertical Shear (VS)
Correct Answer: Anteroposterior Compression Type II (APC-II)
Explanation:
The injury mechanism is anteroposterior compression (APC). APC-II is characterized by disruption of the symphysis pubis (or anterior ring fractures) along with disruption of the anterior sacroiliac ligaments, sacrotuberous, and sacrospinous ligaments, while the posterior sacroiliac ligaments remain intact. This causes rotational instability but preserves vertical stability. APC-III involves complete disruption of both anterior and posterior SI ligaments, resulting in both rotational and vertical instability.
Question 14:
A 34-year-old man suffers an ankle injury after slipping on ice. Radiographs reveal a transverse fracture of the medial malleolus and a short oblique fracture of the lateral malleolus starting at the level of the joint line. According to the Lauge-Hansen classification, what is the most likely mechanism of injury?
Options:
- Supination-Adduction (SAD)
- Supination-External Rotation (SER)
- Pronation-Abduction (PAB)
- Pronation-External Rotation (PER)
- Axial loading
Correct Answer: Supination-External Rotation (SER)
Explanation:
The Lauge-Hansen Supination-External Rotation (SER) injury is the most common type of ankle fracture. The sequence of injury is: 1) Anterior inferior tibiofibular ligament (AITFL) rupture, 2) Short oblique/spiral fracture of the fibula at the level of the syndesmosis, 3) Posterior inferior tibiofibular ligament (PITFL) rupture or posterior malleolus fracture, 4) Medial malleolus transverse fracture or deltoid ligament rupture. The short oblique fibula fracture at the joint line is characteristic of SER injuries.
Question 15:
A 48-year-old female secretary presents with numbness and tingling in her thumb, index, and middle fingers that wakes her up at night. She has noted weakness in her grip and visible flattening of her thenar eminence. She is diagnosed with severe carpal tunnel syndrome. Which of the following thenar muscles is NOT innervated by the median nerve and would therefore be spared in this condition?
Options:
- Abductor pollicis brevis
- Opponens pollicis
- Superficial head of flexor pollicis brevis
- Adductor pollicis
- First lumbrical
Correct Answer: Adductor pollicis
Explanation:
The recurrent motor branch of the median nerve innervates the 'OAF' muscles of the thenar eminence: Opponens pollicis, Abductor pollicis brevis, and the superficial head of the Flexor pollicis brevis. The Adductor pollicis, along with the deep head of the flexor pollicis brevis, is innervated by the deep branch of the ulnar nerve and is spared in carpal tunnel syndrome.
Question 16:
A 20-year-old college student falls onto an outstretched hand and presents with anatomic snuffbox tenderness. Initial radiographs are negative, but an MRI obtained 3 days later confirms a non-displaced fracture of the proximal pole of the scaphoid. The patient is at high risk for avascular necrosis due to the scaphoid's retrograde blood supply. Which of the following vessels provides the primary blood supply to the proximal pole of the scaphoid?
Options:
- Volar carpal branch of the radial artery
- Dorsal carpal branch of the radial artery
- Superficial palmar arch
- Deep palmar arch
- Anterior interosseous artery
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The primary blood supply to the scaphoid comes from the dorsal carpal branch of the radial artery, which enters the scaphoid near the waist in a distal-to-proximal (retrograde) fashion. Because the proximal pole relies entirely on this retrograde flow, fractures at the waist or proximal pole put the proximal segment at significant risk of avascular necrosis and nonunion.
Question 17:
A 6-year-old boy presents with a painless limp of several months' duration. Examination reveals restricted hip abduction and internal rotation. Radiographs demonstrate sclerosis and flattening of the capital femoral epiphysis consistent with Legg-Calve-Perthes disease. According to the Waldenström classification, what is the sequence of radiographic stages in this disease?
Options:
- Fragmentation, Initial, Reossification, Healed
- Initial, Fragmentation, Reossification, Healed
- Reossification, Initial, Fragmentation, Healed
- Initial, Reossification, Fragmentation, Healed
- Healed, Reossification, Fragmentation, Initial
Correct Answer: Initial, Fragmentation, Reossification, Healed
Explanation:
The Waldenström classification of Legg-Calve-Perthes disease outlines four stages: 1) Initial (infarction/necrosis) stage, characterized by sclerosis and cessation of growth; 2) Fragmentation stage, where the epiphysis appears fragmented as necrotic bone is resorbed; 3) Reossification stage, where new bone forms; and 4) Healed (residual) stage, where the bone is fully reossified, though often with a deformed head.
