Resection of Calcaneonavicular Coalition: An Intraoperative Masterclass for Rigid Flatfoot

Key Takeaway
Master calcaneonavicular coalition resection with this intraoperative guide. We cover essential anatomy, patient positioning, meticulous incision, and precise bone resection. Learn critical techniques for interposition grafting using fat or local muscle, ensuring optimal subtalar motion restoration. Understand postoperative protocols and complication management for successful patient outcomes. This detailed masterclass prepares you for every surgical nuance.
Comprehensive Introduction and Patho-Epidemiology
A calcaneonavicular coalition represents a complex, congenital embryological failure of mesenchymal segmentation, resulting in an abnormal connection between the anterior process of the calcaneus and the lateral aspect of the navicular bone. This pathological bridging profoundly disrupts the normal kinematics of the peritalar complex. While these coalitions are present from birth, they characteristically remain asymptomatic during early childhood. The clinical manifestation of this anomaly typically coincides with the physiological ossification of the midfoot, most frequently emerging between the ages of 8 and 12 years. As the initial fibrous (syndesmosis) or cartilaginous (synchondrosis) bridge progressively ossifies into a rigid bony synostosis, the mechanical compliance of the hindfoot is drastically reduced, leading to the hallmark presentation of a painful, rigid flatfoot.
The true incidence of tarsal coalitions in the general population is estimated to be between 1% and 13%, with calcaneonavicular and talocalcaneal coalitions constituting the vast majority (approximately 90%) of these anomalies. Calcaneonavicular coalitions are slightly more prevalent than their talocalcaneal counterparts and are bilateral in up to 60% of cases. The genetic transmission is widely considered to be autosomal dominant with variable penetrance, necessitating a thorough family history during the initial clinical evaluation.
The pathophysiology of pain in a calcaneonavicular coalition is multifactorial. In the pre-ossification stages, micro-motion across the syndesmosis or synchondrosis during weight-bearing activities generates localized inflammatory responses and mechanical pain. As the coalition rigidifies, the subtalar joint—which functions biomechanically as a complex, multi-axial mitered hinge—becomes effectively locked. This loss of subtalar inversion and eversion forces the adjacent articulations, particularly the talonavicular and calcaneocuboid joints (Chopart's joint), to absorb abnormal, unphysiological torsional stresses. Consequently, patients develop adaptive muscular guarding, historically and somewhat inaccurately termed "peroneal spastic flatfoot," which is essentially an adaptive shortening of the peroneal musculature in response to chronic hindfoot valgus and pain.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the intricate osteology, ligamentous restraints, and neurovascular arborization of the midfoot and hindfoot is absolutely paramount. The surgical resection of a calcaneonavicular coalition is an exercise in precise anatomical navigation; straying even millimeters from the intended resection plane can result in catastrophic iatrogenic injury to adjacent vital structures.
Osteology and Articular Boundaries
The boundaries of the calcaneonavicular coalition dictate the limits of our surgical resection. The posterior margin of the coalition is formed by the anterior process of the calcaneus, while the anterior margin is defined by the lateral, non-articular aspect of the navicular.
Crucially, the surgeon must maintain acute spatial awareness of the talar head, which lies immediately medial and slightly proximal to the coalition. The articular cartilage of the talonavicular joint represents a "danger zone" during the medial-most aspect of the resection. Penetration into this joint space guarantees premature osteoarthritis. Plantarly and laterally, the medial edge of the cuboid serves as a critical anatomical landmark. A complete resection is achieved when the medial border of the resected anterior calcaneal process aligns flush with the medial border of the cuboid. The sinus tarsi, a conical, fat-filled cavity situated between the neck of the talus and the anterosuperior aspect of the calcaneus, serves as the primary surgical corridor to access the pathology.
Muscular and Ligamentous Intervals
The surgical approach exploits the internervous and intermuscular plane along the lateral aspect of the foot. The primary superficial interval lies between the extensor tendon group (extensor digitorum longus) dorsally and the peroneal tendon complex (peroneus longus and brevis) inferiorly.
