Masterclass: Precision Syme and Boyd Amputations for Congenital Fibular Deficiency

Key Takeaway
This masterclass guides fellows through Syme and Boyd amputations for congenital fibular deficiency. We cover comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution, emphasizing critical steps like heel pad preservation and neurovascular protection. Learn to manage unique challenges, prevent complications, and optimize functional outcomes for these complex pediatric limb salvage procedures.
Comprehensive Introduction and Patho-Epidemiology
Congenital fibular deficiency, historically and somewhat inaccurately termed fibular hemimelia, represents the most common longitudinal long bone deficiency encountered in pediatric orthopaedic practice. The nomenclature shift from "hemimelia" to "deficiency" is critical; it reflects our modern understanding that this pathology is not merely an isolated absence or hypoplasia of the fibula, but rather a complex, pan-limb dysplasia. This spectrum of anomalies affects the entire lower extremity, extending from the proximal femur down to the terminal phalanges of the foot. Recognizing this pan-limb involvement is the foundational step in formulating a comprehensive, definitive treatment strategy for these complex pediatric patients.

The clinical presentation of fibular deficiency is highly variable, demanding a nuanced approach to patient evaluation. Patients typically present with a constellation of deformities that may include profound limb shortening, an equinovalgus foot posture, and characteristic skin dimpling over the mid-anterior tibia. The severity of the deformity exists on a wide continuum, ranging from a nearly normal clinical appearance with mild limb-length discrepancy to severe, debilitating deformities characterized by a completely absent fibula, a severely bowed tibia, and a non-functional, oligodactylous foot.
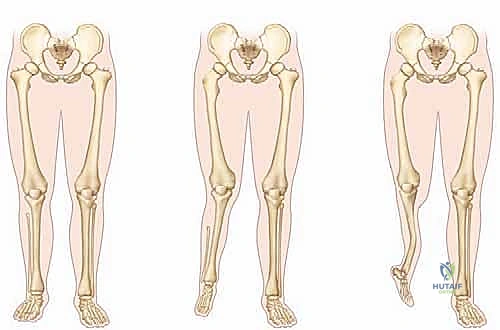
Understanding the associated ipsilateral deformities is paramount for the operating surgeon. At the level of the femur, one frequently encounters mild to moderate shortening, femoral retroversion, and lateral femoral hypoplasia. The knee joint is notoriously problematic, often exhibiting cruciate ligament deficiency (predominantly the anterior cruciate ligament), significant valgus alignment, and patellofemoral instability. It is imperative to remember that severe anterior or posterior laxity, evidenced by a profoundly positive Lachman's test, dramatically increases the risk of knee subluxation if extensive limb lengthening were to be erroneously attempted. The tibia typically demonstrates shortening and a characteristic anteromedial diaphyseal bowing (tibial kyphosis). Unlike anterolateral bowing associated with neurofibromatosis or congenital pseudarthrosis, this anteromedial bow typically does not portend an increased fracture risk, though it complicates alignment.
At the level of the ankle and foot, the structural deficits often dictate the surgical intervention. The ankle frequently exhibits severe valgus, an absent lateral malleolus, profound subluxation or instability, and the classic "ball-and-socket" ankle joint morphology. The hindfoot typically demonstrates drastically reduced subtalar motion, which should immediately raise the surgeon's clinical suspicion for underlying tarsal coalitions. Finally, the foot itself often suffers from absent tarsal bones, complex coalitions, and the absence of one or more lateral rays. A rigid, insensate, or nonfunctional foot is widely considered a primary and strong indication for early amputation, as it precludes the development of a normal, propulsive gait cycle regardless of any proximal lengthening procedures.
Detailed Surgical Anatomy and Biomechanics
Mastery of the surgical anatomy is the absolute prerequisite for executing either a Syme or a Boyd amputation with precision. The most critical anatomical consideration in these procedures is the meticulous preservation of the posterior tibial neurovascular bundle. The posterior tibial artery and nerve course posterior to the medial malleolus before bifurcating into the medial and lateral plantar nerves and arteries. The viability of the heel pad—the specialized, fibrofatty tissue that will become the primary weight-bearing surface of the amputated stump—is entirely dependent on the medial calcaneal branches arising from the posterior tibial artery. Iatrogenic injury to this bundle during the posterior dissection of the calcaneus will invariably lead to catastrophic flap necrosis.
The heel pad itself is a marvel of biomechanical engineering, uniquely suited for the demands of end-bearing. Unlike typical subcutaneous fat, the adipose tissue of the heel pad is compartmentalized within dense, U-shaped fibrous septa that anchor the thick plantar dermis directly to the periosteum of the calcaneus. This loculated structure acts as a highly efficient hydraulic shock absorber, dissipating the immense compressive and shear forces generated during the heel strike phase of the gait cycle. During the subperiosteal dissection required in both the Syme and Boyd procedures, the surgeon must stay strictly within the subperiosteal plane to avoid violating these fibrous septa; disrupting this architecture significantly degrades the pad's load-bearing capacity and increases the risk of painful adventitial bursa formation.

