Full Question & Answer Text (for Search Engines)
Question 1:
A 12-year-old boy with a BMI in the 98th percentile presents with 3 weeks of vague left groin and knee pain. He walks with an antalgic, externally rotated gait. Radiographs confirm a stable left slipped capital femoral epiphysis (SCFE). Which of the following is the strongest indication for prophylactic in situ pinning of his asymptomatic right hip?
Options:
- Age greater than 14 years at initial presentation
- Posterior sloping angle of 40 degrees on the affected side
- Concomitant diagnosis of hypothyroidism
- Unilateral slip angle greater than 60 degrees
- BMI greater than the 95th percentile
Correct Answer: Concomitant diagnosis of hypothyroidism
Explanation:
Endocrine disorders (such as hypothyroidism, panhypopituitarism, or renal osteodystrophy) and previous radiation therapy are strong indications for prophylactic contralateral pinning in SCFE due to the exceptionally high risk of a subsequent contralateral slip. While young age (e.g., < 10 years) and open triradiate cartilage are also considered risk factors for contralateral disease, a high BMI alone or the severity of the unilateral slip does not represent an absolute indication for prophylactic pinning.
Question 2:
A 65-year-old male undergoes a primary total hip arthroplasty using a titanium alloy (Ti-6Al-4V) femoral stem and a cobalt-chromium (CoCr) alloy femoral head. Five years later, he presents with progressive groin pain and a large cystic mass on MRI, without evidence of infection. Revision surgery reveals black debris and damage at the head-neck taper junction. What is the primary pathophysiologic mechanism of this wear pattern?
Options:
- Galvanic corrosion exclusively
- Mechanically assisted crevice corrosion
- Intergranular corrosion
- Pitting corrosion
- Stress corrosion cracking
Correct Answer: Mechanically assisted crevice corrosion
Explanation:
The scenario describes trunnionosis, which is primarily caused by mechanically assisted crevice corrosion (MACC), also known as fretting and crevice corrosion. Micro-motion at the modular junction (fretting) disrupts the protective passivating oxide layer of the metals. Because this occurs in a restricted space (crevice), local fluid chemistry changes (decreased pH, decreased oxygen), which accelerates the corrosion process. While galvanic corrosion can play a minor role when dissimilar metals are used, MACC is the dominant mechanism for taper failure in modern THA.
Question 3:
A 42-year-old male presents to the trauma bay following a high-speed motorcycle collision. He is diagnosed with a closed extra-articular scapular body fracture. According to current literature, which of the following is considered an indication for operative management of this fracture?
Options:
- Medial displacement of the glenoid fragment of 5 mm
- Angular deformity of the scapular body of 15 degrees
- A glenopolar angle of 35 degrees
- An associated undisplaced middle-third clavicle fracture
- Medial displacement of the glenoid fragment greater than 20 mm
Correct Answer: Medial displacement of the glenoid fragment greater than 20 mm
Explanation:
Indications for operative fixation of extra-articular scapular fractures include severe medialization of the glenoid fragment (typically >20 mm, though some suggest >10 mm coupled with other factors), significant angular deformity (>45 degrees), or a glenopolar angle < 22 degrees. An undisplaced clavicle fracture (forming an undisplaced floating shoulder) is generally managed non-operatively. Medialization of >20 mm represents significant displacement that alters the resting length of the rotator cuff and periscapular musculature, warranting fixation.
Question 4:
During a total hip arthroplasty utilizing the direct anterior approach (Smith-Petersen interval), the surgeon must be cautious of a nerve that typically exits the pelvis medial to the anterior superior iliac spine (ASIS) and crosses the surgical field. Injury to this nerve will result in which of the following deficits?
Options:
- Weakness in hip abduction
- Weakness in knee extension
- Sensory loss over the lateral aspect of the thigh
- Sensory loss over the medial aspect of the thigh
- Weakness in hip external rotation
Correct Answer: Sensory loss over the lateral aspect of the thigh
Explanation:
The lateral femoral cutaneous nerve (LFCN) is at risk during the direct anterior approach to the hip. It provides pure sensation to the lateral and anterolateral aspect of the thigh. It does not provide motor innervation. Weakness in hip abduction implies superior gluteal nerve injury, knee extension points to the femoral nerve, medial thigh sensation to the obturator nerve, and hip external rotation involves several short external rotators and associated nerves.
Question 5:
A 72-year-old male presents with worsening hand clumsiness, frequent falls, and a broad-based gait. Physical examination reveals a positive Hoffmann sign bilaterally. An MRI of the cervical spine is obtained. Which of the following MRI signal characteristics within the spinal cord is most strongly associated with a poor prognosis for neurologic recovery following surgical decompression?
Options:
- Focal T2 hyperintensity without T1 changes
- Multisegmental T2 hyperintensity without T1 changes
- Combined T1 hypointensity and T2 hyperintensity
- Ligamentum flavum hypertrophy > 5 mm
- Modic Type I changes in the adjacent vertebral bodies
Correct Answer: Combined T1 hypointensity and T2 hyperintensity
Explanation:
In the setting of cervical spondylotic myelopathy (CSM), MRI changes in the spinal cord can have prognostic significance. T2 hyperintensity alone generally signifies edema and reversible changes, portending a relatively fair to good prognosis. However, T1 hypointensity combined with T2 hyperintensity reflects myelomalacia, cystic necrosis, and permanent spinal cord damage, which is a strong predictor of poor functional outcome and limited neurologic recovery post-operatively.
