Full Question & Answer Text (for Search Engines)
Question 1:
A 12-year-old obese boy presents with vague left thigh and knee pain. He is diagnosed with a Slipped Capital Femoral Epiphysis (SCFE) as seen in similar clinical scenarios. During percutaneous in-situ fixation, unrecognized penetration of the guide wire into the hip joint occurs. What is the most likely specific complication resulting from this technical error?
Options:
- Chondrolysis
- Avascular necrosis
- Osteomyelitis
- Slipped progression
- Heterotopic ossification
Correct Answer: Chondrolysis
Explanation:
Chondrolysis is a severe complication of SCFE characterized by rapid destruction of the articular cartilage. While it can occur idiopathically, its most established iatrogenic cause is unrecognized intra-articular hardware penetration. The 'approach-withdraw' fluoroscopic technique is required during pinning to assure pins are entirely intraosseous. Avascular necrosis (AVN) is usually due to damage to the epiphyseal blood supply (retinacular vessels) secondary to the initial displacement, forceful closed reduction, or posterosuperior pin placement.
Question 2:
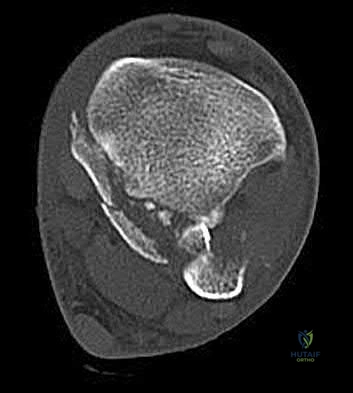
A 28-year-old male sustains a severe hyper-dorsiflexion injury to his ankle in a motor vehicle accident, resulting in a Hawkins Type III talar neck fracture. Which of the following arteries provides the predominant blood supply to the body of the talus, placing it at significant risk for avascular necrosis in this injury?
Options:
- Artery of the sinus tarsi
- Anterior tibial artery
- Dorsalis pedis
- Artery of the tarsal canal
- Peroneal artery
Correct Answer: Artery of the tarsal canal
Explanation:
The artery of the tarsal canal, which is a branch of the posterior tibial artery, provides the dominant blood supply to the talar body. In a Hawkins Type III fracture (talar neck fracture with subtalar and tibiotalar dislocation), the blood supply from the artery of the tarsal canal, the artery of the sinus tarsi, and capsular vessels are disrupted, leading to an avascular necrosis (AVN) rate approaching 100%.
Question 3:
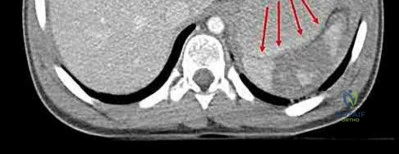
A 15-year-old boy presents with a permeative lytic lesion in the femoral diaphysis with aggressive periosteal reaction ('onion skinning'). Biopsy reveals uniform small round blue cells. Cytogenetic analysis of this tumor will most likely demonstrate which of the following translocations?
Options:
- t(11;22)
- t(9;22)
- t(2;13)
- t(X;18)
- t(12;16)
Correct Answer: t(11;22)
Explanation:
The clinical and radiographic description is classic for Ewing sarcoma. The characteristic cytogenetic abnormality is a balanced translocation t(11;22)(q24;q12), which fuses the EWS gene on chromosome 22 with the FLI1 gene on chromosome 11. This is seen in approximately 85-90% of Ewing sarcomas. t(9;22) is the Philadelphia chromosome (CML), t(X;18) is seen in synovial sarcoma, t(2;13) in alveolar rhabdomyosarcoma, and t(12;16) in myxoid liposarcoma.
Question 4:
During anterior cruciate ligament (ACL) reconstruction, an allograft is tensioned prior to final fixation. Over time, the graft experiences a gradual increase in deformation despite being held under a constant applied load. What biomechanical property does this describe?
Options:
- Creep
- Stress relaxation
- Hysteresis
- Fatigue
- Anisotropy
Correct Answer: Creep
Explanation:
Creep is the viscoelastic property defined as the progressive deformation of a material over time when subjected to a constant load. Stress relaxation is the decrease in stress over time when a material is held at a constant strain/deformation. Hysteresis represents the energy lost (as heat) during the loading and unloading cycles of a viscoelastic material. Anisotropy means a material's physical properties depend on the direction of applied load.
Question 5:
A 45-year-old male is involved in a high-speed motor vehicle collision and presents with the cervical spine radiograph findings typical of traumatic spondylolisthesis of the axis. Which of the following describes the primary mechanism of injury for this specific fracture pattern (Hangman's fracture)?
