Masterclass: Limb-Sparing Resection of Popliteal Fossa Sarcomas

Key Takeaway
This masterclass guides orthopaedic fellows through limb-sparing popliteal fossa sarcoma resection. We cover meticulous preoperative planning, exact patient positioning, and comprehensive surgical anatomy focusing on neurovascular structures. Follow a granular, real-time intraoperative execution from incision to closure, emphasizing technique, instrument use, and critical decision-making. Learn pearls, pitfalls, and postoperative care for optimal outcomes.
Introduction and Epidemiology
Soft tissue sarcomas (STS) of the popliteal fossa represent a rare and anatomically formidable subset of musculoskeletal malignancies, accounting for less than 5% of all extremity soft tissue sarcomas. Despite their relative infrequency, the surgical management of tumors in this specific anatomic compartment presents exceptional challenges to the orthopedic oncologist. Achieving a wide, en bloc resection with negative oncologic margins (R0) is inherently constrained by the tight, unyielding periarticular space and the immediate proximity of the tumor pseudocapsule to critical neurovascular structures.
Historically, the inability to clear these margins without sacrificing the primary neurovascular bundle dictated that transfemoral amputations were the definitive standard of care to ensure local oncologic control. However, modern sarcoma management has undergone a profound paradigm shift. Enhanced comprehension of tumor biology, the advent of high-resolution cross-sectional imaging, and the strategic integration of neoadjuvant radiotherapy and systemic chemotherapy now facilitate limb-sparing procedures in over 85% of these complex cases.
The histologic subtypes most frequently encountered in the popliteal fossa include undifferentiated pleomorphic sarcoma (UPS, formerly classified as malignant fibrous histiocytoma), synovial sarcoma, myxoid and dedifferentiated liposarcoma, and leiomyosarcoma. The aggressive biological behavior of these high-grade tumors necessitates a highly coordinated multidisciplinary approach. While local control is primarily a surgical mandate, systemic disease control and the eradication of micro-metastatic foci rely heavily on neoadjuvant and adjuvant medical oncology.
A critical, yet historically underemphasized, aspect of limb-salvage surgery in the posterior knee is the meticulous preservation of the superficial venous system—specifically, the greater saphenous vein (GSV). Because popliteal sarcomas frequently abut, encase, or directly invade the popliteal vein, en bloc resection of the deep venous system is sometimes an unavoidable oncologic necessity. In such scenarios, the GSV rapidly transitions into the primary, indispensable conduit for the venous outflow of the entire lower leg. Iatrogenic injury to the GSV during medial surgical exposure or subsequent gastrocnemius flap mobilization can precipitate catastrophic postoperative venous hypertension, severe intractable lymphedema, acute compartment syndrome, and ultimately, delayed amputation due to limb unviability.
Surgical Anatomy and Biomechanics
Osteofascial Boundaries of the Popliteal Fossa
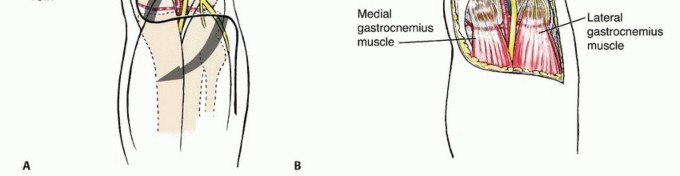
The popliteal space is a complex, diamond-shaped anatomic transition zone bridging the posterior thigh and the lower leg. Superiorly, it is delineated by the diverging hamstring muscles: the semimembranosus and semitendinosus form the superomedial border, while the long and short heads of the biceps femoris establish the superolateral border. Inferiorly, the fossa is bounded by the converging medial and lateral heads of the gastrocnemius muscle.
