Distal Femoral Endoprosthetic Reconstruction: A Masterclass in Oncologic Limb Salvage
Key Takeaway
This masterclass provides an exhaustive, real-time guide to distal femoral endoprosthetic reconstruction for limb salvage. Fellows will learn comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative execution from incision to implant. We cover precise dissection, oncologic margins, hardware application, and soft tissue management, alongside critical pearls, pitfalls, and postoperative care, ensuring a functional, pain-free outcome for complex cases.
Introduction and Epidemiology
The paradigm of managing malignant bone tumors of the distal femur underwent a revolutionary shift in the early 1970s. Pioneered by Ralph C. Marcove at Memorial Sloan Kettering Cancer Center and Kenneth C. Francis at New York University Medical Center, limb-sparing resection replaced amputation as the standard of care for osteosarcoma. This surgical evolution was inextricably linked to the advent of effective neoadjuvant and adjuvant chemotherapeutic agents, specifically doxorubicin and methotrexate. The synergistic effect of systemic chemotherapy and en bloc surgical resection permitted safe limb salvage without compromising overall oncologic survival.
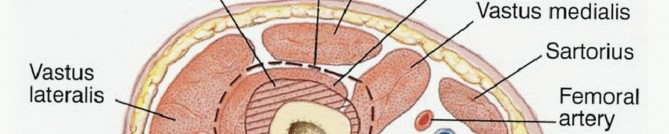
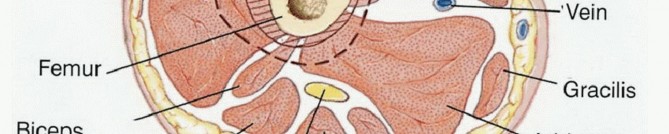
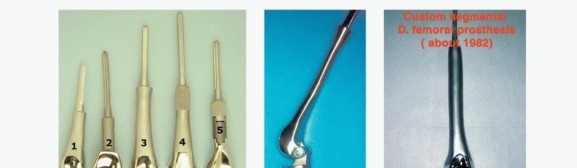
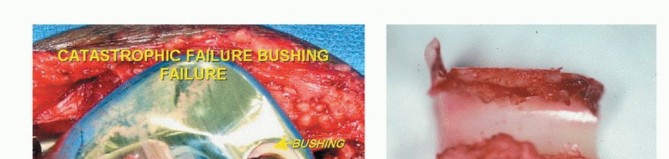
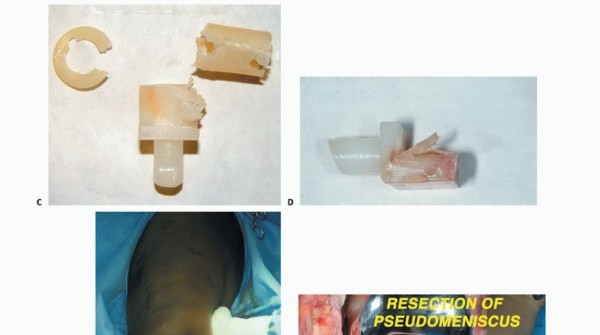
Over the subsequent decades, distal femoral endoprosthetic reconstruction has undergone continuous refinement in both surgical technique and biomechanical engineering. Early constrained hinge designs frequently failed due to aseptic loosening secondary to unyielding stress transfer at the bone-cement interface. The introduction of the kinematic rotating hinge knee by Peter Walker in 1980 resolved this by allowing axial rotation, thereby dissipating torsional forces. Modern modular systems, featuring forged components, Morse taper locks, and porous-coated extramedullary sleeves, have drastically reduced the incidence of mechanical failure, making distal femoral replacement one of the most reliable and functionally rewarding procedures in orthopedic oncology.
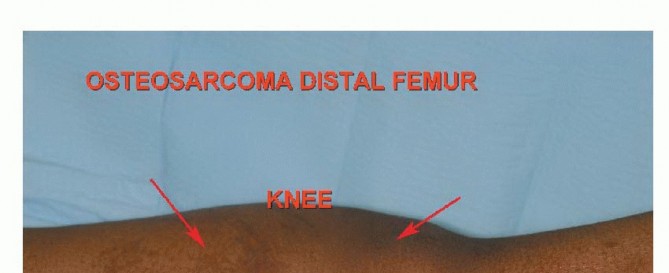
The distal femur remains the most common anatomic location for primary malignant bone tumors, particularly osteosarcoma and Ewing sarcoma, which exhibit a predilection for the rapidly growing metaphyses of the adolescent skeleton. Giant cell tumor of bone, a locally aggressive benign entity, also frequently manifests in the distal femoral epiphysis of young adults. Furthermore, the distal femur is a frequent site for metastatic carcinoma (e.g., breast, prostate, lung, renal, and thyroid) and multiple myeloma. The epidemiological distribution dictates a bimodal age presentation, with primary sarcomas dominating the pediatric and adolescent demographic, and metastatic lesions or secondary sarcomas (e.g., Pagetoid osteosarcoma, radiation-induced sarcoma) presenting in the older adult population.