Options:
- Flexion and distraction
- Hyperextension and axial loading
- Lateral bending
- Axial rotation
- Flexion and compression
Correct Answer: Hyperextension and axial loading
Explanation:
A 'Hangman's fracture' is a traumatic spondylolisthesis of the axis (C2) involving fractures through the pars interarticularis. The classical mechanism of injury in modern trauma (e.g., unrestrained passenger hitting the windshield) is hyperextension and axial loading. Flexion-distraction typically causes Chance fractures, while flexion-compression typically causes anterior wedge or teardrop fractures.
Question 6:
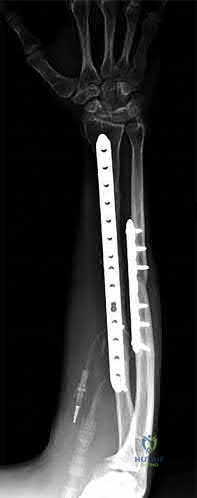
A 22-year-old male falls onto an outstretched hand and sustains a displaced fracture through the proximal pole of the scaphoid. Avascular necrosis of the proximal pole is highly likely due to the disruption of its primary vascular supply. Which vessel provides this critical retrograde perfusion?
Options:
- Superficial palmar branch of the radial artery
- Dorsal carpal branch of the radial artery
- Volar carpal branch of the ulnar artery
- Anterior interosseous artery
- Deep palmar arch
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The primary blood supply to the scaphoid is from the dorsal carpal branch of the radial artery, which enters the dorsal ridge of the scaphoid at the waist and courses proximally. This retrograde blood flow makes proximal pole fractures highly susceptible to avascular necrosis and nonunion. The superficial palmar branch provides a minor supply (about 20%) to the distal pole.
Question 7:
A 55-year-old active female undergoes a primary total hip arthroplasty. The surgeon opts for a ceramic-on-ceramic bearing surface to maximize longevity. Which of the following complications is uniquely associated with this specific bearing couple compared to metal-on-polyethylene?
Options:
- Trunnionosis
- Squeaking
- Galvanic corrosion
- Accelerated osteolysis from submicron particles
- Pseudotumor formation
Correct Answer: Squeaking
Explanation:
Squeaking is an audible complication unique to hard-on-hard bearings, specifically ceramic-on-ceramic (CoC) total hip arthroplasties. It occurs in up to 10% of CoC THAs and may be related to component malposition, edge loading, or microseparation. Trunnionosis and galvanic corrosion are associated with modular junctions (like a metal head on a metal stem). Pseudotumors are classically linked to metal-on-metal bearings.
Question 8:
According to Perren's strain theory of bone healing, primary bone healing (osteonal reconstruction without callus formation) can only occur under conditions of absolute stability. What is the maximum interfragmentary strain tolerated for primary bone healing to occur?
Options:
- < 2%
- 2 - 10%
- 10 - 30%
- 30 - 50%
- > 50%
Correct Answer: < 2%
Explanation:
Perren's strain theory states that the type of tissue that forms in a fracture gap is dictated by the mechanical strain. Primary bone healing requires absolute stability, meaning the interfragmentary strain must be less than 2%. Strains between 2% and 10% allow for secondary bone healing (callus formation), typically seen with relative stability (e.g., intramedullary nailing or bridge plating). Granulation tissue tolerates up to 100% strain.
Question 9:
A 30-year-old male sustains a severe midfoot sprain. Radiographs reveal widening between the bases of the first and second metatarsals. The primary ligamentous stabilizer disrupted in this classic Lisfranc injury connects which two osseous structures?
Options:
- Medial cuneiform to 1st metatarsal base
- Medial cuneiform to 2nd metatarsal base
- Middle cuneiform to 2nd metatarsal base
- Lateral cuneiform to 3rd metatarsal base
- Navicular to medial cuneiform
Correct Answer: Medial cuneiform to 2nd metatarsal base
Explanation:
The Lisfranc ligament is the strongest ligament in the tarsometatarsal joint complex. It courses obliquely from the lateral aspect of the medial cuneiform to the medial base of the second metatarsal. It acts as the primary stabilizer of the second metatarsal base. Disruption results in the classic widening between the first and second rays, often with an avulsion fragment ('fleck sign').
Question 10:
A 6-week-old female is diagnosed with developmental dysplasia of the hip (DDH) and placed in a Pavlik harness. During a follow-up visit, it is noted that the anterior straps are overly tightened, causing hyperflexion of the hips. Which of the following nerve palsies is most commonly associated with this specific positioning error?
