Full Question & Answer Text (for Search Engines)
Question 1:
A 6-year-old child falls onto an outstretched hand resulting in the injury shown. Which nerve is most commonly injured in extension-type supracondylar humerus fractures with posteromedial displacement of the distal fragment?
Options:
- Anterior interosseous nerve (AIN)
- Ulnar nerve
- Radial nerve
- Musculocutaneous nerve
- Axillary nerve
Correct Answer: Radial nerve
Explanation:
In extension-type supracondylar fractures, the distal fragment displaces posteriorly. If it displaces posteromedially, the proximal fragment's sharp metaphysis is driven anterolaterally, thereby placing the radial nerve at the highest risk of injury. Conversely, posterolateral displacement of the distal fragment drives the proximal spike anteromedially, putting the median nerve (specifically the AIN) and brachial artery at risk.
Question 2:
A 45-year-old man is involved in a high-speed motor vehicle collision. The AP pelvis radiograph demonstrates an acetabular fracture. According to the Letournel classification, which of the following radiographic lines is typically disrupted in an isolated transverse acetabular fracture?
Options:
- Iliopectineal line only
- Ilioischial line only
- Both the iliopectineal and ilioischial lines
- Radiographic teardrop only
- Anterior wall line only
Correct Answer: Both the iliopectineal and ilioischial lines
Explanation:
A transverse acetabular fracture is an elementary fracture pattern that involves a single fracture line crossing the acetabulum horizontally. Because it bisects both the anterior and posterior columns of the acetabulum, it disrupts both the iliopectineal line (anterior column marker) and the ilioischial line (posterior column marker) on a standard AP pelvis radiograph.
Question 3:
A 32-year-old woman presents with persistent knee pain. Imaging reveals an eccentric, lytic epiphyseal lesion extending to the subchondral bone, characteristic of a giant cell tumor of bone. She is prescribed denosumab prior to surgical intervention. What is the precise mechanism of action of this medication?
Options:
- Inhibits osteoclast ruffled border proton pumps
- Binds to RANK ligand (RANKL) preventing its interaction with the RANK receptor
- Binds to the RANK receptor preventing osteoclast differentiation
- Induces direct apoptosis of neoplastic osteoblasts
- Neutralizes parathyroid hormone-related peptide (PTHrP)
Correct Answer: Binds to RANK ligand (RANKL) preventing its interaction with the RANK receptor
Explanation:
Denosumab is a human monoclonal antibody that binds specifically to RANKL (Receptor Activator of Nuclear factor Kappa-B Ligand), a protein essential for the formation, function, and survival of osteoclasts. By neutralizing RANKL, denosumab prevents it from binding to the RANK receptor on osteoclast precursors, dramatically decreasing osteoclast-mediated bone destruction, which is the primary pathology in Giant Cell Tumor of Bone.
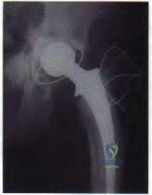
Question 4:
You are reviewing the wear characteristics of total hip arthroplasty (THA) bearing surfaces. The introduction of highly cross-linked polyethylene (HXLPE) has significantly reduced volumetric wear rates. Which of the following processing steps in HXLPE manufacturing is directly responsible for a decrease in the material's fracture toughness?
Options:
- Electron beam irradiation
- Vitamin E infusion
- Post-irradiation remelting
- Gamma sterilization in an inert gas
- Addition of calcium stearate
Correct Answer: Post-irradiation remelting
Explanation:
Highly cross-linked polyethylene requires irradiation to form cross-links (which improves wear resistance) but this process generates free radicals. To prevent oxidation, the material undergoes thermal processing. Post-irradiation remelting (heating above the melting point) effectively eliminates free radicals but significantly decreases the material's crystallinity, which compromises its ultimate tensile strength, fatigue strength, and fracture toughness. Annealing or utilizing Vitamin E are alternatives to preserve mechanical properties.
