Masterclass: Operative Management of Thumb CMC Joint Fractures

Key Takeaway
Join us in the OR for a comprehensive masterclass on operative management of thumb CMC joint fractures. This guide details preoperative planning, precise surgical anatomy, step-by-step intraoperative execution for Bennett and Rolando fractures, including both closed reduction percutaneous pinning (CRPP) and open reduction internal fixation (ORIF) techniques. Learn critical pearls, potential pitfalls, and comprehensive postoperative care for optimal patient outcomes.
Introduction and Epidemiology
The first carpometacarpal joint is the functional cornerstone of the human hand, providing the essential mobility and stability required for prehension, grip, and pinch strength. Intra-articular fractures of the thumb metacarpal base represent significant disruptions to this highly specialized articulation. Because the thumb contributes up to fifty percent of overall hand function, failure to recognize and anatomically restore these fracture-dislocations inevitably leads to chronic pain, profound weakness, and rapid onset of debilitating post-traumatic arthrosis.
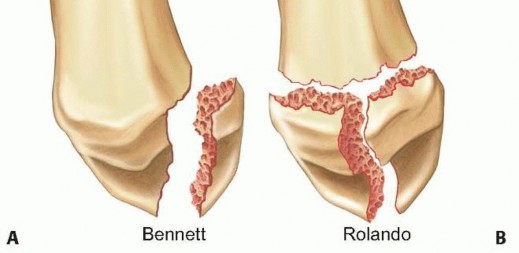
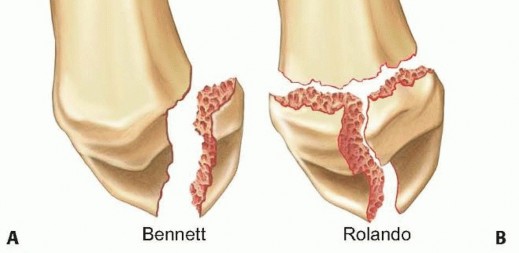
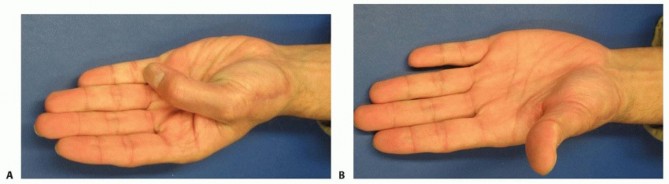
A Bennett fracture is defined as an intra-articular, unicondylar fracture-dislocation of the base of the first metacarpal. The hallmark of this injury is the retention of the volar-ulnar fragment in its anatomical position, secured by the strong anterior oblique ligament, while the remainder of the metacarpal shaft is displaced by unyielding muscular forces.
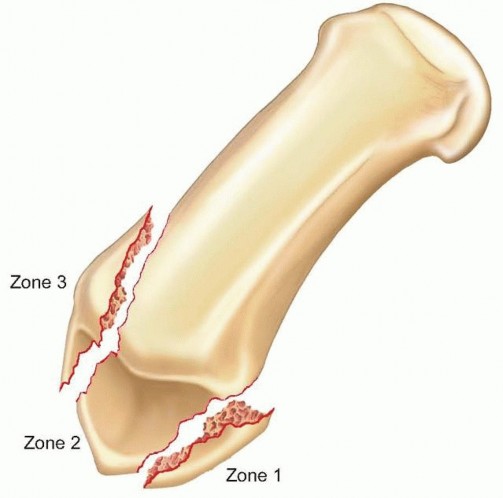
A Rolando fracture, first described in 1910 by Silvio Rolando, is a more severe, complex intra-articular fracture of the first metacarpal base. Classically characterized by a three-part T- or Y-shaped fracture pattern, the modern definition encompasses any multifragmentary or highly comminuted articular fracture of the thumb base where no portion of the metacarpal shaft remains in continuity with the carpometacarpal joint.



