Masterclass: Limb-Sparing Quadriceps Resection for Sarcoma
Key Takeaway
This masterclass details limb-sparing quadriceps resection for sarcomas, guiding fellows through comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution. We cover precise dissection, neurovascular protection, and advanced reconstructive techniques, emphasizing critical pearls and pitfalls. Learn patient positioning, incision planning, and muscle-specific resections, along with essential postoperative care for optimal functional outcomes in these complex oncologic cases.
Introduction and Epidemiology
The quadriceps muscle group represents the most frequent anatomical site for the development of extremity soft tissue sarcomas. The predominant histological subtypes encountered in this anterior compartment include liposarcomas (ranging from well-differentiated to pleomorphic variants), undifferentiated pleomorphic sarcomas (UPS), and leiomyosarcomas. Historically, massive tumors of the anterior thigh often mandated radical amputations, such as hip disarticulations or high transfemoral amputations, due to the perceived inability to achieve adequate oncologic margins while preserving a functional limb. However, contemporary orthopedic oncology emphasizes limb-sparing resections, which are now feasible and safe for the vast majority of patients.
The success of limb salvage relies heavily on a multidisciplinary paradigm. The utilization of induction chemotherapy combined with either preoperative or postoperative adjuvant radiation therapy is critical for eradicating microscopic residual disease within the reactive zone or pseudocapsule. Soft tissue sarcomas expand by compressing surrounding normal tissue, forming this pseudocapsule, which invariably contains microscopic tumor extensions or satellite lesions. Consequently, even when achieving wide surgical margins necessitates the en bloc extirpation of substantial muscle tissue, the entire compartment, or adjacent critical neurovascular structures like the superficial femoral artery, functional limb salvage can be achieved. Advanced reconstructive techniques for the extensor mechanism—utilizing local muscle transfers such as the sartorius or hamstrings, or massive allografts—yield highly satisfactory functional outcomes.
Histopathologic Diagnoses in Anterior Thigh Sarcomas
| Tumor Type | Number of Patients |
|---|---|
| Malignant Soft Tissue Tumors | |
| Malignant fibrous histiocytoma (UPS) | 4 |
| High-grade liposarcoma | 3 |
| Recurrent low-grade liposarcoma | 1 |
| Leiomyosarcoma | 3 |
| Malignant peripheral nerve sheath tumor | 2 |
| Benign Aggressive Soft Tissue Tumors | |
| Recurrent aggressive fibromatosis | 2 |
| Total | 15 |
(Representative cohort demonstrating typical histopathologic distribution of anterior compartment tumors requiring extensor mechanism reconstruction).

Surgical Anatomy and Biomechanics
Compartmental Anatomy of the Thigh
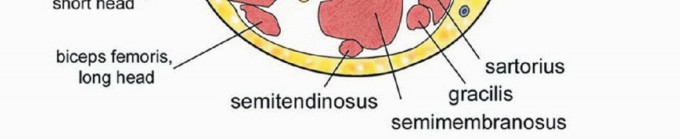
The thigh is anatomically segregated into three distinct compartments enveloped and divided by robust fascial septa: the anterior compartment (quadriceps and sartorius muscles), the medial compartment (adductor muscle group), and the posterior compartment (hamstring muscles). The fascia lata forms the unyielding outer boundary of these compartments, playing a vital role in containing tumor growth until late in the disease process.
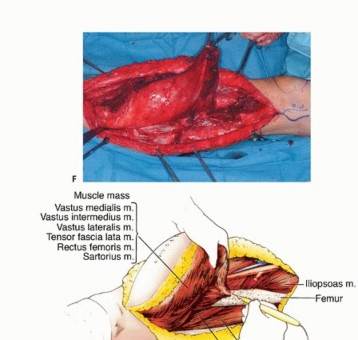
The quadriceps femoris comprises four distinct muscle bellies: the vastus medialis, vastus lateralis, rectus femoris, and vastus intermedius.
* Vastus Medialis and Lateralis: Originate from the proximal femur and the respective intermuscular septa. The vastus lateralis is the largest component, receiving its vascular supply from the descending branch of the lateral circumflex femoral artery.
* Vastus Intermedius: Originates directly from the anterior and lateral surfaces of the femoral shaft and the linea aspera, effectively blanketing the femur.
* Rectus Femoris: The sole biarticular muscle of the group, originating from the anterior inferior iliac spine (AIIS) and the supra-acetabular tubercle. It acts as both a hip flexor and a knee extensor.
Distally, these four heads coalesce to form the quadriceps tendon, inserting onto the superior pole of the patella. Biomechanically and oncologically, the vastus intermedius serves as a critical barrier; by covering the anterior femur, it frequently protects the underlying cortical bone from direct local invasion by sarcomas arising in the more superficial quadriceps components. Because soft tissue sarcomas often remain anatomically confined to a single muscle belly, partial muscle group resections are frequently adequate to achieve negative margins.



