Masterclass in Wide Resection and Reconstruction of Soleus Muscle Sarcomas
Key Takeaway
This masterclass guides orthopaedic fellows through wide soleus muscle sarcoma resection. We cover meticulous preoperative planning, detailed surgical anatomy, precise intraoperative steps including neurovascular protection, and advanced Gore-Tex reconstruction techniques. Emphasis is placed on achieving negative margins while preserving limb function. Postoperative care and complication management are also thoroughly discussed, ensuring comprehensive understanding of this challenging procedure.
Introduction and Epidemiology
The management of soft tissue sarcomas (STS) of the lower extremity has undergone a profound paradigm shift over the last several decades. Historically, high-grade sarcomas involving the deep compartments of the leg, particularly the triceps surae, were managed with radical ablative procedures, typically above-knee amputations, to ensure local oncologic control. Today, the standard of care is limb-sparing surgery, a transition made possible by the evolution of advanced cross-sectional imaging, the strategic implementation of neoadjuvant and adjuvant radiotherapy, and a more sophisticated understanding of musculoskeletal oncology principles.
Tumors arising within the soleus muscle represent a distinct and challenging subset of lower extremity sarcomas. The soleus is deeply situated, intimately associated with the major neurovascular bundle of the posterior leg (the tibial nerve and popliteal/tibial vessels), and covered by the gastrocnemius muscle. Achieving a wide, en bloc resection with negative microscopic (R0) margins while simultaneously preserving the heads of the gastrocnemius demands meticulous surgical technique. The bipartite goal of this procedure is to eradicate the local tumor burden while maximizing postoperative functional capacity. By carefully delaminating the soleus and preserving the gastrocnemius heads alongside their discrete neurovascular pedicles, orthopedic oncologists can successfully salvage a highly functional limb with powerful push-off capabilities. This comprehensive review delineates the anatomical, surgical, and oncologic principles governing soleus resection for primary soft tissue sarcomas.
Surgical Anatomy and Biomechanics
A profound mastery of the superficial and deep posterior compartments of the leg is the absolute prerequisite for executing a safe and oncologically sound soleus resection. The triceps surae acts as a powerful functional unit, but its components possess distinct anatomical origins, insertions, and neurovascular supplies, which allows for selective resection.
Anatomy of Triceps Surae Muscle
The triceps surae represents the primary plantarflexor apparatus of the ankle joint. It is composed of the biarticular gastrocnemius, the uniarticular soleus, and the vestigial plantaris.
Figure: Overview of the triceps surae muscle system, illustrating its role as the primary plantarflexor of the ankle.
The gastrocnemius muscle is the most superficial muscle of the posterior compartment. It is a bipennate structure consisting of predominantly Type II (fast-twitch) muscle fibers, making it vital for explosive movements such as jumping and sprinting.
* Medial head: Originates from the popliteal surface of the femur, just superior to the medial femoral condyle. It is anatomically larger and extends further distally than the lateral head.
* Lateral head: Originates from the lateral surface of the lateral femoral condyle.
Both heads converge distally to form a broad aponeurosis that merges with the soleus tendon to form the Achilles (calcaneal) tendon.
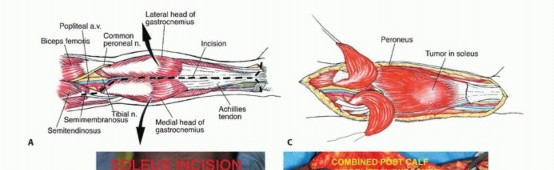
Figure: The bipennate structure of the gastrocnemius muscle, highlighting the distinct medial and lateral heads.
Deep to the gastrocnemius lies the soleus muscle. This is a broad, thick, unipennate muscle composed predominantly of Type I (slow-twitch) muscle fibers, reflecting its primary role as a postural muscle responsible for sustained standing and walking. Its origins are extensive and complex:
* The posterior aspect of the fibular head and the superior quarter of the posterior fibular shaft.
* The soleal line on the posterior surface of the tibia.