The roof (posterior aspect) of the fossa is formed by the popliteal fascia, a thin but exceptionally resilient aponeurotic sheet continuous with the fascia lata proximally and the deep crural fascia distally. The floor (anterior aspect) is composed of the posterior, flat surface of the distal femur (the popliteal surface), the posterior capsule of the knee joint (reinforced by the oblique popliteal ligament), and the popliteus muscle investing the proximal tibia.
Anatomic boundaries and deep structures of the popliteal fossa, highlighting the diamond-shaped configuration.
Arterial and Venous Architecture
The popliteal artery and vein enter the superior aspect of the popliteal space medially, traversing the adductor hiatus (Hunter's canal), and course obliquely and laterally to lie directly apposed to the posterior capsule of the knee joint. The popliteal artery is the deepest central structure within the fossa. It gives rise to a rich, redundant periarticular anastomotic network consisting of the paired superior genicular arteries, a single middle genicular artery (which pierces the oblique popliteal ligament to supply the cruciate ligaments), and the paired inferior genicular arteries. After passing deep to the tendinous arch of the soleus, the popliteal artery bifurcates into the anterior tibial artery and the tibioperoneal trunk.

Arterial anatomy of the popliteal fossa, demonstrating the genicular branching patterns and distal trifurcation.
The popliteal vein is situated superficial (posterior) to the popliteal artery and slightly lateral to it in the proximal segment of the fossa, before crossing to the medial side as it descends.
Peripheral Nerve Topography
The central neurovascular structures are bisected longitudinally by the tibial nerve, which is the most superficial and direct continuation of the sciatic nerve. The common peroneal nerve diverges laterally from the sciatic bifurcation, closely following the medial border of the biceps femoris tendon. It exits the popliteal fossa by wrapping anteriorly around the fibular neck, making it highly vulnerable to traction injuries during lateral retraction.
Topographic relationship of the sciatic nerve bifurcation, tibial nerve, and common peroneal nerve within the popliteal space.
Venous Hemodynamics and the Greater Saphenous Vein Conduit
Comprehensive knowledge of venous hemodynamics is paramount in popliteal sarcoma surgery. The short saphenous vein (SSV) ascends the posterior midline of the calf, piercing the popliteal fascia to terminate in the popliteal vein. In the context of posterior compartment resections, the SSV is routinely sacrificed en bloc with the tumor.
Conversely, the greater saphenous vein (GSV) courses medially along the leg and thigh, remaining anatomically distinct from the popliteal fossa proper. Under normal physiologic conditions, the deep venous system (popliteal vein and its tributaries) accommodates 85% to 90% of the lower extremity's venous return. When oncologic principles dictate the resection of the popliteal vein, the venous hemodynamics are abruptly shunted to the superficial system. The GSV must rapidly dilate to manage this massive volume overload. If the GSV is compromised—whether by preexisting deep vein thrombosis, prior venous stripping, or iatrogenic transection during medial surgical approaches—the limb will experience profound, often irreversible venous congestion.
Indications and Contraindications
The surgical decision-making algorithm for complex popliteal resections demands a meticulous balance between securing an R0 oncologic margin and preserving a functional, sensate, and biomechanically viable extremity.
| Clinical Scenario | Management Strategy | Rationale and Oncologic Considerations |
|---|---|---|
| Operative Limb Salvage | Wide local excision, neurovascular preservation or reconstruction | The gold standard for localized STS. Feasibility requires intact or reconstructable arterial inflow and at least one robust venous outflow tract (e.g., an uncompromised GSV). |
| Operative Amputation | Above-knee amputation (AKA) or through-knee amputation | Indicated for massive, multi-compartmental tumors, complete encasement of the sciatic/tibial nerve precluding functional salvage, or extensive vascular involvement where both bypass grafting and superficial venous return (GSV) are compromised. |
| Neoadjuvant Therapy | Preoperative external beam radiotherapy (EBRT) and/or systemic chemotherapy | Utilized to sterilize peripheral reactive zones, reduce tumor volume, and induce a fibrous pseudocapsule. This frequently separates the tumor from critical neurovascular structures, converting an unresectable lesion into a limb-salvage candidate. |
Absolute and Relative Contraindications to Limb Salvage:
1. Neurovascular Encasement: Inability to achieve negative margins without the simultaneous sacrifice of all major motor nerves (sciatic/tibial and common peroneal), resulting in a flail, insensate limb.
