Mastering Intercalary Reconstruction: Allografts and Segmental Endoprostheses
Key Takeaway
Step into the operating room for a masterclass on intercalary reconstruction. This guide covers comprehensive preoperative planning, precise anatomical considerations, and granular intraoperative execution for allografts and segmental prostheses. Learn critical techniques for oncologic resection, fixation, and managing potential pitfalls. Gain insights into postoperative care for optimal patient outcomes in complex limb salvage procedures.
Alright team, gather around. Welcome to the operating theater. Today, we're tackling one of the most challenging yet rewarding procedures in orthopaedic oncology: intercalary reconstruction. This isn't just about replacing a piece of bone; it's about restoring function, preserving a limb, and achieving oncologic control. You're scrubbed in with me, so pay close attention. Every decision, every cut, every screw matters.
Understanding Intercalary Reconstruction
Let's start with the basics, fellows. An intercalary reconstruction is precisely defined as the replacement of the diaphyseal portion of a long bone after a segmental skeletal resection, which we term a diaphysectomy. Our primary goal here is to maintain the patient's native joints, both proximal and distal to the reconstruction. This approach typically yields superior functional outcomes compared to more extensive limb-sparing procedures that necessitate joint replacement.
We have two main avenues for reconstruction: bulk allografts or modular intercalary endoprostheses. Most commonly, we lean towards bulk allografts, as they offer the potential for biological integration and long-term stability through osseous healing. However, allograft reconstruction isn't always feasible. In cases of poor host factors, such as compromised vascularity, small residual host segments, or in patients undergoing planned radiation or chemotherapy that could impede healing, an intercalary endoprosthetic reconstruction becomes our preferred option. This also holds true for patients who have experienced a prior failed allograft reconstruction. The beauty of modular intercalary prostheses is their inherent flexibility; they can be easily converted to a conventional endoprosthetic replacement, using joint-replacing modules at either end, either during the initial surgery or for future revisions.
Segmental prostheses offer immediate stable fixation, which allows for early rehabilitation and a rapid return of function. While aseptic loosening is a known complication with traditional endoprosthetic replacements, it is rarely, if ever, seen with intercalary implants. This is largely due to the absence of bearing surfaces that generate wear debris and the lack of exposure to joint fluid, both of which contribute to implant longevity. Newer implant designs have dramatically reduced the length of bone needed for stable fixation, thereby expanding the indications for these prostheses.
Comprehensive Surgical Anatomy
Before we make any incision, a deep understanding of the regional anatomy is paramount. We're not just operating on bone; we're navigating a complex landscape of neurovascular structures, muscle compartments, and osteological nuances.
Femoral Considerations
When we're operating on the femur, we must account for its natural anterior bow and the degree of femoral anteversion. These anatomical features are critical for proper alignment and rotational control during reconstruction. Most importantly, we must always be acutely aware of the superficial femoral artery (SFA). As it courses distally, especially near the adductor hiatus, it lies in close proximity to the posteromedial aspect of the distal femur. Unplanned injury to the SFA can lead to catastrophic limb ischemia, so meticulous dissection and protection are non-negotiable.
Tibial Considerations
For the tibia, the primary concern is the limited soft tissue coverage anteromedially. This makes wound closure challenging and increases the risk of wound complications and infection, particularly over the implant or allograft. Posteriorly, the posterior tibial neurovascular bundle – comprising the posterior tibial artery, veins, and tibial nerve – runs in close proximity to the posteromedial tibia. Again, precise identification and protection are crucial to avoid neurovascular compromise.
Humeral Considerations
In the humerus, the radial nerve is our most significant anatomical landmark and risk. It spirals around the posterior mid-humeral shaft within the spiral groove. During any dissection or fixation in this region, especially for tumor resection, careful identification and protection of the radial nerve are absolutely essential to prevent iatrogenic palsy.
Forearm Considerations
Finally, for the forearm, particularly the radius, we must consider the natural radial bow. This curvature is vital for normal forearm rotation and function. Any reconstruction must aim to replicate this natural contour to ensure optimal biomechanics.
Preoperative Planning: The Blueprint for Success
Alright team, let's talk about the bedrock of success in these complex cases: Preoperative Planning. This isn't just about reviewing images; it's about crafting a meticulous blueprint for every single step we'll take in the operating theater. We're dealing with oncologic resections here, and the stakes are incredibly high for both limb salvage and oncologic cure.