Osteologically, the pediatric ankle presents unique challenges due to the presence of open physes and extensive cartilaginous anlagen. The distal tibial physis is a crucial landmark and must be meticulously preserved to ensure continued longitudinal growth of the stump. In infants and young children, a significant portion of the distal tibia and the tarsal bones, particularly the calcaneus, remains unossified cartilage. This requires the surgeon to rely heavily on tactile feedback and a deep understanding of pediatric cross-sectional anatomy, rather than purely radiographic landmarks, when performing the calcaneal osteotomy in a Boyd procedure or when resecting the malleoli in a Syme amputation.

Biomechanically, the goal of both the Syme and Boyd amputations is to create a robust, end-bearing stump that allows for direct load transfer through the distal residuum. This is in stark contrast to a standard transtibial (below-knee) amputation, which relies on total contact or patellar tendon-bearing sockets that offload the distal end. The end-bearing capability of the Syme and Boyd stumps provides superior proprioception, allows for short-distance ambulation without a prosthesis (e.g., walking to the bathroom at night), and generally permits a more physiological gait pattern. The Boyd procedure, by preserving a portion of the calcaneus and fusing it to the tibia, theoretically provides a broader, more stable bony base for the heel pad, though the Syme disarticulation remains the gold standard due to its slightly lower technical complexity and excellent long-term outcomes.
Exhaustive Indications and Contraindications
The decision-making process regarding amputation versus complex limb reconstruction and lengthening in congenital fibular deficiency is one of the most challenging in pediatric orthopaedics. It requires a highly individualized approach, taking into account the severity of the anatomical deficits, the projected limb-length discrepancy at skeletal maturity, the functional status of the foot, and the psychosocial dynamics of the patient's family. We generally advocate for amputation when the projected leg-length discrepancy at skeletal maturity is anticipated to be massive, typically defined as greater than 30% of the contralateral limb length, or an absolute difference exceeding 15 to 20 centimeters.
A paramount consideration is the functional capacity of the foot. A nonfunctional foot, characterized by severe rigidity, absent lateral rays, profound equinovalgus deformity that cannot be rendered plantigrade, or absent sensation, is a definitive indication for amputation, irrespective of the presence or absence of a hypoplastic fibula. Attempting to lengthen a limb that terminates in a useless, painful foot is a disservice to the patient, leading to multiple morbid surgeries and ultimately, functional failure. Furthermore, severe ankle instability or profound subluxation, often seen in conjunction with a ball-and-socket ankle joint, makes extensive limb lengthening highly impractical and prone to catastrophic failure, further tipping the scales toward early amputation.
The timing of the amputation is a critical factor in optimizing outcomes. Extensive clinical experience and long-term outcome studies strongly support early amputation, ideally performed between 10 to 18 months of age. This window coincides with the child's natural developmental milestone of pulling to stand and initiating independent ambulation. Performing the amputation at this stage allows the child to incorporate the prosthesis into their developing body schema seamlessly. Psychosocial adjustment for both the child and the parents is remarkably rapid and robust at this age, whereas delayed amputations performed in older childhood or adolescence are frequently fraught with severe psychological distress, body image issues, and prolonged rehabilitation.
| Clinical Parameter | Indications for Syme/Boyd Amputation | Contraindications / Favor Lengthening |
|---|---|---|
| Projected LLD at Maturity | > 30% or > 15-20 cm | < 20% or < 10-15 cm |
| Foot Function | Rigid, insensate, non-plantigrade, missing >2 rays | Supple, plantigrade, sensate, functional rays |
| Ankle Stability | Severe instability, unbraceable ball-and-socket | Stable, functional range of motion |
| Knee Stability | Severe cruciate deficiency, high subluxation risk | Stable knee, negative Lachman's |
| Psychosocial Factors | Family desires definitive, early functional outcome | Family committed to multi-stage, multi-year lengthening |
| Vascular Status | Intact posterior tibial neurovascular bundle | Compromised posterior tibial artery (Absolute Contraindication) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning serves as the blueprint for surgical success in these complex reconstructions. The surgeon must develop a comprehensive, three-dimensional understanding of the patient's unique pathological anatomy, their remaining growth potential, and the ultimate functional goals. This begins with a rigorous imaging protocol. High-quality, full-length standing anteroposterior (AP) and lateral radiographs of the entire lower extremity, extending from the hips to the ankles, are crucial for assessing overall mechanical alignment, the degree of tibial bowing, and the presence of associated knee deformities in ambulatory children.
To accurately predict the expected leg-length discrepancy at skeletal maturity, a precise scanogram and a bone age determination (typically utilizing the Greulich and Pyle atlas of the left hand and wrist) are essential. Utilizing the Multiplier Method or the Paley Growth charts, the surgeon calculates the anticipated discrepancy. In the context of planning a Syme or Boyd amputation, we ideally aim for a residual limb length difference of at least 3.5 to 5.0 centimeters at maturity. This specific discrepancy is necessary to accommodate the vertical build height of a modern, energy-storing prosthetic foot mechanism beneath the stump, ensuring the knees remain level during the swing phase of gait.