Question 18:
A 60-year-old woman presents 4 weeks after sustaining a nondisplaced distal radius fracture, which was managed in a short arm cast. She now complains of a sudden inability to actively extend the interphalangeal joint of her thumb. Which of the following represents the most likely etiology of this complication?
Options:
- Injury to the posterior interosseous nerve
- Attritional rupture of the extensor pollicis longus tendon over Lister's tubercle
- Volar subluxation of the distal radioulnar joint
- Adhesion of the flexor pollicis longus tendon
- Ischemic contracture of the forearm musculature
Correct Answer: Attritional rupture of the extensor pollicis longus tendon over Lister's tubercle
Explanation:
Extensor pollicis longus (EPL) tendon rupture is a known complication following distal radius fractures, peculiarly most often associated with non-displaced or minimally displaced fractures. It occurs due to attritional wear as the tendon glides over the fracture callus near Lister's tubercle, combined with focal ischemia within the third dorsal compartment. The classic presentation is a sudden inability to extend the IP joint of the thumb a few weeks post-injury. Treatment is typically an extensor indicis proprius (EIP) to EPL tendon transfer.
Question 19:
A 70-year-old man presents with progressive bilateral hand clumsiness, difficulty buttoning his shirt, and gait instability. Examination reveals a positive Hoffman's sign bilaterally, inverted radial reflex, and hyperreflexia in the lower extremities. An MRI of the cervical spine is ordered. What is the most likely diagnosis?
Options:
- Amyotrophic lateral sclerosis
- Cervical spondylotic myelopathy
- Syringomyelia
- Multiple sclerosis
- Guillain-Barre syndrome
Correct Answer: Cervical spondylotic myelopathy
Explanation:
The patient exhibits classic signs of cervical spondylotic myelopathy (CSM), which is the most common cause of spinal cord dysfunction in adults over 55. Symptoms include loss of fine motor skills (hand clumsiness) and gait changes. Physical exam reveals upper motor neuron signs such as Hoffman's sign, hyperreflexia, Babinski sign, and the inverted radial reflex.
Question 20:
A 28-year-old man sustains a closed, highly comminuted tibia fracture. He is admitted for observation. Several hours later, he reports escalating leg pain that is out of proportion to his injury and is not relieved by opioid analgesics. Passive stretching of his toes elicits severe pain. Compartment pressures are measured. What criteria strongly indicates the need for an emergent four-compartment fasciotomy?
Options:
- Absolute compartment pressure greater than 15 mmHg
- Diastolic blood pressure minus compartment pressure (Delta p) less than 30 mmHg
- Systolic blood pressure minus compartment pressure less than 50 mmHg
- Compartment pressure equal to venous pressure
- Loss of palpable distal pulses
Correct Answer: Diastolic blood pressure minus compartment pressure (Delta p) less than 30 mmHg
Explanation:
Acute compartment syndrome is a surgical emergency. The most reliable objective parameter indicating the need for fasciotomy is the Delta P, defined as the diastolic blood pressure minus the intracompartmental pressure. A Delta P of less than 30 mmHg (some authors use 30-40 mmHg) is highly indicative of compartment syndrome and dictates immediate fasciotomy. Loss of pulses is a very late and often absent sign.
Question 21:
A 35-year-old male is involved in a high-speed motor vehicle collision. Radiographs demonstrate a traumatic spondylolisthesis of the axis (Hangman's fracture) with severe angulation and >3 mm of translation. The C2-C3 disc space is disrupted, and the C2 articular facets are dislocated anteriorly. According to the Levine and Edwards classification (Type III), what is the most appropriate management?
Options:
- Rigid cervical orthosis for 6 weeks
- Halo vest immobilization after closed postural reduction
- Closed reduction with skeletal traction
- Posterior open reduction of the facets and C2-C3 fusion
- Anterior C2-C3 fusion alone
Correct Answer: Posterior open reduction of the facets and C2-C3 fusion
Explanation:
Levine and Edwards Type III Hangman's fractures involve bilateral C2-C3 facet dislocations with severe angulation and translation. They are highly unstable and cannot be managed with closed reduction or traction due to the risk of further displacement and catastrophic neurologic injury. The recommended treatment is posterior open reduction of the dislocated facets followed by C2-C3 posterior spinal fusion.