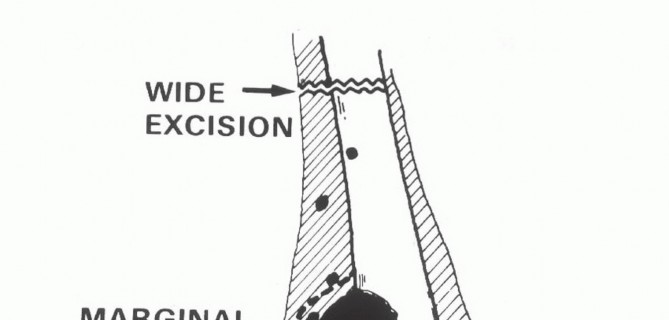
Understanding the diverse biological behavior of these entities is paramount. High-grade spindle cell sarcomas require wide en bloc resection with negative margins, whereas metastatic lesions may be managed with intralesional curettage and cementation or intercalary resections depending on the expected patient longevity and degree of bone destruction. The evolution of endoprosthetic reconstruction has expanded the indications for limb salvage, allowing surgeons to provide immediate structural stability and early mobilization even in cases of massive osseous destruction.




Surgical Anatomy and Biomechanics
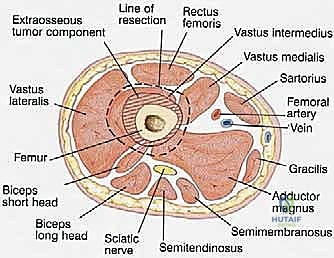
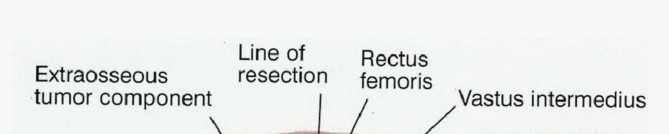
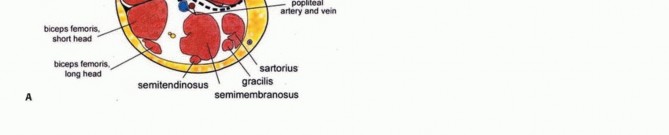
A profound understanding of the cross-sectional, vascular, and muscular anatomy of the distal thigh is an absolute prerequisite for executing a safe oncologic resection and functional reconstruction. The distal femur is enveloped by distinct muscular compartments that serve as natural barriers to tumor extension, provided the fascial borders remain unviolated.
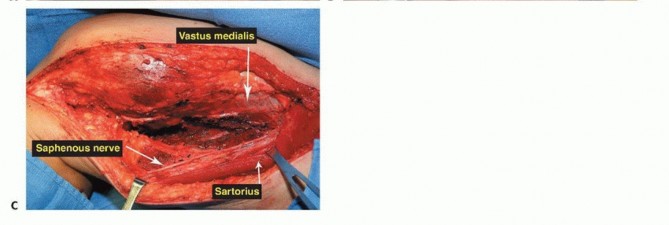
The Sartorial Canal and Vascular Anatomy
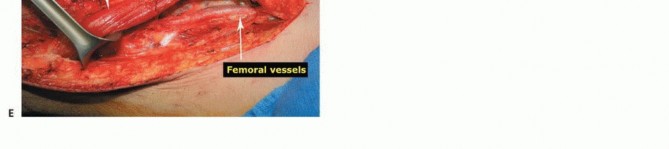
The sartorial canal is an intermuscular space bordered by the vastus medialis anteriorly and laterally, the sartorius medially, and the adductor longus and magnus posteriorly. It serves as the conduit for the superficial femoral artery and vein, and the saphenous nerve. In the presence of large sarcomas, the canal is frequently displaced. However, the deep fascia of the vastus medialis and the robust vascular sheath typically act as reliable anatomic barriers, preventing direct tumor invasion into the vessels. The transition of the superficial femoral vessels to the popliteal vessels occurs at the adductor hiatus, a critical anatomic landmark during distal femoral resection. Careful dissection at the hiatus is required to mobilize the vessels away from the posterior cortex of the femur, particularly when the tumor breaches the posterior cortex.
