Masterclass: ORIF of Capitellum and Capitellar–Trochlear Shear Fractures
Key Takeaway
Welcome, fellows, to an immersive intraoperative masterclass on open reduction and internal fixation (ORIF) of capitellum and capitellar–trochlear shear fractures. We'll navigate complex elbow anatomy, meticulous surgical techniques, and critical decision-making. From precise patient positioning to advanced fixation strategies, this session will equip you with the expertise to achieve optimal outcomes for these challenging distal humerus injuries.
Introduction to Capitellar and Capitellar–Trochlear Shear Fractures
Welcome to the operating theater, fellows. Today, we're tackling a fascinating and often challenging injury: fractures of the capitellum and the more complex capitellar–trochlear shear fractures. While uncommon, accounting for less than 1% of all elbow fractures and roughly 6% of distal humerus fractures, their management is critical for restoring elbow function. These injuries frequently present in conjunction with radial head fractures and posterior elbow dislocations, demanding a comprehensive diagnostic and treatment approach.
Surgical Anatomy: A Deeper Dive
Let's begin by reviewing the intricate anatomy of the distal humerus, which is paramount to our surgical success. The distal humerus flares into two condyles, forming the lateral and medial columns that support the central trochlea.
- The Capitellum: This is the anterior aspect of the lateral column, entirely covered by articular cartilage anteriorly, but notably devoid of it posteriorly. It is directed distally and anteriorly at an angle of approximately 30 degrees relative to the long axis of the humerus. The radial head articulates with the anterior surface of the capitellum during elbow flexion and with its inferior surface in extension. Remember, the capitellum is the first epiphyseal center of the elbow to ossify.
- Neurovascular Considerations:
- Blood Supply: The capitellum's blood supply is derived predominantly posteriorly, originating from the lateral arcade—an anastomosis between the radial collateral arteries of the profunda brachii and the radial recurrent artery. This posterior supply is a critical consideration, as extensive posterior dissection or disruption can compromise vascularity and increase the risk of osteonecrosis.
- Nerves:
- Radial Nerve: Proximally, it travels between the brachialis and brachioradialis muscles. Meticulous dissection is required to protect it, especially during proximal extension of our lateral approach.
- Posterior Interosseous Nerve (PIN): This motor branch of the radial nerve is vulnerable distally, particularly when reflecting the common extensor origin or developing the interval between the anconeus and the extensor carpi ulnaris (ECU). Keeping the forearm pronated can help shift the PIN anteriorly and medially, offering some protection.
- Ulnar Nerve: Located in the cubital tunnel behind the medial epicondyle, it requires careful identification and protection, especially with posterior approaches or when dealing with medial column involvement. In some cases, in situ decompression may be necessary to prevent iatrogenic injury.
- Ligamentous Attachments: The lateral collateral ligament (LCL) inserts adjacent to the lateral margin of the capitellum. Avulsion of this complex is common with these fractures and must be addressed during closure.
- Muscular Intervals:
- Köcher Approach: This utilizes the interval between the anconeus posteriorly and the extensor carpi ulnaris (ECU) anteriorly. This interval is favored for its relative safety regarding the posterior interosseous nerve.
- Common Extensor Origin: Comprising the ECU, extensor digitorum communis (EDC), and extensor carpi radialis longus (ECRL), this origin can be sharply elevated off the lateral epicondyle and reflected anteriorly to enhance exposure.
Classification Systems
Understanding the fracture pattern is paramount. We primarily use two systems:
- Bryan and Morrey (Modified by McKee):
- Type 1: Complete fractures of the capitellum. These typically involve a significant subchondral bone component.
- Type 2: Superficial subchondral fractures of the capitellar articular surface. These are often smaller, thinner articular fragments.
- Type 3: Comminuted fractures, displaying variable amounts of fragmentation.