2. Vascular Unreconstructability: Complete encasement of the popliteal artery and vein in a patient with severe baseline peripheral arterial disease or an absent superficial venous system (e.g., prior GSV harvest for coronary artery bypass grafting).
3. Severe Baseline Dysfunction: Preexisting functional impairment where a modern prosthetic limb following amputation would provide superior ambulatory capacity compared to a heavily morbid, salvaged limb.
Pre Operative Planning and Patient Positioning
Advanced Cross-Sectional and Vascular Imaging
Rigorous preoperative imaging is the absolute cornerstone of surgical planning in the popliteal fossa. Magnetic Resonance Imaging (MRI) with and without gadolinium contrast is mandatory. T1-weighted sequences provide superior anatomic definition of muscle compartment architecture and fascial boundaries. T2-weighted and Short Tau Inversion Recovery (STIR) sequences are essential for delineating peritumoral edema, identifying satellite nodules, and mapping the true extent of the reactive zone.
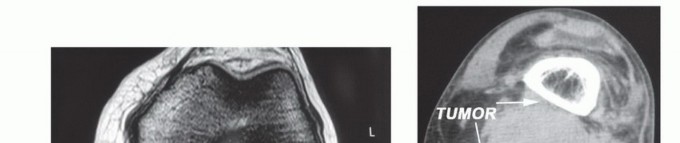
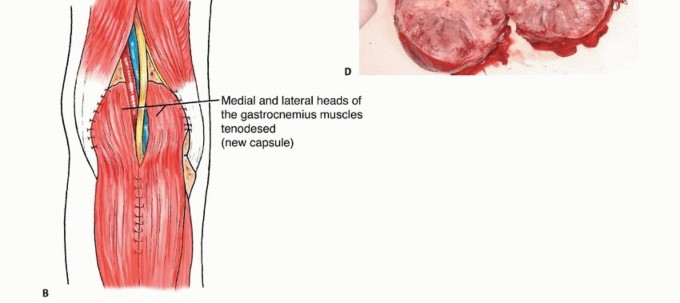
Normal axial MRI of the distal popliteal space (diamond configuration) at the level of the medial and lateral gastrocnemius muscle insertions onto the femoral condyles.
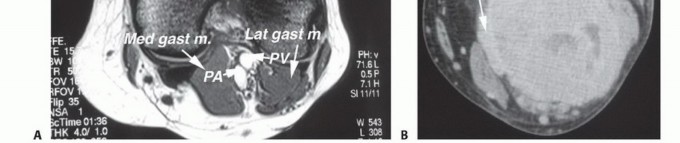
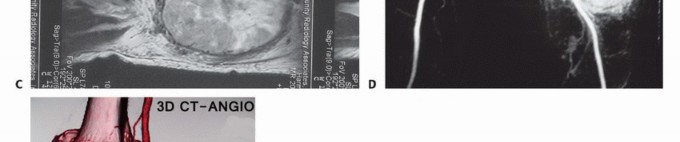
Axial MRI demonstrating a large popliteal soft tissue sarcoma causing significant posterior displacement and compression of the central neurovascular bundle.
Sagittal and axial planes are particularly critical for evaluating the tumor's proximity to the posterior capsule of the knee joint and the distal femoral cortex. If the posterior capsule is breached or intimately involved, an extra-articular resection incorporating the posterior capsule, or a partial intra-articular resection, must be templated.
