Full Question & Answer Text (for Search Engines)
Question 1:
A 28-year-old male sustains a closed midshaft tibia fracture. He is treated with a reamed intramedullary nail. Which of the following is the most significant advantage of reaming the canal prior to nail insertion compared to unreamed nailing for closed tibia fractures?
Options:
- Lower rates of compartment syndrome
- Decreased incidence of malunion
- Higher rates of union and lower rates of implant failure
- Reduced operation time
- Lower incidence of anterior knee pain
Correct Answer: Higher rates of union and lower rates of implant failure
Explanation:
The SPRINT (Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures) trial demonstrated that for closed tibia fractures, reamed intramedullary nailing is associated with significantly higher rates of union and lower rates of implant failure compared to unreamed nailing. Anterior knee pain rates are similar between both techniques.
Question 2:
In modern total hip arthroplasty, the use of highly cross-linked polyethylene (HXLPE) compared to conventional ultra-high-molecular-weight polyethylene is associated with which of the following?
Options:
- Increased incidence of catastrophic liner fracture
- Decreased volumetric wear rates and decreased osteolysis
- Increased risk of polyethylene oxidation when annealed
- Higher wear rates when used with larger femoral heads
- Increased risk of impingement due to required thicker liners
Correct Answer: Decreased volumetric wear rates and decreased osteolysis
Explanation:
Highly cross-linked polyethylene (HXLPE) was developed to reduce wear debris in THA. Cross-linking via irradiation significantly decreases volumetric wear rates and subsequent particle-induced osteolysis. However, irradiation creates free radicals, which are eliminated by thermal treatments (remelting or annealing) to prevent oxidation, though remelting decreases some mechanical properties.
Question 3:
A 22-year-old female soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BTB) autograft. During the rehabilitation phase, she is at highest risk for which of the following complications compared to a hamstring autograft?
Options:
- Deep infection
- Anterior knee pain
- Hamstring weakness
- Graft rupture
- Saphenous nerve injury
Correct Answer: Anterior knee pain
Explanation:
BTB autograft is considered the 'gold standard' for ACL reconstruction but is associated with a higher incidence of donor-site morbidity, specifically anterior knee pain and pain with kneeling, when compared to hamstring autograft. Deep infection rates are similar or slightly higher in hamstring autografts.
Question 4:
Which of the following transcription factors most strongly promotes the differentiation of mesenchymal stem cells into osteoblasts during fracture healing?
Options:
- Low oxygen tension
- High strain environment
- Core binding factor alpha-1 (Runx2)
- Sclerostin
- Tumor necrosis factor-alpha
Correct Answer: Core binding factor alpha-1 (Runx2)
Explanation:
Core binding factor alpha-1 (Cbfa1), also known as Runx2, is the master transcription factor responsible for the differentiation of multipotent mesenchymal stem cells into the osteoblast lineage. Sclerostin is a Wnt antagonist that inhibits bone formation. High strain promotes fibrous tissue, and low oxygen promotes cartilage formation.
Question 5:
A 13-year-old obese boy presents with 3 weeks of left groin pain and a limp. Examination reveals obligatory external rotation of the left hip during passive flexion. A radiograph is provided. What is the recommended definitive management for a stable slipped capital femoral epiphysis (SCFE)?
Options:
- Closed reduction and spica casting
- Open reduction and internal fixation
- In situ single screw fixation
- Proximal femoral osteotomy
- Observation and non-weight bearing
Correct Answer: In situ single screw fixation
Explanation:
A stable SCFE is characterized by the patient's ability to bear weight (with or without crutches). The standard of care for a stable SCFE is in situ fixation with a single cannulated screw placed centrally within the epiphysis. Closed reduction is contraindicated due to the high risk of avascular necrosis.
Question 6:
A 45-year-old woman presents with severe carpal tunnel syndrome. During open carpal tunnel release, the surgeon must be careful to avoid injuring the recurrent motor branch of the median nerve. This branch most commonly exhibits which of the following anatomic variations?
Options:
- Extraligamentous with recurrent course
- Subligamentous with recurrent course
- Transligamentous
- Ulnar to the median nerve main trunk
- Piercing the transverse carpal ligament at the ulnar border
Correct Answer: Extraligamentous with recurrent course
Explanation:
According to Lanz's classification, the most common anatomic course of the recurrent motor branch of the median nerve is extraligamentous with a recurrent course (approximately 50-80% of cases), branching distal to the transverse carpal ligament and turning back to innervate the thenar musculature.
Question 7:
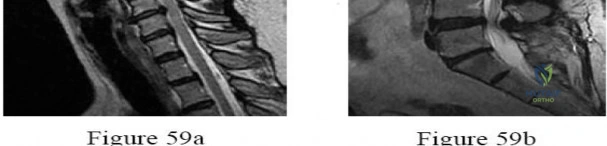
A 65-year-old man presents with progressive clumsiness in his hands, difficulty buttoning his shirt, and a broad-based gait. A T2-weighted MRI shows spinal cord compression with intrinsic cord signal change at C4-C5. Which of the following MRI findings is associated with the poorest prognosis for neurological recovery after surgical decompression in cervical spondylotic myelopathy?
Options:
- T2 hyperintensity that is single-level
- T1 hypointensity corresponding to the T2 hyperintensity
- T2 hyperintensity involving less than 50% of the cord cross-sectional area
- Presence of osteophytes at the level of compression
- Decreased CSF space without cord signal change
Correct Answer: T1 hypointensity corresponding to the T2 hyperintensity
Explanation:
In cervical spondylotic myelopathy, the presence of T1 hypointensity corresponding to a T2 hyperintense lesion indicates myelomalacia or cystic necrosis of the spinal cord. This finding is a strong predictor of poor functional recovery following surgical decompression.
Question 8:
A 25-year-old male sustains a midfoot injury. Weight-bearing radiographs demonstrate widening of the interval between the medial and middle cuneiforms. The Lisfranc ligament connects which of the following two structures?
Options:
- First metatarsal base and medial cuneiform
- Second metatarsal base and medial cuneiform
- Second metatarsal base and middle cuneiform
- First metatarsal base and second metatarsal base
- Third metatarsal base and lateral cuneiform
Correct Answer: Second metatarsal base and medial cuneiform
Explanation:
The Lisfranc ligament is an interosseous ligament that connects the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. It is critical for the stability of the midfoot arch, as there is no direct ligamentous connection between the bases of the first and second metatarsals.
Question 9:
A 15-year-old boy presents with a destructive, bone-forming lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. Biopsy confirms high-grade osteosarcoma. Assuming the patient has localized disease, which of the following is the most important prognostic factor for long-term survival?