Epidemiological Profile
Fractures of the base of the first metacarpal account for approximately four percent of all hand fractures and represent the most frequent fracture involving the thumb. These injuries predominantly affect young, active males, typically occurring in the second to fourth decades of life. The mechanism of injury almost universally involves an axial load applied to a partially flexed and abducted thumb metacarpal. This frequently occurs during athletic endeavors, particularly in combat sports, football, and skiing, or as a result of high-energy trauma such as motor vehicle collisions or workplace incidents.
Mechanism of Injury and Pathoanatomy
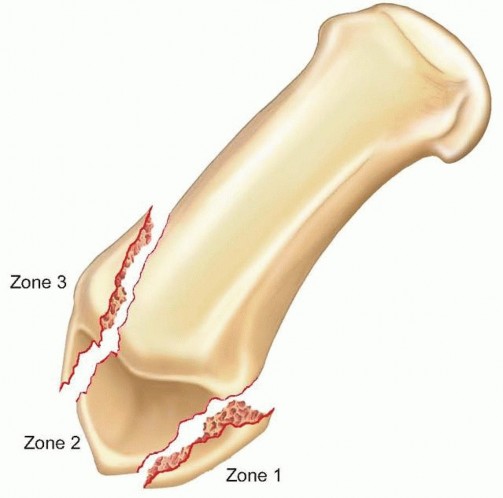
The transmission of force through the first carpometacarpal joint during axial loading dictates the fracture pattern. When the thumb is slightly flexed, the volar lip of the metacarpal base impacts the trapezium. The strong volar ligaments, particularly the anterior oblique ligament, hold the volar-ulnar fragment in place. As the axial force continues, the metacarpal shaft shears dorsally, radially, and proximally. In high-energy scenarios, the articular surface fails in multiple planes, resulting in the comminution characteristic of a Rolando fracture or a highly comminuted variant.


Classification Systems
While Bennett and Rolando are the most commonly used eponymous designations, several formal classification systems exist to guide treatment. The Green and O'Brien classification categorizes first metacarpal base fractures into four types. Type I is the classic Bennett fracture. Type II is the Rolando fracture. Type III represents extra-articular transverse or oblique fractures of the metacarpal base, and Type IV describes pediatric epiphyseal injuries, most commonly Salter-Harris Type II fractures. Understanding these classifications is paramount for the orthopedic surgeon, as the presence and degree of articular involvement strictly dictate the necessity and modality of operative intervention.
Surgical Anatomy and Biomechanics
A profound understanding of the complex osteology, ligamentous restraints, and dynamic muscular forces acting upon the first carpometacarpal joint is an absolute prerequisite for successful operative management.
Osteology of the First Carpometacarpal Joint
The first carpometacarpal joint is a highly specialized, biconcavoconvex saddle joint formed by the articulation between the base of the first metacarpal and the distal articular surface of the trapezium. The trapezium is concave in the radioulnar plane and convex in the dorsovolar plane. Conversely, the base of the first metacarpal is convex in the radioulnar plane and concave in the dorsovolar plane. This unique geometry permits a wide arc of motion across multiple planes, including flexion, extension, abduction, adduction, and the composite motion of opposition, while inherently sacrificing intrinsic bony stability.