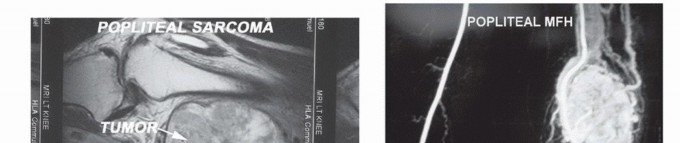
Sagittal MRI sequence illustrating the intimate relationship of a popliteal sarcoma to the posterior distal femur and the articular knee joint capsule.
Computed Tomography (CT) Angiography or conventional digital subtraction angiography (DSA) is highly recommended for large, hypervascular tumors. Angiography allows the surgical team to map arterial displacement, identify dominant feeding vessels (frequently the sural or genicular arteries), and plan for potential interposition vascular reconstruction. In highly vascularized subtypes, preoperative selective arterial embolization can drastically mitigate intraoperative hemorrhage.
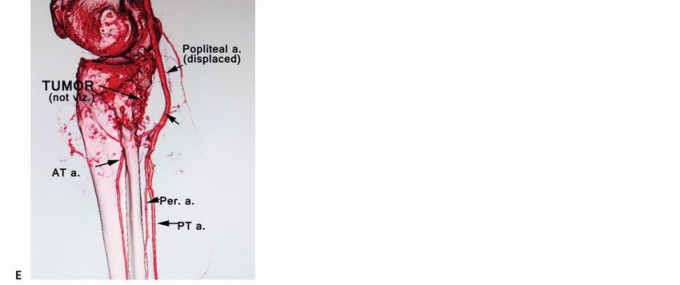
Digital subtraction angiogram of a hypervascular popliteal sarcoma. Preoperative arterial embolization is a valuable adjunct to minimize intraoperative blood loss.
Oncologic Biopsy Principles
Histologic diagnosis must be confirmed via an image-guided core needle biopsy prior to definitive surgical intervention. The biopsy tract must be meticulously planned by the operating surgeon to ensure it can be excised en bloc with the tumor specimen. For popliteal masses, the biopsy approach should be strictly posterior and midline. Medial or lateral approaches risk contaminating pristine tissue planes, thereby jeopardizing future reconstructive flap coverage or inadvertently injuring the GSV.
Patient Positioning and Operative Preparation
The patient is typically positioned prone on a radiolucent Jackson table or standard operating table with chest and pelvic rolls. Meticulous padding of all bony prominences (anterior superior iliac spines, patellae, and thorax) is required to prevent pressure necrosis and positioning neuropraxia. A sterile pneumatic tourniquet is placed on the proximal thigh. While the tourniquet is frequently left uninflated to allow continuous assessment of tissue perfusion and identification of small vascular pedicles, it remains essential for rapid hemostatic control in the event of catastrophic major vessel injury.
The entire lower extremity, from the iliac crest to the toes, must be prepped and draped free. This facilitates intraoperative manipulation of the knee (flexion relaxes the posterior neurovascular structures and the gastrocnemius complex), allows continuous assessment of distal pedal pulses, and provides immediate access to the contralateral limb if an autologous reversed saphenous vein graft is required for arterial reconstruction.
Detailed Surgical Approach and Technique
Incision Design and Superficial Dissection
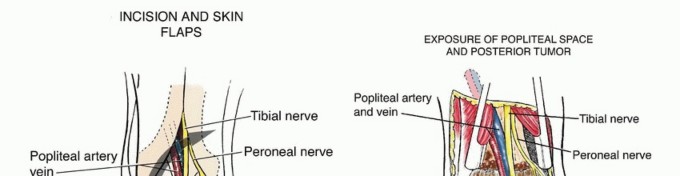
The surgical approach utilizes an expansile lazy-S or Z-type incision traversing the popliteal fossa. Transverse incisions, though historically described for benign pathology, offer severely limited proximal and distal extension and are universally avoided in oncologic resections. The vertical limbs of the incision are strategically placed to allow proximal access to the medial and lateral hamstring compartments and distal access to the gastrocnemius heads.