Question 6:
A 22-year-old collegiate soccer player requires revision anterior cruciate ligament (ACL) reconstruction. The surgeon decides to use a bone-patellar tendon-bone (BPTB) allograft. Which of the following sterilization methods most significantly compromises the biomechanical structural properties of the allograft?
Options:
- Ethylene oxide treatment
- Gamma irradiation with 1.2 Mrad
- Gamma irradiation with >2.5 Mrad
- Fresh-freezing at -80°C
- Lyophilization (freeze-drying)
Correct Answer: Gamma irradiation with >2.5 Mrad
Explanation:
High-dose gamma irradiation (>2.5 Mrad or 25 kGy) is required to reliably eliminate the HIV virus and other pathogens from allografts. However, irradiation at or above this level causes significant dose-dependent deterioration of the mechanical and structural properties of the graft (disruption of collagen cross-links). Lower doses (1.0-1.2 Mrad) do not significantly affect biomechanical properties but are less effective at viral sterilization. Fresh-freezing does not alter biomechanics. Ethylene oxide causes an inflammatory response and is largely abandoned for graft sterilization.
Question 7:
A 24-year-old male falls on an outstretched hand and sustains a proximal pole scaphoid fracture. This specific fracture location has a notoriously high rate of avascular necrosis and nonunion. Which vessel is the predominant source of blood supply to the proximal pole of the scaphoid?
Options:
- Superficial palmar arch
- Volar carpal branch of the radial artery
- Dorsal carpal branch of the radial artery
- Anterior interosseous artery
- Deep palmar arch
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The primary blood supply to the scaphoid is retrograde. The dorsal carpal branch of the radial artery enters the dorsal ridge of the scaphoid at the waist and supplies the proximal 70-80% of the bone. A fracture through the proximal pole or waist often disrupts this retrograde flow, putting the proximal pole at high risk for avascular necrosis. The volar carpal branch supplies only the distal 20-30% of the bone.
Question 8:
A 35-year-old female sustains a midfoot sprain. Weight-bearing radiographs demonstrate subtle widening between the medial and middle cuneiforms. The true Lisfranc ligament acts as the primary stabilizer of the second tarsometatarsal joint. What are the specific anatomic attachments of the Lisfranc ligament?
Options:
- Medial aspect of the medial cuneiform to the base of the first metatarsal
- Lateral aspect of the medial cuneiform to the base of the second metatarsal
- Anterior aspect of the middle cuneiform to the base of the second metatarsal
- Medial aspect of the intermediate cuneiform to the base of the first metatarsal
- Plantar aspect of the lateral cuneiform to the base of the third metatarsal
Correct Answer: Lateral aspect of the medial cuneiform to the base of the second metatarsal
Explanation:
The Lisfranc ligament is an interosseous ligament that connects the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. It is the strongest and most important ligament for stabilizing the second tarsometatarsal joint. There is no direct ligamentous connection between the base of the first and second metatarsals.
Question 9:
A 16-year-old male presents with a painful mass near his distal femur. Radiographs show a destructive, permeative lesion with a 'sunburst' periosteal reaction. Biopsy confirms osteosarcoma. Following standard neoadjuvant chemotherapy and wide surgical resection, which of the following is the most significant prognostic factor for long-term overall survival?
Options:
- Initial size of the primary tumor
- Anatomic location of the tumor
- Percentage of tumor necrosis in the resected specimen
- Serum alkaline phosphatase level at initial presentation
- Use of limb salvage surgery versus amputation
Correct Answer: Percentage of tumor necrosis in the resected specimen
Explanation:
In the treatment of high-grade osteosarcoma, the histologic response of the tumor to neoadjuvant chemotherapy (measured by the percentage of tumor necrosis in the definitive surgical specimen) is widely considered the single most important prognostic factor for long-term survival. A good response is typically defined as >90% or >95% necrosis. Limb salvage versus amputation does not impact overall survival, provided negative surgical margins are obtained.
Question 10:
A 45-year-old patient with a highly comminuted diaphyseal femur fracture is treated with a bridging locked intramedullary nail. The resulting mechanical construct provides relative stability. Which of the following predominantly characterizes the bone healing process in this mechanical environment?
Options:
- Primary bone healing via Haversian remodeling and cutting cones
- Secondary bone healing via endochondral ossification
- Intramembranous ossification directly without a cartilage intermediate
- Creeping substitution
- Appositional direct bone growth only
Correct Answer: Secondary bone healing via endochondral ossification
Explanation:
A bridging construct (such as an IM nail or a bridge plate for a comminuted fracture) provides relative stability rather than absolute stability. This allows for micromotion at the fracture site, which stimulates secondary bone healing. Secondary bone healing is characterized by the formation of a soft callus (cartilage intermediate) that subsequently undergoes endochondral ossification into woven bone and then remodeling into lamellar bone. Primary bone healing (cutting cones) requires absolute stability (e.g., lag screw and compression plating).
Question 11:
A 28-year-old male sustains a pelvic ring injury after a fall from height. Radiographs and CT show a symphyseal diastasis of 3.5 cm. The anterior sacroiliac (SI) ligaments, sacrotuberous, and sacrospinous ligaments are disrupted, but the posterior SI ligaments remain intact. Based on the Young-Burgess classification, what is the correct diagnosis?