Ligamentous Anatomy
Because the bony architecture provides minimal constraint, stability is heavily reliant on a robust capsuloligamentous complex. Five primary ligaments stabilize the first carpometacarpal joint.
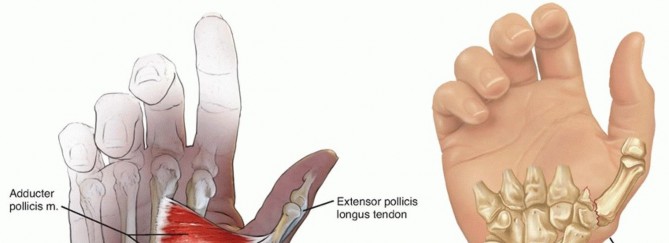
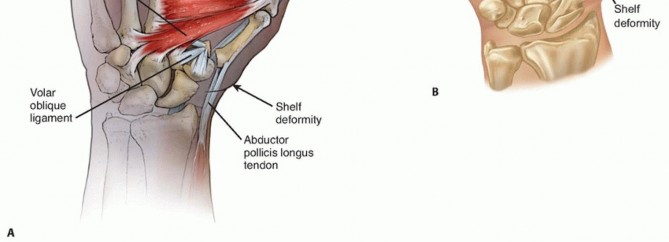
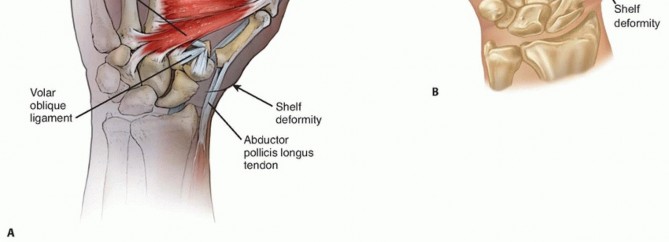
The anterior oblique ligament, often referred to as the volar beak ligament, is the most critical stabilizer against dorsal subluxation of the metacarpal. It originates from the palmar tubercle of the trapezium and inserts onto the volar-ulnar lip of the first metacarpal. In a Bennett fracture, this ligament remains intact, tethering the small volar-ulnar fragment to the trapezium.
The dorsoradial ligament is broad and stout, providing significant resistance to dorsal dislocation. Recent biomechanical studies suggest the dorsoradial ligament may be just as critical, if not more so, than the anterior oblique ligament in preventing dorsal subluxation during early opposition.
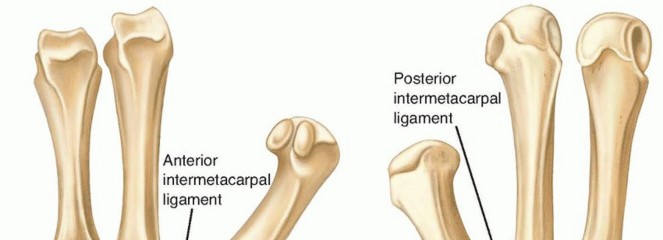
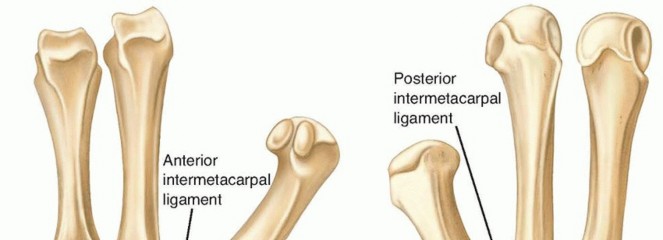
The intermetacarpal ligament tethers the base of the first metacarpal to the base of the second metacarpal, resisting radial displacement. The posterior oblique ligament and the ulnar collateral ligament of the carpometacarpal joint provide additional secondary stability.
Muscular Deforming Forces
The characteristic displacement of a Bennett fracture is driven by three primary muscular forces that must be overcome during reduction.
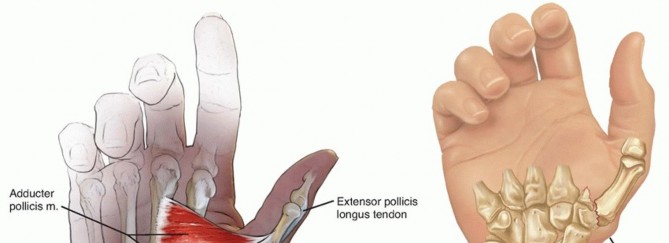
First, the abductor pollicis longus inserts on the dorsal-radial base of the first metacarpal. Upon fracture, the abductor pollicis longus forcefully pulls the metacarpal shaft proximally, dorsally, and radially.
Second, the adductor pollicis, inserting on the ulnar sesamoid and the ulnar base of the proximal phalanx, exerts a supination and adduction force on the distal aspect of the metacarpal, exacerbating the displacement and creating a varus deformity at the fracture site.
Third, the extensor pollicis longus and extensor pollicis brevis contribute to the proximal and dorsal migration of the shaft. The interplay of these unyielding forces makes closed reduction difficult to maintain without mechanical fixation.

