Full Question & Answer Text (for Search Engines)
Question 1:
A 35-year-old male is brought into the trauma bay after a high-speed motorcycle crash. His blood pressure is 80/50 mmHg and heart rate is 130 bpm. An AP pelvis radiograph demonstrates an anteroposterior compression (APC) type III pelvic ring fracture. Following the immediate application of a pelvic binder, his blood pressure remains 85/50 mmHg despite administration of 2L of crystalloid and 2 units of uncrossmatched PRBCs. What is the most appropriate next step in management?
Options:
- Immediate exploratory laparotomy
- Pre-peritoneal pelvic packing and/or angiography
- Definitive internal fixation of the anterior and posterior pelvic ring
- Removal of the pelvic binder and application of an external fixator
- Placement of an IVC filter
Correct Answer: Pre-peritoneal pelvic packing and/or angiography
Explanation:
In hemodynamically unstable patients with pelvic ring injuries, the first step is mechanical stabilization of the pelvic volume (e.g., pelvic binder or sheet). If the patient remains persistently hypotensive despite resuscitation and stabilization, hemorrhage control is required. Institutional protocols vary between pre-peritoneal pelvic packing (to control venous bleeding, which is the most common source) and angiography with embolization (for arterial bleeding). Laparotomy is contraindicated unless there is a clear concurrent intra-abdominal source of bleeding, as it eliminates the tamponade effect.
Question 2:
A 13-year-old obese male presents to the emergency department with severe left thigh pain and an inability to bear weight on the left leg for the past 2 weeks, even with crutches. Radiographs demonstrate a slipped capital femoral epiphysis. Which of the following defines this as an 'unstable' SCFE, and what is the primary associated complication risk?
Options:
- Symptom duration less than 3 weeks; high risk of chondrolysis
- Inability to bear weight; high risk of avascular necrosis (AVN)
- Slip angle greater than 50 degrees; high risk of AVN
- Open triradiate cartilage; high risk of nonunion
- Presence of an effusion on ultrasound; high risk of septic arthritis
Correct Answer: Inability to bear weight; high risk of avascular necrosis (AVN)
Explanation:
The Loder classification defines an unstable SCFE by the patient's inability to bear weight, even with assistive devices. This distinction is critical because unstable SCFEs carry a much higher risk of avascular necrosis (AVN) of the femoral head (approaching 47%) compared to stable SCFEs (<10%). Symptom duration previously defined acute vs. chronic but doesn't dictate stability.
Question 3:
A 65-year-old male of Asian descent presents with progressive clumsiness in his hands, difficulty buttoning his shirts, and a broad-based, spastic gait. Lateral cervical radiograph demonstrates a continuous, dense strip of ossification along the posterior aspect of the vertebral bodies from C3 to C6. Which of the following best describes the primary pathophysiology of this condition?
Options:
- Ectopic ossification of the ligamentum flavum
- Ossification of the posterior longitudinal ligament (OPLL)
- Hypertrophy of the uncinate processes and facet joints
- Degenerative disc disease leading to massive anterior osteophyte formation
- Autoimmune fusion of the anterior longitudinal ligament
Correct Answer: Ossification of the posterior longitudinal ligament (OPLL)
Explanation:
The clinical presentation (cervical myelopathy) and radiographic findings (dense ossification posterior to the vertebral bodies) are classic for Ossification of the Posterior Longitudinal Ligament (OPLL). This condition most commonly occurs in the cervical spine of patients of Asian descent. The ossification mass encroaches on the spinal canal, leading to compression of the spinal cord.