Options:
- Anteroposterior Compression I (APC I)
- Anteroposterior Compression II (APC II)
- Anteroposterior Compression III (APC III)
- Lateral Compression II (LC II)
- Lateral Compression III (LC III)
Correct Answer: Anteroposterior Compression II (APC II)
Explanation:
The Young-Burgess classification describes the mechanism of injury for pelvic fractures. Anteroposterior Compression II (APC II) injuries are characterized by symphyseal diastasis > 2.5 cm with tearing of the anterior SI ligaments, sacrotuberous, and sacrospinous ligaments. Crucially, the posterior SI ligaments are intact, meaning the hemipelvis is rotationally unstable but vertically stable. APC III involves complete disruption of both anterior and posterior SI ligaments, resulting in both rotational and vertical instability.
Question 12:
A 4-month-old female is diagnosed with Developmental Dysplasia of the Hip (DDH). She is placed in a Pavlik harness. To successfully maintain hip reduction while preventing iatrogenic avascular necrosis, the Pavlik harness safely restricts which of the following combined movements?
Options:
- Flexion and abduction
- Extension and adduction
- Flexion and internal rotation
- Extension and abduction
- Flexion and external rotation
Correct Answer: Extension and adduction
Explanation:
The Pavlik harness is a dynamic flexion-abduction orthosis used to treat DDH. It maintains the hip in flexion and limits adduction and extension, thereby stabilizing the reduction. It does not rigidly lock the hip in position but acts as a tether to prevent extension and adduction (the positions that favor dislocation). Excessive forced abduction is avoided as it significantly increases the risk of iatrogenic avascular necrosis of the femoral head.
Question 13:
A 68-year-old male complains of bilateral posterior leg pain when walking. You are attempting to differentiate neurogenic claudication (due to lumbar spinal stenosis) from vascular claudication. Which of the following is most characteristic of neurogenic claudication?
Options:
- The pain typically propagates from distal to proximal during walking
- Symptoms are consistently worsened by stationary cycling
- Normal pedal pulses with symptoms relieved by lumbar flexion (e.g., sitting or leaning forward)
- Pain typically resolves quickly upon simply standing perfectly still
- Pain distance is extremely predictable and invariable each time the patient walks
Correct Answer: Normal pedal pulses with symptoms relieved by lumbar flexion (e.g., sitting or leaning forward)
Explanation:
Neurogenic claudication classicially improves with lumbar flexion (e.g., leaning over a shopping cart, sitting) because flexion increases the cross-sectional area of the spinal canal, relieving neural compression. Stationary cycling in a flexed posture typically does not reproduce symptoms (unlike vascular claudication, which is tied purely to muscle oxygen demand). Neurogenic pain usually radiates proximal to distal, whereas vascular often radiates distal to proximal (calf first). Normal pedal pulses further favor a neurogenic etiology.
Question 14:
A 70-year-old female undergoes a primary posterior-stabilized total knee arthroplasty. Intraoperatively, the surgeon realizes that the knee is well-balanced in extension but unacceptably tight in flexion. Which of the following technical errors most frequently causes an isolated tight flexion gap?
Options:
- Excessive distal femoral resection
- Oversizing the femoral component in the anteroposterior (AP) dimension
- Undersizing the femoral component in the anteroposterior (AP) dimension
- Increasing the posterior slope of the tibial cut
- Recessing the joint line (patella alta)
Correct Answer: Oversizing the femoral component in the anteroposterior (AP) dimension
Explanation:
The flexion gap in TKA is dictated primarily by the size of the posterior femoral condyles and the AP dimension of the femoral component. Oversizing the femoral component in the AP dimension (and specifically adding posterior offset) stuffs the posterior joint space, leading to a tight flexion gap. Excessive distal femoral resection affects the extension gap (making it loose). Increasing the posterior tibial slope would actually increase (loosen) the flexion gap.
Question 15:
A 19-year-old athlete undergoes an arthroscopic partial meniscectomy and meniscal repair. Understanding the vascular anatomy of the meniscus is crucial for deciding which tears are repairable. Which anatomical zone of the meniscus possesses the highest intrinsic healing potential?
Options:
- The inner third (avascular zone)
- The middle third (red-white zone)
- The peripheral third (red-red zone)
- The white-white zone
- The anterior horn exclusively
Correct Answer: The peripheral third (red-red zone)
Explanation:
The blood supply to the meniscus comes from the periphery via the perimeniscal capillary plexus (branches of the superior and inferior genicular arteries). The peripheral 10-25% of the meniscus is highly vascularized (the red-red zone) and has the greatest healing potential after repair. The middle third (red-white zone) has partial vascularity with intermediate healing potential. The inner third (white-white zone) is entirely avascular and relies on diffusion for nutrition, making repairs in this zone generally unsuccessful.
Question 16:
A 55-year-old female with severe, long-standing carpal tunnel syndrome is scheduled for an open carpal tunnel release. To avoid iatrogenic injury, the surgeon must be aware of the anatomic variations of the recurrent motor branch of the median nerve. What is the most common anatomic relationship of the recurrent motor branch to the transverse carpal ligament?
Options:
- Extraligamentous with a recurrent course
- Subligamentous
- Transligamentous
- Preligamentous
- Ulnar to the hook of the hamate
Correct Answer: Extraligamentous with a recurrent course
Explanation:
The extraligamentous origin with a recurrent course is the most common anatomic variation of the recurrent motor branch of the median nerve, occurring in approximately 46-90% of cases (historically cited around 50-80% in various studies). In this pattern, the branch arises distal to the transverse carpal ligament and loops back to innervate the thenar muscles. Subligamentous (arising within the tunnel) and transligamentous (piercing the ligament) are less common but put the nerve at higher risk of direct injury during ligament division if the surgeon strays too far radially.