(Quadriceps resection types. Type A: resection of the vastus lateralis. Type B: resection of the vastus medialis. Type C: resection of the rectus femoris and vastus intermedius. Type D: subtotal resection of the quadriceps muscle. Note that Type A and B resections frequently incorporate the vastus intermedius to ensure deep margins).
Intermuscular Septa and Neurovascular Anatomy
The intermuscular septa are dense connective tissue structures that dictate the pathways of tumor extension and surgical dissection. The lateral intermuscular septum separates the anterior compartment from the posterior compartment, attaching to the linea aspera. The medial intermuscular septum divides the anterior and medial compartments.
The primary neural structure of the anterior compartment is the femoral nerve, which emerges from the lumbar plexus (L2-L4), passes beneath the inguinal ligament, and arborizes rapidly into motor branches supplying the quadriceps and sensory branches (including the saphenous nerve). Oncologic resection in the anterior thigh frequently requires sacrificing branches of the femoral nerve that tether directly into the tumor mass. Resection of the entire femoral nerve results in profound quadriceps paralysis, necessitating robust extensor mechanism reconstruction or lifelong bracing.

Superficial Femoral Artery and Adductor Canal
The superficial femoral artery (SFA) is the primary axial vessel of the lower extremity. After branching from the common femoral artery at the femoral bifurcation, the SFA courses distally through the anterior compartment within the femoral triangle, entering the adductor canal (Hunter's canal). The canal is bounded anterolaterally by the vastus medialis, posteriorly by the adductor longus and magnus, and roofed by the sartorius muscle and the subsartorial fascia.
In the context of massive anterior thigh sarcomas, particularly those arising in the vastus medialis or deep rectus femoris, the tumor frequently abuts or encases the SFA. Historically, encasement of the major neurovascular bundle was an absolute contraindication to limb salvage. Currently, if the SFA is encased, en bloc resection of the artery with the tumor, followed by immediate vascular reconstruction (bypass grafting), is the standard of care, allowing for limb preservation without compromising oncologic margins.


Indications and Contraindications
The decision-making process for surgical intervention in anterior thigh sarcomas is complex and requires careful consideration of tumor biology, anatomical location, and patient-specific factors. The primary objective is complete eradication of the tumor with negative margins (R0 resection), followed by the preservation of a functional extremity.
Criteria for Limb Salvage
Limb-sparing surgery is indicated for the vast majority of extremity soft tissue sarcomas. The advent of microvascular surgery and advanced reconstructive techniques has significantly expanded these indications. Involvement of the superficial femoral artery or vein is no longer a contraindication to limb salvage; these structures can be resected en bloc and reconstructed. Similarly, localized involvement of the femur can be addressed with extra-articular resection and endoprosthetic reconstruction.
Absolute contraindications to limb salvage are rare but include extensive neurovascular involvement that precludes reconstruction, massive tumors where resection would leave a functionless and painful limb, or severe baseline patient comorbidities that prohibit prolonged reconstructive surgery.
| Clinical Scenario | Surgical Strategy | Rationale and Considerations |
|---|---|---|
| Tumor confined to single muscle belly (e.g., Rectus Femoris) | Limb-Sparing Resection (Type C) | Wide margins achievable with compartmental or sub-compartmental resection. Excellent functional recovery expected. |
| Tumor abutting Superficial Femoral Artery | Limb-Sparing Resection with Subadventitial Dissection | If the adventitia is not invaded, meticulous dissection can spare the vessel. Preoperative radiation aids in sterilizing the margin. |
| Tumor encasing Superficial Femoral Artery | Limb-Sparing Resection with Vascular Reconstruction | En bloc resection of SFA to achieve negative margins. Reconstruction with reversed saphenous vein graft or synthetic conduit. |
| Extensive involvement of Sciatic and Femoral Nerves | High Transfemoral Amputation or Hip Disarticulation | Resection of both major nerves results in a flail, insensate limb prone to ulceration and severe dysfunction. Amputation provides better rehabilitation potential. |
| Fungating, infected tumor mass with sepsis | Palliative Amputation | Source control is the priority. Limb salvage in the setting of gross infection and tissue necrosis carries an unacceptably high failure rate. |