The Knee Joint and Cruciate Ligaments
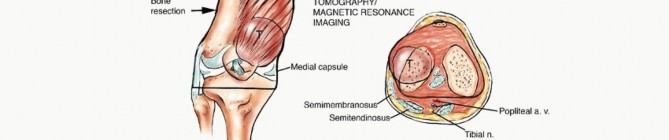
Direct sarcomatous invasion of the knee joint is rare. When intra-articular contamination occurs, it is usually iatrogenic, secondary to a pathologic fracture, or via direct extension along the intra-articular cruciate ligaments. The bone-tendinous junction at the intercondylar notch lacks a cartilaginous barrier, providing a path of least resistance for tumor extension. If cruciate involvement is identified on MRI, an extra-articular resection is not strictly mandated; rather, the cruciates can be resected en bloc with the proximal tibial plateau cut. The suprapatellar pouch must be carefully evaluated on preoperative imaging, as superior extension of the tumor may necessitate resection of the bursa and a portion of the quadriceps tendon.
The Popliteal Space and Neurovascular Bundle
The popliteal fossa contains the popliteal artery, popliteal vein, and sciatic nerve. The popliteal vessels enter through the adductor hiatus and lie in close proximity to the posterior capsule of the knee joint. Preoperative evaluation of the popliteal fat pad is critical; a normal margin of fat usually indicates that the vessels are free from tumor. Intraoperative frozen section analysis of the popliteal adventitia should be utilized if margins are questionable. The sciatic nerve typically bifurcates into the tibial and common peroneal nerves at the superior apex of the popliteal fossa. The tibial nerve courses centrally with the popliteal vessels, while the common peroneal nerve follows the medial border of the biceps femoris. Protection of these neural structures during posterior dissection and retractor placement is vital to prevent postoperative foot drop or plantar sensory deficits.
Biomechanical Considerations of Endoprostheses
The biomechanics of distal femoral reconstruction are inherently complex due to the massive joint reaction forces and the loss of native ligamentous stabilizers. The native knee relies on the collateral and cruciate ligaments to guide the complex rolling and gliding kinematics of flexion and extension. Following an intra-articular distal femoral resection, these ligaments are sacrificed, necessitating a constrained or semi-constrained implant.
Modern rotating hinge endoprostheses are designed to uncouple flexion and extension from axial rotation. A fixed hinge transmits torsional loads directly to the intramedullary stem, leading to high shear stresses at the cement-bone or bone-implant interface, which historically resulted in catastrophic aseptic loosening. The rotating hinge mechanism incorporates a highly cross-linked polyethylene bushing or bearing that allows for 10 to 15 degrees of internal and external rotation, dissipating these torsional forces into the surrounding soft tissue envelope. Furthermore, the selection of stem fixation (cemented versus press-fit) relies on host bone quality and remaining diaphyseal length. Cemented stems rely on a mantle of polymethylmethacrylate for immediate rigid fixation, ideal for irradiated bone or patients with limited life expectancy. Press-fit, porous-coated stems rely on osteointegration and are preferred in young, active patients with robust cortical bone to ensure long-term survivorship.


Indications and Contraindications
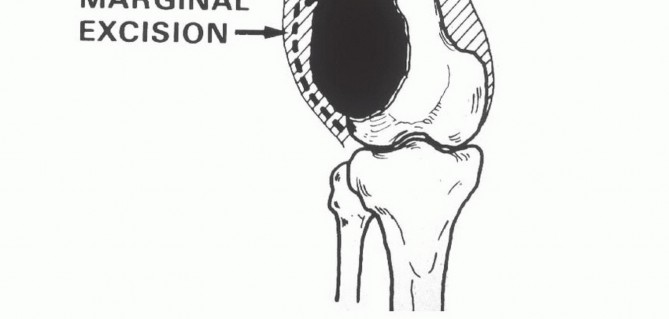
The decision to proceed with a limb-sparing distal femoral resection versus amputation (e.g., transfemoral amputation or rotationplasty) requires a multidisciplinary approach. The primary objective is always the complete eradication of the tumor with negative oncologic margins. Limb salvage is only indicated when it can provide a functional extremity without compromising overall survival or local recurrence rates.