Question 17:
A 42-year-old male sustains an acute, closed mid-substance Achilles tendon rupture playing basketball. He is evaluating operative versus nonoperative management. Based on high-level randomized controlled trials employing modern early functional rehabilitation protocols, which of the following is true?
Options:
- Operative treatment offers a significantly lower rerupture rate than nonoperative treatment
- Operative treatment is associated with higher overall complication rates, such as deep infection
- Nonoperative treatment results in significantly less plantarflexion strength long-term
- Nonoperative treatment necessitates strict immobilization in a cast for a minimum of 12 weeks
- Operative treatment completely eliminates the risk of tendon elongation
Correct Answer: Operative treatment is associated with higher overall complication rates, such as deep infection
Explanation:
Recent high-quality randomized controlled trials (such as Willits et al.) have demonstrated that when modern early functional weight-bearing rehabilitation protocols are used, the rerupture rates between nonoperative and operative treatment of acute Achilles tendon ruptures are statistically similar (often both around 3-5%). However, operative treatment carries an increased risk of surgical complications, including infection, wound breakdown, and sural nerve injury. Plantarflexion strength outcomes are generally comparable with early functional rehab.
Question 18:
A 32-year-old female presents with wrist pain. Radiographs demonstrate an expansile, eccentrically located lytic lesion in the distal radius epiphysis without a sclerotic rim. Biopsy confirms a giant cell tumor of bone. Because the tumor involves the joint extensively, neoadjuvant medical therapy is planned to facilitate joint-sparing surgery. The primary medical treatment (denosumab) for this condition targets which of the following?
Options:
- Receptor activator of nuclear factor-kappa B (RANK) receptor
- Receptor activator of nuclear factor-kappa B ligand (RANKL)
- Osteoprotegerin (OPG)
- Macrophage colony-stimulating factor (M-CSF)
- Vascular endothelial growth factor (VEGF)
Correct Answer: Receptor activator of nuclear factor-kappa B ligand (RANKL)
Explanation:
Giant cell tumor of bone is characterized by neoplastic mononuclear stromal cells that express RANKL, which subsequently recruits and activates normal osteoclast-like giant cells that express RANK, leading to bone resorption. Denosumab is a human monoclonal antibody that binds directly to RANKL (not the RANK receptor itself), preventing its interaction with RANK. This inhibits osteoclast-like giant cell formation and survival, leading to tumor consolidation and intralesional ossification.
Question 19:
A 55-year-old male is undergoing an arthroscopic rotator cuff repair. A thorough understanding of the anatomic footprint of the rotator cuff is critical for successful anatomic restoration. According to anatomical studies (e.g., Mochizuki et al.), which of the following tendons has the largest insertion footprint on the greater tuberosity?
Options:
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
- Long head of the biceps
Correct Answer: Infraspinatus
Explanation:
Historically, the supraspinatus was thought to have a larger insertion on the greater tuberosity. However, landmark anatomical studies by Mochizuki et al. demonstrated that the infraspinatus footprint is substantially larger than that of the supraspinatus. The infraspinatus sweeps anteriorly and occupies a significant portion of the greater tuberosity (the lateral aspect), while the supraspinatus insertion is restricted to a much smaller anteromedial area of the greater tuberosity. The subscapularis inserts on the lesser tuberosity.
Question 20:
A 25-year-old male sustains a comminuted tibia fracture and is treated with an intramedullary nail. Twelve hours postoperatively, he complains of severe, unrelenting leg pain out of proportion to the injury, unrelieved by IV opioids. He has pain with passive stretch of his great toe. Compartment pressures are measured. Which of the following parameters provides the most reliable indication for emergent four-compartment fasciotomy?
Options:
- Absolute anterior compartment pressure > 20 mmHg
- Absolute anterior compartment pressure > 30 mmHg
- Diastolic blood pressure minus compartment pressure < 30 mmHg
- Mean arterial pressure minus compartment pressure < 30 mmHg
- Systolic blood pressure minus compartment pressure < 30 mmHg
Correct Answer: Diastolic blood pressure minus compartment pressure < 30 mmHg
Explanation:
The clinical diagnosis of acute compartment syndrome requires a high index of suspicion, with pain out of proportion and pain with passive stretch being early signs. When utilizing compartment pressure monitoring, the delta pressure (ΔP) is the most accurate diagnostic threshold. A ΔP (Diastolic Blood Pressure minus Absolute Compartment Pressure) of less than 30 mmHg is the widely accepted criteria for surgical intervention (fasciotomy). Relying on an absolute pressure > 30 mmHg can lead to unnecessary fasciotomies, especially in hypertensive patients.
Question 21:
A 35-year-old male is brought to the trauma bay following a high-speed motorcycle crash. His heart rate is 125 bpm, and his blood pressure is 80/50 mmHg. An anteroposterior radiograph of the pelvis reveals a widened pubic symphysis (>2.5 cm) and significant widening of the bilateral sacroiliac joints. A pelvic binder is appropriately applied, and he receives 2 units of uncrossmatched blood. A FAST exam is negative. He remains hemodynamically unstable. Which of the following is the most appropriate next step in management?