Deep to the investing fascia, the extensor digitorum brevis (EDB) muscle is the most critical soft-tissue landmark. The EDB originates directly from the superolateral surface of the anterior calcaneus, intimately associated with the lateral opening of the sinus tarsi. To adequately expose the coalition, the EDB must be meticulously elevated from its origin and reflected distally. The bifurcate ligament, a Y-shaped structure connecting the anterior calcaneus to both the cuboid and the navicular, is invariably involved in the coalition mass and must be resected along with the abnormal bone to ensure adequate mobilization of the Chopart joint.
Neurovascular Considerations
The dorsolateral aspect of the foot is heavily populated with terminal sensory branches that are highly susceptible to iatrogenic injury. The superficial peroneal nerve (SPN), specifically its intermediate dorsal cutaneous branch, frequently traverses the planned oblique incision site. Careful blunt dissection in the subcutaneous layer is mandatory to identify, mobilize, and protect these branches. Injury to the SPN can result in a debilitating postoperative neuroma, which often eclipses the pain of the original coalition.
Deep within the operative field, the dorsalis pedis artery and the deep peroneal nerve lie medial to the resection zone, safely protected by the talar head and neck, provided the surgeon does not violate the medial boundaries of the dissection. The sural nerve courses along the lateral border of the foot, typically remaining inferior and posterior to the primary incision, though anatomical variants require the surgeon to remain vigilant during the inferior retraction of the peroneal tendons.
Exhaustive Indications and Contraindications
The decision to proceed with surgical resection of a calcaneonavicular coalition must be predicated on a rigorous clinical and radiographic evaluation. Not all radiographically identified coalitions require surgical intervention; asymptomatic coalitions discovered incidentally should be managed with benign neglect.
Surgical intervention is indicated primarily for patients exhibiting a symptomatic, rigid flatfoot that has proven recalcitrant to a comprehensive trial of conservative management. Conservative modalities typically include a minimum of 3 to 6 months of activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), custom medial longitudinal arch supports, UCBL orthoses, or a period of immobilization in a short-leg walking cast or controlled ankle motion (CAM) boot.
The surgical decision-making process is further nuanced by the size of the coalition and the presence of secondary degenerative changes. A simple resection is generally highly successful in adolescents without established arthritis. However, in older patients or those with massive coalitions (involving >50% of the talonavicular joint space) or severe, uncorrectable hindfoot valgus, a simple resection may fail to relieve pain and could exacerbate instability, necessitating primary arthrodesis.
| Parameter | Indications for Resection | Contraindications for Resection |
|---|---|---|
| Clinical Status | Symptomatic pain localized to sinus tarsi/lateral foot; failure of 3-6 months non-operative care. | Asymptomatic coalition; active local or systemic infection. |
| Age Group | Typically 8-14 years (prior to skeletal maturity and secondary joint adaptation). | Advanced age with established, rigid biomechanical adaptations. |
| Joint Health | Absence of degenerative joint disease in the subtalar or talonavicular joints. | Radiographic or MRI evidence of advanced osteoarthritis in adjacent joints. |
| Coalition Size | Small to moderate size (< 50% of the navicular articular face). | Massive coalition (> 50% involvement); concurrent talocalcaneal coalition. |
| Foot Alignment | Mild to moderate planovalgus that is passively correctable. | Severe, rigid planovalgus deformity requiring structural realignment (osteotomy/fusion). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful resection. The surgeon must construct a comprehensive three-dimensional mental model of the patient's specific anatomy before the first incision is made.
Advanced Imaging Review
Standard weight-bearing plain radiographs of the foot (anteroposterior, lateral, and oblique) are the initial diagnostic modality. The lateral radiograph frequently demonstrates the pathognomonic "anteater nose" sign—an abnormal, elongated anterior process of the calcaneus projecting toward the navicular.