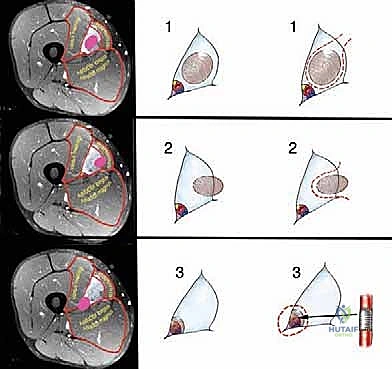
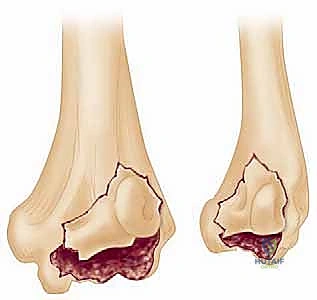
- Type 4: Coronal shear fractures that include a portion of the trochlea as well as the capitellum as one piece. These are inherently more unstable and complex.
FIG 1 • Type 4 coronal shear fractures of the distal humerus.
- Ring and Jupiter: This classification expands on the understanding that isolated capitellum fractures are rare, often involving five anatomic components:
- The capitellum and lateral aspect of the trochlea
- The lateral epicondyle
- The posterior aspect of the lateral column
- The posterior aspect of the trochlea
- The medial epicondyle
Pathogenesis and Natural History
These fractures typically result from a fall on an outstretched hand or forearm, where the radial head impacts the capitellum. In capitellar–trochlear shear fractures, this impaction occurs in a semi-extended position, leading to a shearing mechanism of the distal humerus. The fracture fragments commonly displace proximally and anteriorly into the radial fossa, causing impingement with elbow flexion.
Capitellar fractures are almost exclusively seen in adults, particularly females due to a higher carrying angle. Elderly patients are also more susceptible due to osteoporosis. Untreated displaced fractures lead to progressive loss of motion, pain, crepitus, and post-traumatic arthrosis, underscoring the necessity of operative intervention for most patterns.
Differential Diagnosis
When evaluating a patient with suspected capitellar fracture, always consider:
* Radial head fracture
* Distal humeral lateral condyle fracture
* Elbow dislocation
Nonoperative Management: A Cautious Approach
Nonoperative management is rarely indicated. Only truly nondisplaced and isolated capitellum fractures, typically Type 1, might be managed with 3 weeks of splinting followed by protected motion. However, this requires absolute confirmation of stability and anatomic alignment. We do not advocate nonoperative management for any other type of capitellum fracture, especially capitellar–trochlear shear fractures, due to their inherent instability and articular incongruity. Closed reduction techniques, while described, must achieve complete anatomic reduction; anything less is unacceptable and warrants ORIF.
Preoperative Planning: The Blueprint for Success
Before we make any incision, a meticulous preoperative plan is essential.
Imaging and Diagnostic Studies
Standard radiographs are often insufficient.
* Lateral Radiographs: Best for initial evaluation and can reveal the characteristic "double arc" sign in coronal shear fractures.

FIG 2 • A. Characteristic “double arc” sign on lateral radiographs of coronal shear fractures.
* Anteroposterior (AP) Views: Not reliably diagnostic as the distal humerus outline may not be consistently affected.
* Radial Head–Capitellum View: A lateral oblique projection (x-ray beam 45 degrees dorsoventrally) that eliminates ulno- and radiohumeral articulation shadows, helping to identify capitellum fractures.
* Computed Tomography (CT) Scans: Absolutely necessary in all cases. Perform at 1- to 2-mm intervals with axial or transverse cuts to delineate the fracture pattern, comminution, and displacement.
* Three-Dimensional (3D) CT Reconstructions: If available, these provide the best detail and ability to appreciate the anatomic orientation of complex fracture patterns, allowing for superior surgical planning.

FIG 2 • B,C. 3D CT reconstructions of a coronal shear fracture of the distal humerus.
Surgical Timing and Logistics
- Timing: Ideally, surgery should be performed within 2 weeks of injury, after acute swelling has subsided but before significant osseous healing complicates reduction.
- Implants and Hardware: Ensure all necessary implants are readily available:
- 0.045-inch K-wires for provisional fixation.
- Headless compression screws (e.g., Herbert screws) in various lengths.
- Small-fragment AO cancellous screws.
- Reduction tenaculums, small fragment sets, and specialized elbow trays.