Biomechanics of the Thumb Base
The biomechanical loads experienced by the first carpometacarpal joint are disproportionately high relative to its size. During simple pinch maneuvers, the joint reaction forces at the carpometacarpal articulation are magnified significantly due to the lever arm mechanics of the thumb. A one-kilogram pinch force at the tip of the thumb translates to approximately twelve kilograms of compressive force across the carpometacarpal joint. During strong power grip, these forces can exceed one hundred and twenty kilograms.
This massive force transmission explains why even minor articular incongruities (greater than one millimeter) rapidly lead to altered contact mechanics, focal cartilage overload, and advanced post-traumatic osteoarthritis. Anatomical reduction is not merely a radiographic goal; it is a biomechanical necessity for long-term joint survival.
Indications and Contraindications
The decision-making process for thumb carpometacarpal joint fractures hinges on the degree of articular displacement, the presence of comminution, and the inherent instability of the fracture pattern. Because of the high joint reaction forces, the tolerance for articular step-off is exceedingly low.

Operative vs Non Operative Criteria
| Clinical Scenario | Treatment Modality | Primary Indications |
|---|---|---|
| Non-Operative | Closed Reduction and Cast Immobilization | Extra-articular fractures with minimal angulation (<30 degrees). Intra-articular fractures with absolutely no displacement (<1mm) that remain stable under fluoroscopic stress. |
| Operative (CRPP) | Closed Reduction and Percutaneous Pinning | Bennett fractures reducible to <1mm articular step-off via closed maneuvers. Large volar-ulnar fragment capable of capturing a K-wire. |
| Operative (ORIF) | Open Reduction and Internal Fixation | Bennett fractures with >1mm step-off after closed reduction attempts. Rolando fractures with large, reconstructable articular fragments. Delayed presentations. |
| Operative (Ex-Fix) | External Fixation / Distraction | Severe, highly comminuted Rolando fractures where internal fixation is impossible. Severe soft tissue compromise. |
Contraindications to Surgical Intervention
Absolute contraindications to internal fixation include active local or systemic infection, severe medical comorbidities precluding anesthesia, and non-ambulatory patients with minimal functional demands where the risks of surgery outweigh the benefits.
Relative contraindications include pre-existing, advanced, symptomatic osteoarthritis of the first carpometacarpal joint. In older patients with significant pre-existing Eaton-Littler Stage III or IV arthrosis who sustain a Bennett or Rolando fracture, attempting osteosynthesis may be futile and counterproductive. In such specific scenarios, primary acute trapeziectomy with or without ligament reconstruction and tendon interposition, or primary arthrodesis, may be considered as a definitive single-stage procedure.



Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential to anticipate the required fixation constructs and minimize intraoperative delays.
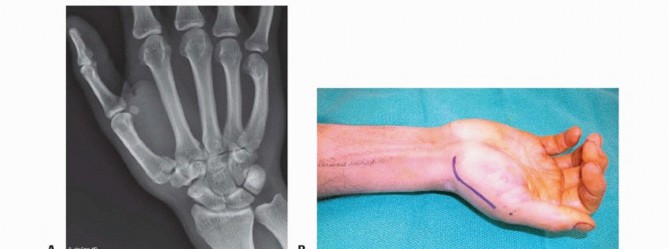
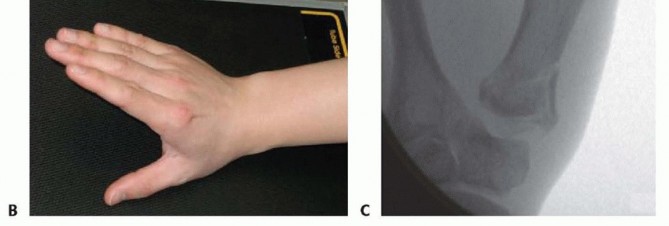
Radiographic Evaluation
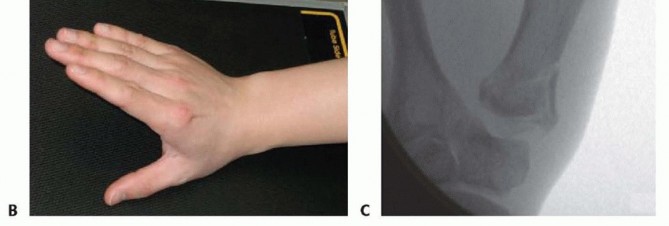
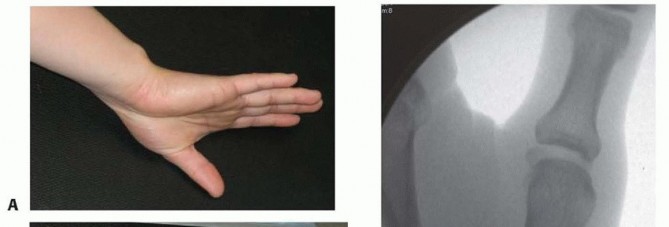
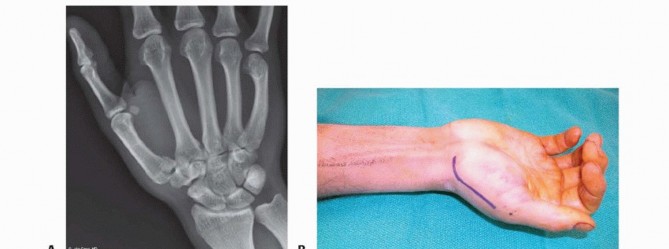
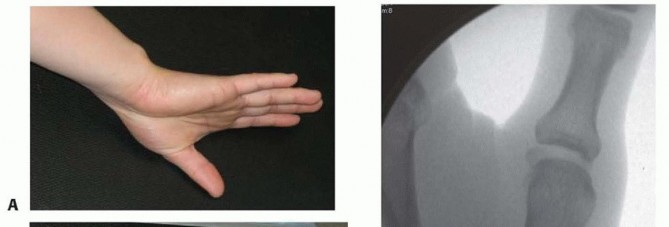
Standard anteroposterior, lateral, and oblique radiographs of the hand are often insufficient for detailed evaluation of the first carpometacarpal joint due to the natural pronation of the thumb. A true anteroposterior view of the first carpometacarpal joint, known as the Robert's view, is mandatory. This is obtained by hyperpronating the patient's forearm with the dorsum of the thumb resting flat against the cassette, and directing the X-ray beam at a fifteen-degree angle distal to proximal.
A Bett's view can also be utilized to profile the trapeziometacarpal joint without overlap. For complex Rolando fractures, a fine-cut computed tomography scan with sagittal and coronal reconstructions, as well as three-dimensional surface rendering, is highly recommended. The computed tomography scan delineates the exact number of articular fragments, the degree of impaction, and the precise location of the fracture lines, which is critical for planning plate placement and screw trajectories.


Patient Positioning and Operating Room Setup
The patient is positioned supine on the operating table with the affected extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The use of a regional axillary or supraclavicular brachial plexus block is highly advantageous, providing excellent intraoperative muscle relaxation and prolonged postoperative analgesia.
The fluoroscopy unit (C-arm) is positioned either perpendicular to the hand table or coming from the head/foot of the bed, depending on surgeon preference, ensuring unimpeded access to the surgical field. The monitor must be placed in the direct line of sight of the primary surgeon.
Equipment Selection
The surgical tray must include a comprehensive mini-fragment set. For Bennett fractures, 1.5 millimeter and 2.0 millimeter lag screws are typically utilized. For Rolando fractures, 1.5 millimeter or 2.0 millimeter T-plates, L-plates, or specialized condylar locking plates are required. A wide array of Kirschner wires (0.035, 0.045, and 0.062 inches) must be available for provisional fixation and potential definitive pinning. Dental picks, small Freer elevators, and fine reduction forceps (pointed tenaculums) are essential for manipulating small articular fragments.