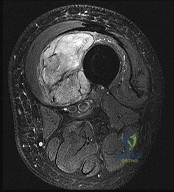
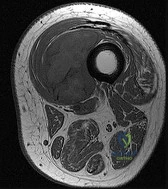
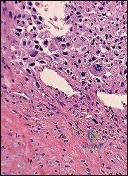
Question 4:
A 32-year-old female presents with progressive knee pain. Imaging reveals an eccentric, lytic epiphyseal-metaphyseal lesion of the distal femur. A biopsy demonstrates multinucleated giant cells in a background of mononuclear stromal cells. If neoadjuvant medical therapy is utilized prior to curettage, the mechanism of action of the most appropriate drug is:
Options:
- Direct cytotoxicity targeting multinucleated giant cells
- Inhibition of osteoclast proton pumps
- Inhibition of RANK ligand (RANKL)
- Inhibition of Vascular Endothelial Growth Factor (VEGF)
- Downregulation of parathyroid hormone receptors
Correct Answer: Inhibition of RANK ligand (RANKL)
Explanation:
The diagnosis is Giant Cell Tumor (GCT) of bone. Denosumab is a monoclonal antibody often used in the medical management of GCT. Its mechanism of action is the inhibition of RANK ligand (RANKL). In GCT, the neoplastic cells are the mononuclear stromal cells, which express RANKL. This recruits and activates the non-neoplastic, multinucleated osteoclast-like giant cells that cause the massive bone resorption.
Question 5:
A 22-year-old collegiate football player sustains a twisting injury to his knee during a tackle. Radiographs reveal an avulsion fracture of the lateral aspect of the proximal tibia, just distal to the articular surface (a Segond fracture). Which ligamentous injury is most strongly associated with this pathognomonic finding?
Options:
- Posterior cruciate ligament (PCL) tear
- Medial collateral ligament (MCL) tear
- Lateral collateral ligament (LCL) tear
- Anterior cruciate ligament (ACL) tear
- Medial patellofemoral ligament (MPFL) tear
Correct Answer: Anterior cruciate ligament (ACL) tear
Explanation:
A Segond fracture is an avulsion fracture of the anterolateral capsule and the anterolateral ligament (ALL) complex from the lateral tibial plateau. It is considered pathognomonic for an anterior cruciate ligament (ACL) tear. It typically occurs via an internal rotation and varus stress mechanism.
Question 6:
A 68-year-old female underwent a total hip arthroplasty (THA) utilizing a ceramic-on-ceramic bearing surface one year ago. She now complains of a loud, audible squeaking sound originating from her hip during normal ambulation. Which of the following factors regarding component positioning is most strongly associated with this complication?
Options:
- Acetabular cup retroversion
- Edge loading due to a steeply placed acetabular cup
- Excessive femoral stem varus
- Excessive femoral anteversion
- Impingement of the greater trochanter on the ilium
Correct Answer: Edge loading due to a steeply placed acetabular cup
Explanation:
Squeaking is a known complication specific to hard-on-hard bearing surfaces, most notably ceramic-on-ceramic THA. The primary etiology is edge loading, which disrupts the fluid film lubrication. Edge loading is most frequently caused by acetabular cup malposition, specifically excessive abduction (a 'steep' cup) or version errors, as well as impingement leading to micro-separation.
Question 7:
A 25-year-old manual laborer presents with 6 months of radial-sided wrist pain. He recalls a fall on an outstretched hand approximately one year ago but did not seek medical attention at the time. Radiographs demonstrate a scaphoid waist nonunion with sclerosis and cystic changes, but there is no evidence of radioscaphoid or midcarpal arthritis. What is the most appropriate surgical treatment?
Options:
- Four-corner fusion
- Proximal row carpectomy
- Scaphoid excision and four-corner fusion
- Open reduction internal fixation with bone grafting
- Total wrist arthrodesis
Correct Answer: Open reduction internal fixation with bone grafting
Explanation:
The patient has a scaphoid nonunion but lacks degenerative arthritic changes (this is pre-SNAC or SNAC stage 0). In the absence of arthritis, the goal is to obtain union of the scaphoid to prevent the progression of carpal collapse and arthritis. This is best achieved via ORIF with bone grafting (non-vascularized or vascularized, depending on proximal pole viability). Salvage procedures like four-corner fusion or PRC are reserved for established SNAC arthritis.