- Image Intensifier (Fluoroscopy): Essential for intraoperative confirmation of reduction and hardware placement. Our C-arm should be draped and ready.
Patient Positioning and Anesthesia
General anesthesia is recommended for optimal muscle relaxation and patient comfort.
- Standard Position: The patient is typically positioned supine on the operating table, with a radiolucent hand table to support the arm. This allows for easy access to the lateral elbow and facilitates fluoroscopy.
- Alternative Positions: For more complex capitellar–trochlear shear fractures, particularly those requiring extensile exposure or olecranon osteotomy, a lateral or prone position may be considered. If prone, the anterior surface of the elbow must be supported by a padded bolster to allow for a universal posterior approach.
Intraoperative Masterclass: Capitellar Fractures (Type 1, 2, 3)
Alright, fellows, let's scrub in. We'll start with the approach for isolated capitellar fractures.
Exposure: The Lateral Approach
- Incision Planning: We'll begin by marking our incision. It should start approximately 2 cm proximal to the lateral epicondyle and extend 3 to 4 cm distally, aiming towards the radial neck. This provides ample working space.
- Skin and Subcutaneous Dissection: Make a meticulous skin incision down to the subcutaneous tissue. Use electrocautery for hemostasis, ensuring a bloodless field.
- Identifying the Interval:
- Pre-existing Capsular Violation: In many cases, the injury itself creates a capsular violation. This is a gift, as we can exploit this defect to directly access the fracture, minimizing further iatrogenic soft tissue damage.
- Köcher Approach (Anconeus-ECU Interval): If no significant capsular defect is present, we will utilize the direct lateral Köcher approach. Carefully identify the interval between the anconeus muscle posteriorly and the extensor carpi ulnaris (ECU) anteriorly. This interval offers excellent exposure while protecting the posterior interosseous nerve (PIN).
- Raising the Common Extensor Origin: To further enhance visualization, particularly when the fracture extends more broadly or requires anterior access, we will sharply raise the common extensor origin (ECU, extensor digitorum communis, and extensor carpi radialis longus) off the lateral epicondyle. Reflect this muscle mass anteriorly.
> Surgical Warning: As we raise the common extensor origin, be acutely aware of the radial nerve proximally, traveling between the brachialis and brachioradialis. Distally, the posterior interosseous nerve is at risk when reflecting the ECU anteriorly. Keep the forearm pronated to help move the PIN away from our dissection plane. - Lateral Ligamentous Complex: Often, the lateral ligamentous complex (LCL, annular ligament, LUCL) will be avulsed from the distal humerus, sometimes with a piece of the lateral epicondyle. This traumatic disruption can be advantageous, allowing us to hinge open the joint on the intact medial collateral ligament (MCL) with a gentle varus stress, significantly improving exposure of the articular surface.
Reduction and Fixation: Precision is Key
Now, for the critical step of reduction and stabilization. The capitellar fracture fragment is typically displaced proximally and rotated, often with no soft tissue attachments, making it mobile but challenging to control.
- Fragment Visualization and Debridement: Carefully visualize the fracture fragment(s). Irrigate the joint to remove any hematoma, small bone chips, or soft tissue interposition that might impede reduction.
- Reduction Maneuver: Use a small dental pick or a fine-tipped Freer elevator to gently manipulate the fragment. Reduce it under direct visualization, ensuring perfect anatomical alignment with the remaining articular surface of the distal humerus.
- Provisional Fixation: Once reduced, hold the fragment securely with small reduction tenaculums. Then, insert one or two 0.045-inch K-wires from an anterior-to-posterior direction. These K-wires provide temporary stability, preventing displacement while we prepare for definitive fixation.
-
Definitive Internal Fixation: Our choice of hardware depends on the fracture type and the amount of subchondral bone present.
- Headless Compression Screws (e.g., Herbert screws): These are ideal for fragments with less subchondral bone, such as Type 2 fractures and smaller Type 1 fragments. They offer excellent compression and can be inserted from either anterior-to-posterior or posterior-to-anterior.