Specific, dedicated radiographic series of the ankle and foot are mandatory to evaluate for the presence of ball-and-socket ankle morphology, occult tarsal coalitions, or absent/hypoplastic tarsal bones, which will directly influence the surgical approach and the choice between a Syme disarticulation and a Boyd arthrodesis. While advanced cross-sectional imaging such as MRI or CT is not routinely required for standard amputations, it may be selectively utilized in highly complex, atypical cases to precisely delineate aberrant soft tissue anatomy, assess ligamentous integrity, or map complex, multi-planar tarsal coalitions prior to surgical intervention.
Patient positioning and operating room setup must be executed flawlessly to facilitate precise surgical execution. The pediatric patient is placed supine on the operating table. A small bump or bolster is strategically placed beneath the ipsilateral greater trochanter; this serves to internally rotate the hip slightly, counteracting the natural external rotation of the limb and ensuring the foot and ankle are positioned in neutral alignment for optimal surgical access. A pneumatic tourniquet is applied high on the proximal thigh. Exsanguination and tourniquet inflation provide an absolutely bloodless surgical field, which is a non-negotiable requirement for the meticulous, microscopic dissection required to identify and preserve the delicate posterior tibial neurovascular structures. The limb is prepped and draped free from the mid-thigh down to the toes, utilizing a sterile stockinette and split sheet to allow for unrestricted, multi-planar manipulation of the foot and ankle throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The Syme Amputation: Precision Disarticulation
The Syme amputation is essentially a precise ankle disarticulation coupled with the meticulous preservation and repositioning of the specialized heel pad. The procedure begins with the design of the classic fish-mouth incision. The dorsal incision is initiated by identifying the tip of the lateral malleolus (or its anticipated location if absent). A curvilinear incision is drawn across the anterior aspect of the ankle joint, terminating approximately 1 to 1.5 centimeters distal to the tip of the medial malleolus. This specific termination point is critical to ensure the medial malleolar vascular plexus is preserved.


The plantar incision connects the medial and lateral extents of the dorsal incision. It begins at the midportion of the metatarsal shafts, carrying proximally along the medial and lateral borders of the foot, curving gently to meet the anterior incision. This creates the essential fish-mouth pattern, ensuring an abundance of thick, specialized plantar skin and soft tissue to provide robust coverage for the distal tibial stump.



Deep dissection commences by deepening the dorsal incision directly down to the bone using a #15 blade, maintaining a perpendicular angle to the skin to ensure clean, viable edges. The anterior compartment structures, including the extensor tendons, the anterior tibial artery, and the deep peroneal nerve, are sharply divided. The anterior ankle joint capsule is then incised, exposing the talar dome.