Options:
- Patient age at presentation
- Histologic subtype (e.g., osteoblastic vs. chondroblastic)
- Extent of tumor necrosis following neoadjuvant chemotherapy
- Size of the primary tumor
- Serum alkaline phosphatase level at presentation
Correct Answer: Extent of tumor necrosis following neoadjuvant chemotherapy
Explanation:
In non-metastatic high-grade osteosarcoma, the histologic response to neoadjuvant chemotherapy (typically measured by the percentage of tumor necrosis) is one of the most powerful prognostic indicators. Greater than 90% necrosis indicates a 'good responder' and is associated with significantly higher overall survival.
Question 10:
A 30-year-old man sustains a highly comminuted proximal tibia fracture. Twelve hours post-admission, he develops severe pain with passive toe stretch. His diastolic blood pressure is 75 mmHg and anterior compartment pressure is 55 mmHg. What is the most appropriate next step in management?
Options:
- Elevate the leg above the level of the heart
- Apply a long leg cast
- Administer intravenous mannitol
- Perform emergent four-compartment fasciotomies
- Observation and repeat pressures in 2 hours
Correct Answer: Perform emergent four-compartment fasciotomies
Explanation:
The clinical picture is highly suspicious for acute compartment syndrome. The delta pressure (Diastolic BP - Compartment Pressure) is 75 - 55 = 20 mmHg. A delta pressure of 30 mmHg or less is an absolute indication for emergent four-compartment fasciotomy of the lower leg.
Question 11:
A 22-year-old male falls onto an outstretched hand. Follow-up MRI at 2 weeks confirms a nondisplaced fracture of the scaphoid proximal pole. The blood supply to the proximal pole of the scaphoid is tenuous because the major nutrient vessels enter the scaphoid at which location?
Options:
- Through the proximal pole directly
- Distal to the waist and course proximally
- Volar to the tuberosity and course distally
- Through the radioscaphocapitate ligament
- Through the scapholunate interosseous ligament
Correct Answer: Distal to the waist and course proximally
Explanation:
The primary blood supply to the scaphoid comes from the dorsal carpal branch of the radial artery, which enters the scaphoid at the dorsal ridge (distal to the waist) and supplies the proximal 80% of the bone via retrograde intraosseous flow. Fractures at the waist or proximal pole disrupt this supply, leading to high rates of avascular necrosis and nonunion.
Question 12:
A 4-month-old female infant is treated for developmental dysplasia of the hip (DDH) with a Pavlik harness. During treatment, what is the most significant risk associated with excessive abduction of the hips in the harness?
Options:
- Avascular necrosis of the femoral head
- Femoral nerve palsy
- Inferior dislocation of the hip
- Acetabular dysplasia
- Obturator nerve palsy
Correct Answer: Avascular necrosis of the femoral head
Explanation:
In Pavlik harness treatment, excessive abduction of the hips places the medial circumflex femoral artery at risk of compression against the iliopsoas tendon, leading to avascular necrosis of the femoral head. Excessive flexion is associated with femoral nerve palsy.
Question 13:
In the process of endochondral ossification during fracture healing, which type of collagen is most predominantly synthesized by chondrocytes in the hypertrophic zone just prior to calcification?
Options:
- Type I collagen
- Type II collagen
- Type III collagen
- Type IX collagen
- Type X collagen
Correct Answer: Type X collagen
Explanation:
Hypertrophic chondrocytes uniquely synthesize Type X collagen during endochondral ossification. This collagen plays a critical role in the mineralization of the cartilaginous matrix, allowing subsequent vascular invasion and replacement by bone.
Question 14:
A 14-year-old female gymnast presents with insidious onset of low back pain exacerbated by extension. Radiographs show a unilateral pars interarticularis defect at L5. What is the classic radiographic appearance of this defect on an oblique lumbar radiograph?
Options:
- Bamboo spine
- Scottie dog with a collar
- Picture frame vertebra
- Rugger jersey spine
- Ivory vertebra
Correct Answer: Scottie dog with a collar
Explanation:
Spondylolysis, a defect in the pars interarticularis, classically appears as a 'collar' or 'break' around the neck of the 'Scottie dog' on an oblique radiograph of the lumbar spine.
Question 15:
A 25-year-old male undergoes arthroscopy for a bucket-handle tear of the medial meniscus. The surgeon decides to perform an inside-out meniscus repair. Which of the following neurovascular structures is at greatest risk of injury during the posteromedial repair?
Options:
- Common peroneal nerve
- Popliteal artery
- Saphenous nerve
- Sural nerve
- Tibial nerve
Correct Answer: Saphenous nerve
Explanation:
During an inside-out repair of the medial meniscus, the saphenous nerve (specifically its sartorial branch and the main trunk posteriorly) is at highest risk. The common peroneal nerve is at risk during a lateral meniscus repair.
Question 16:
A 65-year-old man presents with anterior knee pain and a feeling of instability during stair climbing 1 year after a primary total knee arthroplasty. Examination reveals a lateral patellar tilt. CT scan is performed to evaluate component rotation. Which of the following errors in component positioning is most likely responsible for his symptoms?
Options:
- External rotation of the femoral component
- Internal rotation of the femoral component
- External rotation of the tibial component
- Anterior placement of the tibial component
- Joint line depression
Correct Answer: Internal rotation of the femoral component
Explanation:
Internal rotation of the femoral component or the tibial component increases the Q angle, leading to lateral patellar maltracking, lateral patellar tilt, and anterior knee pain. External rotation of the components generally improves patellar tracking.
Question 17:
Galvanic corrosion between orthopedic implants occurs when two dissimilar metals are in contact within an electrolytic environment. Which of the following combinations of metals is most likely to result in significant galvanic corrosion in vivo and is generally contraindicated?
Options:
- Titanium and Titanium alloy
- Stainless steel and Cobalt-Chromium
- Stainless steel and Titanium
- Cobalt-Chromium and Titanium
- Zirconium and Titanium
Correct Answer: Stainless steel and Titanium
Explanation:
Stainless steel and titanium have a large electrochemical potential difference. When placed in contact (e.g., a stainless steel plate with a titanium screw), the stainless steel acts as the anode and corrodes rapidly. Cobalt-chromium and titanium are routinely used together (e.g., THA stems and heads) with an acceptable passivation layer preventing severe corrosion.
Question 18:
A 40-year-old recreational athlete sustains an acute Achilles tendon rupture. During surgical repair, the surgeon must be careful to avoid injuring the sural nerve. At approximately what distance proximal to the calcaneal insertion does the sural nerve typically cross the lateral border of the Achilles tendon?