- Technique: Drill a guide wire under fluoroscopic guidance, ensuring it is perfectly centered within the fragment and crosses the fracture line. Measure for screw length. Over-drill for the leading threads, then tap if necessary, and insert the headless screw.
Surgical Warning: When placing headless screws, especially from anterior-to-posterior, it is absolutely critical to ensure the head of the screw is buried completely below the articular cartilage surface. Palpate the articular surface with a probe and confirm with fluoroscopy to prevent impingement.

- Technique: Drill a guide wire under fluoroscopic guidance, ensuring it is perfectly centered within the fragment and crosses the fracture line. Measure for screw length. Over-drill for the leading threads, then tap if necessary, and insert the headless screw.
- Headless Compression Screws (e.g., Herbert screws): These are ideal for fragments with less subchondral bone, such as Type 2 fractures and smaller Type 1 fragments. They offer excellent compression and can be inserted from either anterior-to-posterior or posterior-to-anterior.


TECH FIG 1 • Fixation of a type 1 capitellum fracture with a headless screw anteriorly and AO screws from posterior to anterior.
* **AO Cancellous Screws:** These are best suited for Type 1 fracture fragments with a large subchondral component. They are typically placed from posterior-to-anterior.
* **Technique:** This requires extending the dissection posteriorly around the lateral column to create a purchase point. Drill, measure, tap, and insert the cancellous screw.
> **Surgical Warning:** Extending dissection posteriorly increases the theoretical risk of osteonecrosis due to the posterior blood supply of the capitellum. Weigh this risk carefully against the benefits of robust fixation for large fragments.
* **Type 2 and 3 Fractures:** For Type 2 fractures with small, thin articular pieces not amenable to stable fixation, or for highly comminuted Type 3 fractures where fragments are too small to fix, excision of the fracture fragments may be the only viable option. However, this is a salvage procedure and often results in some degree of functional limitation. Our primary goal is always ORIF.
- Intraoperative Assessment:
- Fluoroscopy: Perform multiple fluoroscopic views (AP, lateral, oblique) to confirm anatomic reduction and optimal hardware position. Ensure no screws are prominent in the joint.
- Range of Motion (ROM): Remove the K-wires. Gently flex and extend the elbow through its full range. Pronate and supinate the forearm. Confirm unrestricted motion without any mechanical block, crepitus, or catching. This is a critical step to ensure a good postoperative outcome.
Closure
- Ligamentous Repair: If the lateral collateral ligament (LCL) complex was avulsed, it must be repaired back to the lateral epicondyle. Use drill holes and nonabsorbable No. 2 suture or suture anchors for a robust repair.
- Capsule Closure: Close the joint capsule meticulously using absorbable suture.
- Muscle Reattachment: The retracted common extensor origin should be relaxed and reattached to the lateral epicondyle and surrounding soft tissue with absorbable sutures.
- Layered Closure: Close the subcutaneous tissue and skin in a standard fashion. Apply a sterile dressing.
Intraoperative Masterclass: Capitellar–Trochlear Shear Fractures (Type 4)
Now, let's move to the more complex capitellar–trochlear shear fractures, classified as Type 4. These often require a more extensile exposure.
Exposure: The Posterior Midline Approach
- Incision Planning: For these complex fractures, a posterior midline incision is our preferred choice. This extensile approach provides excellent visualization and access to both the lateral and medial columns, and it allows for potential osteotomies if needed.

TECH FIG 2 • A. Posterior midline incision used to for capitellar–trochlear shear fractures.
2. Full-Thickness Flaps: Raise full-thickness skin and subcutaneous flaps medially and laterally off the extensor mechanism.
3. Ulnar Nerve Decompression (Medially): Begin medially. Carefully identify and decompress the ulnar nerve in situ behind the medial epicondyle. This involves releasing the fascia of the cubital tunnel. We want to ensure it is free and protected throughout the case.

TECH FIG 2 • B. Ulnar nerve compression medially.
4. Lateral Exposure: Return to the lateral side.
* Exploiting Traumatic Osteotomy: In many cases, the lateral epicondyle will have avulsed from the distal humerus due to the injury. This traumatic osteotomy can be leveraged to improve exposure.