Question 8:
A 28-year-old male sustains a severe axial load to his plantarflexed foot. Radiographs demonstrate a subtle widening between the first and second metatarsal bases and a small avulsion fracture in the first intermetatarsal space (fleck sign). The intact Lisfranc ligament is anatomically attached to which two osseous structures?
Options:
- First metatarsal base and medial cuneiform
- Second metatarsal base and medial cuneiform
- Second metatarsal base and middle cuneiform
- Cuboid and the fourth metatarsal base
- Navicular and the medial cuneiform
Correct Answer: Second metatarsal base and medial cuneiform
Explanation:
The Lisfranc ligament is an incredibly strong, thick interosseous ligament that connects the lateral aspect of the medial cuneiform to the medial base of the second metatarsal. It is the primary stabilizer of the second tarsometatarsal joint. A 'fleck sign' in the first intermetatarsal space represents an avulsion of this ligament and is highly indicative of a Lisfranc injury.
Question 9:
According to Perren's strain theory regarding fracture healing, what biological response is observed when the interfragmentary strain at a fracture site is between 2% and 10%?
Options:
- Primary bone healing via cutting cones
- Resorption of the fracture ends without callus formation
- Callus formation and secondary bone healing
- Granulation tissue formation followed by persistent nonunion
- Woven bone formation directly converting to lamellar bone without intermediate tissues
Correct Answer: Callus formation and secondary bone healing
Explanation:
Perren's strain theory states that the type of tissue that forms at a fracture site is dependent on the strain. Absolute stability (<2% strain) allows for primary bone healing (cutting cones) without callus. Relative stability (2-10% strain) stimulates callus formation (secondary bone healing). Strain greater than 10-15% leads to the formation of fibrous or granulation tissue, ultimately resulting in a nonunion if the strain is not reduced.
Question 10:
A 25-year-old female sustains a Pauwels type III femoral neck fracture after a motor vehicle accident. Which biomechanical force makes this specific fracture pattern particularly prone to fixation failure and varus collapse?
Options:
- Compression forces
- Shear forces
- Tension forces
- Torsional forces
- Bending forces
Correct Answer: Shear forces
Explanation:
The Pauwels classification of femoral neck fractures is based on the angle of the fracture line relative to the horizontal. A Pauwels type III fracture is highly vertical (angle >50 degrees). Because of this vertical orientation, normal joint reactive forces across the hip are converted primarily into high shear forces across the fracture line, predisposing the fracture to varus collapse, loss of fixation, and nonunion compared to the more compressive forces seen in horizontal fractures.
Question 11:
A 4-month-old infant is being treated with a Pavlik harness for Developmental Dysplasia of the Hip (DDH). At the two-week follow-up, the mother notes that the baby is not kicking or extending the knee on the treated side, though ankle and toe movements are intact. Which of the following is the most likely cause of this finding?
Options:
- Avascular necrosis of the femoral head due to excessive abduction
- Femoral nerve palsy due to hyperflexion of the hip
- Obturator nerve palsy due to excessive abduction
- Sciatic nerve compression from the posterior harness straps
- Slipped capital femoral epiphysis caused by the harness
Correct Answer: Femoral nerve palsy due to hyperflexion of the hip
Explanation:
Femoral nerve palsy is a known complication of Pavlik harness treatment. It is typically caused by excessive hyperflexion of the hip in the anterior straps. It presents clinically as an inability to extend the knee (quadriceps weakness) or a lack of kicking on the affected side. The treatment is to temporarily loosen the anterior straps or remove the harness until nerve function returns.
Question 12:
In the Thoracolumbar Injury Classification and Severity (TLICS) score, three main categories are evaluated. Which of the following singular findings contributes the highest point value (3 points) to the total score, strongly favoring surgical stabilization?