FIG 1 • Lateral radiograph demonstrating the classic "anteater nose" sign, indicative of an elongated anterior calcaneal process.
The 45-degree internal rotation oblique view is the definitive plain radiographic projection for visualizing the calcaneonavicular interval, clearly delineating the bony, cartilaginous, or fibrous bridging.
FIG 2 • Oblique radiograph clearly depicting a cartilaginous calcaneonavicular coalition.
While radiographs are diagnostic, a non-contrast Computed Tomography (CT) scan is considered the gold standard for preoperative surgical templating. Fine-cut (1mm) axial, coronal, and sagittal reconstructions allow the surgeon to precisely quantify the cross-sectional area of the coalition, assess the exact proximity of the talar head, and definitively rule out concomitant coalitions (e.g., middle facet talocalcaneal coalitions), which occur in up to 20% of cases. Magnetic Resonance Imaging (MRI) is generally reserved for cases where the diagnosis remains ambiguous or to assess for active marrow edema, which signifies micro-trabecular stress fractures and confirms the coalition as the primary pain generator.
Patient Positioning and Operating Room Setup
The patient is positioned supine on a radiolucent operating table to facilitate unhindered intraoperative fluoroscopy. A substantial gel bump or folded blanket is placed beneath the ipsilateral hemipelvis. This maneuver internally rotates the lower extremity, bringing the lateral aspect of the foot parallel to the floor, thereby optimizing the surgical trajectory.
A sterile pneumatic tourniquet is highly recommended to ensure a bloodless surgical field, which is critical for identifying delicate neurovascular structures and ensuring complete resection of the coalition. If an autologous free fat graft is planned for interposition, the tourniquet must be placed high on the proximal thigh, and the entire limb from the toes to the gluteal fold must be meticulously prepped and draped. This allows sterile access to the gluteal crease or lateral thigh for fat harvesting. If the EDB muscle belly alone will be utilized for interposition, a calf tourniquet is sufficient.
Prior to inflation of the tourniquet, an Examination Under Anesthesia (EUA) is performed. The surgeon meticulously documents the baseline restriction in subtalar inversion and eversion. This baseline is critical; a successful resection should yield an immediate, palpable restoration of subtalar kinematics on the operating table.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution demands a systematic, layered approach, prioritizing the protection of adjacent soft tissues while aggressively addressing the osseous pathology.
Incision and Superficial Dissection
Following exsanguination and tourniquet inflation to 250 mmHg, an oblique incision measuring approximately 5 to 7 centimeters is mapped over the lateral midfoot. The incision is centered directly over the palpable mass of the anterior calcaneal process, coursing from the anterolateral aspect of the calcaneus distally towards the base of the third metatarsal. This trajectory perfectly bisects the interval between the extensor tendons dorsally and the peroneal tendons inferiorly.
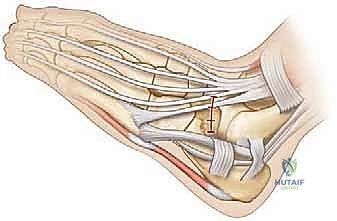
TECH FIG 1 • A. The planned oblique incision lies precisely within the internervous plane between the extensor and peroneal tendon complexes.
The skin is incised sharply with a #15 blade. Subcutaneous dissection must be performed with extreme caution using blunt Metzenbaum scissors. The intermediate dorsal cutaneous branch of the superficial peroneal nerve frequently crosses this field. Once identified, the nerve branches are gently mobilized and retracted dorsally using vessel loops. The inferior skin flap is minimally undermined to expose the superior peroneal retinaculum, ensuring the peroneal tendons remain undisturbed in their sheath.
Deep Dissection and EDB Reflection
Deep to the subcutaneous fat, the investing fascia of the foot is encountered. The fascia overlying the extensor digitorum brevis (EDB) is incised longitudinally. The EDB muscle belly is a critical anatomical guide. Using a combination of sharp dissection and a periosteal elevator, the origin of the EDB is meticulously detached from the lateral aspect of the calcaneus and the lateral opening of the sinus tarsi.