* Formal Lateral Epicondyle Osteotomy: If the lateral epicondyle is intact but visualization is insufficient, a formal lateral epicondyle osteotomy can be performed. This involves carefully cutting the epicondyle to hinge it anteriorly with the attached common extensor origin, preserving the integrity of the lateral ligamentous complex.
* Anconeus-ECU Interval: Develop the interval between the anconeus and the ECU. Again, a pre-existing capsular violation can be exploited to gain direct access to the joint.

TECH FIG 2 • C. Lateral approach to elbow taking advantage of violation of the capsule and extensor muscles at the level of the extensor carpi ulnaris (ECU) and anconeus.
5. Reflecting Common Extensor Origin: The common extensor origin (ECU, EDC, ECRL) is then sharply raised off the lateral epicondyle and reflected anteriorly. This significantly improves visualization, especially medially towards the trochlea.
> Surgical Warning: As with isolated capitellar fractures, maintain vigilance for the radial nerve proximally and the posterior interosseous nerve distally. Keep the forearm pronated during this reflection.
6. Olecranon Osteotomy (If Necessary): For extremely comminuted or extensively displaced fractures involving the medial and posterior aspects of the distal humerus, an olecranon osteotomy may be required. This provides unparalleled visualization of the entire distal humerus articular surface. If performed, plan for a tension band or plate fixation of the osteotomy at the end of the case.
7. Fragment Visualization: At this point, the fracture fragments, which are most commonly displaced proximally and internally rotated, should be clearly visualized and accounted for.

TECH FIG 2 • D. The fracture fragments tend to displace proximally and become internally rotated.
Reduction and Fixation: Reconstructing the Articular Surface
The goal here is meticulous anatomical reduction of the entire articular block.
- Fragment Disimpaction and Debridement: The fragments may be impacted. Use a small osteotome or elevator to gently disimpact them. Thoroughly irrigate and debride the joint of any hematoma or small osteochondral fragments.
- Reduction Maneuver: Using reduction tenaculums, carefully manipulate the large capitellar–trochlear fragment back into its anatomical position. This often involves a distal and external rotation maneuver.
> Surgical Warning: If you encounter inability to achieve anatomic reduction, suspect fracture impaction requiring more aggressive disimpaction, or a bone graft may be needed to fill a metaphyseal defect if there's significant bone loss. Do not accept malreduction. - Provisional Fixation: Once reduced, provisionally fix the fragment with 0.045-inch K-wires, typically from anterior-to-posterior. Ensure these K-wires are placed in non-articulating areas or in a path that will not interfere with definitive screw placement.

TECH FIG 3 • A. The fracture is reduced and pinned with 0.045-inch K-wires.
4. Definitive Internal Fixation:
* **Headless Compression Screws:** These are often preferred for capitellar–trochlear shear fractures due to their ability to be buried below the articular surface and provide strong compression. They can be inserted from either anterior-to-posterior or posterior-to-anterior, depending on the fragment morphology and surgical access.
* **Technique:** Under fluoroscopic guidance, drill a guide wire across the fracture line. Measure, over-drill, tap (if needed), and insert the headless screw. Confirm the screw head is subchondral.
* **AO Cancellous Screws:** If a large subchondral component exists, cancellous screws can be used, typically from posterior-to-anterior. However, remember the increased risk of osteonecrosis with extensive posterior dissection.
* **Plate and Screws:** For larger, more unstable fragments, or if the lateral column needs additional support, small fragment plates (e.g., 1/3 tubular plate or specially designed distal humerus plates) may be used in conjunction with screws to bridge defects or provide buttress support.
- Intraoperative Assessment:
- Fluoroscopy: Obtain multiple views (AP, lateral, obliques) to confirm perfect anatomical reduction and optimal hardware placement. Ensure no screw prominence.
- Range of Motion (ROM): Remove K-wires. Gently move the elbow through its full flexion-extension arc and pronation-supination. Confirm unrestricted motion without any mechanical block or catching. This is paramount for preventing postoperative stiffness.