Comprehensive Imaging Review and Templating
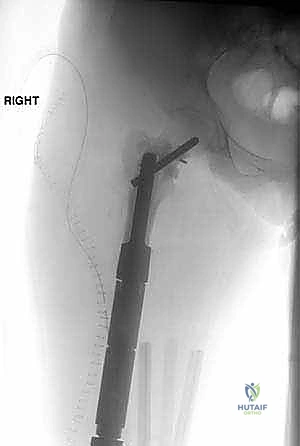
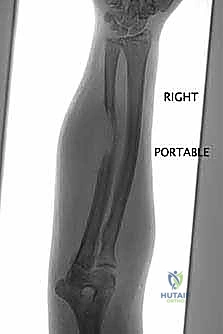
"First, we gather all our intelligence. This involves a multi-modality imaging approach. We start with plain radiographs – AP and lateral views are crucial. Look closely at the bone geometry, the exact size of the lesion, and critically, the remaining host bone stock. We need to assess its quality and quantity to ensure it can adequately support our planned reconstruction, whether it's an allograft or an endoprosthesis. Remember, inadequate bone stock means we must convert to a joint-replacing reconstruction, so this assessment is non-negotiable. Radiographs also give us our initial templating parameters for allograft sizing.

Here we see a preoperative AP radiograph, clearly delineating a diaphyseal lesion in the femur. This is our starting point for understanding the extent of bone involvement.
Next, Computed Tomography (CT) scanning is indispensable. This provides us with exquisite detail of the bone geometry and the extent of bone destruction by the lytic lesion. We use 3D reconstructions from the CT data to truly understand the tumor's bony footprint and plan our osteotomy levels with millimeter precision.
Then, Magnetic Resonance Imaging (MRI). This is our window into the soft tissue extension of the lesion, the intraosseous or marrow extent of the tumor, and its proximity to adjacent joints. Crucially, MRI assesses the neurovascular structures. We're looking at sagittal and coronal images to measure the exact resection length from stable anatomical landmarks, usually the adjacent joints, to our planned osteotomy levels. This gives us a reproducible method for identifying these levels intraoperatively, often using K-wires as guides.
Observe this coronal MRI image, demonstrating the intramedullary and extramedullary extent of the lesion. This is vital for defining our oncologic margins.
Another view of the coronal MRI, further solidifying our understanding of the tumor's reach.

And here, a sagittal MRI scan, critically showing the precise length of tumor to be resected. This measurement is key for our osteotomy planning.
Finally, a bone scan helps us rule out additional osseous sites of disease, a critical step in oncologic staging. While the role of Positron Emission Tomography (PET) scanning for sarcomas is still evolving, we often use it to assess metastatic disease, which can significantly alter our surgical strategy.
Surgical Strategy and Implant Selection
During this phase, we're not just looking at the tumor; we're templating our reconstruction. If we're considering an allograft, we'll order it from the bone bank, often requiring radiographs of the allograft itself to ensure a size match. For endoprosthetic implants, especially customized modular components, remember the lead time – typically 3 to 4 weeks for design and manufacturing. This isn't a last-minute decision, fellows.
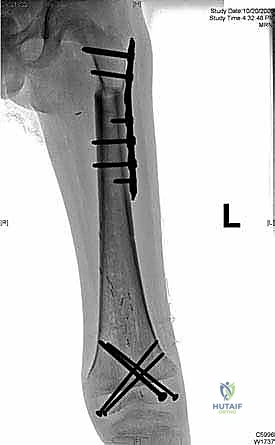
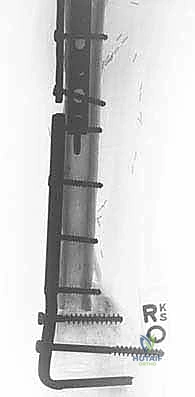
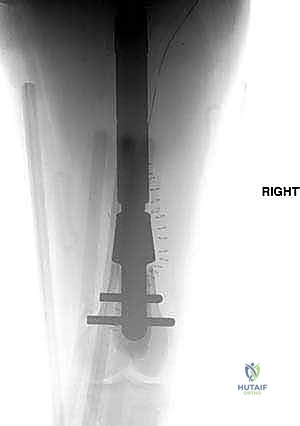
We also decide on the type and length of fixation. Plate fixation allows for standard osteosynthesis techniques and compression across the allograft-host junctions, which we believe improves healing. However, the screw holes created in the allograft are a recognized risk factor for late allograft fracture. Alternatively, intramedullary (IM) nail fixation, while potentially requiring additional incisions, generally provides stronger, more protective long-term fixation for the allograft without creating stress risers from screw holes. The challenge with IM fixation can be achieving compression at the host-graft junctions, which may impede healing. Sometimes, a combination of techniques is employed.