Question 22:
A 45-year-old male presents after a motorcycle accident with an anteroposterior compression (APC) Type III pelvic ring injury. He is hemodynamically unstable despite initial resuscitation, massive transfusion protocol, and application of a pelvic binder. What is the next most appropriate step in management?
Options:
- Immediate application of a supra-acetabular external fixator
- Preperitoneal pelvic packing and/or angioembolization
- Open reduction and internal fixation of the pubic symphysis
- Retrograde urethrogram to rule out urologic injury
- Percutaneous sacroiliac screw fixation
Correct Answer: Preperitoneal pelvic packing and/or angioembolization
Explanation:
In a hemodynamically unstable patient with an APC III pelvic ring injury who does not respond to a pelvic binder and initial fluid resuscitation, the source of bleeding is typically venous (presacral plexus) or arterial. Preperitoneal pelvic packing and/or angiography with embolization are the most appropriate next steps to achieve hemodynamic stability before any definitive orthopedic fixation.
Question 23:
A patient with a chronic high median nerve palsy requires tendon transfers to restore function. Which of the following combinations of tendon transfers is most appropriate to restore thumb flexion, thumb opposition, and index/long finger flexion?
Options:
- Brachioradialis (BR) to FPL, ECRL to FDP, EIP to APB
- ECRL to FPL, FCU to FDP, ADM to APB
- ECU to FPL, ECRB to FDP, PL to APB
- BR to FPL, ECU to FDP, EIP to APB
- ECRL to FPL, BR to FDP, EDM to APB
Correct Answer: Brachioradialis (BR) to FPL, ECRL to FDP, EIP to APB
Explanation:
In a high median nerve palsy, there is loss of thumb flexion (FPL), index/long finger flexion (FDP), and thumb opposition (APB). A common set of transfers includes the Brachioradialis (BR) to the Flexor Pollicis Longus (FPL) to restore thumb flexion, the Extensor Carpi Radialis Longus (ECRL) to the FDP of the index and long fingers to restore finger flexion, and the Extensor Indicis Proprius (EIP) to the Abductor Pollicis Brevis (APB) (Burkhalter transfer) to restore opposition.
Question 24:
The Lisfranc ligament is a critical stabilizing structure of the midfoot. Between which two bones does the primary interosseous Lisfranc ligament traverse?
Options:
- Medial cuneiform and the base of the first metatarsal
- Medial cuneiform and the base of the second metatarsal
- Middle cuneiform and the base of the second metatarsal
- Lateral cuneiform and the base of the third metatarsal
- Cuboid and the base of the fourth metatarsal
Correct Answer: Medial cuneiform and the base of the second metatarsal
Explanation:
The Lisfranc ligament is a strong interosseous ligament that connects the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. It is critical for the stability of the tarsometatarsal joint complex, particularly because there is no transverse intermetatarsal ligament between the bases of the first and second metatarsals.
Question 25:
A 13-year-old obese male underwent in situ single-screw pinning for a severe, unstable slipped capital femoral epiphysis (SCFE) 6 months ago. He now complains of progressive hip stiffness and pain. Radiographs demonstrate marked concentric joint space narrowing of the affected hip without evidence of avascular necrosis. What is the most likely diagnosis?
Options:
- Deep joint space infection
- Heterotopic ossification
- Chondrolysis
- Screw penetration into the joint
- Cam-type femoroacetabular impingement
Correct Answer: Chondrolysis
Explanation:
Chondrolysis is a known complication of SCFE, characterized by acute articular cartilage destruction, concentric joint space narrowing (typically <3 mm), stiffness, and pain. It is more common in severe slips, unstable slips, and historically with spica cast immobilization or unrecognized intra-articular hardware penetration, though it can occur idiopathically post-slip.
Question 26:
Demineralized bone matrix (DBM) is commonly used as a bone graft extender in spinal fusion surgery. Which of the following correctly describes the biologic properties of DBM?