Absolute and Relative Indications
Limb-sparing resection is indicated for primary malignant bone tumors (Enneking Stage IIA and IIB) confined to the distal femur, provided that wide margins can be achieved. It is also indicated for locally aggressive benign tumors (Enneking Stage 3) such as giant cell tumors with extensive cortical destruction where joint preservation is impossible. For metastatic disease, endoprosthetic reconstruction is indicated when life expectancy exceeds the recovery period, and the lesion has caused a pathologic fracture or impending fracture not amenable to standard osteosynthesis.
Contraindications to limb salvage have evolved. Historically, a pathologic fracture was an absolute contraindication to limb salvage due to the risk of hematoma contamination of the surrounding soft tissue compartments. However, modern preoperative imaging and neoadjuvant chemotherapy have rendered this a relative contraindication, provided the hematoma can be resected en bloc. Absolute contraindications include major neurovascular bundle encasement that cannot be bypassed or reconstructed, extensive soft tissue contamination precluding adequate muscle coverage, and active, uncontrolled periprosthetic or systemic infection. In pediatric patients under the age of 8, massive limb length discrepancy following physeal resection may make rotationplasty or amputation a more functional long-term option, although expandable endoprostheses have significantly expanded the age range for limb salvage.
Operative Versus Non Operative Management Guidelines
| Clinical Scenario | Recommended Management Strategy | Rationale and Oncologic Principles |
|---|---|---|
| Enneking Stage IIB Osteosarcoma | Limb-Sparing Resection and Endoprosthesis | Standard of care if wide margins are achievable and neurovascular bundle is free. |
| Major Neurovascular Encasement | Amputation or Rotationplasty | Inability to achieve negative margins without sacrificing the limb's viability. |
| Pathologic Fracture with Contamination | Neoadjuvant Chemotherapy then Re-evaluation | If hematoma is contained and shrinks, limb salvage is possible; otherwise, amputation. |
| Extensive Metastatic Destruction | Palliative Resection and Cemented Prosthesis | Provides immediate mechanical stability and pain relief; cemented stem allows immediate weight-bearing. |
| Uncontrolled Local Infection | Amputation | Endoprosthetic reconstruction in an infected bed carries an unacceptably high failure rate. |
| Pediatric Patient (Extensive Growth Remaining) | Expandable Endoprosthesis or Rotationplasty | Prevents severe leg length discrepancy. Non-invasive expandable implants are preferred. |




Pre Operative Planning and Patient Positioning
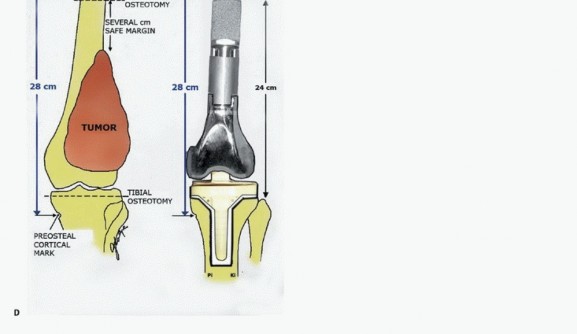
Thorough preoperative planning is the cornerstone of a successful oncologic resection and reconstruction. The objective is to define the exact intramedullary and extramedullary extent of the tumor, plan the osteotomy level, and select the appropriate modular components to restore limb length and joint kinematics.