Options:
- Preperitoneal pelvic packing
- Retrograde urethrogram
- Application of a second pelvic binder
- Exploratory laparotomy
- Immediate open reduction internal fixation of the anterior ring
Correct Answer: Preperitoneal pelvic packing
Explanation:
This patient has an Anteroposterior Compression Type III (APC III) pelvic ring injury and is in hemorrhagic shock. In a hemodynamically unstable patient with a pelvic ring injury and a negative FAST (ruling out massive intra-abdominal hemorrhage), the source of bleeding is presumed to be the pelvis (often venous or cancellous bone, though arterial bleeding can occur). Preperitoneal pelvic packing or angioembolization (depending on institutional protocol and immediate availability) are the appropriate next steps after mechanical stabilization with a binder. Exploratory laparotomy is incorrect as the FAST is negative.
Question 22:
During a posterior-stabilized Total Knee Arthroplasty (TKA), the surgeon uses spacer blocks to assess the flexion and extension gaps. The extension gap is symmetric and perfectly balanced. However, the flexion gap is unacceptably tight, preventing the knee from flexing past 80 degrees without lifting the joint off the tibia. What is the most appropriate intraoperative adjustment to correct this mismatch?
Options:
- Resect an additional 2 mm of distal femur
- Decrease the femoral component size (using a posterior referencing system)
- Increase the thickness of the polyethylene insert
- Release the posterior capsule
- Resect an additional 2 mm of proximal tibia
Correct Answer: Decrease the femoral component size (using a posterior referencing system)
Explanation:
A tight flexion gap with a balanced extension gap implies that the posterior condyles of the femur are projecting too far posteriorly, tightening the collateral ligaments only in flexion. Downsizing the femoral component using a posterior referencing system will result in a thicker posterior femoral cut, effectively opening the flexion gap without altering the distal femoral cut (which controls the extension gap). Resecting more proximal tibia would loosen both gaps equally. Resecting more distal femur would loosen only the extension gap.
Question 23:
A 45-year-old manual laborer presents with chronic, progressive right wrist pain. Radiographs demonstrate a nonunion of the scaphoid with advanced arthritic changes narrowing the radioscaphoid articulation as well as the scaphocapitate joint. The radiolunate joint is completely preserved. What is the correct classification and an appropriate surgical treatment for this condition?
Options:
- SNAC I; Radial styloidectomy
- SNAC II; Proximal row carpectomy
- SNAC III; Scaphoid excision and 4-corner fusion
- SNAC III; Total wrist arthrodesis
- SLAC II; Scapholunate ligament repair
Correct Answer: SNAC II; Proximal row carpectomy
Explanation:
Scaphoid Nonunion Advanced Collapse (SNAC) progresses in a predictable pattern. SNAC I involves only the radial styloid and distal scaphoid pole. SNAC II involves the entire radioscaphoid joint and the scaphocapitate joint. SNAC III progresses to periscaphoid arthritis (including the capitolunate joint). The radiolunate joint is characteristically spared. A condition involving the radioscaphoid and scaphocapitate joints is SNAC II. Acceptable salvage procedures for SNAC II include proximal row carpectomy (PRC) or scaphoid excision with 4-corner fusion.
Question 24:
A 14-year-old boy presents with a painful, swollen thigh. Radiographs reveal a permeative, diaphyseal lesion of the femur with an extensive 'onion-skin' periosteal reaction. A core needle biopsy is performed. Which of the following chromosomal translocations and resulting fusion proteins is most characteristic of this tumor?
Options:
- t(X;18); SYT-SSX
- t(11;22); EWS-FLI1
- t(12;16); TLS-CHOP
- t(2;13); PAX3-FKHR
- t(9;22); BCR-ABL
Correct Answer: t(11;22); EWS-FLI1
Explanation:
The clinical and radiographic presentation is classic for Ewing sarcoma. Ewing sarcoma is a small round blue cell tumor most commonly arising in the diaphysis of long bones in children and adolescents. It is defined by the t(11;22)(q24;q12) translocation in ~85% of cases, which produces the EWS-FLI1 fusion protein. SYT-SSX is associated with synovial sarcoma. TLS-CHOP is seen in myxoid liposarcoma. PAX3-FKHR is seen in alveolar rhabdomyosarcoma.
Question 25:
A 12-year-old obese male presents with left knee pain and an antalgic gait. Physical examination reveals an obligate external rotation of the left hip as it is passively flexed. Radiographs confirm a displaced Slipped Capital Femoral Epiphysis (SCFE) on the left. Prophylactic percutaneous pinning of the contralateral (asymptomatic) hip is most strongly indicated if the patient has a history of which of the following conditions?
Options:
- Hyperthyroidism
- Type 1 Diabetes Mellitus
- Hypothyroidism
- Addison's disease
- Hyperparathyroidism
Correct Answer: Hypothyroidism
Explanation:
Prophylactic pinning of the contralateral hip in SCFE is controversial but is generally strongly recommended in patients with an underlying endocrinopathy or metabolic bone disease (e.g., hypothyroidism, renal osteodystrophy, growth hormone deficiency), as well as in patients presenting at an unusually young age (often defined as <10 years old). These patients have an extremely high risk (up to 100% in some metabolic conditions) of developing a contralateral slip.