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful oncologic surgery. A multidisciplinary tumor board review involving orthopedic oncologists, medical oncologists, radiation oncologists, musculoskeletal radiologists, and vascular surgeons is mandatory.
Advanced Imaging Modalities
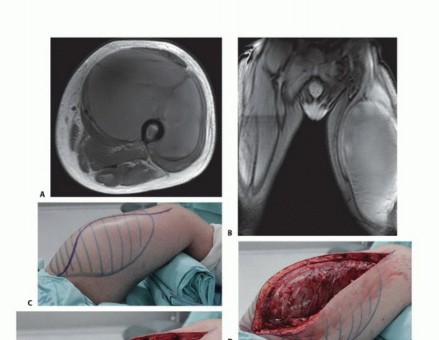
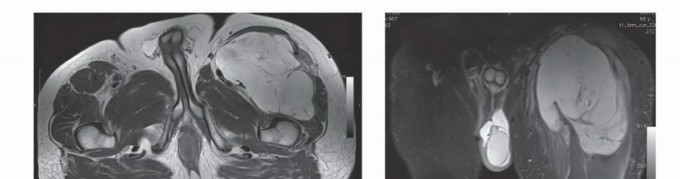
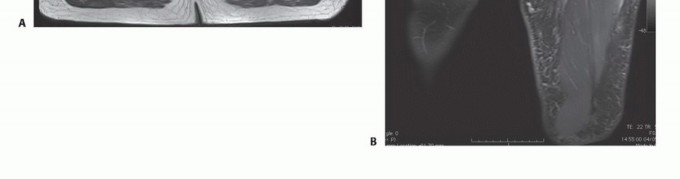
Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard for local staging. MRI delineates the intra- and extra-compartmental extent of the tumor, its relationship to the intermuscular septa, and its proximity to the superficial femoral artery and femoral nerve. T1-weighted images are excellent for assessing marrow infiltration if bone involvement is suspected, while fluid-sensitive sequences (T2-weighted fat-suppressed or STIR) highlight peritumoral edema, which often dictates the extent of the reactive zone and the required surgical margin.
Computed Tomography (CT) of the chest is required for systemic staging, as the lungs are the most common site of metastasis for extremity soft tissue sarcomas. If the MRI suggests encasement or intimate involvement of the SFA, a CT Angiography (CTA) or Magnetic Resonance Angiography (MRA) is indicated. This provides a vascular roadmap, identifying the patency of the SFA, the status of the profunda femoris (which may provide critical collateral flow), and the distal runoff vessels, which is essential information if vascular reconstruction is planned.

Patient Positioning and Preparation
The patient is positioned supine on a radiolucent operating table. A bump may be placed under the ipsilateral hemipelvis to internally rotate the leg slightly, bringing the anterior and medial thigh into optimal view.
Crucially, the entire lower extremity from the umbilicus to the toes must be prepped and draped in a sterile fashion. If vascular reconstruction is anticipated, the contralateral lower extremity must also be prepped and draped to allow for the harvest of the great saphenous vein. The use of a sterile pneumatic tourniquet placed as proximally as possible on the thigh is standard; however, for very proximal tumors, a sterile tourniquet may not be feasible. In such cases, proximal vascular control must be obtained surgically at the level of the common femoral artery beneath the inguinal ligament before proceeding with tumor mobilization.


Detailed Surgical Approach and Technique
The surgical execution of a limb-sparing quadriceps resection requires meticulous attention to oncologic principles, precise anatomical dissection, and proficient reconstructive skills.
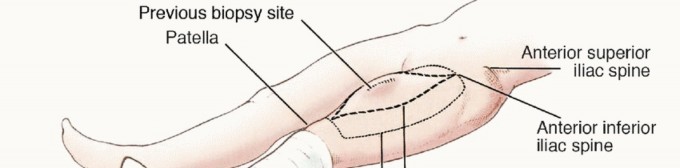
Incision and Biopsy Tract Management
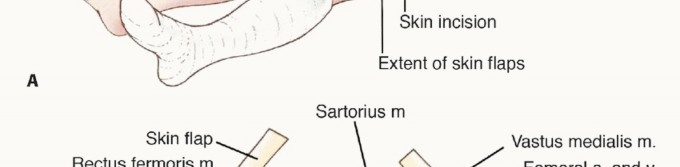
The skin incision must be carefully planned to incorporate the previous biopsy tract. The biopsy tract is considered contaminated with microscopic tumor cells and must be excised en bloc with the main tumor specimen. An elliptical incision is made encompassing the biopsy site, ensuring at least a 1 to 2-centimeter margin of normal skin around the tract. The incision is then extended proximally and distally along the longitudinal axis of the thigh, typically following the course of the sartorius muscle or the midline of the anterior thigh, depending on the tumor's exact location.
Full-thickness fasciocutaneous flaps are elevated medially and laterally. It is imperative to maintain the deep fascia on the tumor specimen; the dissection plane should be between the subcutaneous fat and the fascia lata, except where the tumor superficially invades the subcutaneous tissue, in which case a thicker layer of healthy fat must be left attached to the specimen.

