Masterclass: Percutaneous Intramedullary Screw Fixation for Jones Fractures

Key Takeaway
This masterclass provides an immersive, step-by-step guide to percutaneous intramedullary screw fixation for Jones fractures. Fellows will learn comprehensive surgical anatomy, meticulous preoperative planning, and precise intraoperative execution, including guidewire placement, reaming, and screw insertion. We cover critical pearls, potential pitfalls, and detailed postoperative care to ensure optimal patient recovery and minimize complications, focusing on the unique challenges of the fifth metatarsal's watershed blood supply.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass. Today, we are addressing a common yet notoriously challenging orthopedic injury: the Jones fracture. This is not merely another metatarsal fracture to be triaged and treated with benign neglect; its unique anatomical location and precarious vascular supply demand a precise understanding of bone biology, biomechanics, and meticulous surgical technique. Our goal is to ensure successful union, minimize the risk of refracture, and facilitate a rapid return to high-level activity, particularly for our elite athletic patient population.
Let us begin by establishing a rigorous definition of the pathology. A true Jones fracture represents an acute injury occurring specifically at the metaphyseal–diaphyseal junction of the fifth metatarsal. Crucially, as originally described and later refined in the orthopedic literature, the fracture line must not extend distal to the fourth–fifth intermetatarsal articulation. This strict anatomical distinction is vital for accurate diagnosis, as it differentiates the Jones fracture from proximal tuberosity avulsion fractures (pseudo-Jones fractures) and more distal diaphyseal stress fractures, both of which possess distinct natural histories, healing potentials, and treatment algorithms.

The natural history and outcomes of both nonoperative and operative treatments have historically been complex to interpret due to heterogenous reporting that frequently conflated acute Jones fractures with chronic diaphyseal stress fractures. However, contemporary epidemiological data unequivocally demonstrates that these fractures are disproportionately prevalent in the athletic population. The pathogenesis typically involves a combination of ankle plantarflexion and forefoot adduction, generating immense tensile forces across the lateral cortex of the fifth metatarsal. This specific vector of force, often experienced during rapid changes of direction, cutting maneuvers, or awkward landings in sports such as football, basketball, and soccer, initiates a transverse fracture pattern that, if severe, can propagate medially into the metatarsocuboid joint.

To guide our clinical decision-making and surgical strategy, we rely heavily on the Torg classification system. This framework categorizes fifth metatarsal base fractures into three distinct subsets based on chronicity, radiographic appearance, and healing potential. Type 1 represents the acute fracture. Radiographically, these lesions exhibit sharp, well-defined fracture margins without any evidence of intramedullary sclerosis, and the fracture typically involves only the lateral cortex initially, though it may be complete. Type 2 describes a delayed union. In these cases, the fracture line involves both cortices, and we observe associated periosteal new bone formation, a widening or cystic appearance of the fracture line, and early intramedullary sclerosis indicating a stalled biological healing response.

Finally, Type 3 denotes a frank nonunion. This represents a complete failure of the osteogenic process. Radiographs will demonstrate significant bone resorption with a wide radiolucent gap at the fracture site, and the medullary canal will be completely obliterated by dense sclerotic bone. Nonoperative treatment of acute Jones fractures, particularly in high-demand individuals, is associated with an unacceptably high risk of progression from Type 1 to Types 2 and 3. This progression is primarily dictated by the watershed blood supply at this critical junction, necessitating surgical intervention to alter the mechanical environment and stimulate osteogenesis.

Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a comprehensive, three-dimensional understanding of the regional anatomy is paramount. The proximal fifth metatarsal is a complex anatomical nexus where osteology, powerful tendinous insertions, and a vulnerable vascular network converge. The fifth metatarsal articulates proximally with the cuboid bone, forming the lateral aspect of the tarsometatarsal (Lisfranc) joint complex. Distally, it articulates with the proximal phalanx of the fifth toe. The metaphyseal-diaphyseal junction, our specific area of interest, lies immediately distal to the prominent fifth metatarsal tuberosity. The tuberosity itself serves as a crucial palpable landmark for surgical orientation and tendon insertions.
Muscular Attachments and Biomechanical Forces
Several powerful tendinous structures insert onto the proximal fifth metatarsal, exerting significant biomechanical forces that dictate fracture morphology and complicate healing. The peroneus brevis tendon inserts onto the dorsolateral aspect of the prominent tuberosity. As a primary evertor and plantarflexor of the foot, its eccentric contraction can distract fracture fragments, particularly in proximal avulsion injuries, but it also contributes to the bending moments experienced at the metaphyseal-diaphyseal junction.
Furthermore, the peroneus tertius tendon inserts onto the dorsal aspect of the metatarsal base, often extending precisely to the metaphyseal–diaphyseal junction. Acting as a dorsiflexor and evertor, its intimate anatomical relationship with the Jones fracture site means we must be acutely aware of its location during our surgical approach to avoid iatrogenic injury. Additionally, the lateral band of the plantar fascia has a robust insertion along the plantar aspect of the tuberosity. This structure is critical for longitudinal arch support and transmits massive tensile forces during the terminal stance and preswing phases of the gait cycle, further stressing the lateral cortex of the fifth metatarsal.
Neurovascular Considerations
Protecting the regional neurovascular structures is a non-negotiable priority during percutaneous fixation. The lateral aspect of the foot is innervated by branches of the sural nerve, which courses posterior to the lateral malleolus and provides critical sensory innervation to the lateral hindfoot, midfoot, and fifth digit. Dorsally, branches of the superficial peroneal nerve traverse the surgical field. Specifically, the lateral dorsal cutaneous branch is at high risk during percutaneous wire placement and screw insertion.
Surgeons must employ meticulous, blunt soft-tissue dissection down to the bone to avoid iatrogenic injury to these sensory nerves. Laceration, entrapment, or traction injury can result in debilitating neuromas, complex regional pain syndrome (CRPS), or persistent dysesthesias that can overshadow a successful bony union. The dorsal venous arch and its lateral tributaries are also present in this region and should be carefully mobilized or judiciously ligated to prevent postoperative hematoma formation, which can compromise wound healing.
Critical Blood Supply and the Watershed Zone
The most critical anatomical consideration governing the behavior of Jones fractures is the notoriously precarious blood supply of the proximal fifth metatarsal. The vascular architecture here creates a biological environment highly susceptible to ischemia. The diaphyseal shaft is primarily supplied by a single nutrient artery, which typically enters the bone from the medial cortex at the junction of the proximal and middle thirds of the diaphysis. This artery sends branches proximally toward the metaphysis.

Conversely, the base and tuberosity receive their blood supply from an extraosseous network of secondary epiphyseal and metaphyseal arteries. This anatomical arrangement creates a distinct watershed zone at the metaphyseal-diaphyseal junction—precisely where the Jones fracture occurs. This zone relies on the terminal, low-pressure anastomoses between the intramedullary nutrient supply and the extramedullary metaphyseal supply.
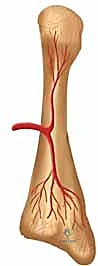
When a fracture occurs at this junction, it frequently disrupts these fragile anastomoses, rendering the fracture site relatively avascular. This inherent vascular vulnerability, combined with the high tensile forces acting on the lateral cortex, is the primary reason why nonoperative management of acute Jones fractures yields unacceptably high rates of delayed union and nonunion. Our surgical technique of intramedullary screw fixation aims to bypass this biological deficit by providing absolute mechanical stability, thereby allowing primary bone healing to occur across the watershed zone.

Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a Jones fracture requires a nuanced assessment of the fracture morphology, the patient's physiological status, and their functional demands. While nonoperative management (strict non-weight-bearing in a short leg cast) remains an option for truly acute (Type 1) fractures in low-demand, sedentary individuals, the paradigm has shifted heavily toward early surgical fixation for a vast majority of patients to mitigate the high risk of nonunion and prolonged disability.
The primary indication for percutaneous intramedullary screw fixation is an acute Jones fracture (Torg Type 1) in a high-demand patient, such as a competitive athlete, manual laborer, or active military personnel. In these populations, the goal is to minimize time away from sport or duty and provide the most predictable path to union. Furthermore, any patient presenting with a Torg Type 2 (delayed union) or Torg Type 3 (nonunion) fracture is an absolute candidate for surgical intervention, as these lesions will not heal with conservative measures alone. In cases of frank nonunion, intramedullary fixation must often be augmented with autogenous bone grafting (e.g., calcaneal or iliac crest autograft) or orthobiologics to stimulate the stalled biological environment.
Contraindications, while relatively few, must be strictly respected to avoid catastrophic outcomes. Active local or systemic infection represents an absolute contraindication to any internal fixation. Severe comminution of the metaphyseal-diaphyseal junction may preclude isolated intramedullary screw fixation, as the screw may not achieve adequate purchase or may fail to control rotational instability; in such cases, lateral plate osteosynthesis may be required. Furthermore, skeletal immaturity with an open proximal apophysis requires careful consideration; while smooth wires can be used, large-diameter threaded screws crossing an open physis can lead to premature closure and growth disturbance. Finally, patients with severe peripheral vascular disease, profound neuropathy (e.g., Charcot neuroarthropathy), or those who are demonstrably non-compliant with postoperative protocols are poor candidates for this procedure.
| Category | Specific Criteria | Rationale / Clinical Note |
|---|---|---|
| Indications | Acute Torg Type 1 in athletes | Minimizes downtime, predictable union, prevents progression to nonunion. |
| Torg Type 2 (Delayed Union) | Requires mechanical stabilization to overcome stalled healing. | |
| Torg Type 3 (Nonunion) | Absolute indication; usually requires adjunctive bone grafting. | |
| Patient Preference | Low-demand patients who refuse prolonged non-weight-bearing casting. | |
| Contraindications | Active Infection | Absolute contraindication to hardware placement. |
| Severe Comminution | IM screw cannot provide adequate rotational/length stability; consider plating. | |
| Skeletal Immaturity | Risk of apophyseal arrest; requires modified techniques (e.g., K-wires). | |
| Severe Neuropathy/PVD | High risk of hardware failure, nonunion, or wound breakdown. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful percutaneous intramedullary screw fixation. The anatomy of the fifth metatarsal is highly variable, particularly regarding the medullary canal diameter and the degree of lateral bowing. Failure to appreciate these nuances preoperatively frequently leads to catastrophic intraoperative complications, such as lateral cortical blowout or inadequate fracture compression.
Standard radiographic evaluation must include high-quality anteroposterior (AP), lateral, and oblique views of the foot. The AP view is critical for assessing the fracture gap and the medial-lateral diameter of the medullary canal. The lateral view is essential for evaluating the dorsal-plantar canal diameter and, most importantly, the plantar bow of the metatarsal shaft. The oblique view provides the best visualization of the metaphyseal-diaphyseal junction and the fourth-fifth intermetatarsal articulation. In cases of delayed union, nonunion, or complex fracture patterns, a computed tomography (CT) scan is highly recommended to assess bone stock, exact canal dimensions, and the presence of cystic changes that might necessitate bone grafting.

Templating is an absolute requirement. The surgeon must determine the appropriate screw diameter and length before the patient enters the operating room. The ideal screw should have a diameter that allows its threads to engage the endosteal diaphyseal cortex distal to the fracture site without causing excessive radial expansion that could fracture the bone. Typically, screw diameters range from 4.0 mm to 5.5 mm, with 4.5 mm and 5.0 mm being the most common in athletic populations. Regarding length, the screw must bypass the fracture site and engage the narrowest portion of the diaphysis (the isthmus) to ensure adequate pull-out strength. However, it must not be so long that it impinges on the lateral cortex due to the natural lateral bow of the metatarsal. The threads must cross the fracture line entirely to achieve interfragmentary compression.