Options:
- 2 cm
- 6 cm
- 10 cm
- 15 cm
- 20 cm
Correct Answer: 10 cm
Explanation:
The sural nerve crosses the lateral border of the Achilles tendon approximately 10 cm (range 9-12 cm) proximal to its insertion on the calcaneal tuberosity. It is highly susceptible to injury during percutaneous or minimally invasive Achilles repairs in this region.
Question 19:
A 32-year-old man sustains a closed spiral fracture of the distal third of his humerus (Holstein-Lewis fracture). He has a wrist drop on presentation. Initial management with a functional fracture brace is selected. At what point is surgical exploration of the radial nerve indicated if there is no clinical or electromyographic improvement?
Options:
- 2 weeks
- 6 weeks
- 3-4 months
- 6-8 months
- Immediately
Correct Answer: 3-4 months
Explanation:
Primary radial nerve palsy in a closed humeral shaft fracture is typically managed expectantly, as spontaneous recovery rates exceed 70%. If there is no clinical or EMG evidence of recovery by 3 to 4 months, surgical exploration of the nerve is indicated.
Question 20:
A 55-year-old man presents with dull, aching pain in his right pelvis for 6 months. Radiographs reveal a large, lytic lesion in the right ilium with 'popcorn' calcifications. Biopsy demonstrates a moderately cellular cartilage tumor with plump, binucleated chondrocytes. What is the most appropriate definitive management for this patient?
Options:
- Neoadjuvant chemotherapy followed by wide surgical resection
- Wide surgical resection alone
- Intralesional curettage and bone grafting
- Primary radiation therapy
- Observation with serial radiographs
Correct Answer: Wide surgical resection alone
Explanation:
Conventional chondrosarcoma is generally resistant to both chemotherapy and radiation therapy due to its poor vascularity and slow growth. The mainstay of treatment for intermediate or high-grade chondrosarcoma of the pelvis is wide surgical resection.
Question 21:
A 24-year-old athlete sustains a hyperplantarflexion injury to the midfoot. Radiographs show widening between the 1st and 2nd metatarsal bases. The primary stabilizing ligament of this joint originates from and inserts into which of the following structures?
Options:
- Medial cuneiform to 1st metatarsal base
- Medial cuneiform to 2nd metatarsal base
- Intermediate cuneiform to 2nd metatarsal base
- Lateral cuneiform to 2nd metatarsal base
- Medial cuneiform to 3rd metatarsal base
Correct Answer: Medial cuneiform to 2nd metatarsal base
Explanation:
The Lisfranc ligament is the largest and most important of the ligaments stabilizing the tarsometatarsal joint. It originates on the lateral aspect of the medial cuneiform and inserts on the medial aspect of the base of the second metatarsal. Rupture of this ligament leads to diastasis between the first and second rays.
Question 22:
A 45-year-old man is involved in a motor vehicle collision. Imaging demonstrates a traumatic spondylolisthesis of the axis (Hangman's fracture) with 15 degrees of angulation and 2 mm of translation (Levine and Edwards Type IIA). Which of the following treatments or maneuvers is strictly CONTRAINDICATED in the initial nonoperative management of this specific fracture pattern?
Options:
- Cervical traction
- Halo vest immobilization in slight extension
- Rigid cervical collar
- Application of compression forces
- Supine positioning
Correct Answer: Cervical traction
Explanation:
A Levine and Edwards Type IIA Hangman's fracture is characterized by severe angulation with minimal translation. This pattern indicates disruption of the posterior longitudinal ligament and the C2-C3 disc with an intact anterior longitudinal ligament acting as a hinge. Cervical traction is strictly contraindicated because it will distract the fracture site, exacerbate the angulation deformity, and cause neurologic injury. Treatment consists of closed reduction in slight extension and compression in a halo vest.
Question 23:
A 12-year-old obese boy presents with a left-sided slipped capital femoral epiphysis (SCFE). Which of the following represents the strongest indication for prophylactic in situ pinning of the contralateral, asymptomatic hip?
Options:
- Age greater than 14 years
- Male gender
- Presence of an endocrine disorder
- Grade III slip on the symptomatic side
- Acute-on-chronic presentation
Correct Answer: Presence of an endocrine disorder
Explanation:
The presence of an underlying endocrine disorder (such as hypothyroidism, panhypopituitarism, or renal osteodystrophy) is a strong risk factor for bilateral SCFE, with some studies reporting nearly 100% eventual bilateral involvement. Prophylactic pinning of the contralateral hip is highly recommended in these patients. Other indications include prior radiation therapy and age younger than 10.
Question 24:
The pivot shift test is widely considered the most specific clinical examination maneuver for an anterior cruciate ligament (ACL) tear. Which of the following best describes the biomechanics of a positive pivot shift test in an ACL-deficient knee?
Options:
- The tibia subluxates anteriorly in flexion and reduces in extension
- The tibia subluxates anteriorly in extension and reduces in flexion at 20-30 degrees
- The tibia subluxates posteriorly in extension and reduces in flexion
- The tibia subluxates anteriorly at 90 degrees of flexion and reduces in full extension
- The femur subluxates anteriorly in extension and reduces in flexion
Correct Answer: The tibia subluxates anteriorly in extension and reduces in flexion at 20-30 degrees
Explanation:
In an ACL-deficient knee, the tibia rests in an anteriorly subluxated position when the knee is in full extension. As the examiner flexes the knee with a valgus and internal rotation force, the iliotibial band (ITB) transitions from acting as a knee extensor (anterior to the axis of rotation) to a knee flexor (posterior to the axis of rotation) at approximately 20-30 degrees of flexion. This vector change creates a posterior force on the tibia, abruptly reducing the joint and producing the classic 'clunk' of the pivot shift.
Question 25:
Bone morphogenetic proteins (BMPs) play a crucial role in osteoinduction and are utilized in various spine and trauma applications. Which of the following intracellular signaling molecules is directly phosphorylated following the binding of BMP-2 or BMP-7 to its serine/threonine kinase membrane receptor?
Options:
- Beta-catenin
- Smad 1/5/8
- Smad 2/3
- Smad 4
- Runx2
Correct Answer: Smad 1/5/8
Explanation:
BMPs exert their effects by binding to specific serine/threonine kinase receptors on the cell surface. This binding leads to the direct phosphorylation of the receptor-regulated Smads (R-Smads), specifically Smad 1, 5, and 8. These then form a complex with the common-mediator Smad 4, which translocates to the nucleus to upregulate osteogenic genes like Runx2. TGF-beta, in contrast, signals via Smad 2 and 3.
Question 26:
A 28-year-old rugby player presents with an inability to actively flex the distal interphalangeal (DIP) joint of his ring finger after catching it in an opponent's jersey. Radiographs reveal a small bony avulsion fragment located volar to the proximal interphalangeal (PIP) joint. According to the Leddy and Packer classification, what is the correct injury type and the anatomic structure that arrests the retracted tendon?