* The middle third of the medial border of the tibia.
* The fibrous soleal arch (arcade of the soleus), which spans between the tibial and fibular origins. This arch is a critical surgical landmark, as the popliteal vessels and tibial nerve pass directly beneath it to enter the deep posterior compartment.
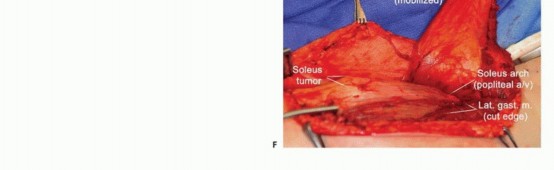
Figure: The deep anatomical orientation of the soleus muscle, demonstrating its extensive origins across the tibia and fibula.
The plantaris muscle is a small, functionally insignificant muscle originating from the lateral supracondylar line of the femur. Its long, slender tendon descends obliquely between the gastrocnemius and soleus. During tumor resection, the plantaris tendon must be correctly identified, as it can be inadvertently confused with the sural nerve or minor vascular structures.
Neurovascular Supply of Triceps Surae
The feasibility of resecting the soleus while preserving the gastrocnemius relies entirely on their independent neurovascular pedicles.
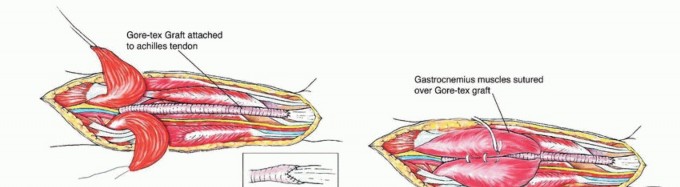
Figure: The tibial nerve (L4-S3) descending through the popliteal fossa, providing distinct branches to the triceps surae.
- Nerve Supply: Innervation to the entire triceps surae is provided by the tibial nerve (L4-S3).
- The medial and lateral heads of the gastrocnemius receive discrete branches from the tibial nerve high in the popliteal fossa. These branches enter the deep surface of the proximal muscle bellies.
- The soleus receives multiple branches from the tibial nerve. A proximal branch often enters the superficial (posterior) surface of the muscle near the soleal arch, while additional distal branches may enter the deep (anterior) surface.
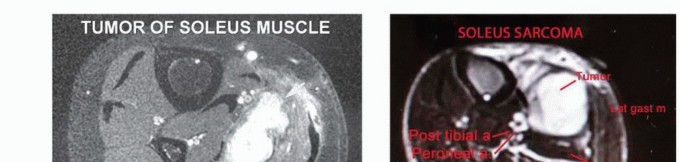
Figure: The complex arterial supply of the posterior leg, illustrating the sural arteries and the deep posterior tibial and fibular vessels.
- Arterial Supply:
- The gastrocnemius heads are supplied by the sural arteries (medial and lateral), which are direct branches of the popliteal artery. These vessels are end-arteries; their preservation is non-negotiable if the gastrocnemius is to survive.
- The soleus has a robust, segmental blood supply. Proximally, it receives contributions from the popliteal artery and sural arteries. Distally, it is supplied by numerous perforating branches from the posterior tibial artery and the fibular (peroneal) artery. This segmental supply requires meticulous ligation during en bloc resection to prevent significant hemorrhage.
- Venous Drainage: Venous drainage mirrors the arterial supply, utilizing venae comitantes that ultimately empty into the popliteal vein.
Biomechanical Implications of Soleus Resection
The biomechanical roles of the gastrocnemius and soleus dictate the functional outcome of the surgery. Because the gastrocnemius crosses both the knee and ankle joints, its efficiency as a plantarflexor is highly dependent on knee position (most effective with the knee extended). The soleus, crossing only the ankle joint, is the primary plantarflexor regardless of knee flexion.
