Sartorial Canal Tumor Resection: An Intraoperative Masterclass in Limb Salvage
Key Takeaway
This masterclass guides fellows through the complex resection of sartorial canal tumors. We'll meticulously cover preoperative planning, patient positioning, and real-time surgical execution, emphasizing comprehensive anatomy, neurovascular protection, and oncologic principles. Learn precise dissection, vascular management, and soft tissue reconstruction techniques for optimal limb salvage and functional outcomes, including handling potential complications.
Alright, team, let's gather around. Today, we're tackling a challenging case: a tumor residing deep within the sartorial canal. This isn't just another soft tissue mass; these are extracompartmental space tumors, and their intimate relationship with the main neurovascular structures of the lower limb demands our absolute precision and respect. This masterclass will walk you through every critical step, from preoperative assessment to meticulous reconstruction.
Understanding the Sartorial Canal: A Critical Anatomical Review
Before we make any incision, let's re-establish our anatomical bearings. The sartorial canal, also known as the subsartorial canal, Hunter's canal, or adductor canal, is a crucial conduit in the medial thigh. It extends from the apex of the femoral triangle proximally, transitioning distally to the popliteal fossa via the adductor hiatus.
Boundaries of the Canal
Imagine an inverted triangle in cross-section, fellows:
* Roof: This is formed by the sartorius muscle, which lies anterior and medial to the canal. This muscle will be our initial landmark and, at times, a critical component of our exposure.
* Floor: Composed primarily of the adductor longus muscle proximally, and the adductor magnus muscle more distally.
* Lateral Border: The thick fascia overlying the vastus medialis muscle.
* Posterior Border: Primarily the adductor magnus muscle and its dense fascial covering.
Neurovascular Contents and Risks
Within this confined space lie vital structures that we must protect at all costs:
* Superficial Femoral Artery: The primary arterial supply to the distal limb.
* Superficial Femoral Vein: Often lies posterior and lateral to the artery, though its position can be variable.
* Saphenous Nerve: A purely sensory branch of the femoral nerve. It accompanies the femoral artery, initially lateral to it, then anterior, and finally medial as it exits the canal to supply sensation to the medial aspect of the leg and foot. Damage to this nerve can lead to significant sensory deficit and neuropathic pain.
* Nerve to Vastus Medialis: A motor branch of the femoral nerve that typically enters the vastus medialis muscle within the canal.
* Thick Fascial Sheath: Crucially, the superficial femoral artery and vein are encased throughout their length by a very thick fascial sheath. This sheath often serves as a vital oncologic barrier, separating the tumor from the major vessels, providing a potential safe plane of dissection.
The vessels typically exit the canal distally through the adductor hiatus, a fibrous opening in the distal part of the adductor magnus muscle, to become the popliteal artery and vein. Understanding these precise relationships is paramount, as tumors here can rapidly distort this anatomy.
Preoperative Planning: Charting Our Course
This is where we formulate our battle plan. Remember, every tumor in the sartorial canal should be considered malignant until proven otherwise, and early, definitive resection is key to preventing vessel invasion and reducing metastatic risk.
Imaging and Staging Studies
Our comprehensive imaging suite provides the roadmap:
* Plain Radiography: We always start here to rule out direct invasion of the femur or the presence of soft tissue calcifications, which can be pathognomonic for certain histologies like synovial sarcoma or hemangiomas.
* Computed Tomography (CT) with 3D Reconstruction and Arterial Contrast: This is invaluable for assessing the precise anatomic relationship between the tumor and the main vessels. In such a small, confined space, tumors distort normal anatomy early, displacing vessels. The 3D reconstructions allow us to visualize this distortion in multiple planes.
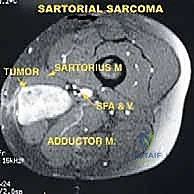
* Magnetic Resonance Imaging (MRI): Our gold standard for soft tissue evaluation. MRI precisely delineates tumor size, its invasion into neighboring structures (sartorius, vastus medialis, adductor muscles), and its proximal and distal extent into the femoral triangle or popliteal spaces. It often helps us identify the specific muscle or structure from which the tumor originates.