Options:
- Type I, retracts to the palm and is held by the lumbrical origin
- Type II, retracts to the PIP joint and is held by the vinculum longum
- Type III, retracts to the A2 pulley
- Type III, retracts to the A4 pulley and involves a large bony avulsion
- Type IV, involves an avulsion from the distal phalanx base with an associated central slip injury
Correct Answer: Type II, retracts to the PIP joint and is held by the vinculum longum
Explanation:
Jersey finger injuries are classified by Leddy and Packer. Type I involves retraction of the FDP tendon into the palm, often requiring repair within 7-10 days due to compromised blood supply. Type II involves retraction to the level of the PIP joint, where it is caught by the intact vinculum longum (or Camper's chiasm) and often has a small bony fragment visible on X-ray at the PIP level. Type III involves a large bony avulsion that gets caught at the A4 pulley.
Question 27:
A 15-year-old boy is diagnosed with a high-grade intramedullary osteosarcoma of the distal femur. He undergoes a standard protocol of neoadjuvant chemotherapy followed by wide surgical resection. Which of the following factors has been established as the single most important prognostic indicator for his long-term survival?
Options:
- Tumor volume at initial presentation
- Histologic subtype of the tumor
- Percentage of tumor necrosis following neoadjuvant chemotherapy
- Anatomic location of the lesion
- Presence of a pathological fracture at presentation
Correct Answer: Percentage of tumor necrosis following neoadjuvant chemotherapy
Explanation:
The most important prognostic factor for survival in patients with localized, high-grade osteosarcoma is the histologic response of the tumor to neoadjuvant chemotherapy. Patients with >90% tumor necrosis are considered 'good responders' and have a significantly better prognosis and 5-year survival rate compared to 'poor responders' (<90% necrosis).
Question 28:
A 35-year-old skier sustains a Schatzker Type II (split-depression) tibial plateau fracture after a fall. Which of the following intra-articular structures is most frequently injured in conjunction with this specific fracture pattern?
Options:
- Medial meniscus
- Lateral meniscus
- Anterior cruciate ligament
- Posterior cruciate ligament
- Medial collateral ligament
Correct Answer: Lateral meniscus
Explanation:
Schatzker Type II fractures involve a split-depression of the lateral tibial plateau. Associated soft tissue injuries are extremely common in tibial plateau fractures. The lateral meniscus is torn or entrapped in the fracture site in up to 40-50% of lateral plateau fractures (Schatzker I and II), making it the most frequently injured structure in this context.
Question 29:
A 68-year-old man presents with bilateral leg pain, heaviness, and cramping that worsens after walking two blocks. The orthopedic surgeon is attempting to distinguish between neurogenic claudication secondary to lumbar spinal stenosis and vascular claudication. Which of the following clinical findings most reliably points toward a diagnosis of neurogenic claudication?
Options:
- Pain is rapidly relieved by standing still
- Diminished distal pedal pulses on examination
- Pain is relieved or prevented by walking up an incline
- Pain is rapidly exacerbated by riding a stationary bicycle
- Presence of a stocking-glove sensory deficit
Correct Answer: Pain is relieved or prevented by walking up an incline
Explanation:
Neurogenic claudication is exacerbated by lumbar extension (which decreases the cross-sectional area of the spinal canal) and relieved by lumbar flexion. Walking up an incline causes the patient to lean forward (flex the lumbar spine), thereby keeping the spinal canal open and preventing symptoms. Conversely, walking up an incline increases metabolic demand, which would worsen vascular claudication. Bicycling also involves flexion and is typically well-tolerated in neurogenic claudication.
Question 30:
A 45-year-old male recreational athlete sustains an acute mid-substance Achilles tendon rupture. He is discussing management options with his surgeon. Based on current high-level evidence, which of the following statements comparing nonoperative management versus surgical repair is most accurate?
Options:
- When early functional rehabilitation is employed, nonoperative management has a similar re-rupture rate to surgical repair but avoids surgical complications.
- Surgical repair has a significantly lower re-rupture rate than nonoperative management with early functional rehab.
- Plantarflexion strength is significantly better after nonoperative management compared to surgery.
- The risk of sural nerve injury is highest with open repair compared to percutaneous repair.
- Nonoperative treatment mandates strict rigid cast immobilization for 12 weeks to achieve equivalent outcomes.
Correct Answer: When early functional rehabilitation is employed, nonoperative management has a similar re-rupture rate to surgical repair but avoids surgical complications.
Explanation:
Historically, surgical repair was thought to have a lower re-rupture rate. However, recent Level 1 evidence (RCTs and meta-analyses) has shown that when patients undergo nonoperative management combined with an early functional rehabilitation protocol (early weight-bearing in a functional brace), the re-rupture rates are not statistically different from surgical repair. Nonoperative management avoids the risks of wound healing complications and infection inherent to surgery.
Question 31:
A 6-week-old infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). During a routine follow-up, the parents report that the child has stopped actively kicking the affected leg. On physical examination, there is an absent patellar reflex and decreased active knee extension. The harness is found to be in excessive hyperflexion. Which of the following nerves is most likely compressed?
Options:
- Sciatic nerve
- Femoral nerve
- Obturator nerve
- Superior gluteal nerve
- Lateral femoral cutaneous nerve
Correct Answer: Femoral nerve
Explanation:
Femoral nerve palsy is a known complication of Pavlik harness treatment, usually resulting from hyperflexion of the hip (anterior straps too tight). It manifests as decreased spontaneous movement of the leg, specifically decreased active knee extension (quadriceps weakness) and an absent patellar reflex. The treatment involves loosening the anterior straps or temporarily removing the harness.
Question 32:
A 50-year-old woman complains of acute posterior knee pain and a 'pop' while squatting deeply. MRI reveals a complete tear of the medial meniscus posterior root. Biomechanically, if left untreated, a complete posterior root tear of the medial meniscus acts as the equivalent to which of the following?
Options:
- A 25% partial medial meniscectomy
- A 50% partial medial meniscectomy
- A total medial meniscectomy
- An anterior cruciate ligament tear
- A medial collateral ligament tear
Correct Answer: A total medial meniscectomy
Explanation:
The meniscal roots anchor the meniscus to the tibial plateau, allowing it to convert axial loads into circumferential hoop stresses. A complete disruption of the posterior root disrupts these hoop stresses entirely, rendering the meniscus functionally incompetent. Biomechanical studies have proven that a medial meniscus posterior root tear alters contact pressures and kinematics equivalent to those seen in a complete (total) medial meniscectomy, predisposing the joint to rapid osteoarthritis.