Detailed Surgical Approach and Technique
The surgical management of thumb base fractures demands meticulous soft tissue handling and precise osteosynthesis. The choice of technique is dictated by the fracture pattern.
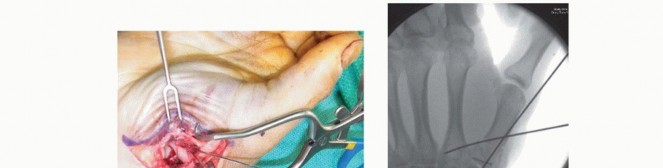
Closed Reduction and Percutaneous Pinning
For Bennett fractures where closed reduction achieves an articular step-off of less than one millimeter, percutaneous pinning is the treatment of choice.
The reduction maneuver must counteract the deforming muscular forces. The surgeon grasps the patient's thumb and applies longitudinal axial traction. The thumb is then placed into palmar abduction and pronation. This maneuver tensions the intact volar ligaments and uses the intact soft tissue hinge to guide the metacarpal shaft back to the volar-ulnar fragment. Finally, direct manual pressure is applied to the dorsal-radial base of the metacarpal to push it volarly and ulnarly.
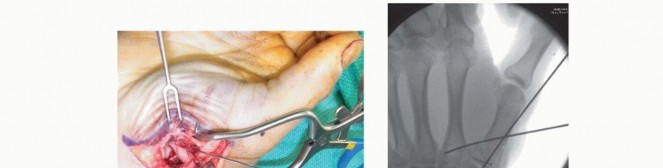
Once reduction is confirmed via fluoroscopy in multiple planes, percutaneous pinning is performed. A 0.045-inch Kirschner wire is driven from the dorsal-radial aspect of the metacarpal shaft into the trapezium to maintain the reduction. A second pin is often placed from the metacarpal shaft into the base of the second metacarpal for additional rotational stability. Attempting to pin the small volar-ulnar fragment directly is technically demanding and often unnecessary; transfixing the shaft to the carpus or adjacent metacarpal neutralizes the deforming forces effectively.


Open Reduction and Internal Fixation
When closed reduction fails to restore articular congruity, or in the presence of a displaced Rolando fracture, open reduction and internal fixation is mandated.
The Wagner Approach
The classic radiopalmar approach, described by Wagner, provides excellent visualization of the first carpometacarpal joint. An L-shaped or gently curved incision is made along the glabrous border of the thenar eminence, curving dorsally over the base of the first metacarpal.
Subcutaneous dissection must proceed with extreme caution to identify and protect the sensory branches of the superficial radial nerve dorsally and the lateral antebrachial cutaneous nerve volarly. Retraction of these nerves must be gentle to prevent debilitating postoperative neuromas.
The thenar musculature (abductor pollicis brevis and opponens pollicis) is elevated extraperiosteally from the metacarpal shaft and retracted volarly. The abductor pollicis longus tendon is identified and retracted dorsally. This exposes the capsule of the carpometacarpal joint. A longitudinal or T-shaped arthrotomy is performed to visualize the articular surface.



Fracture Reduction and Fixation
Hematoma and soft tissue interposition are meticulously cleared from the fracture site using a dental pick and irrigation. The articular surface is directly visualized.
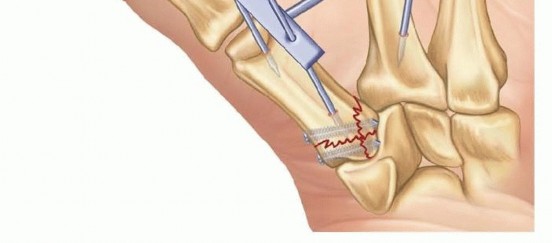
For a Bennett fracture, the shaft is reduced to the volar-ulnar fragment using a pointed reduction forceps. Provisional fixation is achieved with a 0.035-inch Kirschner wire. Definitive fixation is typically accomplished using one or two 1.5 millimeter or 2.0 millimeter lag screws. The gliding hole is drilled in the near cortex (the shaft), and the thread hole is drilled in the far cortex (the volar-ulnar fragment). Countersinking is crucial to prevent the screw head from prominent impingement beneath the skin or tendons, but care must be taken not to plunge through the thin metaphyseal cortex.
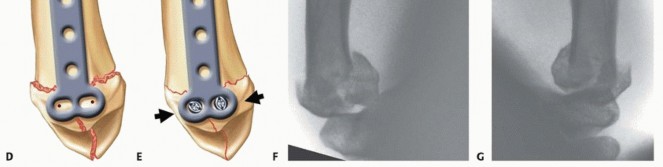
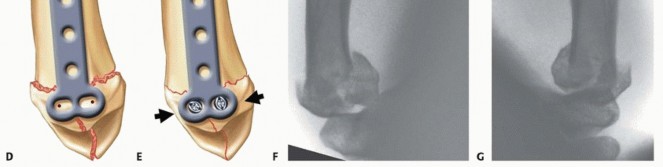
For a Rolando fracture, the complexity of fixation increases exponentially. The articular fragments must be assembled first. Often, the volar and dorsal fragments are reduced and provisionally pinned, converting the T- or Y-fracture into a two-part fracture resembling a Bennett pattern. A small T-plate or condylar plate is then contoured to the dorsal-radial aspect of the metacarpal base. Locking plates provide superior biomechanical stability in osteopenic bone or highly comminuted patterns. Bone grafting, utilizing cancellous autograft from the distal radius, may be necessary to support articular elevation in cases of severe impaction.