Options:
- Sciatic nerve
- Femoral nerve
- Obturator nerve
- Superior gluteal nerve
- Lateral femoral cutaneous nerve
Correct Answer: Femoral nerve
Explanation:
In a Pavlik harness, excessive flexion (over-tightening of the anterior straps) can compress the femoral nerve against the inguinal ligament, leading to a transient femoral nerve palsy (manifesting as decreased quadriceps function). Conversely, excessive abduction (over-tightening of the posterior straps) places the hip at significant risk for avascular necrosis (AVN) of the femoral head.
Question 11:
A poly-trauma patient presents hemodynamically unstable with an anteroposterior compression (APC-III) pelvic ring injury. A circumferential pelvic binder is requested to reduce pelvic volume and control hemorrhage. To be anatomically effective, the binder must be centered precisely over which of the following landmarks?
Options:
- Iliac crests
- Anterior superior iliac spines
- Greater trochanters
- Ischial tuberosities
- Symphysis pubis
Correct Answer: Greater trochanters
Explanation:
For optimal mechanical advantage and effective reduction of an 'open book' pelvic fracture (APC type), a pelvic binder must be applied directly over the greater trochanters of the femurs. Applying it higher, such as over the iliac crests, is a common error that fails to adequately close the pelvic ring and can paradoxically open the true pelvis.
Question 12:
A 55-year-old patient presents with a slowly enlarging, painful mass in the proximal humerus. Biopsy reveals a hyaline cartilage matrix with cellular atypia, confirming a diagnosis of central conventional chondrosarcoma. Which of the following genetic mutations is most frequently identified in this specific tumor?
Options:
- EXT1 / EXT2
- IDH1 / IDH2
- GNAS
- TP53 / RB1
- RUNX2
Correct Answer: IDH1 / IDH2
Explanation:
Mutations in the isocitrate dehydrogenase genes, IDH1 and IDH2, are found in up to 50-60% of central conventional chondrosarcomas and enchondromas. EXT1 and EXT2 mutations are characteristic of multiple hereditary exostoses (osteochondromas). GNAS mutations are seen in fibrous dysplasia. TP53 and RB1 mutations are hallmark aberrations in osteosarcoma.
Question 13:
A 40-year-old diabetic male presents with a swollen, painful right index finger after a puncture wound. You suspect pyogenic flexor tenosynovitis. Kanavel's classical cardinal signs for this condition include all of the following EXCEPT:
Options:
- Fusiform swelling of the entire digit
- Pain with passive extension of the digit
- Flexed resting posture of the digit
- Erythema extending proximally into the mid-palm
- Tenderness to palpation along the flexor tendon sheath
Correct Answer: Erythema extending proximally into the mid-palm
Explanation:
Kanavel's four cardinal signs of flexor tenosynovitis are: 1) fusiform (sausage-like) swelling of the digit, 2) severe pain with passive extension, 3) a flexed resting posture of the digit, and 4) tenderness along the entire course of the flexor tendon sheath. Erythema extending to the mid-palm is not one of Kanavel's specific signs, though localized erythema may be present.
Question 14:
A 65-year-old male presents with deteriorating handwriting, dropping objects, and an unsteady, broad-based gait. On physical examination, flicking the volar nail of the middle finger results in an involuntary flexion reflex of the thumb and index finger. What is the name of this sign and its corresponding pathology?
Options:
- Wartenberg's sign - Ulnar neuropathy
- Hoffman's reflex - Cervical myelopathy
- Babinski reflex - Upper motor neuron lesion
- Lhermitte's sign - Multiple sclerosis
- Froment's sign - Anterior interosseous nerve syndrome
Correct Answer: Hoffman's reflex - Cervical myelopathy
Explanation:
The Hoffman's reflex is elicited by flicking the nail of the middle finger; a positive response is flexion of the IP joint of the thumb and index finger. It indicates an upper motor neuron lesion, classically cervical spondylotic myelopathy. Wartenberg's sign is the abducted posture of the small finger due to ulnar neuropathy. Lhermitte's sign is shock-like sensations down the spine with neck flexion. Froment's sign tests for ulnar nerve palsy (adductor pollicis weakness).
Question 15:
Following a traumatic knee injury, a 24-year-old athlete undergoes an arthroscopic meniscal repair. Which zone of the meniscus has the highest healing potential, and from which vessels does it derive its primary blood supply?
Options:
- Red-red zone; middle geniculate artery
- Red-red zone; medial and lateral superior/inferior geniculate arteries
- White-white zone; popliteal artery
- Red-white zone; descending genicular artery
- White-white zone; avascular (relies on synovial fluid)
Correct Answer: Red-red zone; medial and lateral superior/inferior geniculate arteries
Explanation:
The peripheral 10% to 30% of the meniscus (the red-red zone) is well-vascularized and thus has the highest healing potential. The blood supply to this peripheral zone is derived from the capsular and synovial branches of the medial and lateral, superior and inferior geniculate arteries. The central white-white zone is avascular and relies on diffusion from synovial fluid, lacking the intrinsic capacity to heal.