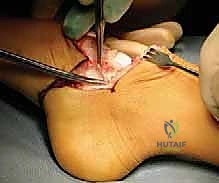
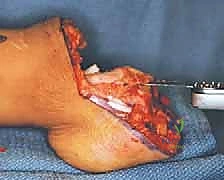
The most perilous and technically demanding phase of the Syme amputation is the posterior dissection and the enucleation of the calcaneus from the heel pad. As the foot is forcefully plantarflexed, the collateral ligaments are released from the inside out. The dissection must proceed strictly in the subperiosteal plane along the medial, lateral, and posterior aspects of the calcaneus.


Utilizing a sharp Cobb elevator or a specialized pediatric periosteal elevator, the surgeon meticulously peels the thick periosteal sleeve off the calcaneus. Straying even millimeters outside this plane medially risks catastrophic transection of the posterior tibial artery and the medial calcaneal branches, dooming the heel pad to ischemic necrosis. The Achilles tendon is carefully detached from the calcaneal tuberosity, taking care not to buttonhole the posterior skin.


Once the foot is entirely removed, attention is turned to the distal tibia. In the pediatric patient, the medial and lateral malleoli (if present) are carefully resected flush with the distal tibial articular surface. It is of paramount importance to strictly avoid violating the distal tibial physis during this resection, as premature physeal arrest will lead to a severely shortened stump and significant prosthetic fitting challenges later in life.


Finally, the heel pad is meticulously centralized over the distal tibia. To prevent the notorious complication of heel pad migration, the pad is typically secured to the distal tibia using heavy absorbable sutures passed through drill holes in the distal tibial metaphysis, or temporarily pinned with a smooth Kirschner wire driven through the heel pad and into the medullary canal of the tibia.

The Boyd Amputation: Calcaneotibial Arthrodesis
The Boyd amputation represents a sophisticated evolution of the Syme, designed to preserve a portion of the calcaneus and achieve a calcaneotibial arthrodesis. This technique preserves the calcaneal apophysis, theoretically maintaining a slightly longer, more bulbous stump that provides a superior, broader base for end-bearing and enhanced suspension of the prosthesis. The initial incisions are similar to the Syme but are placed slightly more distally to accommodate the retained calcaneal bone.


Following the initial deep dissection and anterior capsulotomy, the talus is excised. The crucial step in the Boyd procedure is the calcaneal osteotomy. The anterior process of the calcaneus is resected, and a horizontal osteotomy is performed to remove the superior articular surfaces of the calcaneus, creating a flat, bleeding cancellous bone bed.


Simultaneously, the articular cartilage of the distal tibia is meticulously denuded, exposing the subchondral bone while taking extreme care to preserve the underlying physis. The prepared calcaneus is then translated anteriorly and superiorly, docking it directly against the prepared distal tibia.

The arthrodesis site is rigidly fixed, typically utilizing one or two smooth, stout Kirschner wires driven retrograde from the plantar aspect of the heel pad, through the retained calcaneus, and across the physis into the distal tibial metaphysis. Proper alignment is critical; the calcaneus must be positioned in neutral dorsiflexion/plantarflexion and neutral varus/valgus to ensure an even distribution of weight-bearing forces.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following Syme and Boyd amputations in the pediatric population can occur and must be anticipated. The most frequent and functionally detrimental complication is the migration of the heel pad. If the heel pad drifts posteriorly or medially, the distal tibia will bear weight directly against thin, unspecialized anterior skin, leading to rapid skin breakdown, ulceration, and an inability to wear a prosthesis. This underscores the absolute necessity of secure intraoperative fixation of the pad to the bone.
Ischemic necrosis of the heel pad flap is a catastrophic complication, almost exclusively resulting from iatrogenic injury to the posterior tibial artery or its medial calcaneal branches during the difficult subperiosteal dissection of the calcaneus. If significant necrosis occurs, salvage options are severely limited and often require conversion to a higher-level, transtibial amputation, sacrificing the immense benefits of an end-bearing stump.
Neuroma formation, particularly of the transected deep peroneal or posterior tibial nerves, can cause intractable stump pain. Meticulous technique, involving proximal traction, sharp transection, and allowing the nerve end to retract deep into the proximal soft tissue bed away from the weight-bearing surface and the surgical scar,
Clinical & Radiographic Imaging Archive