Advanced Diagnostic Imaging
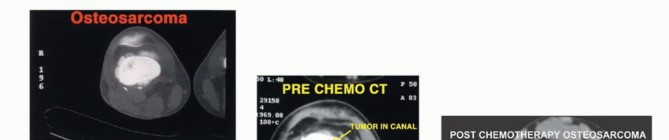
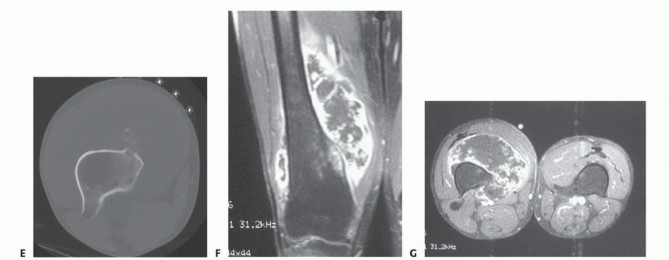
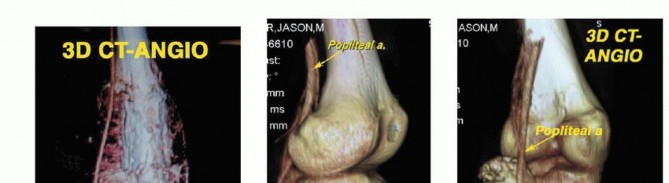
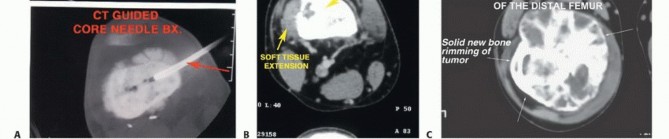
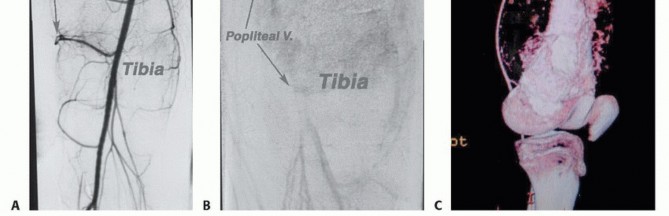
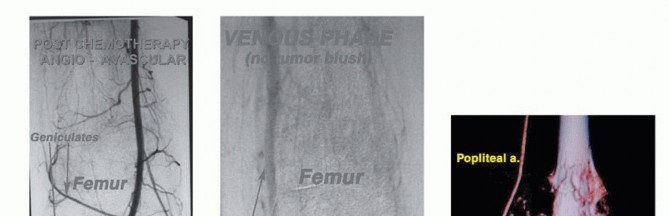
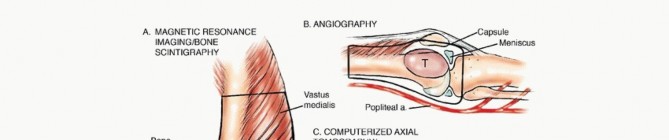
High-resolution magnetic resonance imaging of the entire femur is mandatory. T1-weighted longitudinal images are critical for identifying the intramedullary extent of the tumor and detecting skip metastases within the same bone. T2-weighted and STIR sequences delineate the soft tissue extension and peritumoral edema. The osteotomy level is typically planned 2 to 3 centimeters proximal to the most proximal abnormal marrow signal on T1-weighted MRI. Computed tomography of the chest and a whole-body PET-CT or bone scan are required for systemic staging. Angiography or CT angiography may be indicated if the tumor is in close proximity to the popliteal or superficial femoral vessels, aiding in the assessment of vascular displacement versus encasement.
Biopsy Principles
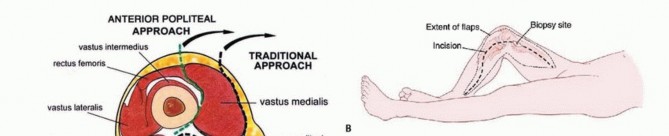
The biopsy is a critical step that dictates the definitive surgical approach. The biopsy tract must be considered contaminated with tumor cells and must be excised en bloc with the surgical specimen. Therefore, a longitudinal incision should be used, placed perfectly in line with the planned extensile surgical approach (typically anteromedial or anterolateral). Transverse incisions are strictly contraindicated. Meticulous hemostasis must be achieved to prevent a post-biopsy hematoma, which would disseminate tumor cells into adjacent fascial planes. Core needle biopsy under imaging guidance is currently the gold standard, minimizing tissue trauma and contamination compared to open incisional biopsy.
Templating and Implant Selection
Digital templating utilizing calibrated orthogonal radiographs is performed to determine the resection length, stem diameter, and required modular segments. The joint line must be accurately restored to ensure proper patellofemoral tracking and soft tissue tensioning. The contralateral normal extremity can be radiographed with a magnification marker to serve as a template for limb length. Custom cutting guides and 3D-printed models are increasingly utilized for complex metaphyseal or diaphyseal resections, ensuring precise execution of the preoperative plan. The surgeon must ensure that a wide array of modular components, including various stem lengths, diameters, and intercalary segments, are available in the operating room.