Question 5:
A 65-year-old man presents with progressive clumsiness in his hands, difficulty buttoning his shirt, and a broad-based gait. Examination reveals a positive Hoffman's sign and inverted brachioradialis reflex. Which of the following physical exam findings is most highly specific for diagnosing cervical myelopathy?
Options:
- Positive Spurling test
- Hyperreflexia in the bilateral Achilles tendons
- Positive Babinski sign
- Ankle clonus
- Finger escape sign (Wartenberg's sign of the hand)
Correct Answer: Finger escape sign (Wartenberg's sign of the hand)
Explanation:
The finger escape sign (inability to hold the ulnar digits in adduction and extension due to intrinsic weakness and altered tone) is highly specific for cervical myelopathy. While hyperreflexia, Babinski sign, and clonus are classic upper motor neuron signs associated with myelopathy, they are less specific than the finger escape sign in localizing cervical cord compression. The Spurling test evaluates for cervical radiculopathy, not myelopathy.
Question 6:
A 28-year-old carpenter sustains a sharp knife laceration to the volar aspect of his index finger at the level of the proximal phalanx. He is unable to flex the DIP and PIP joints. Which zone of flexor tendon injury does this represent, and what is its anatomic definition?
Options:
- Zone I; insertion of FDS to the insertion of FDP
- Zone II; from the distal palmar crease (A1 pulley) to the mid-middle phalanx (FDS insertion)
- Zone III; lumbrical origin in the palm
- Zone IV; within the carpal tunnel
- Zone V; proximal to the carpal tunnel
Correct Answer: Zone II; from the distal palmar crease (A1 pulley) to the mid-middle phalanx (FDS insertion)
Explanation:
Zone II flexor tendon injuries occur between the distal palmar crease (the proximal edge of the A1 pulley) and the insertion of the flexor digitorum superficialis (FDS) on the middle phalanx. Historically termed 'no man\'s land' by Bunnell, this zone contains both the FDS and FDP tendons tightly enclosed within the flexor tendon sheath, making repair prone to adhesions.
Question 7:
During a primary anterior cruciate ligament (ACL) reconstruction, the surgeon is carefully determining femoral tunnel placement. Placing the femoral tunnel too anteriorly (shallow) relative to the anatomic footprint will result in which of the following kinematic abnormalities of the graft?
Options:
- Laxity in flexion and tightness in extension
- Tightness in flexion and laxity in extension
- Equal tension throughout the full range of motion
- Impingement against the PCL in extension
- Isolated rotatory instability with a normal Lachman test
Correct Answer: Tightness in flexion and laxity in extension
Explanation:
Anterior placement of the femoral tunnel (too shallow in the notch) brings the femoral attachment of the ACL graft anterior to the knee's axis of rotation. During knee flexion, the distance between the tibial and femoral tunnels increases, causing the graft to become exceedingly tight in flexion, limiting motion or leading to graft failure. Conversely, the graft will be loose in extension.
Question 8:
A 24-year-old football player sustains a high-energy hyperplantarflexion injury to his midfoot. Weight-bearing radiographs suggest a subtle Lisfranc injury. Which of the following anatomic descriptions accurately characterizes the primary strong band of the Lisfranc ligament complex?
Options:
- It connects the medial cuneiform to the base of the first metatarsal
- It connects the medial cuneiform to the base of the second metatarsal
- It connects the middle cuneiform to the base of the second metatarsal
- It connects the lateral cuneiform to the base of the third metatarsal
- It connects the cuboid to the base of the fourth metatarsal
Correct Answer: It connects the medial cuneiform to the base of the second metatarsal
Explanation:
The Lisfranc ligament is an oblique, interosseous ligament that originates on the lateral aspect of the medial cuneiform and inserts on the medial aspect of the base of the second metatarsal. It is critical for midfoot stability because there is no direct intermetatarsal ligamentous connection between the bases of the first and second metatarsals.
