Full Question & Answer Text (for Search Engines)
Question 1:
A 32-year-old female presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion. Biopsy shows multinucleated giant cells and mononuclear stromal cells. Denosumab therapy is considered. What is the precise mechanism of action of Denosumab?
Options:
- Binds to RANKL, preventing interaction with RANK
- Binds directly to RANK on osteoclasts
- Inhibits osteoprotegerin production
- Inhibits bisphosphonate absorption in the gut
- Directly inhibits vascular endothelial growth factor (VEGF)
Correct Answer: Binds to RANKL, preventing interaction with RANK
Explanation:
Denosumab is a monoclonal antibody that specifically binds to RANKL (Receptor Activator of Nuclear factor Kappa-B Ligand). By binding to RANKL, it prevents it from interacting with the RANK receptor on the surface of osteoclasts and giant cells, thereby profoundly inhibiting osteoclastogenesis and tumor-associated bone lysis in giant cell tumors.
Question 2:
A 6-year-old boy falls on an outstretched hand. Radiographs of the elbow are shown below: On physical examination, the child is unable to flex the interphalangeal joint of the thumb. Which nerve is most likely injured?
Options:
- Ulnar nerve
- Radial nerve
- Anterior interosseous nerve
- Posterior interosseous nerve
- Musculocutaneous nerve
Correct Answer: Anterior interosseous nerve
Explanation:
The inability to flex the interphalangeal joint of the thumb indicates an injury to the flexor pollicis longus (FPL), which is innervated by the Anterior Interosseous Nerve (AIN). AIN neuropraxia is the most common nerve injury associated with extension-type supracondylar humerus fractures.
Question 3:
A 45-year-old male sustains a severe open distal femur fracture. Following debridement, a massive bone defect is treated with the induced membrane (Masquelet) technique. What is the peak time to harvest or graft the induced membrane for optimal vascular endothelial growth factor (VEGF) and bone morphogenetic protein-2 (BMP-2) expression?
Options:
- 2 weeks
- 4 weeks
- 8 weeks
- 12 weeks
- 16 weeks
Correct Answer: 4 weeks
Explanation:
The induced membrane created in the Masquelet technique possesses peak osteogenic and angiogenic properties, including maximum expression of VEGF, BMP-2, and TGF-beta, at approximately 4 weeks. Most surgeons perform the second-stage bone grafting between 4 and 6 weeks to capitalize on this biological peak.
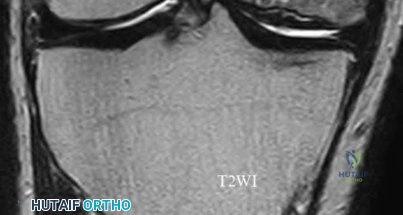
Question 4:
A 55-year-old woman feels a 'pop' in the back of her knee while squatting. An MRI is shown: A posterior horn medial meniscus root tear is identified. Biomechanically, a complete medial meniscus posterior root tear alters contact pressures to a degree equivalent to which of the following?
Options:
- Total meniscectomy
- Partial meniscectomy
- Anterior cruciate ligament tear
- Posterior cruciate ligament tear
- Medial collateral ligament tear
Correct Answer: Total meniscectomy
Explanation:
A complete posterior root tear of the medial meniscus leads to a complete loss of hoop stresses, resulting in meniscal extrusion. Biomechanically, this alters peak tibiofemoral contact pressures and reduces contact area to a degree equivalent to a total meniscectomy, leading to rapid articular cartilage degeneration.
Question 5:
A 68-year-old male presents with deteriorating handwriting, frequent falls, and numbness in his hands. A sagittal T2 MRI is shown: He demonstrates a positive Hoffman sign. Which physical examination finding corresponds to the loss of proprioception in the dorsal columns commonly seen in this condition?
Options:
- Lhermitte's sign
- Positive Romberg test
- Sustained clonus
- Inverted radial reflex
- Babinski sign
Correct Answer: Positive Romberg test
Explanation:
Cervical spondylotic myelopathy affects various spinal tracts. Involvement of the dorsal columns leads to loss of proprioception, resulting in a wide-based gait and a positive Romberg test. Corticospinal tract involvement leads to upper motor neuron signs like hyperreflexia, clonus, Babinski sign, and Hoffman sign.