External Fixation and Distraction
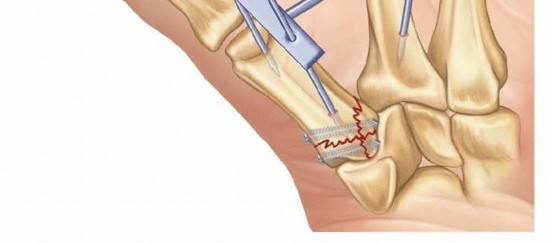
In highly comminuted Rolando fractures where the fragments are too small to hold internal fixation, the principles of ligamentotaxis are employed. A mini-external fixator is applied construct spanning the first carpometacarpal joint. Pins are placed in the trapezium (or distal radius) and the first metacarpal shaft. Distraction is applied to restore length and align the articular fragments via the tensioning of the intact capsuloligamentous structures. Limited open reduction and percutaneous pinning of major articular fragments can be performed as an adjunct to the external fixator.


Complications and Management
Despite meticulous surgical technique, complications following the operative treatment of thumb base fractures are not uncommon. The surgeon must be prepared to identify and manage these issues effectively.
Summary of Complications
| Complication | Estimated Incidence | Etiology and Pathophysiology | Management and Salvage Strategies |
|---|---|---|---|
| Post-Traumatic Arthritis | 20-50% (Long-term) | Inadequate articular reduction (>1mm step-off), initial cartilage impact necrosis. | Conservative (NSAIDs, splinting, injections). Salvage: Trapeziectomy with LRTI or CMC Arthrodesis. |
| Superficial Radial Neuroma | 5-10% | Iatrogenic traction injury or direct laceration during the Wagner or dorsal approach. | Gabapentinoids, desensitization therapy. Surgical excision and nerve burial into muscle/bone for refractory cases. |
| Hardware Prominence | 10-15% | Prominent screw heads or bulky plates under the thin dorsal skin causing tendon irritation. | Hardware removal after complete radiographic union (typically >6 months post-op). |
| Pin Tract Infection | 5-15% (with CRPP) | Bacterial colonization of percutaneous K-wires. | Oral antibiotics, local wound care. Early pin removal if deep infection or osteomyelitis is suspected. |
| Loss of Reduction | 2-5% | Premature pin removal, non-compliant patient, inadequate initial fixation. | Revision ORIF if identified early. Late presentation requires corrective osteotomy or salvage arthroplasty. |
Post Traumatic Osteoarthritis
Post-traumatic osteoarthritis is the most frequent long-term complication. Even with anatomical reduction, the initial chondral injury sustained at the moment of impact can initiate a cascade of cartilage degradation. Patients present with insidious onset of pain localized to the thumb base, exacerbated by pinch and grip activities. Radiographs demonstrate joint space narrowing, subchondral sclerosis, and osteophyte formation.
Initial management is non-operative, utilizing rigid thumb spica orthoses, non-steroidal anti-inflammatory drugs, and intra-articular corticosteroid injections. When conservative measures fail, surgical salvage is indicated. In young, high-demand manual laborers, a trapeziometacarpal arthrodesis is preferred to provide a stable, painless pinch, albeit at the cost of mobility. In older or lower-demand patients, trapeziectomy with or without ligament reconstruction and
Clinical & Radiographic Imaging












You Might Also Like