Question 33:
Articular cartilage exhibits complex viscoelastic properties under loading. When a constant deformation (strain) is rapidly applied and maintained on articular cartilage, the internal peak stress gradually decreases over time until it reaches an equilibrium. Which of the following terms best describes this specific biomechanical phenomenon?
Options:
- Creep
- Stress relaxation
- Hysteresis
- Anisotropy
- Fatigue failure
Correct Answer: Stress relaxation
Explanation:
Stress relaxation is a hallmark of viscoelastic materials, defined as the decrease in internal stress over time when subjected to a constant strain (deformation). Creep, conversely, is the progressive increase in strain (deformation) over time when subjected to a constant stress (load). Hysteresis refers to the energy lost (usually as heat) during the loading and unloading cycle of a viscoelastic material.
Question 34:
A 30-year-old male is brought to the trauma bay with hemodynamic instability following a high-speed motorcycle crash. Pelvic radiographs show a severely displaced 'open-book' pelvic fracture (APC-III). An emergency pelvic binder is to be applied to reduce pelvic volume. To be biomechanically effective and stabilize the fracture, the binder should be centered directly over which of the following anatomical landmarks?
Options:
- Iliac crests
- Anterior superior iliac spines (ASIS)
- Greater trochanters
- Symphysis pubis
- Ischial tuberosities
Correct Answer: Greater trochanters
Explanation:
To effectively reduce pelvic volume in an open-book fracture, the compressive force must be applied across the greater trochanters. Placing the binder higher over the iliac crests or ASIS can paradoxically widen the pelvis at the level of the symphysis pubis and fail to stabilize the posterior ring.
Question 35:
A 45-year-old woman undergoes an open carpal tunnel release. Postoperatively, she reports a new, severe weakness in thumb opposition, despite normal opposition preoperatively. The surgeon suspects an iatrogenic nerve injury. The affected nerve branch most likely originates from which aspect of the median nerve?
Options:
- Ulnar side of the median nerve, proximal to the transverse carpal ligament
- Radial side of the median nerve, frequently just distal to the transverse carpal ligament
- Ulnar side of the median nerve, within Guyon's canal
- Posterior interosseous nerve branch
- Anterior interosseous nerve branch
Correct Answer: Radial side of the median nerve, frequently just distal to the transverse carpal ligament
Explanation:
The recurrent motor branch of the median nerve innervates the thenar muscles (opponens pollicis, abductor pollicis brevis, superficial head of flexor pollicis brevis). In the most common anatomic variation (extraneous), it branches from the radial side of the median nerve just distal to the transverse carpal ligament and courses recurrently. Injury to this branch during carpal tunnel release results in loss of thumb opposition.
Question 36:
A 60-year-old man presents with progressive, deep pelvic pain. A core needle biopsy of a large lytic lesion in the ilium confirms the diagnosis of conventional Grade II chondrosarcoma. Staging studies are negative for metastasis. Which of the following is the standard of care for definitive management?
Options:
- Neoadjuvant chemotherapy followed by wide surgical excision
- Wide surgical excision alone
- Intralesional curettage with adjuvant cryotherapy and cementation
- Primary fractionated radiation therapy
- Surgical excision followed by adjuvant systemic chemotherapy
Correct Answer: Wide surgical excision alone
Explanation:
Conventional chondrosarcoma is notoriously resistant to both systemic chemotherapy and radiation therapy due to its poor vascularity and slow division rate. The mainstay of treatment for intermediate and high-grade (Grade II and III) chondrosarcomas, as well as those located in the pelvis, is wide surgical excision with negative margins. Intralesional curettage is only appropriate for some low-grade (Grade I) lesions in the appendicular skeleton.
Question 37:
A 55-year-old patient with long-standing, poorly controlled diabetes mellitus presents with a swollen, erythematous, and warm right foot. Radiographs reveal periarticular fragmentation, bony debris, and early subluxation of the midfoot joints. Laboratory markers for infection are negative. According to the Eichenholtz classification, what is the current stage of this patient's Charcot arthropathy and the most appropriate initial management?
Options:
- Stage 0; rigid internal fixation
- Stage 1; total contact casting and non-weight-bearing
- Stage 2; custom orthotic shoe wear
- Stage 3; midfoot arthrodesis
- Stage 1; immediate operative debridement
Correct Answer: Stage 1; total contact casting and non-weight-bearing
Explanation:
Eichenholtz Stage 1 is the developmental or fragmentation stage of Charcot arthropathy. It is clinically characterized by a hot, red, swollen foot. Radiographically, there is bony fragmentation, joint subluxation/dislocation, and debris. The cornerstone of treatment in the acute fragmentation stage is immediate offloading and immobilization, typically achieved with a total contact cast (TCC) to halt the progression of deformity until the joint coalesces.
Question 38:
A 2-week-old infant is being treated for idiopathic congenital talipes equinovarus using the Ponseti method of serial casting. According to this method, the components of the deformity must be corrected sequentially. Which of the following represents the correct sequence of correction?
Options:
- Cavus, Adductus, Varus, Equinus
- Adductus, Varus, Cavus, Equinus
- Equinus, Varus, Adductus, Cavus
- Cavus, Varus, Adductus, Equinus
- Varus, Cavus, Equinus, Adductus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method addresses clubfoot deformities in the order summarized by the mnemonic CAVE: Cavus, Adductus, Varus, Equinus. The cavus is corrected first by supinating the forefoot to elevate the first ray. Next, the adductus and varus are simultaneously corrected by abducting the forefoot around the fulcrum of the talar head. Finally, the equinus is corrected, which frequently requires a percutaneous Achilles tenotomy.
Question 39:
A 22-year-old collegiate football player presents with recurrent anterior shoulder instability. Advanced imaging reveals a 15% anterior glenoid bone loss and a large, engaging Hill-Sachs lesion. He undergoes an arthroscopic Bankart repair combined with a remplissage procedure. What structure is transferred or tenodesed into the Hill-Sachs defect during a remplissage?
Options:
- Subscapularis tendon
- Infraspinatus tendon and posterior joint capsule
- Supraspinatus tendon
- Long head of the biceps tendon
- Teres major tendon
Correct Answer: Infraspinatus tendon and posterior joint capsule
Explanation:
The remplissage procedure (French for 'to fill') addresses a large, engaging Hill-Sachs lesion that may otherwise lever the humeral head out of the glenoid even after a Bankart repair. It involves capsulotenodesis of the posterior capsule and the infraspinatus tendon into the humeral head defect. This effectively makes the Hill-Sachs lesion extra-articular and prevents it from engaging the anterior glenoid rim during abduction and external rotation.