Question 6:
In designing a cementless femoral stem for a total hip arthroplasty, the manufacturer utilizes a porous coating. What pore size range is optimal for reliable biological bone ingrowth?
Options:
- 10-50 micrometers
- 50-400 micrometers
- 400-800 micrometers
- 800-1200 micrometers
- >1200 micrometers
Correct Answer: 50-400 micrometers
Explanation:
The optimal pore size for biological bone ingrowth in cementless arthroplasty implants is generally between 50 and 400 micrometers. Pores smaller than 50 µm are too small for osteons and lead predominantly to fibrous tissue ingrowth, whereas pores larger than 400 µm decrease the structural integrity of the coating and increase the risk of micromotion.
Question 7:
A 54-year-old male with long-standing diabetes presents with a swollen, warm, and erythematous left foot. Radiographs reveal fragmentation and periarticular debris at the tarsometatarsal joints. Which classification system is commonly used to stage the anatomical location of this disease process?
Options:
- Eichenholtz classification
- Brodsky classification
- Sanders classification
- Tscherne classification
- Hardinge classification
Correct Answer: Brodsky classification
Explanation:
The Brodsky classification describes the anatomic location of Charcot arthropathy. Type 1 is the tarsometatarsal (Lisfranc) joint, which is the most common. Type 2 involves the Chopart/subtalar joints. Type 3A involves the ankle (tibiotalar), and Type 3B involves the calcaneal tuberosity. The Eichenholtz classification describes the clinical and radiographic progression (development, coalescence, consolidation).
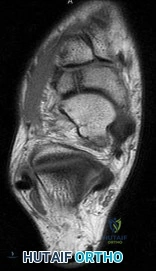
Question 8:
A 24-year-old male falls on an extended wrist. Radiographs are shown: In Mayfield's progressive stages of perilunate instability, what is the final ligamentous structure to fail, resulting in a true lunate dislocation (Stage IV)?
Options:
- Scapholunate interosseous ligament
- Lunotriquetral interosseous ligament
- Dorsal radiocarpal ligament
- Radioscaphocapitate ligament
- Dorsal radiolunate ligament
Correct Answer: Dorsal radiolunate ligament
Explanation:
According to Mayfield's progressive stages of perilunate instability: Stage I involves the scapholunate ligament; Stage II involves the space of Poirier (capitolunate failure); Stage III involves the lunotriquetral ligament (perilunate dislocation); Stage IV involves failure of the dorsal radiolunate ligament, allowing the lunate to dislocate volarly into the carpal tunnel.
Question 9:
When analyzing the mechanical properties of an orthopedic plate, the area under the stress-strain curve up to the point of failure represents which of the following material properties?
Options:
- Elastic modulus
- Yield strength
- Ultimate tensile strength
- Toughness
- Ductility
Correct Answer: Toughness
Explanation:
Toughness is defined as the amount of energy a material can absorb before it fractures, which is graphically represented by the total area under the stress-strain curve. Elastic modulus is the slope of the linear elastic region. Yield strength is the stress at which plastic deformation begins.
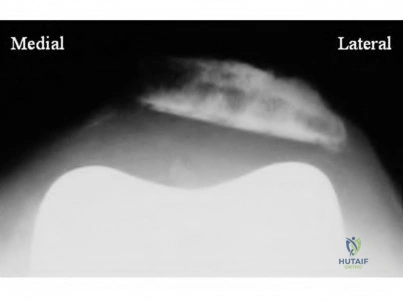
Question 10:
A 15-year-old boy presents with knee pain. Imaging reveals a destructive metaphyseal lesion of the distal femur with a sunburst periosteal reaction. Staging shows no metastasis. Following neoadjuvant chemotherapy and wide surgical resection, what is the most significant prognostic factor for overall survival?
Options:
- Tumor size at presentation
- Serum alkaline phosphatase levels
- Percentage of tumor necrosis on histologic map
- Type of surgical reconstruction performed
- Distance of the tumor from the joint line
Correct Answer: Percentage of tumor necrosis on histologic map
Explanation:
In osteosarcoma, the histologic response to neoadjuvant chemotherapy, measured as the percentage of tumor necrosis in the resected specimen, is the most powerful predictor of disease-free and overall survival. A good response is typically defined as greater than 90% tumor necrosis.