Options:
- A burst fracture morphology
- A complete spinal cord injury (ASIA A)
- Disruption of the posterior ligamentous complex (PLC)
- A compression fracture morphology
- Nerve root injury
Correct Answer: Disruption of the posterior ligamentous complex (PLC)
Explanation:
The TLICS system evaluates Morphology, Neurologic Status, and Posterior Ligamentous Complex (PLC) integrity. Complete disruption of the PLC yields 3 points (Suspected/Indeterminate is 2). In Neurologic status, an incomplete cord injury or cauda equina syndrome yields 3 points, while a complete cord injury only yields 2 points. Therefore, PLC disruption (3 points) is a massive driver for surgical intervention (Total score >4 favors surgery).
Question 13:
A 14-year-old boy completes neoadjuvant chemotherapy for an osteosarcoma of the proximal tibia and undergoes a wide local excision. Pathologic evaluation of the resected specimen is performed. According to the Huvos grading system, what minimum percentage of tumor necrosis is the threshold to define a 'good response' to chemotherapy?
Options:
Correct Answer: 90%
Explanation:
The Huvos grading system evaluates the histologic response of osteosarcoma to neoadjuvant chemotherapy. A 'good response' is defined as 90% or greater tumor necrosis (Grade III is 91-99%, Grade IV is 100%). Less than 90% necrosis (Grades I and II) is considered a poor response and correlates with a worse overall prognosis.
Question 14:
During a posterior-stabilized Total Knee Arthroplasty (TKA), the surgeon utilizes spacer blocks and finds that the knee is perfectly balanced in full extension, but tight in 90 degrees of flexion. What is the most appropriate surgical modification to correct this specific imbalance?
Options:
- Release the posterior capsule
- Resect more bone from the distal femur
- Upsize the femoral component and use a thinner polyethylene insert
- Downsize the femoral component and cut more posterior condyle
- Release the medial collateral ligament
Correct Answer: Downsize the femoral component and cut more posterior condyle
Explanation:
When a TKA is balanced in extension but tight in flexion, the flexion gap must be increased without altering the extension gap. This is achieved by either downsizing the femoral component (which removes more posterior condylar bone, opening the flexion gap) or increasing the posterior slope of the tibial cut (which also increases the flexion gap relatively more than the extension gap). Releasing the posterior capsule or resecting more distal femur would affect the extension gap.
Question 15:
A 20-year-old collegiate swimmer presents with bilateral shoulder pain. On physical examination, she demonstrates a positive sulcus sign and apprehension in abduction/external rotation, but she is able to voluntarily dislocate and reduce her shoulders without pain. She has no history of an acute traumatic dislocation. Which of the following is the most appropriate initial management?
Options:
- Arthroscopic Bankart repair
- Open inferior capsular shift
- Latarjet procedure (coracoid transfer)
- Physical therapy emphasizing periscapular and rotator cuff strengthening
- Thermal capsulorrhaphy
Correct Answer: Physical therapy emphasizing periscapular and rotator cuff strengthening
Explanation:
This patient exhibits classic signs of atraumatic, multidirectional instability (MDI), often characterized by the AMBRI acronym (Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift). The hallmark of treatment for MDI is a prolonged, dedicated physical therapy program focusing on strengthening the dynamic stabilizers of the shoulder (rotator cuff and periscapular muscles). Surgery (inferior capsular shift) is reserved for patients who fail extensive conservative management.
Question 16:
Flexor tendon Zone II in the hand, historically referred to as 'no man's land' due to the poor outcomes associated with primary repair, is defined anatomically by which of the following boundaries?
Options:
- From the distal insertion of the FDS to the distal insertion of the FDP
- From the proximal margin of the A1 pulley to the insertion of the FDS
- From the distal edge of the carpal tunnel to the proximal margin of the A1 pulley
- From the musculotendinous junction to the proximal edge of the carpal tunnel
- From the distal edge of the A4 pulley to the insertion of the FDP
Correct Answer: From the proximal margin of the A1 pulley to the insertion of the FDS
Explanation:
Flexor tendon Zone II extends from the proximal aspect of the A1 pulley to the insertion of the Flexor Digitorum Superficialis (FDS) tendon on the middle phalanx. Within this zone, both the FDS and the Flexor Digitorum Profundus (FDP) tendons run tightly together within the fibro-osseous digital sheath. Adhesions are common after repair here, which originally led Bunnell to term it 'no man's land'.