Expansile lazy-S incision designed for complex popliteal resections, allowing extensive proximal and distal exposure.
During the superficial dissection, full-thickness fasciocutaneous flaps are raised. It is during this precise stage that the Greater Saphenous Vein must be actively identified and protected. The medial skin flap should not be aggressively undermined. The surgeon must locate the GSV within the medial subcutaneous adipose tissue and ensure it is gently retracted with the medial flap, completely isolating it from the zone of oncologic resection.

Superficial dissection highlighting the medial skin flap. Extreme care is taken to avoid deep medial dissection that could compromise the GSV.

Identification and isolation of the Greater Saphenous Vein, ensuring it remains safeguarded during the deep oncologic extirpation.
The short saphenous vein is identified in the distal apex of the incision, coursing between the medial and lateral heads of the gastrocnemius. For centrally located tumors, the SSV is typically ligated and divided at its proximal confluence with the popliteal vein to facilitate deep exposure.
Neurovascular Isolation and Proximal Control
The fundamental tenet of sarcoma surgery in the popliteal fossa is the identification and isolation of major neurovascular structures in normal, un-involved tissue planes proximal and distal to the tumor before approaching the reactive pseudocapsule.
Early identification of the sciatic nerve proximal to the tumor mass, securing it with vessel loops for safe manipulation.
Proximally, the sciatic nerve is identified deep to the long head of the biceps femoris. It is traced distally to its bifurcation. Vessel loops are passed around the tibial and common peroneal nerves. The common peroneal nerve is traced laterally along the biceps tendon; it is exquisitely sensitive to traction injury and must be handled with minimal tension. The tibial nerve is traced centrally. In cases where the nerve is adherent to the posterior aspect of the tumor pseudocapsule, the epineurium can sometimes be meticulously dissected off the tumor under loupe magnification, though this constitutes an R1 (microscopically positive/marginal) resection along the nerve sheath.
Distal tracing of the tibial and common peroneal nerves, ensuring they are completely liberated from the tumor pseudocapsule prior to vascular dissection.
Vascular Mobilization and Tumor Extirpation
Following neurologic protection, attention is directed to the popliteal vessels. Proximally, the popliteal artery and vein are identified as they exit the adductor hiatus. Distally, they are controlled as they pass deep to the soleus bridge.
Vascular control achieved proximal and distal to the tumor. All feeding genicular and sural branches are systematically ligated.
All small venous and arterial pedicles feeding the tumor must be meticulously ligated and divided using hemoclips or suture ligatures. The use of monopolar electrocautery in close proximity to the main popliteal vessels is strictly avoided to prevent delayed thermal necrosis and subsequent pseudoaneurysm formation.
If the popliteal artery is intimately encased, a vascular surgeon should be integrated into the operative team to perform an en bloc resection and interposition bypass graft. Autologous reversed GSV from the contralateral limb is the conduit of choice, though synthetic grafts (e.g., PTFE) may be used. Autologous tissue is vastly preferred in oncologic fields prone to wound complications or those that have received neoadjuvant radiation.

En bloc resection of the popliteal vessels when intimately involved with the sarcoma, necessitating immediate vascular reconstruction.
If the popliteal vein is encased, it is ligated proximally and distally and resected en bloc. It is a widely accepted surgical principle that the popliteal vein does not require routine reconstruction provided the Greater Saphenous Vein is anatomically intact. Venous reconstruction in the popliteal space is fraught with prohibitively high rates of thrombosis due to the low-flow venous state and mechanical kinking during postoperative knee flexion.
En Bloc Resection Mechanics
With the neurovascular bundle mobilized and protected (or resected and reconstructed), the muscular boundaries of the tumor are addressed. Depending on preoperative MRI mapping, portions of the semimembranosus, biceps femoris, or gastrocnemius heads are divided using electrocautery. The resection proceeds methodically from superficial to deep.