Question 40:
A 28-year-old man sustains a high-energy closed comminuted fracture of the tibial diaphysis. Six hours post-injury, he complains of disproportionate leg pain that is severely exacerbated by passive stretch of the toes. The clinical suspicion for acute compartment syndrome is high. Which of the following pressure measurements provides the most widely accepted absolute indication for an emergency four-compartment fasciotomy?
Options:
- Absolute compartment pressure greater than 20 mm Hg
- Absolute compartment pressure greater than 25 mm Hg
- Delta pressure (Diastolic blood pressure minus Compartment pressure) less than 30 mm Hg
- Delta pressure (Mean arterial pressure minus Compartment pressure) less than 40 mm Hg
- Delta pressure (Systolic blood pressure minus Compartment pressure) less than 30 mm Hg
Correct Answer: Delta pressure (Diastolic blood pressure minus Compartment pressure) less than 30 mm Hg
Explanation:
The diagnosis of acute compartment syndrome is primarily clinical, but when pressures are measured (especially in obtunded patients or equivocal cases), the 'Delta P' is the most reliable parameter. A Delta P of less than 30 mm Hg (calculated as Diastolic Blood Pressure minus the Absolute Compartment Pressure) indicates critically impaired tissue perfusion and is a firm indication for emergent fasciotomy. Relying solely on absolute pressure numbers (e.g., >30 mmHg) can lead to unnecessary fasciotomies in hypotensive or hypertensive patients.
Question 41:
A 35-year-old male sustains an isolated closed proximal third tibia fracture and is scheduled for intramedullary nailing. The surgeon elects to use a suprapatellar approach instead of a traditional infrapatellar approach. According to current biomechanical and clinical literature, what is the primary advantage of the suprapatellar approach for this specific fracture pattern?
Options:
- Elimination of long-term anterior knee pain
- Easier maintenance of sagittal plane reduction during nail insertion
- Decreased risk of postoperative compartment syndrome
- Lower incidence of deep intra-articular infection
- Avoidance of the infrapatellar branch of the saphenous nerve
Correct Answer: Easier maintenance of sagittal plane reduction during nail insertion
Explanation:
The suprapatellar approach allows the knee to be positioned in semi-extension (15-20 degrees of flexion) rather than the hyperflexion required for an infrapatellar approach. This positioning significantly neutralizes the deforming forces of the extensor mechanism (quadriceps), preventing the common apex anterior (procurvatum) deformity often seen when nailing proximal third tibia fractures, thereby making it easier to maintain sagittal alignment.
Question 42:
A 13-year-old obese boy presents with right thigh pain and a noticeable limp. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Pathologically, the biomechanical failure and slippage in a SCFE occurs through which specific zone of the proximal femoral physis?
Options:
- Reserve zone
- Proliferative zone
- Zone of hypertrophy
- Zone of provisional calcification
- Primary spongiosa
Correct Answer: Zone of hypertrophy
Explanation:
Slipped capital femoral epiphysis (SCFE) represents a Salter-Harris Type I equivalent fracture. The mechanical failure occurs through the zone of hypertrophy of the physis. This zone is mechanically the weakest because the cells are large, lack structural integrity, and the extracellular matrix is diminished.
Question 43:
A 28-year-old carpenter sustains a laceration to the volar aspect of his index finger, resulting in an inability to flex the distal interphalangeal (DIP) joint. During zone II flexor tendon repair, the surgeon must be mindful of the tendon's blood supply. The segmental vascular supply to the flexor tendons within the digital sheath is provided primarily by:
Options:
- Small branches from the palmar digital arteries entering through the vincula
- Direct branches from the superficial palmar arch
- Diffusion from the surrounding synovial fluid exclusively
- Longitudinal vessels arising directly from the muscle belly
- Branches from the common digital arteries piercing the A2 pulley
Correct Answer: Small branches from the palmar digital arteries entering through the vincula
Explanation:
Flexor tendons in Zone II receive nutrition via a dual mechanism: vascular perfusion and synovial diffusion. The vascular supply is provided segmentally by small branches of the digital arteries that enter the dorsal aspect of the tendons through the vincula (vincula brevia and longa).
Question 44:
A 14-year-old gymnast presents with persistent lower back and radicular leg pain. Imaging reveals an L5-S1 isthmic spondylolisthesis with 60% anterior translation of L5 on S1 (Meyerding Grade III). She has failed non-operative management, and surgical reduction with instrumented fusion is planned. Which nerve root is at the highest risk of iatrogenic traction injury during the reduction maneuver?
Options:
Correct Answer: L5
Explanation:
During the surgical reduction of a high-grade L5-S1 spondylolisthesis, the L5 nerve root is at the highest risk for traction injury. As L5 is pulled posteriorly and superiorly to align with S1, the L5 nerve root becomes stretched over the sacral ala.
Question 45:
A 65-year-old male presents with deep bone pain, fatigue, and recent weight loss. Radiographs demonstrate multiple 'punched-out' lytic lesions in his skull, pelvis, and proximal femurs. Based on the most likely diagnosis, which of the following laboratory findings is expected?
Options:
- Monoclonal spike on serum protein electrophoresis (SPEP)
- Elevated serum alkaline phosphatase with normal serum calcium
- Translocation t(11;22)
- Presence of the BCR-ABL fusion gene
- Mutation in the GNAS1 gene
Correct Answer: Monoclonal spike on serum protein electrophoresis (SPEP)
Explanation:
The clinical presentation and 'punched-out' lytic lesions are classic for Multiple Myeloma, the most common primary malignancy of bone in adults. Diagnosis is supported by identifying a monoclonal spike (M-protein) on serum protein electrophoresis (SPEP) or urine protein electrophoresis (UPEP, Bence Jones proteins).
Question 46:
A 55-year-old male with poorly controlled diabetes mellitus presents with a swollen, erythematous, and painless left foot. Radiographs show fragmentation and subluxation of the midfoot. To differentiate between acute Charcot arthropathy and superimposed osteomyelitis, an MRI is obtained. Which of the following MRI findings is highly specific for osteomyelitis in this setting?
Options:
- Diffuse bone marrow edema
- Significant joint effusion
- Subchondral cysts
- Presence of a sinus tract or the 'ghost sign'
- Periarticular soft tissue edema
Correct Answer: Presence of a sinus tract or the 'ghost sign'
Explanation:
Differentiating Charcot arthropathy from osteomyelitis on MRI can be challenging as both present with marrow edema. However, finding a sinus tract extending from a skin ulcer to the bone, or the 'ghost sign' (disappearance of a bone on T1-weighted images that reappears on T2 or post-contrast images), is highly specific for osteomyelitis.