Question 26:
A 68-year-old male presents with worsening hand clumsiness, frequent falls, and a broad-based shuffling gait. Examination reveals hyperreflexia and a positive Hoffmann's sign bilaterally. MRI demonstrates severe multilevel cervical stenosis from C3 to C6 with intramedullary T2 signal hyperintensity. Standing radiographs show a rigid, 25-degree cervical kyphotic deformity. What is the most appropriate surgical approach?
Options:
- Anterior cervical discectomy and fusion (ACDF)
- Posterior cervical laminectomy without fusion
- Cervical laminoplasty
- Combined anterior corpectomy and posterior instrumented fusion
- Posterior cervical foraminotomy
Correct Answer: Combined anterior corpectomy and posterior instrumented fusion
Explanation:
This patient has cervical spondylotic myelopathy with a rigid kyphotic deformity. A posterior-only indirect decompression (laminectomy or laminoplasty) is contraindicated in the setting of rigid kyphosis because the spinal cord will remain draped over the anterior compressive pathology (it cannot 'drift back'). An anterior approach allows direct decompression, but multilevel anterior corpectomies alone carry a high risk of graft dislodgment and pseudarthrosis. Therefore, a combined anterior-posterior approach (anterior decompression/reconstruction + posterior instrumented fusion) provides the most definitive decompression and mechanical stability.
Question 27:
A 24-year-old male presents to the emergency department after a high-velocity knee dislocation. Following closed reduction, you document an absent pedal pulse, and the vascular surgeon performs an emergent popliteal artery repair. Postoperatively, the patient demonstrates an inability to extend his great toe and reports numbness isolated to the dorsal first web space of the foot. Which of the following knee structures is most likely concomitantly injured?
Options:
- Posteromedial corner
- Anterolateral ligament
- Posterolateral corner
- Superficial peroneal nerve
- Medial collateral ligament
Correct Answer: Posterolateral corner
Explanation:
The inability to extend the great toe (EHL weakness) and numbness in the first dorsal web space indicate a deep peroneal nerve palsy. In the setting of a multi-ligament knee injury or dislocation, peroneal nerve injury is highly associated with damage to the Posterolateral Corner (PLC) of the knee, as the common peroneal nerve wraps around the fibular neck in close proximity to the biceps femoris and LCL.
Question 28:
A 58-year-old male with poorly controlled type 2 diabetes presents with a unilaterally swollen, red, and warm right foot. There are no open ulcers. Radiographs show severe fragmentation of the tarsometatarsal joints, periarticular debris, and joint subluxation. ESR and CRP are within normal limits. Based on the Eichenholtz classification, what stage is this patient in, and what is the standard initial treatment?
Options:
- Stage 0; Custom diabetic footwear
- Stage 1; Total contact casting
- Stage 2; Midfoot arthrodesis
- Stage 3; Charcot Restraint Orthotic Walker (CROW)
- Stage 1; Intravenous antibiotics and ID
Correct Answer: Stage 1; Total contact casting
Explanation:
The clinical and radiographic presentation is classic for acute Charcot neuroarthropathy. The normal inflammatory markers help distinguish this from acute osteomyelitis. Eichenholtz Stage 1 (Developmental/Fragmentation) is characterized by erythema, swelling, warmth, and radiographs showing osteopenia, fragmentation, joint subluxation, and debris. The gold standard treatment for Stage 1 Charcot is strict immobilization and offloading, typically using a total contact cast (TCC) until the erythema, warmth, and swelling resolve, and radiographs show consolidation (Stage 2/3).
Question 29:
Articular cartilage is a highly specialized tissue designed to withstand repetitive compressive forces. When evaluating the structural and biochemical composition of articular cartilage across its depth, which zone is characterized by having the highest concentration of water, the lowest concentration of proteoglycans, and collagen fibrils aligned parallel to the joint surface?
Options:
- Superficial zone
- Middle (transitional) zone
- Deep (radial) zone
- Tidemark
- Calcified cartilage zone
Correct Answer: Superficial zone
Explanation:
The superficial (tangential) zone makes up the top 10-20% of articular cartilage. It is designed to resist sheer stress. It has the highest water content, the lowest proteoglycan concentration, and densely packed type II collagen fibers oriented parallel to the articular surface. The deep zone, in contrast, has the highest concentration of proteoglycans, the lowest water content, and collagen fibers oriented perpendicular to the joint surface to resist compressive loads.
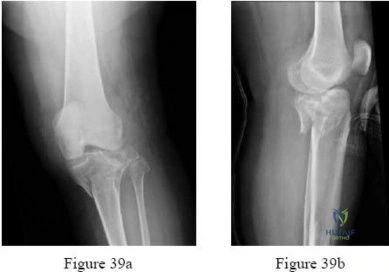
Question 30:
A 42-year-old male presents with severe knee pain after falling off a ladder. An AP radiograph of the knee reveals a depressed fracture fragment in the lateral articular surface along with an oblique fracture line exiting the lateral metaphysis. Which of the following Schatzker classifications accurately describes this fracture, and what is the most commonly associated intra-articular soft tissue injury?
Options:
- Schatzker I; Medial meniscus
- Schatzker II; Lateral meniscus
- Schatzker III; Anterior cruciate ligament
- Schatzker IV; Lateral meniscus
- Schatzker V; Posterior cruciate ligament
Correct Answer: Schatzker II; Lateral meniscus
Explanation:
A split-depression fracture of the lateral tibial plateau is classified as a Schatzker II fracture. This is the most common pattern of tibial plateau fracture. It is highly associated with meniscal injuries, specifically lateral meniscus tears, which occur in approximately 50-70% of cases and often require simultaneous repair or partial meniscectomy during ORIF.