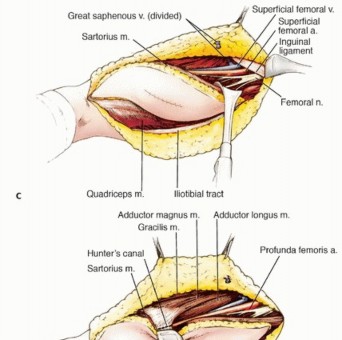
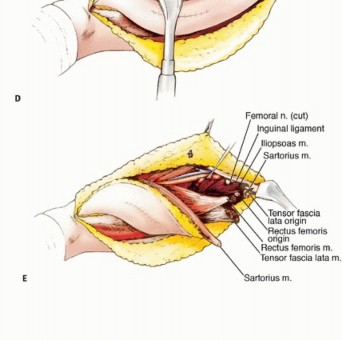
Vascular Dissection and Superficial Femoral Artery Management
Once the flaps are elevated, proximal and distal control of the major vessels is the immediate priority. The femoral triangle is opened proximally. The sartorius muscle is identified and mobilized laterally. The femoral sheath is incised, and the common femoral artery, superficial femoral artery, and femoral vein are identified and encircled with vessel loops. Distal control is obtained by opening the adductor canal distally, near the adductor hiatus, and isolating the popliteal vessels.
If the tumor abuts the SFA but imaging suggests a clear tissue plane, a subadventitial dissection may be attempted. This involves sharply dissecting the tumor off the vessel wall, leaving the adventitia intact. This is a high-risk oncologic maneuver and should only be performed if preoperative radiation has sterilized the microscopic margins, and frozen sections of the vessel bed return negative.
If the tumor encases the SFA, or if a subadventitial dissection is impossible without violating the tumor pseudocapsule, en bloc resection of the artery is mandatory. Systemic heparinization (typically 50-100 units/kg) is administered. Vascular clamps are applied proximally and distally to the tumor. The SFA and accompanying femoral vein are transected with adequate margins.
Vascular reconstruction is typically performed using a reversed great saphenous vein graft harvested from the contralateral leg. The vein provides excellent patency rates and is more resistant to infection than synthetic conduits (such as PTFE), which is a critical consideration in a radiated surgical bed. End-to-end anastomoses are performed using continuous non-absorbable monofilament suture (e.g., 6-0 Prolene) under loupe magnification. Prior to completing the distal anastomosis, the graft is flushed to ensure no twisting or intraluminal thrombi are present. Once flow is restored, meticulous hemostasis is achieved.

En Bloc Muscle Resection
With the vascular structures managed, the muscular resection proceeds. The goal is a wide excision, removing the tumor with a cuff of normal, healthy muscle tissue in all dimensions.
- Type A Resection (Vastus Lateralis): The vastus lateralis is detached from the linea aspera and the lateral intermuscular septum. The descending branch of the lateral circumflex femoral artery is ligated. The vastus intermedius is frequently taken en bloc to provide a deep margin against the femur.
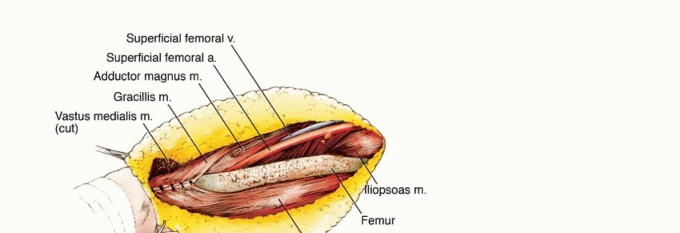
- Type B Resection (Vastus Medialis): The vastus medialis is mobilized from the medial intermuscular septum and the adductor canal. Extreme care is taken to protect or reconstruct the SFA as it courses through the canal.
- Type C Resection (Rectus Femoris and Vastus Intermedius): The rectus femoris is detached proximally from the AIIS. The vastus intermedius is elevated off the anterior femoral cortex using a periosteal elevator. If the tumor is adjacent to the periosteum, the periosteum must be excised; if there is cortical invasion, an extra-articular segmental bone resection is required.
- Type D Resection (Subtotal/Total Quadriceps): For massive tumors, the entire anterior compartment is resected from the proximal origins to the quadriceps tendon distally.
During the deep dissection, branches of the femoral nerve entering the tumor must be sharply transected and ligated to prevent neuroma formation. The sciatic nerve in the posterior compartment is generally well protected by the adductor magnus and the intermuscular septa but must be kept in mind during extremely deep resections.