FIG 2 • A. Axial MR image of a tumor of the sartorial canal that arises from the muscle wall and encroaches on the vessels.

* Angiography: Performed to assess the tumor's vascularity, detect any "tumor blush" (indicating high-grade malignancy), identify feeding vessels, and most critically, determine if the femoral artery is merely displaced or directly invaded by the tumor.
FIG 2 • B. Angiogram of the same lesion showing tumor blush from the late arterial phase.
* Venography: Essential to rule out venous thrombus, mural tumor thrombus, or direct tumor involvement of the femoral vein. This is crucial for planning potential venous sacrifice.
* Bone Scan (Technetium-99m): Used to rule out distant metastatic disease. High-grade tumors may show a strong tumor blush in the late arterial flow phase, providing a clue to their aggressive nature.
Tumor Classification and Surgical Strategy
Based on our imaging, we classify these tumors into three types, which dictates our resection strategy:
* Type 1 (Luminal) Tumors: These arise from within the sartorial canal space itself, typically from fat or fibrous tissue. They lie "loose" within the space, approximating but not adherent to the vessel walls or surrounding muscles.
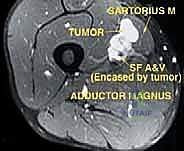
FIG 3 • Type 1 (luminal) tumors lie within the space and are resected with a thin cuff of tissue that surrounds them.
* Type 2 (Wall) Tumors: These originate from one of the muscular walls bordering the canal (sartorius, vastus medialis, adductor magnus, or adductor longus). They arise from within the muscle or its fascia.
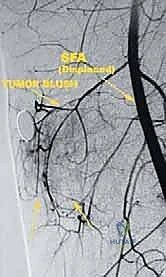
FIG 3 • Type 2 (wall) tumors arise from the muscles surrounding the space and are resected as a typical muscle resection.
* Type 3 (Vessel) Tumors: These are the most challenging, as they directly involve arteries, veins, or nerves. They originate from, or have directly invaded, the vessel wall, not simply juxtaposed to it.
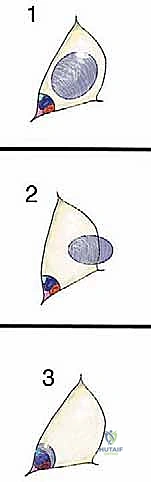
FIG 3 • Type 3 (vessel) tumors invade the vessels and are therefore resected en bloc with the vessels.

This classification helps us predict the difficulty of resection and reconstruction, and critically, the necessary surgical margins.
Biopsy Strategy: Excisional Biopsy with Frozen Section
For sartorial canal tumors, core needle biopsy or open incisional biopsy carries significant risks:
* Hematoma: May spread along the neurovascular bundle, contaminating the entire extremity and potentially necessitating amputation.
* Vessel Puncture: Tumors like leiomyosarcomas can arise directly from vessel walls. A biopsy attempt could cause catastrophic bleeding.
* Inaccurate Diagnosis: The small sample size may miss the true nature or grade of the tumor.
Therefore, our strategy is excisional biopsy with frozen section at the time of definitive surgery. This allows us to obtain a clear diagnosis and confirm negative margins in real-time.
Patient Positioning and OR Setup
Let's get our patient into position.
1. Supine Position: The patient is placed supine on the operating table.
2. Limb Preparation: The entire affected leg, from the iliac crest to the toes, is meticulously prepped and draped free. This allows for full range of motion and access to the entire length of the canal and potentially the popliteal fossa.
3. Contralateral Limb Preparation: Crucially, the contralateral leg is also prepped and draped into the field. This is our backup plan for harvesting a reverse saphenous vein graft if arterial reconstruction becomes necessary.
4. Table Attachments: Ensure appropriate padding for all pressure points. We'll need a stable setup that allows for fluoroscopy if required, though typically not for these resections. A bolster under the ipsilateral hip can help internally rotate the limb slightly, presenting the medial thigh more favorably.
Step-by-Step Intraoperative Execution: The Surgeon's View
Alright, fellows, scalpel in hand. Let's begin.