If a vascularized fibula graft is planned, its timing and the host location for harvesting must be determined well in advance. Remember, vascularized fibular grafts are not required for intercalary implants, only for allografts, particularly in areas of poor vascularity or in high-demand patients.
Soft Tissue Assessment and Rotational Profile
Don't forget the soft tissues! A thorough soft tissue evaluation around the mass or biopsy site is crucial to determine the resection approach and ensure sufficient tissue remains for primary closure. We must anticipate the need for alternative methods of wound closure, such as rotational muscle flaps, to minimize wound complications and infection.
Finally, an examination under anesthesia focusing on the rotational profile of the non-operative leg can be incredibly useful. This provides a baseline to ensure proper rotational alignment of the operative leg during reconstruction. Intraoperative C-arm fluoroscopy will be our indispensable guide to measure and select our planned osteotomy levels.
Patient Positioning: The Foundation of Exposure
Proper patient positioning is the unsung hero of complex oncologic resections. It dictates our exposure, access, and ability to manage potential complications.
Femoral Resections
For femoral resections, we typically position the patient either supine or in the lateral decubitus position. If supine, a bump under the ipsilateral buttock can facilitate exposure, but be cautious, as this might make clinical assessment of rotation more challenging later. Ensure the entire limb, from pelvis to foot, is prepped and draped free to allow full range of motion and intraoperative fluoroscopy.
Tibial Resections
Tibial cases are almost always performed with the patient in the supine position. Again, the entire leg must be free for manipulation and imaging.
Humeral Resections
For the humerus, we can utilize either the supine position or the beach chair position, depending on the specific location of the tumor and the surgeon's preference for exposure. Ensure adequate padding to prevent iatrogenic nerve palsies.
Forearm Reconstructions
Forearm reconstructions are performed with the patient supine, with the arm positioned and draped on a hand table. This provides stable support and optimal access to the forearm.
Surgical Approach: Navigating the Tumor Landscape
The surgical approach is dictated entirely by the incision required for an adequate oncologic resection of the tumor, taking into account the prior biopsy tract.
Femoral Approaches
For femoral reconstructions, an anterolateral or lateral approach to the thigh is often ideal, providing good access to the diaphysis. However, if the tumor is medially located or in close proximity to the neurovascular bundle, medial incisions may be necessary. This allows us to meticulously isolate and protect the superficial femoral artery and vein during the resection, minimizing the risk of vascular injury.
Tibial Approaches
Tibial reconstructions can be performed through an anterolateral or anteromedial approach. Be mindful that an anteromedial approach is more likely to necessitate complicated soft tissue coverage due to the limited soft tissue envelope over the tibia in this region. We must have a plan for robust soft tissue closure or flap coverage.
Humeral Approaches
Humeral resections typically require an extensile anteromedial approach. During this approach, extreme care must be taken to identify and protect the radial nerve as it crosses the posterior aspect of the humerus, especially when oncologically feasible.
Forearm Approaches
For radius reconstructions in the forearm, an anterior approach is generally preferred, providing optimal access while minimizing risk to surrounding structures.
The Oncologic Resection: Precision and Margins
Now, fellows, the moment of truth. We're going to perform the oncologic resection. This is where meticulous planning translates into precise execution.
Initial Exposure and Rotational Marking
"Scalpel, please. We'll proceed with the planned incision, carefully extending it to achieve adequate exposure while respecting our oncologic margins and prior biopsy tract. Once we're down to bone at the proximal and distal extents of our planned resection, we need to mark our bone carefully to ensure proper rotational orientation during reconstruction. This is critical for limb function. The linea aspera of the femur is an excellent anatomical landmark for rotational reference. Alternatively, we can place K-wires or make small, superficial cuts in the bone proximal and distal to the resection area, ensuring they are parallel to each other and perpendicular to the long axis of the bone. This gives us a reliable intraoperative reference."
Neurovascular Dissection and Soft Tissue Mobilization
"Next, we perform our pertinent vascular and neurologic dissection. Identify and protect all critical structures. Use vessel loops to gently retract and isolate the superficial femoral artery, vein, and any major nerves in the vicinity. This is not a step to rush. Once the neurovascular structures are safely out of the way, we meticulously dissect the soft tissues around the tumor mass, staying wide of our planned oncologic margins. We want to create a healthy tissue envelope around the resected area."