Question 47:
A 60-year-old highly active male undergoes a total hip arthroplasty using a ceramic-on-ceramic (CoC) bearing surface. Two years postoperatively, he complains of a highly audible 'squeaking' sound emanating from his hip during ambulation. What is the most widely recognized biomechanical cause for squeaking in CoC articulations?
Options:
- Use of a larger diameter femoral head
- Femoral stem subsidence
- Acetabular component malposition leading to edge loading
- Inadequate fluid film lubrication due to synovial hyperplasia
- Third-body wear from retained bone cement
Correct Answer: Acetabular component malposition leading to edge loading
Explanation:
Squeaking in ceramic-on-ceramic total hip arthroplasties is a known complication. It is strongly associated with component malposition, specifically excessive cup anteversion or abduction, which leads to edge loading. This edge loading disrupts fluid-film lubrication and causes stripe wear on the ceramic head, generating the high-frequency squeaking sound.
Question 48:
A 22-year-old collegiate baseball pitcher presents with vague posterior shoulder pain and a 25-degree loss of internal rotation (GIRD) compared to the contralateral side. An MRI reveals a type II SLAP tear. The 'peel-back' mechanism is widely considered the primary etiology of this lesion in overhead athletes. During which phase of the throwing motion does the 'peel-back' mechanism occur?
Options:
- Wind-up
- Early cocking
- Late cocking
- Acceleration
- Deceleration
Correct Answer: Late cocking
Explanation:
The 'peel-back' mechanism occurs during the late cocking phase of throwing, where the shoulder is in maximal abduction and external rotation. In this position, the biceps vector shifts posteriorly, creating a torsional force at the base of the biceps anchor that 'peels back' the superior labrum from the glenoid rim.
Question 49:
A 35-year-old male sustains an open fracture of the tibial diaphysis. The orthopedic surgeon considers using recombinant human bone morphogenetic protein-2 (rhBMP-2) on a collagen sponge carrier to augment fracture healing. For which of the following indications is rhBMP-2 specifically FDA-approved in orthopedic trauma?
Options:
- Acute closed tibial shaft fractures treated with intramedullary nailing
- Acute open tibial shaft fractures treated with an intramedullary nail
- Recalcitrant nonunions of the femur
- Acute highly comminuted distal radius fractures
- Scaphoid nonunions with avascular necrosis
Correct Answer: Acute open tibial shaft fractures treated with an intramedullary nail
Explanation:
In orthopedic trauma, rhBMP-2 (Infuse) is specifically FDA-approved for acute open tibial shaft fractures treated with an intramedullary nail, when applied within 14 days of the initial injury. It is not FDA-approved for closed tibia fractures, femoral nonunions, or upper extremity fractures.
Question 50:
A hemodynamically unstable 40-year-old male arrives in the trauma bay with an anteroposterior compression (APC) type III pelvic ring injury. The trauma team applies a pelvic circumferential compression device (binder). To achieve optimal biomechanical reduction of the pelvic volume and control hemorrhage, the binder must be centered over which specific anatomical landmarks?
Options:
- Anterior superior iliac spines
- Iliac crests
- Greater trochanters
- Symphysis pubis
- Umbilicus
Correct Answer: Greater trochanters
Explanation:
For a pelvic binder to be mechanically effective in reducing pelvic volume (especially the posterior ring) and minimizing hemorrhage, it must be centered directly over the greater trochanters. Placement over the iliac crests is a common error and is ineffective at closing the pelvic ring; it can even exacerbate the deformity in some injury patterns.
Question 51:
A 45-year-old construction worker presents with chronic wrist pain and weakness. Radiographs reveal a scaphoid nonunion advanced collapse (SNAC) pattern. The imaging demonstrates arthritic changes involving the entire radioscaphoid joint as well as the capitolunate joint, while the radiolunate joint is completely spared. This pattern corresponds to which stage of a SNAC wrist?
Options:
- Stage I
- Stage II
- Stage III
- Stage IV
- Stage V
Correct Answer: Stage III
Explanation:
SNAC wrist staging is based on the progression of arthritis. Stage I: arthrosis at the radial styloid. Stage II: arthrosis involving the entire radioscaphoid articulation. Stage III: arthrosis advances to involve the capitolunate joint. The radiolunate joint is typically spared until end-stage (Stage IV involves the entire carpus).
Question 52:
A 2-week-old infant presents to the clinic with idiopathic congenital talipes equinovarus (clubfoot). The parents agree to proceed with the Ponseti method of serial casting. According to the foundational principles of the Ponseti technique, what is the correct sequence of deformity correction?
Options:
- Cavus, Adductus, Varus, Equinus
- Equinus, Varus, Adductus, Cavus
- Adductus, Cavus, Varus, Equinus
- Varus, Cavus, Adductus, Equinus
- Cavus, Varus, Adductus, Equinus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method strictly follows a specific order of deformity correction, easily remembered by the mnemonic CAVE: Cavus (corrected by elevating the first ray), Adductus, Varus, and finally Equinus. The equinus is corrected last, often requiring a percutaneous Achilles tenotomy.
Question 53:
A 30-year-old female is involved in a motor vehicle collision and sustains a traumatic spondylolisthesis of the axis (Hangman's fracture). Radiographs show severe angulation of C2 on C3, widening of the posterior C2-C3 disk space, but minimal anterior translation. This pattern is consistent with a Levine and Edwards Type IIA fracture. What is the mechanism of injury for a Type IIA fracture, and what early management step is strictly contraindicated?
Options:
- Flexion-distraction; application of axial traction is contraindicated.
- Hyperextension-axial loading; use of a hard cervical collar is contraindicated.
- Flexion-compression; application of a halo vest is contraindicated.
- Hyperextension-distraction; surgical fusion is contraindicated.
- Axial compression; application of axial traction is contraindicated.
Correct Answer: Flexion-distraction; application of axial traction is contraindicated.
Explanation:
A Levine and Edwards Type IIA Hangman's fracture is characterized by severe angulation with minimal translation and an enlarged posterior disc space. The mechanism of injury is flexion-distraction. Application of axial traction is strictly contraindicated as it will further distract the already completely disrupted C2-C3 disc space and can cause catastrophic spinal cord injury.
Question 54:
A 45-year-old recreational tennis player sustains an acute, complete rupture of his Achilles tendon. He considers non-operative management. Based on recent, high-level randomized controlled trials evaluating functional rehabilitation protocols, how does non-operative management compare to open surgical repair?
Options:
- Non-operative management has a significantly higher rate of re-rupture.
- Non-operative management has a significantly higher rate of deep infection.
- Non-operative management with functional bracing yields equivalent re-rupture rates compared to surgery.
- Non-operative management results in a permanent 50% decrease in plantarflexion strength.
- Non-operative management carries an increased risk of iatrogenic sural nerve injury.