Question 16:
During a posterior-stabilized total knee arthroplasty, the surgeon evaluates the gaps using trial components. The assessment demonstrates that the extension gap is perfectly balanced and rectangular, but the flexion gap is excessively tight. What is the most appropriate isolated next step to balance the knee?
Options:
- Release the posterior capsule
- Resect more distal femur
- Downsize the femoral component
- Resect more proximal tibia
- Upsize the femoral component
Correct Answer: Downsize the femoral component
Explanation:
If the flexion gap is tight but the extension gap is balanced, the surgeon must alter the flexion gap without affecting the extension space. Downsizing the femoral component (using the same posterior referencing guide, or using an anterior referencing system) translates the posterior condylar surface anteriorly, effectively increasing the flexion space while leaving the distal femoral resection (extension gap) unchanged.
Question 17:
Articular cartilage is structurally organized into four distinct zones. Which zone contains the highest concentration of proteoglycans, the lowest concentration of water, and collagen fibers oriented perpendicularly to the articular surface?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified cartilage zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage is characterized by collagen fibers aligned perpendicular to the joint surface (providing resistance to compressive forces), the highest concentration of proteoglycans, and the lowest water content. The superficial zone has the highest water content, parallel collagen fibers to resist shear, and lowest proteoglycan content. The tidemark separates the deep zone from the calcified zone.
Question 18:
A 60-year-old diabetic patient presents with a warm, swollen, erythematous foot. Radiographs reveal fragmentation of bone, periarticular debris, subluxation, and joint dislocation. There is no active consolidation. Which stage of the Eichenholtz classification for Charcot arthropathy does this represent?
Options:
- Stage 0 (Prodromal)
- Stage I (Developmental/Fragmentation)
- Stage II (Coalescence)
- Stage III (Consolidation)
- Stage IV (Remodeling)
Correct Answer: Stage I (Developmental/Fragmentation)
Explanation:
The Eichenholtz classification describes the natural history of Charcot neuroarthropathy. Stage I (Developmental/Fragmentation) is characterized by acute inflammation, osteopenia, joint subluxation/dislocation, bone fragmentation, and intra-articular debris. Stage II (Coalescence) shows decreased inflammation and early absorption of debris. Stage III (Consolidation) shows remodeling and robust bony fusion. Stage 0 was later added (Shibata) to denote the acute inflammatory phase prior to radiographic fragmentation.
Question 19:
A 28-year-old male sustains a closed comminuted tibial shaft fracture. Two hours post-injury, he develops severe leg pain unyielding to narcotics. His blood pressure is 120/80 mmHg. Intracompartmental pressure monitoring is performed. Based on current guidelines, which measurement dictates an emergent 4-compartment fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Absolute compartment pressure > 25 mmHg
- Delta pressure (Diastolic BP - Compartment Pressure) < 30 mmHg
- Delta pressure (Systolic BP - Compartment Pressure) < 30 mmHg
- Delta pressure (Mean Arterial Pressure - Compartment Pressure) < 40 mmHg
Correct Answer: Delta pressure (Diastolic BP - Compartment Pressure) < 30 mmHg
Explanation:
Acute compartment syndrome is classically defined by tissue hypoperfusion. The absolute compartment pressure is less reliable than the differential pressure (Delta P). A Delta P (Diastolic Blood Pressure minus Compartment Pressure) of less than 30 mmHg is an absolute indication for emergency fasciotomy, as capillary perfusion gradient is lost when tissue pressure approaches the diastolic pressure.
Question 20:
A 3-year-old girl is evaluated for severe, progressive bilateral genu varum. Radiographs demonstrate medial metaphyseal beaking, fragmentation, and depression of the proximal medial tibial physis. According to the Langenskiöld classification of infantile Blount's disease, at which stage does an overt physeal bony bar (epiphyseal-metaphyseal bridge) definitively form across the medial physis, conferring a high risk of recurrence without bar excision?
Options:
- Stage II
- Stage III
- Stage IV
- Stage V
- Stage VI
Correct Answer: Stage VI
Explanation:
The Langenskiöld classification describes progressive radiographic changes in infantile Blount disease. Stage I-IV show worsening metaphyseal beaking and stepping. Stage V shows a deep cleft separating the medial epiphysis into two portions. Stage VI is definitively characterized by the formation of a solid medial physeal bridge (bony bar) between the epiphysis and metaphysis, halting medial growth completely and often requiring bar resection along with osteotomy.