1. Initial Incision and Flap Elevation
"Alright, team, we've got our patient positioned, prepped, and draped. Let's make our incision. I'm going to mark a generous longitudinal incision directly over the palpable mass, extending proximally into the femoral triangle and distally towards the adductor hiatus, following the course of the sartorius muscle. Remember, wide exposure is key here."
- Skin Incision: Using a #10 blade, I'm making a long, curvilinear incision along the length of the sartorius muscle. We need to be generous here, as inadequate exposure is a common pitfall.
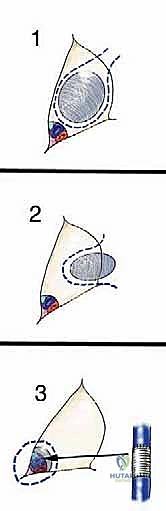
FIG 4 • Surgical approach to resecting a tumor of the sartorial canal. Skin incision is carried along the sartorius muscle.
* Fasciocutaneous Flaps: Now, with electrocautery, we'll raise full-thickness fasciocutaneous flaps, both anteriorly and posteriorly. This provides the wide exposure necessary to identify all relevant anatomical structures and achieve oncologically sound margins. Be mindful of the subcutaneous tissue and superficial lymphatic channels to minimize postoperative lymphedema.
2. Identifying and Mobilizing the Sartorius Muscle
"Now that our flaps are raised, the sartorius muscle is clearly visible. This muscle forms the roof of our canal. We need to mobilize it to gain access."
- Sartorius Mobilization: Carefully dissect along the medial and lateral borders of the sartorius muscle. For most resections, especially for Type 1 and 2 tumors, we'll disconnect the sartorius muscle at its distal insertion. This allows us to retract the muscle anteriorly and laterally, exposing the underlying sartorial canal.
- Surgical Directive: "Assistant, please place a broad Richardson retractor under the distal sartorius and gently retract it anteriorly and laterally. Be careful not to put excessive tension on its proximal neurovascular supply if we plan to preserve it."
- Oncologic Consideration: If the tumor is a Type 2 lesion arising directly from the sartorius, or grossly invades it, then the sartorius muscle will be resected en bloc with the tumor as part of our oncologic margin.
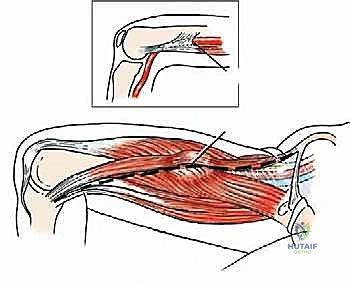
FIG 4 • The sartorius muscle is either resected with the tumor if necessary from an oncologic point of view or disconnected distally for wide exposure.
3. Proximal and Distal Neurovascular Control
"This is a critical step, fellows. Before we even approach the tumor itself, we must gain proximal and distal control of the major neurovascular structures. This is non-negotiable, especially with the risk of vessel invasion."
- Proximal Control (Femoral Triangle): I'm carefully dissecting proximally into the femoral triangle. Here, we'll identify the common femoral artery and vein, just distal to the inguinal ligament. We'll use vessel loops to secure both the superficial femoral artery and vein proximally.
- Distal Control (Adductor Hiatus/Popliteal Fossa): Distally, we'll dissect towards the adductor hiatus. If necessary, we'll carefully open the fibrous adductor hiatus to better expose the superficial femoral artery and vein as they transition into the popliteal vessels. For large tumors extending into the popliteal fossa, we may need to detach the femoral insertions of the medial hamstrings (semitendinosus, semimembranosus) and the medial head of the gastrocnemius to achieve adequate exposure.
- Surgical Directive: "Assistant, let's get some vascular loops ready. We need both proximal and distal control before we get anywhere near this tumor."
- Surgical Warning:
> Surgical Warning: Always identify the saphenous nerve and attempt to preserve it if not involved by tumor. It runs with the vessels and is vulnerable during this dissection. Also, be acutely aware of the greater saphenous vein. Resection of the femoral vein may be unavoidable, but we must preserve the greater saphenous vein if possible to avoid severe venous insufficiency.
- Ligation of Perforating Vessels: As we expose the main vessels, we will encounter small perforating vessels connecting the tumor to the main superficial femoral artery and vein. These must be meticulously ligated and divided with clips or bipolar cautery.