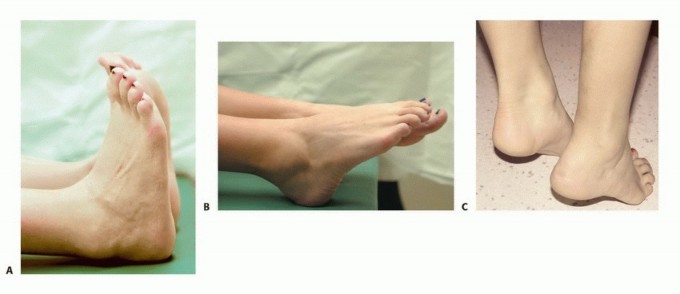
En bloc resection of the soleus results in a measurable deficit in sustained plantarflexion strength and endurance. Patients often experience fatigue during prolonged walking or standing. However, by meticulously preserving the gastrocnemius heads and their innervation, the patient retains explosive push-off strength and active plantarflexion. This selective resection avoids the profound and disabling drop-foot or complete loss of plantarflexion that would accompany a total posterior compartmentectomy.
Indications and Contraindications
The decision to perform a limb-sparing soleus resection requires a rigorous multidisciplinary evaluation. The primary objective is oncologic clearance; functional preservation, while critical, remains secondary to achieving an R0 margin.
Indications for Soleus Resection
- Primary Soleus Malignancy: Confirmed histological diagnosis of a primary soft tissue sarcoma (e.g., Undifferentiated Pleomorphic Sarcoma [UPS], Myxoid Liposarcoma, Synovial Sarcoma, Leiomyosarcoma) localized to the soleus muscle.
- Resectability with Negative Margins: High-resolution MRI must confirm that the tumor can be excised with a margin of normal, healthy tissue without sacrificing critical structures required for limb viability (specifically, the main trunk of the tibial nerve and the popliteal/tibial vessels).
- Favorable Neoadjuvant Response: Tumors that initially abut critical structures may become resectable following neoadjuvant radiotherapy or chemotherapy. Radiation often induces the formation of a fibrous pseudocapsule, creating a safer surgical plane.
- Adequate Patient Performance Status: The patient must be medically optimized to tolerate a major surgical procedure, potential reconstructive flap coverage, and an extended rehabilitation protocol.
Contraindications to Soleus Resection
- Irresectability (Absolute Contraindication): Tumor encasement of the tibial nerve, popliteal artery, or popliteal vein where segmental resection and grafting are not feasible or would result in a functionally useless limb. Extensive infiltration into the tibia or fibula requiring massive bone resection may also favor amputation.
- Diffuse Compartment Involvement: Tumor extending widely into the deep posterior compartment or completely infiltrating the gastrocnemius heads, precluding selective preservation.
- Uncontrollable Systemic Disease: In the presence of rapidly progressive, widespread metastatic disease, aggressive local control via morbid limb-salvage surgery may be contraindicated in favor of palliative management or amputation for symptom control.
- Severe Comorbidities: Patients with severe peripheral vascular disease or profound neuropathy in the affected limb may have unacceptable complication rates or poor functional outcomes post-resection.
Operative vs Non Operative Indications Summary
| Clinical Variable | Operative Considerations (Limb Salvage) | Non-Operative or Amputation Considerations |
|---|---|---|
| Tumor Extent | Confined to soleus; clear fascial planes separating tumor from gastrocnemius and major neurovascular bundles. | Diffuse infiltration of triceps surae; encasement of tibial nerve or popliteal vessels; extensive bone invasion. |
| Oncologic Margins | High probability of achieving wide or marginal (R0) margins based on preoperative MRI. | Inability to achieve R0 margins without sacrificing limb viability or causing unacceptable functional loss. |
| Neoadjuvant Response | Tumor downstaging or pseudocapsule formation following RT/chemotherapy. | Tumor progression through neoadjuvant therapy; fungating tumor; intractable pain requiring immediate palliation. |
| Systemic Disease | Localized disease or stable, oligometastatic disease where local control improves quality of life. | Widespread, uncontrolled metastatic disease with short life expectancy (palliation preferred). |
| Patient Status | Medically fit for prolonged anesthesia; highly motivated for aggressive rehabilitation. | High perioperative risk; severe peripheral vascular disease; non-ambulatory baseline status. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful musculoskeletal oncology surgery. The margin of error in the posterior compartment is minimal.