Correct Answer: Non-operative management with functional bracing yields equivalent re-rupture rates compared to surgery.
Explanation:
Recent high-quality evidence (such as the Willits et al. trial) demonstrates that non-operative management of acute Achilles tendon ruptures using an early functional mobilization and bracing protocol results in re-rupture rates that are statistically equivalent to open surgical repair, while avoiding surgical complications like infection and nerve injury.
Question 55:
A 68-year-old female is undergoing a primary total knee arthroplasty for a severe fixed valgus deformity. Intraoperatively, after the standard bone cuts, the trial components are placed, and the lateral side is found to be symmetrically tight in BOTH 90 degrees of flexion and full extension. Which lateral soft-tissue structure is the primary restraint to lateral opening in both flexion and extension, and should be released to balance the knee?
Options:
- Popliteus tendon
- Lateral collateral ligament (LCL)
- Iliotibial (IT) band
- Lateral head of the gastrocnemius
- Biceps femoris tendon
Correct Answer: Lateral collateral ligament (LCL)
Explanation:
In the valgus knee, specific structures affect specific gaps. The iliotibial (IT) band primarily tightens the extension gap. The popliteus tendon primarily tightens the flexion gap. The Lateral Collateral Ligament (LCL) is the primary restraint to varus stress in BOTH flexion and extension. Thus, if both gaps are symmetrically tight laterally, releasing the LCL will increase both gaps.
Question 56:
Articular cartilage relies on a highly specialized architectural organization to resist complex mechanical loads. In the deep (radial) zone of articular cartilage, which statement accurately describes the orientation of Type II collagen fibers and the concentration of proteoglycans?
Options:
- Collagen fibers are parallel to the joint surface; proteoglycan concentration is lowest.
- Collagen fibers are parallel to the joint surface; proteoglycan concentration is highest.
- Collagen fibers are perpendicular to the joint surface; proteoglycan concentration is lowest.
- Collagen fibers are perpendicular to the joint surface; proteoglycan concentration is highest.
- Collagen fibers are randomly oriented; proteoglycan concentration is intermediate.
Correct Answer: Collagen fibers are perpendicular to the joint surface; proteoglycan concentration is highest.
Explanation:
Articular cartilage is divided into zones. In the superficial zone, collagen fibers are parallel to the surface to resist shear, water content is highest, and proteoglycan content is lowest. In the deep (radial) zone, the collagen fibers are oriented perpendicularly to the subchondral bone to resist compressive forces, and the proteoglycan concentration is at its highest.
Question 57:
A 28-year-old male sustains an isolated, grade III posterior cruciate ligament (PCL) injury during a rugby match. He opts for non-operative management. Long-term follow-up studies of isolated, non-operatively treated PCL tears indicate that altered knee kinematics most commonly lead to the premature development of osteoarthritis in which compartments?
Options:
- Medial and patellofemoral compartments
- Lateral and patellofemoral compartments
- Medial and lateral compartments
- Lateral compartment only
- Patellofemoral compartment only
Correct Answer: Medial and patellofemoral compartments
Explanation:
A deficient PCL leads to posterior tibial sag. This altered biomechanics increases contact pressures significantly in both the medial compartment and the patellofemoral joint. Long-term natural history studies of non-operatively treated PCL tears consistently show a high incidence of degenerative changes in the medial and patellofemoral compartments.
Question 58:
A 32-year-old male is admitted with a highly comminuted, closed tibial shaft fracture. Four hours after admission, he complains of unrelenting pain out of proportion to his injury and exquisite pain with passive stretch of his toes. Compartment pressures are measured. What pressure differential (Delta P) is considered the standard clinical threshold indicating the need for emergent four-compartment fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Diastolic blood pressure minus compartment pressure < 30 mmHg
- Systolic blood pressure minus compartment pressure < 40 mmHg
- Mean arterial pressure minus compartment pressure < 30 mmHg
- Diastolic blood pressure minus compartment pressure > 45 mmHg
Correct Answer: Diastolic blood pressure minus compartment pressure < 30 mmHg
Explanation:
Acute compartment syndrome is definitively diagnosed using a pressure differential (Delta P). A Delta P of less than 30 mmHg (calculated as Diastolic Blood Pressure minus the absolute Compartment Pressure) indicates inadequate tissue perfusion and is the standard threshold for emergent fasciotomy.
Question 59:
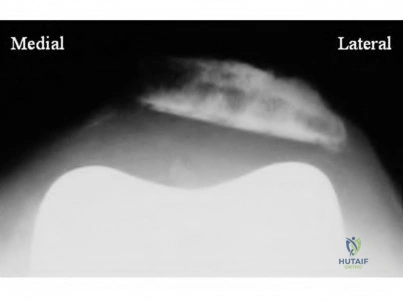
A 42-year-old female presents with an acute finger injury after her hand was struck by a basketball. Radiographs reveal a dorsal avulsion fracture of the distal phalanx involving 45% of the articular surface, accompanied by volar subluxation of the distal phalanx (bony mallet finger). What is the most appropriate management for this specific injury pattern?
Options:
- Aluminum splinting of the DIP joint in slight hyperextension for 6-8 weeks
- Closed reduction and percutaneous pinning (e.g., extension block pinning)
- Immediate DIP joint arthrodesis
- Excision of the fracture fragment and primary tendon advancement
- Buddy taping to the adjacent middle finger for 4 weeks
Correct Answer: Closed reduction and percutaneous pinning (e.g., extension block pinning)
Explanation:
While conservative splinting is appropriate for soft tissue mallet fingers and small avulsion fractures, surgical intervention is indicated for bony mallet fingers when the fracture fragment involves >30-50% of the articular surface or when there is volar subluxation of the distal phalanx. Closed reduction and percutaneous extension block pinning is the standard surgical treatment.
Question 60:
A 60-year-old male presents with a dull, aching pain in his proximal thigh. Radiographs reveal a large, destructive lytic lesion in the proximal femur with intralesional 'popcorn' calcifications. Core needle biopsy confirms a conventional, intermediate-grade (Grade II) chondrosarcoma. What is the standard, definitive treatment for this primary bone tumor?
Options:
- Neoadjuvant chemotherapy followed by wide surgical resection
- Wide surgical resection alone
- Intralesional curettage supplemented with liquid nitrogen cryotherapy
- Primary fractionated external beam radiation therapy
- Radiofrequency ablation combined with cementation
Correct Answer: Wide surgical resection alone
Explanation:
Conventional chondrosarcomas are notoriously resistant to both chemotherapy and radiation therapy due to their low mitotic rate and poor vascularity within the hyaline cartilage matrix. Therefore, the standard of care for Grade II and III conventional chondrosarcomas is wide surgical resection alone.