Closure
- Lateral Epicondyle Repair: If a lateral epicondyle osteotomy was performed, or if it was avulsed, it must be repaired meticulously. A tension band technique or a small plate and screws can be used to achieve stable fixation.
- Olecranon Osteotomy Repair: If an olecranon osteotomy was performed, repair it with a tension band wiring technique or a small olecranon plate and screws.
- Capsule Closure: Close the joint capsule with absorbable sutures.
- Muscle Reattachment: Relax and reattach the common extensor origin to the lateral epicondyle. Close the interval and surrounding soft tissues.
- Ulnar Nerve Transposition (Optional): If the ulnar nerve was significantly mobilized or if there's concern for postoperative compression, consider anterior transposition.
- Layered Closure: Close the subcutaneous tissue and skin in a standard fashion. Apply a sterile dressing.

TECH FIG 3 • B. Postoperative radiographs illustrate repair of the lateral epicondyle and fracture fixation.
Postoperative Rehabilitation and Complication Management
Our work isn't done when the dressing is applied. Postoperative care is crucial for maximizing recovery.
Immediate Postoperative Period
- Immobilization: A well-padded posterior splint is typically applied in 90 degrees of flexion for comfort and protection for the first few days.
- Pain Management: Aggressive multimodal pain management is critical to facilitate early motion.
- DVT Prophylaxis: Standard DVT prophylaxis protocols should be initiated.
- Wound Care: Monitor the incision for signs of infection or dehiscence.
Rehabilitation Protocol
The goal is early, protected motion to prevent stiffness while protecting our fixation.
- Initiation of Motion:
- Within 3-5 days: Begin gentle, active-assisted range of motion (AAROM) exercises under the guidance of a physical therapist. We'll aim for a specific arc of motion (e.g., 30-100 degrees initially), gradually increasing as tolerated.
- Passive Range of Motion (PROM): Introduce gentle PROM as tolerated, ensuring no undue stress on the repair.
- Forearm Rotation: Active pronation and supination should be encouraged early.
- Weight-Bearing Status:
- Non-weight bearing: The affected arm should remain non-weight bearing for at least 6-8 weeks to allow for adequate bone healing.
- Gradual Strengthening: After 6-8 weeks, once radiographic signs of healing are present, progressive strengthening exercises can begin.
- Return to Activity: Full return to strenuous activities or sports typically takes 4-6 months, contingent on fracture healing, pain levels, and restoration of motion and strength.
Potential Complications and Management
💡 Pearls and Pitfalls
Imaging
* Plain radiographs are insufficient for accurate diagnosis and planning; a CT scan should be performed routinely in all cases.
* Order 3D reconstructions whenever possible; they provide invaluable insight into fracture morphology and aid in preoperative templating.Nonoperative Management
* Nonoperative management should be chosen extremely cautiously and only for truly nondisplaced, isolated capitellum fractures.
* Anatomic and stable reduction is absolutely necessary. Otherwise, a painful elbow with restricted motion and post-traumatic arthrosis is highly likely.
* **Never treat capitellar
REFERENCES
-
Alvarez E, Patel M, Nimberg P, et al. Fractures of the capitellum humeri. J Bone Joint Surg Am 1975;57A:1093–1096.
-
Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am 1986;68A:669–674.
-
Bryan RS, Morrey BF. Fractures of the distal humerus. In: Morrey BF, ed. The Elbow and Its Disorders. Philadelphia: WB Saunders, 1985:302–399.
-
Christopher F, Bushnell L. Conservative treatment of fractures of the capitellum. J Bone Joint Surg 1935;17:489–492.
-
Cobb TK, Morrey BF. Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79A:826–832.
-
Collert S. Surgical management of fracture of the capitulum humeri. Acta Orthop Scand 1977;48:603–606.
-
Dubberley JH, Faber KJ, Macdermid JC, et al. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 2006;88A:46–54.
-
Fowles JV, Kassab MT. Fracture of the capitulum humeri: treatment by excision. J Bone Joint Surg Am 1975;56A:794–798.