Question 31:
A 2-year-old girl is evaluated for severe bowing of her lower extremities. You suspect infantile Blount's disease rather than physiologic bowing. Which of the following radiographic parameters is the most reliable predictor that the deformity will progress to clinical Blount's disease and likely require intervention?
Options:
- Tibiofemoral angle > 10 degrees
- Metaphyseal-diaphyseal angle (Drennan angle) > 16 degrees
- Mechanical axis deviation > 2 cm
- Epiphyseal-metaphyseal angle > 20 degrees
- Neck-shaft angle < 120 degrees
Correct Answer: Metaphyseal-diaphyseal angle (Drennan angle) > 16 degrees
Explanation:
The metaphyseal-diaphyseal angle (Drennan's angle) is used to differentiate physiologic genu varum from infantile Blount's disease. An angle > 16 degrees is highly predictive of progressive infantile Blount's disease. An angle < 10 degrees is typical for physiologic bowing, which usually resolves spontaneously. Angles between 10 and 16 degrees represent a gray area requiring close clinical and radiographic observation.
Question 32:
A 62-year-old male with a metal-on-polyethylene total hip arthroplasty (THA) placed 8 years ago presents with insidious onset of anterior groin pain. Hip aspiration reveals cloudy fluid with normal leukocyte counts and negative cultures. MRI with metal artifact reduction sequence (MARS) demonstrates a cystic mass adjacent to the greater trochanter. Serum cobalt levels are markedly elevated, while chromium levels are normal. What is the most likely etiology of this patient's presentation?
Options:
- Adverse local tissue reaction secondary to trunnionosis
- Polyethylene wear osteolysis
- Periprosthetic joint infection
- Aseptic loosening of the femoral stem
- Metal-on-metal articulation wear
Correct Answer: Adverse local tissue reaction secondary to trunnionosis
Explanation:
The patient has a metal-on-polyethylene bearing but demonstrates systemic and local signs of metal toxicity (pseudotumor/ALTR). Elevated serum cobalt out of proportion to chromium in the setting of a non-metal-on-metal bearing is the hallmark of mechanically assisted crevice corrosion (trunnionosis) at the modular head-neck junction. Polyethylene wear causes osteolysis but not elevated cobalt or classic ALTR cystic masses. Infection is ruled out by the negative aspirate.
Question 33:
A 21-year-old collegiate rugby player presents with recurrent anterior shoulder instability. He has had 5 dislocations over the past year. A 3D reconstructed CT scan of the shoulder reveals an inverted-pear glenoid with an estimated 28% anterior inferior bone loss. Which of the following surgical interventions provides the most reliable biomechanical stability and lowest recurrence rate for this specific patient?
Options:
- Arthroscopic Bankart repair
- Open Bankart repair with inferior capsular shift
- Latarjet procedure
- Remplissage
- Glenoid resurfacing with allograft
Correct Answer: Latarjet procedure
Explanation:
Anterior glenoid bone loss exceeding 20-25% (often described visually as an 'inverted pear' glenoid) is a critical threshold in anterior shoulder instability. Soft tissue procedures alone, such as arthroscopic or open Bankart repairs, have unacceptably high failure rates in this setting. The Latarjet procedure (transfer of the coracoid process with the attached conjoint tendon to the anterior glenoid) reconstructs the bony arc and provides a dynamic sling effect, making it the standard of care for critical glenoid bone loss.
Question 34:
Following a primary repair of a Zone II flexor digitorum profundus (FDP) laceration, a hand surgeon opts for a specific postoperative rehabilitation protocol to prevent tendon adhesions. The protocol employs a dorsal blocking splint, and the patient actively extends the digit against the resistance of a rubber band attached to the fingernail, which then passively pulls the digit back into flexion. Which protocol does this describe?
Options:
- Duran protocol
- Kleinert protocol
- Early active motion protocol
- Modified Chow protocol
- Immobilization protocol
Correct Answer: Kleinert protocol
Explanation:
The Kleinert protocol utilizes active extension and passive flexion via rubber band traction while the hand is in a dorsal block splint. The Duran protocol involves controlled passive extension and passive flexion exercises performed by the patient or therapist. Early active motion protocols (e.g., Belfast, Indiana) allow true active flexion and extension within strict limits, minimizing adhesions but requiring a stronger initial core suture construct (e.g., 4 or 6 strands).
Question 35:
A 32-year-old female presents with knee pain. Radiographs show a large, eccentric, purely lytic, expansile lesion in the distal femoral epiphysis extending to the subchondral bone. A biopsy reveals numerous multinucleated giant cells in a stroma of mononuclear cells. For advanced, unresectable cases, or as a neoadjuvant therapy to facilitate intralesional curettage, which of the following monoclonal antibodies is an FDA-approved targeted treatment?
Options:
- Bevacizumab
- Infliximab
- Denosumab
- Rituximab
- Zoledronic acid
Correct Answer: Denosumab
Explanation:
The lesion described is a Giant Cell Tumor (GCT) of bone. The neoplastic cells in GCT are actually the spindle-shaped mononuclear stromal cells, which highly express RANKL. This stimulates the recruitment and differentiation of osteoclast-like multinucleated giant cells that cause the aggressive bone lysis. Denosumab is a monoclonal antibody against RANKL, effectively inhibiting this pathway, leading to tumor consolidation and ossification. Zoledronic acid is a bisphosphonate, not a monoclonal antibody.