4. Tumor Resection Based on Type
Now, with excellent exposure and proximal/distal control, we proceed with the definitive resection, tailored to our preoperative classification.
A. Type 1 (Luminal) Tumor Resection
"This appears to be a Type 1 tumor, fellows. It's lying within the space, approximating the vessels but not grossly adherent. This is generally the most straightforward oncologic resection."
- Dissection Plane: We will carefully dissect around the tumor, staying within a thin layer of normal tissue that abuts the tumor. This "normal tissue" is typically the thick fascial sheath surrounding the superficial femoral artery and vein.
- En Bloc Resection: The tumor is resected en bloc with this thin cuff of surrounding tissue.

TECH FIG 1 • A. Intraoperative picture of the tumor encroaching on the vessels. The sartorius muscle has been disconnected distally to improve exposure.
* Frozen Section Analysis: Once the tumor is resected, we will send the fibrous sheath surrounding the vessels for frozen section analysis. This is critical to rule out microinvasion and confirm negative margins.
* Surgical Directive: "Pathology, please. We're sending the fibrous sheath overlying the vessels for frozen section. We need to confirm this sheath is free of tumor."
* Vascular Preservation: Vascular resection is typically not required for Type 1 tumors.
B. Type 2 (Wall) Tumor Resection
"This tumor, fellows, is a Type 2 lesion, arising directly from the vastus medialis fascia. Our approach will be a wide local excision, including the muscle of origin."
- Muscle Resection: We will resect the tumor en bloc with a generous cuff of the muscle from which it originates (e.g., vastus medialis, adductor magnus, sartorius). This includes the fascia covering that muscle and any adjacent fat within the canal.

TECH FIG 1 • B. The tumor has been resected with the thick fascial sheath that lines the vessels and with the muscle and fascia from which it arises. V Med M , vastus medialis muscle; Add Mag , adductor magnus muscle; SF A&V , superficial femoral artery and vein.
* Vessel Sheath: Even if the tumor doesn't grossly invade the vessels, the fibrous sheath surrounding them, if in intimate proximity, should be resected en bloc with the tumor and sent for frozen section to ensure clear margins.
* Surgical Warning:
> Surgical Warning: Sarcomas are known to respect fascial boundaries. Dissecting an intact adventitia off the vessels that is pathologically free of tumor is considered a sufficient resection margin, even if a 1 cm gross margin isn't achievable on the vessel side.
C. Type 3 (Vessel) Tumor Resection: The Ultimate Challenge
"This is our most complex scenario, fellows. Our preoperative imaging and intraoperative assessment confirm direct invasion of the superficial femoral artery. There is no safe way to achieve negative margins without resecting the vessel itself. We have our vascular surgeon on standby."
- Vascular Surgeon Collaboration: At this point, the vascular surgeon takes the lead for the vessel resection and reconstruction.
- Heparinization: The patient is systemically heparinized to prevent thrombus formation.
- Clamping: The superficial femoral artery and vein are clamped proximally and distally, well beyond the tumor involvement.
- En Bloc Resection: The tumor, along with the involved segment of the artery and/or vein, is resected en bloc with any adjacent muscle or fascia as required.
- Arterial Reconstruction:
- Graft Harvest: We will harvest a reverse saphenous vein graft from the contralateral leg. This is our preferred option due to its resistance to infection and superior long-term patency. Alternatively, a synthetic graft (e.g., Gore-Tex) can be used.
- Anastomosis: The graft is then meticulously anastomosed end-to-end to the remaining healthy segments of the superficial femoral artery using fine vascular sutures (e.g., 6-0 Prolene).
- Surgical Directive: "Vascular surgeon, we're ready for your expertise. Let's ensure excellent pulsatile flow through this graft."
- Venous Reconstruction (Optional):
- If the superficial femoral vein is resected, reconstruction is generally not required, provided the ipsilateral greater saphenous vein is intact. The extensive collateral venous drainage usually prevents severe venous insufficiency.