-
Garcia JA, Myulka R, Stanley D. Complex fractures of the distal humerus in the elderly: the role of total elbow replacement as primary treatment. J Bone Joint Surg Br 2002;84B:812–816.
-
Greenspan A, Norman A. The radial head, capitellum view: useful technique in elbow trauma. AJR Am J Roentgenol 1982;138: 1186–1188.
-
Hahn NF. Fall von einer besonderes Varietat der Frakturen des Ellenbogens. Z Wund Geburt 1853;6:185.
-
Jupiter JB, Neff U, Ragazzoni P, et al. Unicondylar fractures of the distal humerus: an operative approach. J Orthop Trauma 1988;2: 102–109.
-
Lansinger O, Mare K. Fracture of the capitulum humeri. Acta Orthop Scand 1981;52:39–44.
-
Liberman N, Katz T, Howard CV, et al. Fixation of capitellar fractures with Herbert screws. Arch Orthop Trauma Surg 1991;110: 155–157.
-
Mahirogullari M, Kiral A, Solakoglu C, et al. Treatment of fractures of the humeral capitellum using Herbert screws. J Hand Surg Eur Vol 2006;31:320–325.
-
Mazel MS. Fracture of the capitellum. J Bone Joint Surg 1935; 17:483–488.
-
McKee MD, Jupiter JB, Bosse G, et al. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996;78A:49–54.
-
Milch H. Fractures and fracture-dislocations of the humeral condyles. J Trauma 1964;13:882–886.
-
Ochner RS, Bloom H, Palumbo RC, et al. Closed reduction of coronal fractures of the capitellum. J Trauma 1996;40:199–203.
-
Richards RR, Khoury GW, Burke FD, et al. Internal fixation of capitellar fractures using Herbert screw: a report of four cases. Can J Surg 1987;30:188–191.
-
Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85A:232–238.
-
Steinthal D. Die isolirte Fraktur der eminentia Capetala in Ellengogelenk. Zentralk Chir 1898;15:17.
-
Yamaguchi K, Sweet FA, Bindra R, et al. The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79A:1653–1662.
-
More recently, Mahirogullari et al 15 reported on 11 cases of type 1 capitellum fractures treated with Herbert screws, which yielded 8 excellent and 3 good results. They recommended fixation in a posterior-to-anterior direction with at least two Herbert screws.
-
Reported outcomes on type 4 capitellar–trochlear shear fractures are limited. McKee et al 17 originally described this pattern and reported on 6 cases.
-
Each case involved an extended lateral Köcher approach and fixation with Herbert screws from an anterior to posterior direction. Good or excellent results were achieved in all cases, with average elbow motion of 15 to 141 degrees, and forearm rotation of 83 degrees pronation and 84 degrees supination.
-
Ring and Jupiter examined 21 cases of articular fractures of the distal humerus treated with Herbert screw fixation and found 4 excellent results, 12 good results, and 5 fair results.
-
All of the fractures healed and had an average range of motion of 96 degrees. No ulnohumeral instability, arthrosis, or osteonecrosis was reported.
-
The authors stressed the importance of proper evaluation of these fractures and awareness that apparent capitellum fractures often are complex articular fractures of the distal humerus. 21
-
Dubberley et al 7 further subclassified type 4 fractures in their series of 28 cases. They achieved an average range of motion of flexion–extension of 25 degrees less than the contralateral elbow and 4 degrees of supination–pronation less than the contralateral elbow.
-
Two comminuted cases required conversion to a total elbow arthroplasty.
-
Varied fixation methods were used, including Herbert screws, cancellous screws, absorbable pins, and supplementation with K-wires.
COMPLICATIONS
- The most common complication of capitellar fractures is loss of elbow motion and residual pain. The compromised motion most commonly is manifested in loss of flexion and extension.
-
Ulnar neuropathy has been noted after ORIF, and some recommend routine ulnar nerve decompression. 21
-
Osteonecrosis may occur from the initial fracture displacement or surgical exposure. Blood is supplied to the capitellum from a posterior to anterior direction and may be compromised by surgical dissection.
-
In symptomatic cases in which revascularization after fixation has not occurred, delayed excision is indicated.
You Might Also Like