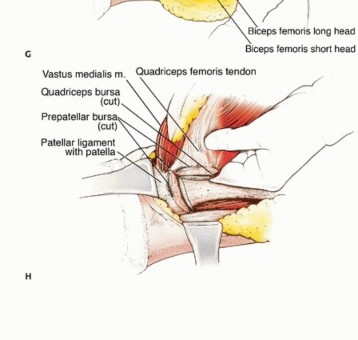
Extensor Mechanism Reconstruction
Resection of a significant portion of the quadriceps, particularly the rectus femoris or the distal quadriceps tendon, necessitates reconstruction to restore knee extension and prevent profound instability.
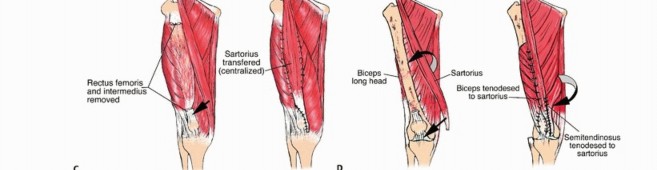
If only one or two muscle bellies are resected, the remaining quadriceps components can often be advanced and sutured to the residual quadriceps tendon or directly to the patella.
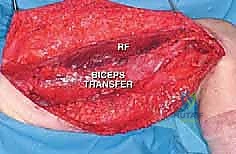
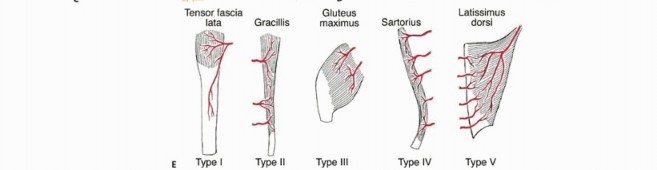
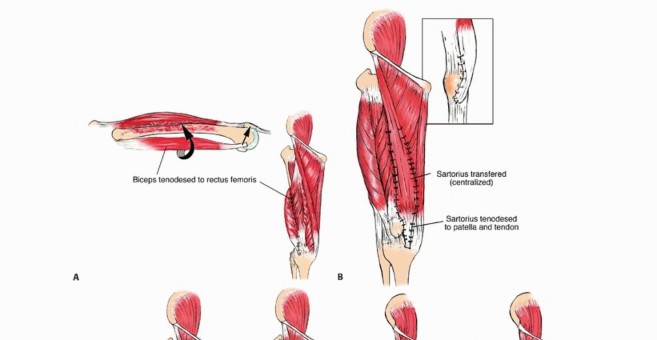
For more extensive defects, local muscle transfers are utilized. The sartorius muscle, due to its proximal origin and distal insertion on the pes anserinus, is an excellent choice. It can be mobilized, rotated anteriorly, and woven into the patellar tendon or remaining quadriceps tendon. Alternatively, the biceps femoris or semitendinosus can be transferred anteriorly.
In cases of total quadriceps extirpation, massive structural reconstruction is required. This can be achieved using a synthetic mesh tube (e.g., Marlex or Prolene mesh) sutured proximally to the remaining musculature or pelvis and distally to the patella. Another robust option is the use of an Achilles tendon allograft with a calcaneal bone block. The bone block is press-fit or screw-fixated into a trough created in the patella, and the tendinous portion is woven into the proximal soft tissues.
If a vascular bypass was performed, it is imperative to provide healthy, well-vascularized soft tissue coverage over the graft to prevent desiccation and blowout. A sartorius muscle flap or a pedicled gastrocnemius flap may be rotated to cover the vascular anastomosis.

Complications and Management
Limb-sparing surgery for massive sarcomas, particularly when combined with neoadjuvant radiation and vascular reconstruction, carries a significant risk of postoperative complications. A proactive approach to identification and management is essential.
Postoperative Complication Profiles
Wound complications are the most frequent morbidity, occurring in up to 30-40% of patients who receive preoperative radiation therapy. Radiation induces microvascular thrombosis and tissue fibrosis, severely impairing wound healing. Meticulous surgical technique, the avoidance of extensive subcutaneous undermining, and the use of closed suction drains until output is minimal are critical preventative measures.
| Complication | Estimated Incidence | Salvage and Management Strategies |
| :---
Clinical & Radiographic Imaging
You Might Also Like