- Surgical Warning:
> Surgical Warning: If both the superficial femoral vein and the ipsilateral greater saphenous vein are ligated or resected, severe, limb-threatening venous insufficiency will result. Always preserve the greater saphenous vein if femoral vein resection is anticipated.
- Tumor Assessment: Even with vessel invasion, the vessel sheath should be opened from the side opposite the tumor to assess the extent of invasion and ensure clear margins on the remaining vessel stump.
5. Soft Tissue Reconstruction and Closure
"With the tumor resected and vascular integrity restored, our next priority is to protect these vital structures and fill the dead space."
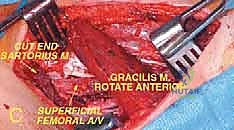
- Muscle Transfer (Gracilis or Sartorius): For large defects or after vascular reconstruction, a soft tissue flap is crucial to protect the vessels and the resection bed, minimizing complications like infection or graft exposure.
- The gracilis muscle transfer is an excellent option. We'll disconnect its distal insertion and rotate the muscle anteriorly. It can then be spread like a fan and reattached anteriorly to cover the exposed vessels and fill the defect.
- The gracilis muscle transfer is an excellent option. We'll disconnect its distal insertion and rotate the muscle anteriorly. It can then be spread like a fan and reattached anteriorly to cover the exposed vessels and fill the defect.
TECH FIG 1 • C. Soft tissue reconstruction with a gracilis muscle transfer affords good coverage of the vessels of the sartorial canal and is crucial. The distal end of the gracilis muscle is disconnected and rotated anteriorly. The muscle is then spread like a fan and reattached anteriorly.
* If the sartorius muscle was preserved, it can also be used to cover the defect.
* Hemostasis: Meticulous hemostasis is achieved throughout the wound using electrocautery and ligatures.
* Drains: Suction drains (e.g., Jackson-Pratt) are placed in the deep wound to prevent hematoma and seroma formation.
* Layered Closure: The fasciocutaneous flaps are meticulously reapproximated, followed by subcutaneous tissue and skin closure with staples or sutures.
Pearls and Pitfalls: Navigating the Challenges
Pearls for Success
- Early & Wide Exposure: Always err on the side of a longer incision and larger flaps. Inadequate exposure leads to compromised margins and increased risk to neurovascular structures.
- Proximal and Distal Vessel Control: This is the golden rule for any tumor near major vessels. Establish it before you touch the tumor.
- Meticulous Dissection: Use a combination of sharp and blunt dissection. Identify and preserve the saphenous nerve and its branches whenever oncologically feasible.
- Frozen Section Reliance: Don't hesitate to send multiple frozen sections, especially of fascial planes and vessel adventitia,
REFERENCES
-
Functional outcome is excellent. Because the surgical resection and postoperative radiation do not cross a joint line, there is no restriction in range of motion.
-
Eilber F, Eckardt J, Rosen G, et al. Large, deep, high-grade extremity sarcomas: treating tumors of the flexor fossae. Surg Oncol 1999; 8:211–214.
rius muscle or, if that was excised with the tumor, the adjacent gracilis muscle. A gracilis muscle transfer ( TECH FIG 1C ) is done by dissecting the distal end of the gracilis free and rotating the muscle anteriorly to cover the canal. This provides good soft tissue coverage.
-
Enneking WP, Spainer SS, Goodma MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res 1980; 153:106–120.
-
Enneking W, Spanier S, Malawer M. The effect of the anatomic setting on the results of surgical procedures for soft parts sarcoma of the thigh. Cancer 1981;47:1005–1022.
-
Gronchi A, Casali P, Olmi P, et al. Status of surgical margins and prognosis in adult soft tissue sarcomas of the extremities: a series of patients treated at a single institution. J Clin Oncol 2005;23: 96–104.
-
Malawer M, Sugarbaker P. Musculoskeletal Cancer Surgery. Norwell, MA: Kluwer Academic, 2001.
-
Peabody TD, Simon MA. Principles of staging of soft-tissue sarcomas. Clin Orthop Relat Res 1993;289:19–31.
-
Rooser B, Attewell R, Berg N, et al. Prognostication in soft tissue sarcoma. Cancer 1988;61:817–823.
You Might Also Like