Patient Positioning and Operating Room Setup
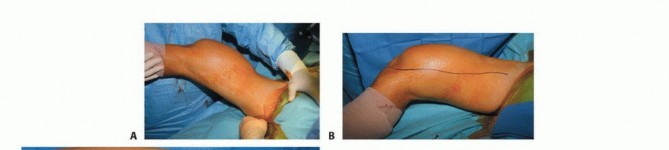
The patient is positioned supine on a radiolucent operating table. A bump may be placed under the ipsilateral hip to correct external rotation and provide neutral alignment of the lower extremity. A sterile tourniquet is applied to the proximal thigh to minimize blood loss during the initial dissection, although it must be deflated prior to tumor resection to assess tissue viability and achieve hemostasis. The entire lower extremity is prepped and draped free, allowing for full range of motion of the hip and knee during the procedure. Intraoperative fluoroscopy must be readily available to confirm osteotomy levels and implant positioning.





Detailed Surgical Approach and Technique
The surgical technique for distal femoral resection and reconstruction demands meticulous dissection, strict adherence to oncologic principles, and precise biomechanical reconstruction. The procedure can be conceptually divided into the approach, vascular isolation, osteotomy, en bloc resection, and endoprosthetic reconstruction.
Incision and Soft Tissue Dissection
An extensile longitudinal incision is made, typically utilizing an anteromedial or anterolateral approach depending on the tumor's soft tissue extension. The previous biopsy tract is circumscribed with an elliptical incision and left attached to the underlying tumor specimen. Full-thickness fasciocutaneous flaps are developed to preserve the vascular supply to the skin. The extensor mechanism is exposed. Depending on the tumor location, a subvastus, midvastus, or standard medial parapatellar arthrotomy is performed. If the tumor involves the vastus intermedius, this muscle must be resected en bloc with the femur, preserving the rectus femoris and vastus medialis/lateralis for subsequent coverage.
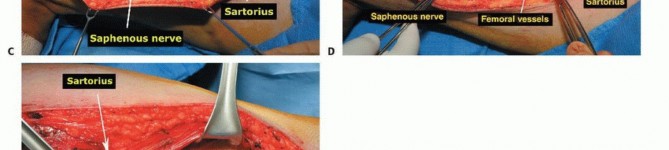
Vascular Dissection and Mobilization
The superficial femoral vessels are identified in the proximal extent of the wound within the sartorial canal. The deep fascia of the vastus medialis is incised, and the vessels are traced distally to the adductor hiatus. The superior medial and superior lateral genicular vessels are identified and ligated to allow mobilization of the popliteal neurovascular bundle away from the posterior capsule of the femur. The perforating branches of the profunda femoris may also require ligation depending on the proximal extent of the resection. Careful blunt dissection with a sponge stick or Kittner dissector is utilized to separate the popliteal fat and vessels from the posterior aspect of the tumor, ensuring a cuff of normal muscle or fat is left on the specimen.
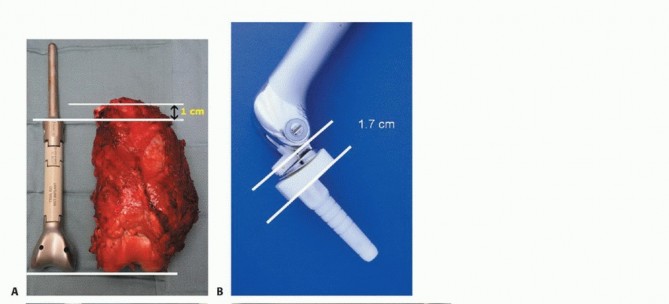
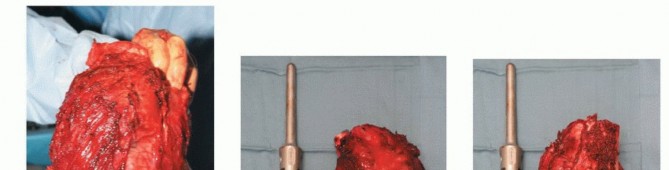
Femoral Osteotomy and Margin Assessment
The planned osteotomy level is measured from the articular surface of the medial or lateral femoral condyle using a sterile ruler or calibrated caliper, correlating with the preoperative MRI. Intraoperative fluoroscopy can be used to confirm the distance from the lesser trochanter or other reliable landmarks. The periosteum is circumferentially incised at the osteotomy site. A transverse osteotomy is performed using an oscillating saw. Immediately following the osteotomy, a sample of the proximal intramedullary
Clinical & Radiographic Imaging



















You Might Also Like