Question 9:
Bone morphogenetic proteins (BMPs) play a crucial role in clinical osteoinduction by promoting the differentiation of mesenchymal stem cells into osteoblasts. Which intracellular signaling pathway is primarily activated immediately following BMP receptor binding?
Options:
- Wnt/beta-catenin pathway
- JAK/STAT pathway
- Smad 1/5/8 pathway
- MAPK/ERK pathway
- Notch signaling pathway
Correct Answer: Smad 1/5/8 pathway
Explanation:
BMPs are members of the TGF-beta superfamily. When a BMP binds to its specific transmembrane serine/threonine kinase receptor, it triggers the phosphorylation of receptor-regulated Smads (R-Smads), specifically Smad 1, 5, and 8. These phosphorylated Smads form a complex with Smad 4 (Co-Smad) and translocate to the nucleus to induce transcription of osteogenic genes like Runx2.
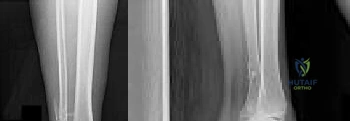
Question 10:
A 29-year-old man sustains a high-energy injury resulting in a femoral neck fracture. Radiographs reveal a Pauwels type III pattern. Which of the following mechanical factors most significantly contributes to the high rate of nonunion and failure of fixation in this specific fracture pattern?
Options:
- High compressive forces across the fracture site
- High shearing forces across the fracture site
- Disruption of the ligamentum teres artery
- Insufficient cancellous bone volume in young patients
- Excessive periosteal callus formation preventing primary bone healing
Correct Answer: High shearing forces across the fracture site
Explanation:
The Pauwels classification of femoral neck fractures is based on the angle of the fracture line relative to the horizontal plane. A Pauwels type III fracture is highly vertical (angle > 50 degrees). This vertical orientation converts normal hip joint reaction forces into destructive shear forces at the fracture site, predisposing it to varus collapse, nonunion, and implant failure, unlike horizontal fractures which experience stabilizing compressive forces.
Question 11:
A 12-year-old boy presents with left knee pain and an antalgic gait. Examination reveals obligate external rotation of the left hip during passive flexion. Radiographs confirm a Slipped Capital Femoral Epiphysis (SCFE). Which of the following factors is considered an absolute indication for prophylactic in situ pinning of the contralateral, asymptomatic hip?
Options:
- Patient age greater than 14 years
- Male sex
- Underlying endocrine disorder (e.g., hypothyroidism)
- High body mass index (BMI > 95th percentile)
- Southwick angle greater than 50 degrees on the affected side
Correct Answer: Underlying endocrine disorder (e.g., hypothyroidism)
Explanation:
The risk of developing a contralateral slip in a patient with an initial unilateral SCFE ranges from 20-40% overall, but approaches 100% in patients with an underlying endocrinopathy (such as hypothyroidism, growth hormone deficiency, or panhypopituitarism) or a history of radiation therapy to the pelvis. In these specific populations, prophylactic pinning of the contralateral hip is absolutely indicated.
Question 12:
According to the Lenke classification system for Adolescent Idiopathic Scoliosis (AIS), curve flexibility is a key determinant in selecting fusion levels. A scoliotic curve is defined as 'structural' if it meets which of the following radiographic criteria on coronal side-bending films?
Options:
- Cobb angle corrects to less than 25 degrees
- Cobb angle fails to correct to less than 25 degrees
- Apical vertebral translation is greater than 2 cm
- Thoracic kyphosis (T2-T12) measures greater than +40 degrees
- Apical vertebral rotation is Nash-Moe Grade III or higher
Correct Answer: Cobb angle fails to correct to less than 25 degrees
Explanation:
In the Lenke classification of AIS, the distinction between a major/structural curve and a minor/non-structural curve dictates the levels to be fused. A curve is considered 'structural' if the Cobb angle remains at 25 degrees or greater on a maximum voluntary supine side-bending radiograph. Additionally, regional sagittal kyphosis of >= +20 degrees also defines a proximal thoracic or main thoracic curve as structural.