Options:
- Osteogenic, osteoinductive, and osteoconductive
- Osteoinductive and osteoconductive only
- Osteoconductive only
- Osteogenic and osteoconductive only
- Osteoinductive only
Correct Answer: Osteoinductive and osteoconductive only
Explanation:
Demineralized bone matrix (DBM) is processed allograft bone that has had the inorganic mineral component removed, leaving the organic collagen matrix and growth factors (such as bone morphogenetic proteins, BMPs). It is osteoinductive (due to the presence of BMPs) and osteoconductive (providing a biologic scaffold). It is not osteogenic because the processing destroys living cells (osteoblasts or osteoprogenitor cells).
Question 27:
A 14-year-old girl presents with pain and swelling over her distal femur. Radiographs show an eccentric, expansile, lytic lesion in the metaphysis. MRI demonstrates multiple fluid-fluid levels. A biopsy confirms an aneurysmal bone cyst (ABC). What is the classic genetic translocation associated with primary ABCs?
Options:
- t(11;22)
- t(12;16)
- t(16;17)
- t(X;18)
- t(9;22)
Correct Answer: t(16;17)
Explanation:
Primary Aneurysmal Bone Cysts (ABCs) are neoplastic processes often associated with a characteristic genetic translocation, t(16;17)(q22;p13), which results in the fusion of the CDH11 and USP6 genes. Secondary ABCs can occur in association with other tumors (like giant cell tumors or chondroblastoma) but lack this specific translocation. t(11;22) is associated with Ewing sarcoma; t(12;16) with myxoid liposarcoma; t(X;18) with synovial sarcoma.
Question 28:
A 68-year-old female undergoes a total hip arthroplasty via a posterior approach. She subsequently sustains a posterior dislocation. Which of the following component positions most increases the risk of posterior dislocation?
Options:
- Increased acetabular anteversion and increased femoral anteversion
- Decreased acetabular anteversion and decreased femoral anteversion
- Increased acetabular abduction angle and increased femoral anteversion
- Decreased acetabular abduction angle and increased acetabular anteversion
- Increased acetabular retroversion and increased femoral retroversion
Correct Answer: Decreased acetabular anteversion and decreased femoral anteversion
Explanation:
Posterior dislocation of a total hip arthroplasty is most commonly associated with relative retroversion of the components (decreased acetabular anteversion and decreased femoral anteversion). This combined position leads to premature impingement anteriorly during flexion, adduction, and internal rotation, which physically levers the femoral head out of the acetabulum posteriorly.
Question 29:
During reconstruction of the posterolateral corner (PLC) of the knee, identifying the insertion of the popliteofibular ligament (PFL) is crucial. Where does the PFL anatomically insert?
Options:
- Anterior aspect of the fibular head
- Posteromedial aspect of the fibular styloid
- Anterolateral aspect of the fibular head
- Posterolateral aspect of the lateral tibial plateau
- Gerdy's tubercle
Correct Answer: Posteromedial aspect of the fibular styloid
Explanation:
The posterolateral corner (PLC) includes the lateral collateral ligament (LCL), popliteus tendon, and popliteofibular ligament (PFL). The PFL originates from the popliteus musculotendinous junction and inserts on the posteromedial aspect of the fibular styloid (tip of the fibular head). This ligament is a primary restraint to external rotation of the tibia.
Question 30:
A 72-year-old female sustains a 3-part proximal humerus fracture. She is indicated for an open reduction and internal fixation (ORIF) with a locking plate via a deltopectoral approach. To avoid injury to the axillary nerve, what is the generally accepted 'danger zone' for plate placement distal to the tip of the greater tuberosity?
Options:
- 2 to 3 cm
- 3 to 4 cm
- 5 to 7 cm
- 8 to 10 cm
- 10 to 12 cm
Correct Answer: 5 to 7 cm
Explanation:
The axillary nerve courses horizontally across the anterior aspect of the upper humerus. The average distance from the superior aspect of the greater tuberosity to the axillary nerve is approximately 5 to 7 cm. When placing a lateral locking plate for proximal humerus fractures, dissecting or passing the plate in this zone puts the nerve at high risk. Care must be taken to either slide the plate under the nerve or clearly identify and protect it.
Question 31:
A 15-year-old female gymnast complains of chronic lower back pain. Lateral lumbar radiographs reveal an isthmic spondylolisthesis at L5-S1 with 65% anterior translation of L5 on S1. According to the Meyerding classification, what grade is this slip?