Question 11:
A 30-year-old male is involved in a motorcycle collision. Radiographs demonstrate a displaced symphysis pubis (3.5 cm) and widening of the left sacroiliac joint. He remains hypotensive despite 2 liters of crystalloid and 2 units of packed RBCs. A pelvic binder was properly placed in the field. What is the most appropriate next step in management?
Options:
- CT scan of the abdomen and pelvis
- Open reduction and internal fixation of the symphysis pubis
- Pre-peritoneal pelvic packing and/or angioembolization
- Application of an external fixator
- Exploratory laparotomy
Correct Answer: Pre-peritoneal pelvic packing and/or angioembolization
Explanation:
In a hemodynamically unstable patient with a pelvic ring injury, despite initial resuscitation and mechanical stabilization (pelvic binder), the immediate priority is hemorrhage control. This is best achieved via pre-peritoneal pelvic packing or angioembolization, depending on institutional protocol. CT is contraindicated in hemodynamically unstable patients.
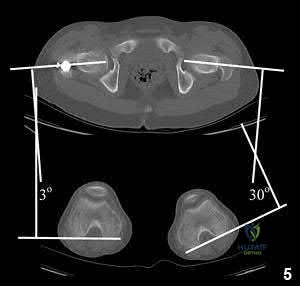
Question 12:
A 13-year-old obese male complains of left knee pain and a limp for 3 weeks. Radiographs are provided: He is able to bear weight with crutches. During physical examination, as the affected hip is passively flexed, into which position will the limb obligately deviate?
Options:
- Internal rotation
- External rotation
- Adduction
- Extension
- Abduction
Correct Answer: External rotation
Explanation:
In slipped capital femoral epiphysis (SCFE), the proximal femoral epiphysis displaces posteriorly and inferiorly relative to the femoral neck. This altered anatomy leads to an obligate external rotation of the thigh during passive hip flexion, a classic physical examination finding.
Question 13:
During a total knee arthroplasty (TKA), the surgeon aims to optimize patellofemoral tracking. Which of the following femoral component positioning errors is most likely to cause patellar maltracking and lateral subluxation?
Options:
- Excessive external rotation of the femoral component
- Internal rotation of the femoral component
- Anterior referencing instead of posterior referencing
- Joint line elevation
- Excessive valgus of the tibial component
Correct Answer: Internal rotation of the femoral component
Explanation:
Internal rotation of the femoral component effectively moves the trochlear groove medially relative to the mechanical axis. This increases the Q-angle, leading to lateral patellar maltracking and a higher risk of lateral patellar subluxation or dislocation.
Question 14:
A 40-year-old mechanic complains of lateral forearm pain that worsens with resisted forearm pronation and supination. There is no demonstrable motor weakness. He has local tenderness approximately 4 cm distal to the lateral epicondyle. Injection of local anesthetic provides temporary relief. The nerve involved is most likely compressed by which of the following structures?
Options:
- Ligament of Struthers
- Lacertus fibrosus
- Arcade of Frohse
- Osborne's fascia
- Arcade of Struthers
Correct Answer: Arcade of Frohse
Explanation:
This clinical presentation is characteristic of Radial Tunnel Syndrome (pain predominantly, without motor weakness, as opposed to PIN syndrome). The most common site of compression of the deep branch of the radial nerve / posterior interosseous nerve (PIN) in this region is the Arcade of Frohse, the proximal fibrous edge of the superficial head of the supinator muscle.
Question 15:
A 21-year-old college football player experiences recurrent anterior shoulder dislocations. Imaging demonstrates a bony Bankart lesion involving 25% of the anterior glenoid width and an engaging Hill-Sachs lesion. Which procedure is most appropriate to stabilize this shoulder and prevent recurrence?
Options:
- Arthroscopic soft-tissue Bankart repair
- Arthroscopic Bankart repair with Remplissage
- Latarjet procedure
- Putti-Platt procedure
- Weaver-Dunn procedure
Correct Answer: Latarjet procedure
Explanation:
For high-demand contact athletes with critical anterior glenoid bone loss (typically >20-25%) or bipolar bone loss with an engaging Hill-Sachs lesion, isolated arthroscopic soft-tissue repair has an unacceptably high failure rate. A bony augmentation procedure, such as the Latarjet (coracoid transfer), is indicated to restore the glenoid articular arc and provide a sling effect.