Question 13:
During a measured resection primary Total Knee Arthroplasty (TKA), the surgeon utilizes trial components and notes the knee is perfectly balanced in full extension but excessively tight in flexion. Which of the following maneuvers is the most appropriate next step to achieve a balanced knee?
Options:
- Resect more distal femur
- Downsize the femoral component
- Resect more proximal tibia
- Release the posterior capsule
- Upsize the polyethylene insert
Correct Answer: Downsize the femoral component
Explanation:
In gap balancing principles for TKA, if the knee is balanced in extension but tight in flexion, the flexion gap must be increased without altering the extension gap. Downsizing the femoral component typically shifts the posterior condylar resection anteriorly (assuming anterior referencing or an offset system is used to maintain anterior flushness), effectively resecting more posterior bone and opening the flexion gap. Resecting the tibia alters both gaps equally.
Question 14:
A 45-year-old manual laborer presents with chronic, activity-related wrist pain. Radiographs demonstrate a scaphoid nonunion advanced collapse (SNAC) pattern. According to the predictable and sequential pattern of arthrosis in a SNAC wrist, which articulation is characteristically preserved until the terminal stages of the disease process?
Options:
- Radioscaphoid joint
- Capitolunate joint
- Scaphocapitate joint
- Radiolunate joint
- Scaphotrapezial joint
Correct Answer: Radiolunate joint
Explanation:
In both Scaphoid Nonunion Advanced Collapse (SNAC) and Scapholunate Advanced Collapse (SLAC) wrists, the radiolunate joint is characteristically spared from degenerative changes until very late. This sparing occurs because the proximal articular surface of the lunate maintains a concentric, conformal geometry with the spherical lunate fossa of the radius, preserving normal contact pressures despite profound carpal instability.
Question 15:
A 55-year-old patient with long-standing, poorly controlled diabetes mellitus presents with an acute, red, hot, and swollen right foot. Radiographs demonstrate extensive osteopenia, periarticular fragmentation, bony debris, and midfoot subluxation. According to the Eichenholtz classification of Charcot neuroarthropathy, which stage does this represent?
Options:
- Stage 0 (High risk/Inflammatory)
- Stage I (Development/Fragmentation)
- Stage II (Coalescence)
- Stage III (Consolidation/Reconstruction)
- Stage IV (Ulceration/Infection)
Correct Answer: Stage I (Development/Fragmentation)
Explanation:
The Eichenholtz classification describes the radiographic evolution of Charcot arthropathy. Stage I (Development or Fragmentation) is characterized by acute inflammation clinically, and radiographs showing osteopenia, periarticular fragmentation, subluxation/dislocation, and bony debris. Stage 0 lacks radiographic findings but has clinical swelling. Stage II (Coalescence) shows absorption of fine debris and early fusion. Stage III (Consolidation) shows remodeling and fixed deformity.
Question 16:
When evaluating a patient with recurrent anterior shoulder instability, the 'glenoid track' concept is utilized to assess the risk of recurrent dislocation. A Hill-Sachs lesion is considered 'off-track' and at high risk of engagement if it meets which of the following criteria?
Options:
- It extends medially beyond the medial margin of the glenoid track
- It is entirely contained within the glenoid track boundaries
- It is associated with greater than 10% anterior glenoid bone loss
- It engages only in isolated external rotation without abduction
- It spares the central articular cartilage of the humeral head
Correct Answer: It extends medially beyond the medial margin of the glenoid track
Explanation:
The glenoid track is defined as the zone of contact between the humeral head and the glenoid during arm abduction and external rotation. It is calculated based on the intact glenoid width minus anterior bone loss. If the medial margin of a Hill-Sachs defect extends further medially than the medial boundary of the glenoid track, the lesion is 'off-track.' This means it will drop over the anterior glenoid rim during functional positioning, 'engaging' and levering the humerus out of joint.