Question 36:
A 40-year-old male construction worker falls 15 feet from scaffolding. He is neurologically entirely intact. CT imaging of the spine reveals a burst fracture of L1 with 40% retropulsion into the spinal canal and 15 degrees of regional kyphosis. MRI reveals an intact posterior ligamentous complex (PLC). Using the Thoracolumbar Injury Classification and Severity Score (TLICS), what is his calculated score and the recommended treatment approach?
Options:
- Score 2; Non-operative management
- Score 4; Operative or non-operative management
- Score 5; Operative management
- Score 7; Operative management
- Score 3; Non-operative management
Correct Answer: Score 2; Non-operative management
Explanation:
The TLICS score is based on three categories: injury morphology, neurological status, and PLC integrity. Morphology: Burst fracture = 2 points. Neurological status: Intact = 0 points. PLC: Intact = 0 points. Total score = 2. A TLICS score of <=3 is an indication for non-operative management (e.g., bracing/TLSO). A score of 4 is indeterminate (surgeon preference), and a score >=5 is an indication for operative stabilization.
Question 37:
A 28-year-old male presents with a severely swollen foot after a high-speed motor vehicle collision. Radiographs demonstrate a displaced fracture of the talar neck. Further imaging reveals that the body of the talus is dislocated from both the subtalar joint and the tibiotalar joint, while the talonavicular joint remains congruent. According to the Hawkins classification, what is the fracture type, and what is the approximate risk of developing avascular necrosis (AVN) of the talar body?
Options:
- Nondisplaced; 0-10%
- Subtalar dislocation; 20-50%
- Subtalar and tibiotalar dislocation; 80-100%
- Subtalar, tibiotalar, and talonavicular dislocation; 20-50%
- Subtalar dislocation; 100%
Correct Answer: Subtalar and tibiotalar dislocation; 80-100%
Explanation:
Hawkins classification for talar neck fractures: Type I is nondisplaced (AVN 0-10%). Type II has subtalar subluxation/dislocation (AVN 20-50%). Type III has both subtalar and tibiotalar dislocation (AVN risk is historically ~80-100%). Type IV adds talonavicular subluxation/dislocation to a Type III pattern. Because this fracture involves dislocation of both the subtalar and ankle (tibiotalar) joints, it is a Type III fracture.
Question 38:
When evaluating the optimal management of acute, completely displaced mid-substance Achilles tendon ruptures, extensive meta-analyses comparing open surgical repair to non-operative management (utilizing strict functional bracing protocols) have demonstrated that surgical repair is statistically associated with which of the following comparative outcome profiles?
Options:
- Higher rate of deep vein thrombosis
- Decreased risk of re-rupture but increased risk of wound complications
- Increased risk of re-rupture and sural nerve injury
- Equivalent re-rupture risk but decreased return to play
- Slower recovery of plantarflexion strength
Correct Answer: Decreased risk of re-rupture but increased risk of wound complications
Explanation:
Historically and in comprehensive meta-analyses, operative repair of the Achilles tendon offers a lower rate of re-rupture compared to non-operative treatment, but at the cost of a higher risk of soft tissue complications, including superficial and deep infections, wound breakdown, and sural nerve injury. Recent studies utilizing early functional mobilization protocols for non-operative treatment have shown rerupture rates approaching those of surgery, but the classic board answer tradeoff remains lower rerupture risk vs. higher wound complication risk.
Question 39:
Bone Morphogenetic Proteins (BMPs) are members of the TGF-beta superfamily and play a critical role in osteoinduction. Which two specific BMPs have been commercially produced using recombinant DNA technology and approved by the FDA for specific orthopedic applications, such as anterior lumbar interbody fusions and open tibial shaft fractures?
Options:
- BMP-1 and BMP-2
- BMP-3 and BMP-4
- BMP-2 and BMP-7
- BMP-4 and BMP-7
- BMP-6 and BMP-9
Correct Answer: BMP-2 and BMP-7
Explanation:
BMP-2 (rhBMP-2, commercial name INFUSE) is FDA-approved for anterior lumbar interbody fusion (ALIF) and open tibial shaft fractures. BMP-7 (rhBMP-7, also known as Osteogenic Protein-1 or OP-1) was FDA-approved under a Humanitarian Device Exemption for recalcitrant long bone nonunions and revision posterolateral lumbar fusions. BMP-3 actually has an inhibitory effect on bone formation.
Question 40:
In total hip arthroplasty (THA), the choice of bearing surface impacts the wear profile and complication risks. Which of the following bearing surface combinations is classically associated with the phenomenon of 'stripe wear' and an increased risk of audible squeaking during ambulation?
Options:
- Metal-on-highly crosslinked polyethylene
- Ceramic-on-polyethylene
- Metal-on-metal
- Ceramic-on-ceramic
- Oxinium-on-polyethylene
Correct Answer: Ceramic-on-ceramic
Explanation:
Ceramic-on-ceramic (CoC) bearings offer extremely low wear rates and no risk of polyethylene osteolysis or metal ion toxicity. However, complications unique to CoC bearings include the risk of ceramic fracture, 'stripe wear' (linear wear patterns caused by edge loading during microseparation of the head and liner), and audible squeaking, which occurs in a small percentage of patients (up to 10% in some series) and can be highly distressing.