Options:
- Grade I
- Grade II
- Grade III
- Grade IV
- Grade V (Spondyloptosis)
Correct Answer: Grade III
Explanation:
The Meyerding classification grades spondylolisthesis based on the percentage of anterior translation of the superior vertebral body over the inferior one. Grade I: 0-25%; Grade II: 26-50%; Grade III: 51-75%; Grade IV: 76-100%; Grade V: >100% (Spondyloptosis). A 65% slip falls into the Grade III category.
Question 32:
A 32-year-old manual laborer presents with dorsal wrist pain and decreased grip strength. Radiographs show sclerosis and fragmentation of the lunate, with proximal migration of the capitate and a loss of carpal height. There is no evidence of radiocarpal or midcarpal osteoarthritis. What is the Lichtman classification stage of this patient's Kienböck's disease?
Options:
- Stage I
- Stage II
- Stage IIIA
- Stage IIIB
- Stage IV
Correct Answer: Stage IIIB
Explanation:
The Lichtman classification for Kienböck's disease (avascular necrosis of the lunate): Stage I has normal x-rays (changes seen only on MRI). Stage II shows lunate sclerosis without collapse. Stage IIIA shows lunate collapse without fixed scaphoid rotation or carpal height loss. Stage IIIB shows lunate collapse with fixed scaphoid flexion, proximal migration of the capitate, and loss of carpal height, but NO osteoarthritis. Stage IV includes secondary radiocarpal or midcarpal osteoarthritis.
Question 33:
A 55-year-old female presents with medial ankle pain and a progressive flatfoot deformity. On examination, she has a flexible flatfoot, valgus hindfoot that corrects on a toe-raise, and she is unable to perform a single-limb heel rise on the affected side. According to the Johnson and Strom classification (modified by Myerson), what stage of Posterior Tibial Tendon Dysfunction (PTTD) does she have?
Options:
- Stage I
- Stage II
- Stage III
- Stage IV
- Stage V
Correct Answer: Stage II
Explanation:
Stage I PTTD involves tenosynovitis with mild pain but no deformity; the patient can still perform a single heel rise. Stage II involves a flexible flatfoot deformity, and the patient is unable to perform a single heel rise. Stage III involves a rigid, fixed flatfoot deformity. Stage IV involves deltoid ligament incompetence with a rigid flatfoot and ankle valgus tilt.
Question 34:
When treating a rigid idiopathic clubfoot using the Ponseti method of serial casting, what is the correct sequence of deformity correction?
Options:
- Equinus, Varus, Adductus, Cavus
- Cavus, Adductus, Varus, Equinus
- Cavus, Equinus, Varus, Adductus
- Adductus, Varus, Cavus, Equinus
- Varus, Cavus, Adductus, Equinus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method dictates a specific sequence of correction commonly remembered by the acronym CAVE. Cavus is corrected first by elevating the first ray (supinating the forefoot). Then the midfoot Adductus and hindfoot Varus are corrected simultaneously by gradually abducting the foot around the fixed talar head. Equinus is corrected last, often requiring a percutaneous Achilles tenotomy.
Question 35:
In normal articular cartilage, which structural zone contains the largest diameter collagen fibrils oriented perpendicular to the joint surface and provides the highest resistance to compressive forces?
Options:
- Superficial tangential zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage contains the largest diameter collagen fibrils that are oriented perpendicular to the joint surface. This zone also has the highest concentration of proteoglycans and the lowest water content, providing the primary resistance to compressive loads. The superficial zone has collagen parallel to the joint, which primarily resists shear forces.
Question 36:
A 65-year-old male presents with severe, atraumatic mid-back pain. Radiographs reveal a compression fracture of T8. Laboratory workup shows anemia, hypercalcemia, and an elevated creatinine. Serum protein electrophoresis demonstrates a monoclonal spike. Which of the following is the most sensitive and appropriate imaging modality to detect additional osteolytic bone lesions in this patient?