Question 17:
Articular cartilage is a highly specialized tissue that exhibits distinct zones from the articular surface down to the subchondral bone. In which zone do the type II collagen fibers orient themselves strictly perpendicular to the joint surface to resist compressive loads?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
In the deep (radial) zone of articular cartilage, chondrocytes are arranged in vertical columns, and the thick type II collagen fibers are oriented perpendicularly to the articular surface. This architecture provides the primary resistance to compressive forces. In contrast, the superficial zone has collagen parallel to the surface (to resist shear), and the middle zone has an oblique, random orientation.
Question 18:
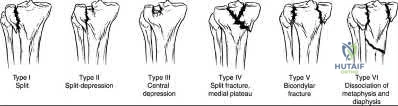
A 40-year-old pedestrian is struck by a vehicle and sustains a complex proximal tibia fracture. Imaging confirms a Schatzker Type IV fracture involving the medial tibial plateau. What is the typical mechanism of injury for this specific fracture pattern, and which anatomic structure is placed under the highest tensile stress?
Options:
- Valgus force; Medial collateral ligament (MCL)
- Varus force; Lateral collateral ligament (LCL)
- Axial load in hyperflexion; Anterior cruciate ligament (ACL)
- Hyperextension force; Popliteal artery
- Rotational force; Patellar tendon
Correct Answer: Varus force; Lateral collateral ligament (LCL)
Explanation:
A Schatzker Type IV fracture involves a fracture of the medial tibial plateau. Unlike lateral plateau fractures (which are typically low-energy valgus injuries), a medial plateau fracture usually results from a high-energy varus force combined with an axial load. This mechanism places extreme tension on the lateral-sided structures, frequently leading to associated Lateral Collateral Ligament (LCL), posterolateral corner, and/or peroneal nerve injuries.
Question 19:
A 35-year-old volleyball player presents with the inability to actively extend the distal interphalangeal (DIP) joint of her long finger after a jamming injury. This classic mallet finger deformity represents a disruption of the terminal extensor tendon. If left untreated, what secondary digit deformity is most likely to develop over time?
Options:
- Boutonniere deformity
- Swan neck deformity
- Pseudoboutonniere deformity
- Intrinsic plus hand
- Lumbrical plus deformity
Correct Answer: Swan neck deformity
Explanation:
A mallet finger results from the avulsion or rupture of the terminal extensor tendon at the base of the distal phalanx. If left untreated, the extensor mechanism retracts proximally, concentrating extensor forces at the central slip over the proximal interphalangeal (PIP) joint. This chronic imbalance leads to progressive hyperextension of the PIP joint combined with flexion of the DIP joint, clinically recognized as a swan neck deformity.
Question 20:
A 14-year-old boy presents with severe thigh pain, low-grade fever, and unintentional weight loss. Radiographs show a permeative, destructive diaphyseal lesion of the femur with a multi-layered 'onion skin' periosteal reaction. A core needle biopsy is performed. Which of the following chromosomal translocations is most highly diagnostic for this malignancy?
Options:
- t(11;22)(q24;q12)
- t(X;18)(p11;q11)
- t(12;16)(q13;p11)
- t(2;13)(q35;q14)
- t(9;22)(q34;q11)
Correct Answer: t(11;22)(q24;q12)
Explanation:
The clinical and radiographic presentation is classic for Ewing sarcoma. Ewing sarcoma is a small round blue cell tumor characterized genetically by a balanced reciprocal translocation, most commonly t(11;22)(q24;q12), which is present in 85-90% of cases and results in the fusion of the EWS and FLI1 genes. The t(X;18) translocation is seen in synovial sarcoma, t(12;16) in myxoid liposarcoma, and t(2;13) in alveolar rhabdomyosarcoma.