Defining Osteotomy Levels
"Now, we'll define our osteotomy levels. Using fluoroscopy and our preoperative measurements, we'll place K-wires perpendicular to the shaft of the bone at the planned proximal and distal osteotomy levels. This provides a precise, reproducible guide for our cuts. Take care to avoid excessive damage to the periosteum adjacent to the planned osteotomy, as this is crucial for future healing."
Performing the Osteotomy
"Power saw, please. We perform a transverse osteotomy with a power saw. Keep the saw blade constantly cooled with irrigant – saline works well – to prevent excessive heat generation. Thermal necrosis of the host bone can compromise healing and lead to nonunion. We want clean, perpendicular cuts. While stepped cuts are an option to increase host-allograft contact, they are more technically demanding, add surgical time, and can cause more periosteal damage. For most intercalary resections, a transverse cut is sufficient and allows for easier rotational adjustments."
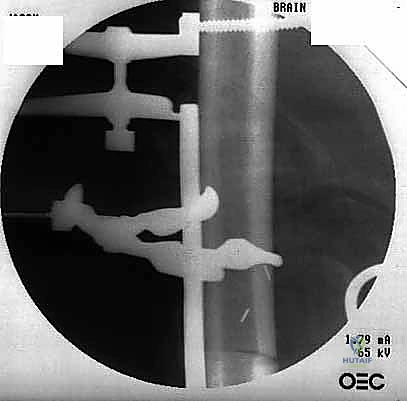
Here, you can see the power saw making a precise transverse osteotomy. Note the constant irrigation to prevent thermal damage to the bone.
Surgical Warning: Thermal Necrosis
Always irrigate your saw blade generously during osteotomy. Excessive heat can cause thermal necrosis of the host bone, leading to delayed union or nonunion at the host-allograft junction.
Specimen Removal and Margin Assessment
"Once both osteotomies are complete, we carefully remove the specimen. Hand me the ruler.
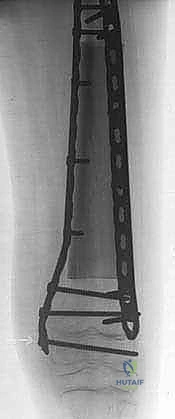
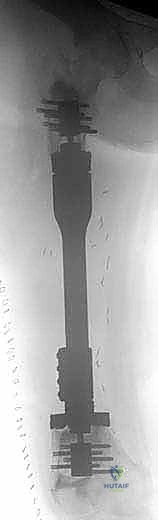
Additional Intraoperative Imaging & Surgical Steps












REFERENCES
-
Infection is the most common cause of allograft and prosthetic failure and can lead to secondary amputation. Aggressive surgical débridement with removal of all foreign bone or materials is necessary.
-
Henshaw RM. Complex massive intercalary endoprosthetic reconstruction of the femur and tibia: a new technique using customized compress implants augmented with cement. Musculoskeletal Tumor Society Annual Meeting 2006;45:61.
-
Makely JT. The use of allografts to reconstruct intercalary defects of long bones. Clin Orthop Relat Res 1988;197:58–75.
-
Muscolo LD, Ayerza MA, Aponte-Tinao LA, et al. Intercalary femur and tibia segmental allografts provide an acceptable alternative in reconstructing tumor resections. Clin Orthop Relat Res 2004;426: 97–102.
-
Muscolo LD, Ayerza MA, Aponte-Tinao LA, et al. Partial epiphyseal preservation and intercalary allograft reconstruction in high-grade metaphyseal osteosarcoma of the knee. J Bone Joint Surg Am 2004; 86A:2686–2692.
-
Sorger JI, Hornicek FJ, Zavatta M, et al. Allograft fractures revisited. Clin Orthop Relat Res 2001;382:66–74.
-
VanderGriend RA. The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76A:657–663.
-
Late fracture of massive allografts can lead to chronic pain and loss of function. Use of intramedullary fixation and avoiding screws in the allograft may help to minimize this complication.
-
Prosthetic loosening rarely if ever occurs for intercalary implants. Implant failure can be revised with use of a new prosthesis.
-
Degeneration of an adjacent joint after either allograft or intercalary implant reconstruction can be treated with surfacereplacing total joint arthroplasty.
You Might Also Like