TECH FIG 1 • B,C. The extensor digitorum brevis (EDB) is carefully identified, elevated from its origin, and reflected distally to expose the underlying coalition.
The muscle is reflected distally and held with a self-retaining retractor (e.g., a Gelpi or Weitlaner). This maneuver unroofs the sinus tarsi and brings the calcaneonavicular coalition into direct view. The fibrofatty plug within the sinus tarsi (the Hoke tonsil) is excised using electrocautery and rongeurs to maximize visibility.
Coalition Localization and Fluoroscopic Confirmation
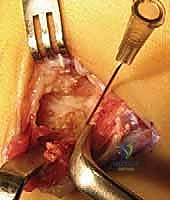
With the osseous structures exposed, the surgeon must definitively map the borders of the coalition. The abnormal bridging tissue—whether fibrous, cartilaginous, or bony—will be visually distinct from normal articular anatomy. A Freer elevator or a smooth Kirschner wire (K-wire) is placed directly across the center of the suspected coalition mass.

TECH FIG 1 • D. Initial localization of the calcaneonavicular coalition using a metallic probe.

TECH FIG 1 • E. Further delineation of the coalition's borders prior to radiographic confirmation.
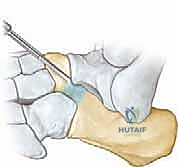
Intraoperative fluoroscopy is then deployed. An oblique (internal rotation) view is obtained to confirm that the K-wire or instrument is perfectly centered on the coalition. This step prevents the catastrophic error of inadvertently resecting the normal calcaneocuboid joint or violating the talonavicular joint.
TECH FIG 1 • F. Fluoroscopic confirmation of the targeted coalition, ensuring accurate anatomical orientation before bone resection begins.
Radical Resection Technique
The goal of the resection is not merely to break the bridge, but to create a massive, rectangular void that physically prevents postoperative re-ossification. A minimum gap of 1.0 to 1.5 centimeters must be achieved.
The resection is initiated using a combination of sharp, straight osteotomes and a surgical mallet. The initial cuts outline the planned rectangular block.
TECH FIG 2 • A. Initial osteotomy cuts are made to define the anterior and posterior boundaries of the resection.

TECH FIG 2 • B. Progressive removal of the osseous bridge using osteotomes and rongeurs.
As the block is mobilized, Kerrison rongeurs and double-action Leksell rongeurs are utilized to meticulously bite away the remaining bone. The surgeon must exercise extreme caution as the resection proceeds medially. The head of the talus is immediately adjacent to the medial border of the coalition. A small Freer elevator can be placed medially to act as a physical barrier, protecting the talar articular cartilage from the jaws of the rongeur.

TECH FIG 2 • C. The gap is progressively widened. The medial aspect of the resection requires meticulous care to avoid the talar head.
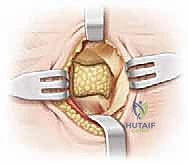
The plantar-medial limit of the resection is dictated by the cuboid. The resection is considered complete only when the medial border of the calcaneus is perfectly flush with the medial border of the cuboid. A high-speed burr can be used to smooth the bony margins and ensure no overhanging osteophytes remain.

TECH FIG 2 • D. Final visualization of the massive, rectangular resection gap. A minimum 1.5 cm void is required to prevent recurrence.
Once the resection is complete, the surgeon must manually manipulate the hindfoot. A dramatic, immediate restoration of subtalar inversion and eversion should be palpable. If restriction persists, the surgeon must re-evaluate the resection margins for residual coalition or consider the presence of an undiagnosed secondary talocalcaneal coalition.
Interposition Grafting and Closure
To prevent the postoperative hematoma from acting as a scaffold for recurrent ossification, the massive dead space created by the resection must be filled with an interposition material.
The two most common autologous options are the EDB muscle belly or a free fat graft. If utilizing the EDB, the previously reflected muscle belly is mobilized, drawn deeply into the resection void, and secured using heavy absorbable sutures (e.g., 0-Vicryl) passed through drill holes in the plantar aspect of the calcaneus or navicular, or secured using suture anchors.
TECH FIG 3 • A. Interposition of the Extensor Digitorum Brevis (EDB) muscle belly into the resection void, secured with sutures to prevent dead space hematoma.
Alternatively, a free fat graft harvested from the gluteal crease provides excellent anti-osteogenic properties and avoids the potential morbidity of EDB transposition. Bone wax is historically mentioned but is generally discouraged in modern practice due to the risk of foreign body reaction and chronic inflammation.