Question 17:
A 55-year-old patient with poorly controlled type 2 diabetes mellitus presents with a severely swollen, red, and warm right foot. There are no open ulcers or breaks in the skin. Radiographs demonstrate joint fragmentation, subluxation of the tarsometatarsal joints, and periarticular bone debris. According to the Eichenholtz classification of Charcot arthropathy, what stage does this represent?
Options:
- Stage 0 (Inflammatory)
- Stage I (Developmental/Fragmentation)
- Stage II (Coalescence)
- Stage III (Reconstruction/Consolidation)
- Stage IV (Ulceration)
Correct Answer: Stage I (Developmental/Fragmentation)
Explanation:
The Eichenholtz classification describes the natural history of Charcot arthropathy. Stage I (Fragmentation) is characterized clinically by acute inflammation (erythema, swelling, warmth) and radiographically by joint subluxation, osteocartilaginous fragmentation, and debris formation. Stage II (Coalescence) shows absorption of fine debris and early fusion. Stage III (Consolidation) shows remodeling and stable deformity. Stage 0 was added later by Shibata and represents clinical inflammation with completely normal radiographs.
Question 18:
Articular cartilage is structurally organized into distinct zones. Which zone is specifically adapted to resist the highest shear forces and is characterized by a dense concentration of collagen fibers oriented parallel to the articular surface?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Tidemark
- Calcified cartilage zone
Correct Answer: Superficial (tangential) zone
Explanation:
The superficial (tangential) zone of articular cartilage comprises the top 10-20% of articular cartilage. It has a high concentration of densely packed collagen type II fibers that are aligned parallel to the joint surface. This specific structural orientation provides the highest tensile strength and the greatest resistance to shear forces within the joint.
Question 19:
A 65-year-old female underwent volar locked plating for a comminuted distal radius fracture 6 months ago. The fracture has healed uneventfully. However, she now presents to the clinic with a sudden inability to actively flex the interphalangeal (IP) joint of her thumb. Which of the following technical errors during the index surgery most likely caused this complication?
Options:
- Over-penetration of the dorsal cortex with locking screws
- Placement of the volar plate distal to the watershed line
- Failure to repair the pronator quadratus over the plate
- Iatrogenic injury to the radial artery during the Henry approach
- Excessive volar tilt correction during reduction
Correct Answer: Placement of the volar plate distal to the watershed line
Explanation:
The patient is presenting with a spontaneous rupture of the Flexor Pollicis Longus (FPL) tendon, which is a well-documented complication of volar plating of the distal radius. It is most commonly caused by iatrogenic plate prominence due to placement of the plate distal to the 'watershed line'. This creates attrition and friction on the FPL tendon as it glides over the prominent hardware, eventually leading to rupture. Prominent dorsal screws would endanger the extensor tendons (e.g., EPL).
Question 20:
A 6-year-old boy falls from the monkey bars and sustains a completely displaced, extension-type supracondylar humerus fracture (Gartland Type III). During your neurologic examination in the emergency department, you ask the child to make an 'OK' sign with his hand, but he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. Which nerve is most likely injured?
Options:
- Radial nerve
- Ulnar nerve
- Anterior interosseous nerve (AIN)
- Posterior interosseous nerve (PIN)
- Musculocutaneous nerve
Correct Answer: Anterior interosseous nerve (AIN)
Explanation:
The anterior interosseous nerve (AIN), a motor branch of the median nerve, is the most commonly injured nerve in extension-type supracondylar humerus fractures (particularly those that displace posterolaterally). It innervates the flexor pollicis longus (FPL), the radial half of the flexor digitorum profundus (FDP to index and middle fingers), and the pronator quadratus. An AIN palsy clinically presents as the inability to form an 'OK' sign (pincer grasp) due to weakness of the FPL and FDP.