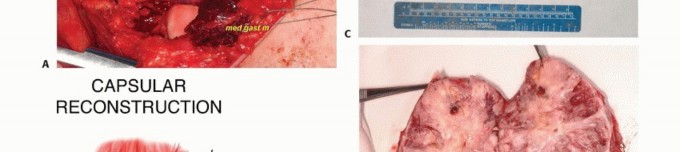
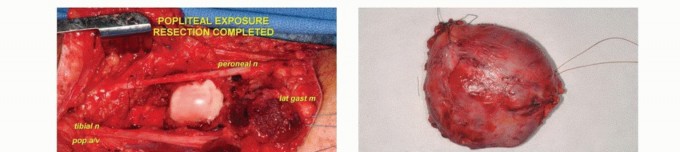
Delivery of the tumor en bloc. The deep margin often consists of the posterior knee capsule or the popliteus muscle fascia.
The deep margin is frequently the posterior capsule of the knee or the popliteum. If the tumor is fixed to the posterior capsule, the capsule is incised, and an extra-articular resection is performed, exposing the articular cartilage of the femoral condyles. Care must be taken not to violate the articular surface unless oncologically mandated. The tumor bed is then heavily irrigated with sterile water (to induce hypotonic tumor cell lysis) and meticulous hemostasis is achieved.
Dead Space Management and Soft Tissue Reconstruction
Extirpation of a large popliteal sarcoma leaves a massive dead space, exposing the neurovascular bundle and potentially the knee joint. Primary closure is often impossible and oncologically ill-advised due to the profound risk of seroma formation, wound dehiscence, and subsequent neurovascular desiccation or graft blowout.

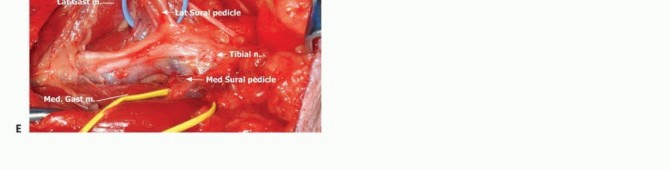
Significant dead space following en bloc resection, highlighting the exposed neurovascular structures requiring vascularized soft tissue coverage.
A pedicled medial or lateral gastrocnemius rotational flap is the reconstructive workhorse for the popliteal fossa. The medial gastrocnemius is generally preferred due to its larger muscle belly volume and longer arc of rotation. During the harvest of the medial gastrocnemius flap, the surgeon must exercise extreme caution to avoid injuring the Greater Saphenous Vein, which lies in the immediate overlying subcutaneous tissue. The flap is rotated into the defect to obliterate dead space and provide robust, well-vascularized tissue over the nerves and vessels. Closed suction drains are placed deep in the wound bed, and the skin is closed in anatomic layers.
Complications and Management
Surgical intervention in the popliteal fossa carries a formidable morbidity profile. This is particularly true in the setting of neoadjuvant radiation therapy, which causes profound microvascular endarteritis and significantly impairs local tissue healing.
| Complication | Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Wound Dehiscence / Necrosis | 15% - 30% | Prevention: Avoid acute-angle incisions; utilize prophylactic gastrocnemius flaps for coverage; minimize undermining of skin flaps. Salvage: Aggressive surgical debridement, negative pressure wound therapy (NPWT), split-thickness skin grafting, or free tissue transfer (e.g., anterolateral thigh flap). |
| Venous Congestion / Lymphedema | 10% - 25% | Prevention: Meticulous identification and protection of the Greater Saphenous Vein during exposure and flap harvest. Salvage: Strict limb elevation, compressive wrapping (only after arterial inflow is confirmed via ABI), and long-term use of graduated compression garments. |
| Neurologic Deficit (Motor/Sensory) | 5% - 15% |
Clinical & Radiographic Imaging



You Might Also Like