TECH FIG 3 • B. Final closure over the interposition graft. Meticulous hemostasis and layered closure are paramount.
The tourniquet is deflated prior to closure to ensure meticulous hemostasis, thereby minimizing hematoma formation. The subcutaneous tissue is closed with interrupted absorbable sutures, and the skin is reapproximated with a running subcuticular suture or nylon mattress sutures. A bulky, sterile compressive dressing and a well-padded short-leg splint in neutral alignment are applied.
Complications, Incidence Rates, and Salvage Management
While resection of a calcaneonavicular coalition is generally highly successful, the surgeon must be acutely aware of potential complications and possess the technical repertoire to manage them. The most common cause of failure is inadequate initial resection leading to recurrence.
Recurrence of the coalition, often due to ossification of the postoperative hematoma, occurs in approximately 10% to 15% of cases. This underscores the absolute necessity of creating a massive (≥1.5 cm) gap and utilizing a robust interposition graft. If recurrence occurs and the patient is highly symptomatic, revision resection can be attempted, though primary triple arthrodesis or talonavicular-calcaneocuboid (Chopart) arthrodesis is often the most reliable salvage procedure.
Iatrogenic injury to the superficial peroneal nerve occurs in up to 5% of cases, leading to painful neuromas. Management begins with gabapentinoids and targeted nerve blocks; however, recalcitrant neuromas may require surgical excision and burying of the proximal nerve stump into deep muscle tissue.
| Complication | Incidence | Etiology / Risk Factors | Salvage Management |
|---|---|---|---|
| Recurrent Coalition | 10% - 15% | Inadequate resection (< 1 cm gap); failure of interposition graft; hematoma ossification. | Revision wide resection with fresh fat graft; Arthrodesis if degenerative changes are present. |
| SPN Neuroma | 2% - 5% | Iatrogenic traction or sharp transection during superficial dissection. | Conservative (medications, blocks); Surgical excision and proximal burying. |
| Talar Head AVN / Injury | < 2% | Aggressive medial resection violating the talonavicular joint capsule and articular cartilage. | Protected weight-bearing; Talonavicular arthrodesis if progressive collapse/arthritis occurs. |
| Progressive Flatfoot | 5% - 10% | Unmasking of underlying severe ligamentous laxity post-resection. | Orthotics; Medial displacement calcaneal osteotomy (MDCO); Lateral column lengthening. |
| Wound Dehiscence | 1% - 3% | Excessive retraction; aggressive undermining of skin flaps; smoking. | Local wound care; oral antibiotics; rarely requires surgical debridement. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must balance the need for early mobilization to prevent scar tissue ossification with the necessity of protecting the healing soft tissues and interposition graft.
Phase 1: Immediate Post-Operative (Weeks 0-2)
The patient is placed in a well-padded, non-weight-bearing short-leg splint immediately post-surgery. Strict elevation above the level of the heart is mandatory to mitigate edema and minimize the risk of wound dehiscence. At the two-week mark, the patient returns to the clinic for suture removal and wound inspection.
Phase 2: Early Mobilization (Weeks 2-6)
Following suture removal, the splint is transitioned to a removable Controlled Ankle Motion (CAM) boot. Crucially, the patient is instructed to remove the boot multiple times daily to perform aggressive, active, and active-assisted subtalar and ankle Range of Motion (ROM) exercises. These exercises—specifically focusing on inversion, eversion, and circumduction—are the primary defense against recurrent stiffness and hematoma ossification. The patient remains non-weight-bearing or touch-down weight-bearing during this phase.
Phase 3: Progressive Weight-Bearing and Strengthening (Weeks 6-12)
At six weeks post-operation, repeat radiographs are obtained to ensure no early recurrence of ossification. The patient is then transitioned to progressive weight-bearing