Preoperative Planning Protocol
- Multidisciplinary Tumor Board (MDT): Mandatory presentation at a sarcoma-specific MDT comprising orthopedic oncologists, medical oncologists, radiation oncologists, musculoskeletal radiologists, and soft tissue pathologists.
- Advanced Imaging:
- MRI: The gold standard. Requires T1-weighted, T2-weighted fat-suppressed, and post-gadolinium contrast sequences. Essential for evaluating the relationship between the tumor pseudocapsule, the soleal arch, the tibial nerve, and the vascular bifurcations.
- CT/PET-CT: CT of the chest is mandatory for metastasis screening (lungs are the most common site for STS metastasis). PET-CT may be utilized for grading and staging of high-grade lesions.
- Biopsy Tract Planning: Core needle biopsy must be planned meticulously. The tract must be placed in-line with the definitive surgical incision (longitudinal, posterior midline) so that the entire tract can be excised en bloc with the tumor specimen. Trans-compartmental biopsies are strictly contraindicated.
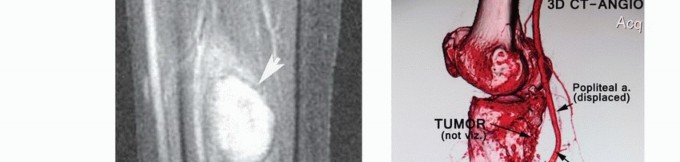
- Vascular Mapping: If the tumor is in close proximity to the popliteal trifurcation, CT Angiography (CTA) or MR Angiography (MRA) is indicated to define vascular anatomy and plan for potential vessel sacrifice and bypass.
- Reconstructive Planning: Collaboration with plastic surgery is advised if a massive soft-tissue defect is anticipated, particularly in the setting of preoperative radiotherapy, which compromises local wound healing.
Patient Positioning
The patient is positioned prone to provide unhindered access to the posterior thigh, popliteal fossa, and posterior leg.
- Padding and Protection: Standard prone positioning protocols apply. Chest rolls are utilized to free the abdomen, reducing inferior vena cava compression and minimizing epidural venous bleeding. All bony prominences (face, iliac crests, patellae, anterior ankles) must be meticulously padded.
- Limb Positioning: The operative limb is prepped and draped freely to allow intraoperative manipulation (knee flexion/extension, ankle dorsiflexion/plantarflexion). A sterile bump may be placed under the anterior ankle to maintain slight knee flexion, relaxing the tension on the gastrocnemius and neurovascular structures.
- Tourniquet: A sterile pneumatic tourniquet is applied to the proximal thigh. Exsanguination is typically performed via elevation rather than an Esmarch bandage to avoid theoretical tumor embolization, though this remains debated.
- Incision Marking: The planned incision and the biopsy tract are marked prior to skin preparation.
Detailed Surgical Approach and Technique
The surgical technique demands meticulous dissection, adherence to oncologic planes, and profound respect for the neurovascular anatomy.
Incision and Initial Dissection
- Incision: A long, longitudinal incision is made over the posterior midline of the calf. It must incorporate the biopsy tract within an elliptical excision. The incision typically extends from the inferior aspect of the popliteal fossa to the distal third of the leg.
- Superficial Dissection: Dissection proceeds through the subcutaneous fat. The sural nerve and lesser saphenous vein are identified. Depending on tumor location and the required margins, these structures are either mobilized and protected or sacrificed if they lie within the necessary oncologic margin.
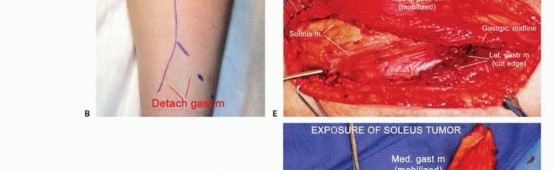
Figure: Initial longitudinal incision and superficial dissection, exposing the deep fascia of the posterior compartment.