Options:
- Technetium-99m whole-body bone scan
- Whole-body MRI or Low-dose whole-body CT
- Ultrasound
- Dual-energy X-ray absorptiometry (DEXA)
- Gallium-67 scan
Correct Answer: Whole-body MRI or Low-dose whole-body CT
Explanation:
Multiple myeloma lesions are purely lytic and typically do not provoke an osteoblastic response, making traditional Technetium-99m bone scans highly unreliable (high false-negative rate). Whole-body MRI and low-dose whole-body CT (or PET-CT) are much more sensitive for detecting lytic myeloma bone disease and are the current standard of care.
Question 37:
During a total knee arthroplasty in a patient with a severe fixed varus deformity, the medial soft tissues are exceedingly tight in both flexion and extension. After releasing the deep medial collateral ligament (MCL) and removing all medial osteophytes, the joint remains tight medially. What is the next most appropriate sequential step for medial release?
Options:
- Release the lateral collateral ligament
- Release the semimembranosus insertion and posteromedial capsule
- Complete release of the superficial MCL off its distal tibial insertion
- Release the popliteus tendon
- Release the medial head of the gastrocnemius
Correct Answer: Release the semimembranosus insertion and posteromedial capsule
Explanation:
The standard sequence for soft tissue release in a varus knee includes: 1) Removal of medial osteophytes and deep MCL release, 2) Release of the posteromedial corner (semimembranosus and posteromedial capsule) - especially if the knee is tight in extension, 3) Release of the superficial MCL (subperiosteal peeling off the proximal tibia). Releasing the semimembranosus/posteromedial capsule is typically done prior to a complete release of the superficial MCL to avoid over-releasing and causing gross medial instability.
Question 38:
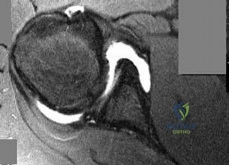
A 24-year-old professional baseball pitcher presents with vague anterior shoulder pain and a 'dead arm' sensation. MR arthrogram reveals a bucket-handle tear of the superior labrum that extends into the long head of the biceps tendon, resulting in an unstable biceps anchor. According to the Snyder classification, what type of SLAP tear is this?
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type IV
Explanation:
The Snyder classification of SLAP (Superior Labrum Anterior to Posterior) tears: Type I is fraying of the superior labrum with an intact biceps anchor. Type II is a detachment of the superior labrum and biceps anchor from the superior glenoid. Type III is a bucket-handle tear of the superior labrum with an intact biceps anchor. Type IV is a bucket-handle tear of the superior labrum that extends into the biceps tendon, resulting in instability of the biceps anchor.
Question 39:
A 62-year-old female underwent volar locked plating for a comminuted distal radius fracture 3 months ago. She now presents with a sudden inability to actively flex the interphalangeal joint of her thumb. Which of the following factors most likely contributed to this complication?
Options:
- Extensor pollicis longus (EPL) attrition from dorsal screw penetration
- Flexor pollicis longus (FPL) rupture secondary to plate prominence at the watershed line
- Iatrogenic transection of the anterior interosseous nerve during exposure
- Flexor digitorum profundus (FDP) rupture from overly long distal screws
- Adhesions of the flexor tendons within the carpal tunnel
Correct Answer: Flexor pollicis longus (FPL) rupture secondary to plate prominence at the watershed line
Explanation:
The patient has experienced a spontaneous rupture of the Flexor Pollicis Longus (FPL) tendon. This is a well-known complication of volar locked plating of distal radius fractures, most commonly caused by placing the plate too far distally so that it extends past the watershed line of the distal radius. The prominent distal edge of the plate causes attritional wear and eventual rupture of the overlying FPL tendon.
Question 40:
A 28-year-old chef sustains a knife laceration over the palmar aspect of his proximal phalanx of the ring finger. Examination reveals an inability to actively flex both the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the ring finger. In which flexor tendon zone did this injury occur?
Options:
- Zone I
- Zone II
- Zone III
- Zone IV
- Zone V
Correct Answer: Zone II
Explanation:
Flexor tendon Zone II, historically known as 'no man's land,' extends from the proximal edge of the A1 pulley (at the metacarpal neck) to the insertion of the Flexor Digitorum Superficialis (FDS) at the middle phalanx. An injury over the palmar aspect of the proximal phalanx occurs within Zone II. Lacerations here typically involve both the FDS and FDP tendons. Zone I is distal to the FDS insertion (FDP only). Zone III is in the palm. Zone IV is within the carpal tunnel.