Question 16:
An 82-year-old female presents after a fall at home. Imaging is shown: She is diagnosed with an unstable intertrochanteric femur fracture. Which of the following anatomic patterns defines an unstable intertrochanteric fracture?
Options:
- Two-part fracture with a non-displaced lesser trochanter
- Intact posteromedial calcar cortex
- Reverse obliquity pattern
- Fracture line extending proximal to the vastus ridge
- Non-displaced transcervical extension
Correct Answer: Reverse obliquity pattern
Explanation:
Unstable intertrochanteric fracture patterns inherently resist stable reduction and include: reverse obliquity fractures, subtrochanteric extension, large posteromedial comminution (loss of the calcar support), and lateral wall blowout. An intact posteromedial cortex or simple two-part fractures are generally considered stable.
Question 17:
Rivaroxaban is a medication commonly prescribed for deep vein thrombosis prophylaxis following total joint arthroplasty. What is its specific mechanism of action in the coagulation cascade?
Options:
- Inhibits antithrombin III
- Direct thrombin (Factor IIa) inhibitor
- Direct Factor Xa inhibitor
- Vitamin K epoxide reductase inhibitor
- Enhances tissue plasminogen activator
Correct Answer: Direct Factor Xa inhibitor
Explanation:
Rivaroxaban and Apixaban are Direct Oral Anticoagulants (DOACs) that specifically and reversibly inhibit Factor Xa. Dabigatran is a direct thrombin (Factor IIa) inhibitor. Warfarin acts by inhibiting vitamin K epoxide reductase.
Question 18:
A 38-year-old male sustains an acute Achilles tendon rupture while playing basketball. He opts for non-operative management with a functional rehabilitation protocol. Based on recent Level I evidence, compared to operative repair, non-operative management utilizing early functional bracing is associated with which of the following?
Options:
- Lower rate of deep vein thrombosis
- Higher rate of wound complications
- Equivalent re-rupture rate
- Significantly higher re-rupture rate
- Increased sural nerve injury rate
Correct Answer: Equivalent re-rupture rate
Explanation:
Recent high-quality level I evidence (such as the Willits study) has demonstrated that when an early functional rehabilitation protocol (early weight-bearing in a functional brace) is utilized, the re-rupture rate of non-operative management is equivalent to that of operative repair, while completely avoiding surgical risks such as wound breakdown and sural nerve injury.
Question 19:
A 14-year-old gymnast presents with chronic, mechanically reproducible low back pain. Radiographs reveal a pars interarticularis defect at L5 with a 30% anterior translation of L5 on S1. According to the Meyerding classification, what grade is this spondylolisthesis, and what is the primary initial management?
Options:
- Grade I; physical therapy and core strengthening
- Grade II; physical therapy and core strengthening
- Grade II; immediate posterior spinal fusion
- Grade III; TLSO brace for 6 months
- Grade III; primary pars repair
Correct Answer: Grade II; physical therapy and core strengthening
Explanation:
The Meyerding classification grades the magnitude of slip based on the superior endplate of the vertebra below. Grade I: 0-25%, Grade II: 26-50%, Grade III: 51-75%, Grade IV: 76-100%, Grade V: >100% (spondyloptosis). A 30% slip is Grade II. The initial management for low-grade (I and II) isthmic spondylolisthesis without progressive neurologic deficit is non-operative, emphasizing activity modification, hamstring stretching, and core stabilization.
Question 20:
A 6-week-old female infant is evaluated for clicking in her hips. An ultrasound is performed to evaluate for Developmental Dysplasia of the Hip (DDH). What alpha angle is considered normal for a mature, appropriately formed hip on a coronal ultrasound view according to Graf's classification?
Options:
- >40 degrees
- >50 degrees
- >60 degrees
- <60 degrees
- <50 degrees
Correct Answer: >60 degrees
Explanation:
According to Graf's classification of infant hip ultrasound, an alpha angle (measuring the bony roof of the acetabulum) of greater than 60 degrees is considered normal (Type I hip). An alpha angle between 50 and 59 degrees is physiologic immaturity (Type IIa) if the infant is <3 months old, and an angle less than 50 indicates dysplasia.