Exposure of the Triceps Surae
- Fasciotomy: The deep investing fascia of the leg is incised longitudinally. This exposes the superficial surface of the gastrocnemius muscle.
- Gastrocnemius Mobilization: The median raphe separating the medial and lateral heads of the gastrocnemius is identified. The heads are carefully mobilized and retracted medially and laterally. This opens the avascular internervous plane between the gastrocnemius superficially and the soleus deeply.
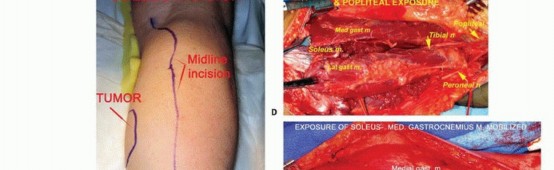
Figure: The medial and lateral heads of the gastrocnemius are retracted to reveal the underlying soleus muscle.
Identification and Preservation of Neurovascular Structures
- Popliteal Fossa Dissection: Dissection begins proximally in the popliteal fossa. The tibial nerve is identified first, as it is the most superficial structure in the neurovascular bundle. Deep and slightly medial to the nerve lie the popliteal vein and artery.
- Sural Artery Preservation: The medial and lateral sural arteries are identified as they branch from the popliteal artery and enter the proximal bellies of the gastrocnemius. These pedicles are isolated with vessel loops and protected throughout the case.
- Tracing the Tibial Nerve: The tibial nerve is traced distally as it dives beneath the soleal arch.

Figure: Deep dissection revealing the tibial nerve and posterior tibial vessels coursing deep to the soleus muscle.
Soleus Delamination and En Bloc Resection
- Defining the Margin: The tumor is palpated (if possible) through the soleus muscle. A margin of healthy soleus muscle is planned around the tumor. If the tumor is large, the entire soleus muscle may require resection (total soleusectomy).
- Release of Origins:
- The soleal arch is carefully incised. This is a critical step, as the tibial nerve and popliteal vessels lie immediately deep to this fibrous band.
- The fibular and tibial origins of the soleus are sharply released from the bone using electrocautery or a periosteal elevator, maintaining a cuff of normal tissue if the tumor is proximal.
- Ligation of Perforators: As the soleus is elevated from proximal to distal, numerous vascular perforators from the posterior tibial and fibular arteries will be encountered entering the deep surface of the muscle. These must be systematically identified, ligated (using ties, clips, or advanced bipolar devices), and divided.
- Distal Transection: Distally, the soleus muscle fibers transition into the deep aspect of the Achilles tendon. The soleus contribution to the tendon is transected, carefully preserving the superficial gastrocnemius contribution to maintain Achilles continuity.
- En Bloc Removal: The specimen is removed en bloc. The tumor bed is inspected for hemostasis. The specimen should be oriented with sutures or clips for the pathologist to facilitate accurate margin assessment.

Figure: Schematic representation of the en bloc soleus resection, emphasizing the preservation of the gastrocnemius and the deep neurovascular bundle.
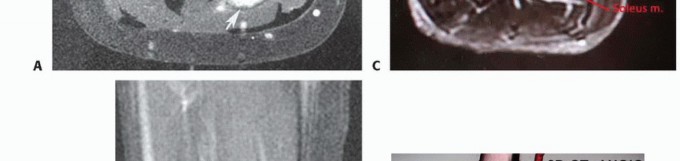
Figure: Intraoperative view demonstrating the elevation of the gastrocnemius heads to access the deep anatomical plane of the soleus.

Figure: Close-up of the soleus muscle dissection, highlighting the distinct fascicular anatomy and the required oncologic margins.
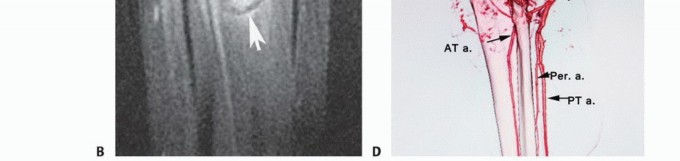
Figure: Dissection along the deep surface of the soleus, a critical zone given its immediate proximity to the deep neurovascular bundle.
Protecting the Heads of the Gastrocnemius
The success of the functional preservation relies on the integrity of the gastrocnemius.
* Fascial Boundary: The deep fascia of the gastrocnemius serves as the superficial surgical margin. It must remain intact unless tumor adherence dictates its excision.
* Thermal Control: The use of monopolar electrocautery on the deep surface of the gastrocnemius should be minimized to prevent thermal necrosis of the muscle fibers.
* Pedicle Protection: Continuous visual confirmation of the sural arteries and the proximal tibial nerve branches to the gastrocnemius is mandatory during the retraction and delamination phases.

Figure: The surgical bed following soleus resection. The gastrocnemius heads remain viable and intact, ready to be repositioned over the defect.
Reconstruction and Closure
- Dead Space Management: Resection of the soleus creates a massive potential dead space, highly prone to hematoma and seroma formation, particularly in irradiated tissue.
- Hemostasis: Meticulous hemostasis is achieved. The tourniquet is deflated prior to closure to identify and address any occult bleeding from muscular branches or perforators.
- Local vs. Free Tissue Transfer:
- In many cases, the preserved gastrocnemius heads can be approximated in the midline to partially obliterate the dead space.
- If the overlying skin and subcutaneous tissue are compromised (e.g., due to prior biopsy, tumor involvement, or severe radiation changes), a soft tissue reconstruction is required. Options include a pedicled gastrocnemius flap (sacrificing some functional preservation for coverage) or a free tissue transfer (e.g., Anterolateral Thigh [ALT] or Latissimus Dorsi flap).
- Drains: Multiple large-bore closed-suction drains are placed deep in the resection bed and brought out through separate stab incisions.
- Closure: The deep fascia is typically left open or only loosely approximated to prevent postoperative compartment syndrome. The subcutaneous tissue and skin are closed in a layered, tension-free manner.

Figure: The extensive surgical defect post-resection, illustrating the significant dead space that must be managed with drains and careful layered closure.
Complications and Management
Major limb-salvage surgery in the posterior compartment carries a significant complication profile. Preoperative radiotherapy, while oncologically beneficial, markedly increases the risk of wound complications.
Common Complications and Salvage Strategies
| Complication | Incidence | Pathophysiology & Presentation | Management and Salvage Strategies |
|---|---|---|---|
| Wound Dehiscence / Necrosis | 15-30% (Higher with RT) | Ischemia of skin flaps, exacerbated by radiation endarteritis and tension. Presents as marginal necrosis or frank dehiscence. | Conservative: NPWT (Wound VAC) for small defects. Surgical: Serial debridement. Rotational or free flap coverage if vital structures (nerve/vessels) are exposed. |
| Seroma / Hematoma | 10-25% | Accumulation of fluid in the massive dead space. Presents as swelling, pain, or prolonged drain output. | Prevention: Meticulous hemostasis, prolonged drain use. Management: Aspiration (sterile technique), compression. Surgical evacuation if causing skin tension or suspected infection. |
| Deep Surgical Site Infection (SSI) | 5-15% | Bacterial seeding of the dead space or hematoma. Presents with erythema, fever, purulent drainage. | Management: Urgent surgical irrigation and debridement (I&D). Deep tissue cultures. Broad-spectrum IV antibiotics transitioning to culture-directed therapy. |
| Nerve Injury (Tibial / Sural) | 5-10% | Tibial: Traction neuropraxia during retraction. Presents as plantarflexion weakness and plantar sensory loss. Sural: Often intentionally sacrificed for margins. Presents as lateral foot numbness. |
Tibial: Expectant management for neuropraxia (EMG at 6 weeks if no recovery). AFO for foot drop. Sural: Reassurance. Excision of painful neuromas if they develop. |
| Vascular Injury | <2% | Iatrogenic injury to popliteal or tibial vessels during deep |
Clinical & Radiographic Imaging

You Might Also Like