Patient positioning must facilitate unhindered fluoroscopic access. The patient is typically positioned supine on a radiolucent operating table. A substantial bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral or slightly internally rotated position. This allows for a true AP view of the foot when the fluoroscopy C-arm is brought in vertically. The C-arm is usually positioned on the contralateral side of the table or coming in from the foot of the bed, depending on surgeon preference. A sterile tourniquet is applied to the thigh or calf, though it is often not inflated for percutaneous procedures unless open bone grafting is required. The operative leg is prepped and draped in standard sterile fashion, ensuring the entire foot and ankle are exposed.
Step-by-Step Surgical Approach and Fixation Technique
The execution of percutaneous intramedullary screw fixation for a Jones fracture is an exercise in precision. The margin for error is minimal, and adherence to a strict, step-by-step fluoroscopically guided protocol is mandatory to achieve optimal outcomes.
Incision and Guidewire Placement
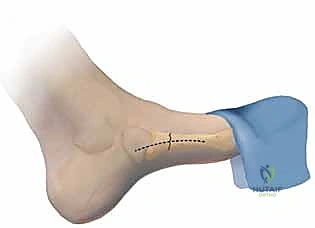
The procedure begins with the identification of the optimal starting point. This is the most critical step of the operation. The starting point must be "high and inside"—meaning slightly dorsal and medial on the proximal tuberosity. Starting too lateral or too plantar will result in a trajectory that inevitably intersects the lateral or plantar cortex of the diaphysis, leading to a blowout when the screw is inserted.
A 1 to 2 cm longitudinal incision is made directly over the base of the fifth metatarsal, extending proximally. Blunt dissection with a hemostat is performed down to the bone, carefully sweeping the sural nerve branches and the peroneus brevis tendon laterally. A soft tissue protector or drill guide is placed directly onto the bony starting point.

Under multi-planar fluoroscopic guidance, a guidewire (typically 1.6 mm or 2.0 mm, depending on the cannulated screw system) is introduced. On the AP view, the wire should be perfectly centered within the medullary canal, aiming toward the head of the fifth metatarsal. On the lateral view, the wire must remain parallel to the plantar cortex, respecting the natural bow of the bone. The guidewire is advanced across the fracture site and seated into the distal diaphysis, stopping short of the metatarsal neck.


Canal Preparation
Once the guidewire is perfectly positioned, canal preparation begins. A cannulated depth gauge is used to determine the appropriate screw length. It is crucial to remember that the screw threads must completely cross the fracture line to achieve compression.

Next, a cannulated drill bit is passed over the guidewire. Drilling should be performed carefully, under continuous or frequent fluoroscopic imaging, to ensure the drill bit does not deviate and breach the cortex. It is highly recommended to tap the proximal cortex and the diaphyseal canal, especially in young athletes with dense cortical bone. Tapping reduces the insertion torque required for the screw, significantly decreasing the risk of iatrogenic fracture distraction or screw breakage during insertion.


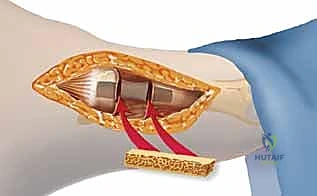
Screw Insertion and Final Assessment
With the canal prepared, the selected cannulated screw is advanced over the guidewire. Solid screws can be used and are biomechanically stronger, but they require removal of the guidewire prior to insertion, which risks losing the precise trajectory. If a cannulated system is used, a partially threaded screw is typically selected to provide interfragmentary compression.
As the screw head engages the proximal cortex, the surgeon must carefully monitor the fracture site on fluoroscopy. The fracture gap should close, indicating successful compression. Over-tightening must be avoided to prevent stripping the diaphyseal threads or crushing the proximal cancellous bone. The screw head should be countersunk slightly to prevent prominent hardware irritation beneath the thin soft-tissue envelope of the lateral foot.

Once the screw is fully seated, the guidewire is removed. Final fluoroscopic images are obtained in the AP, lateral, and oblique planes to confirm anatomic reduction, adequate fracture compression, and appropriate hardware placement without cortical breach. The wound is thoroughly irrigated and closed in layers, ensuring meticulous skin approximation.



Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, percutaneous intramedullary screw fixation of Jones fractures is associated with several distinct complications. Recognizing these risks preoperatively and possessing the surgical repertoire to manage them is the hallmark of an expert foot and ankle surgeon.
The most dreaded complication is symptomatic nonunion or delayed union, which occurs in approximately 5% to 10% of operatively treated cases. This is often multifactorial, stemming from inadequate fracture compression, use of an undersized screw that fails to provide rotational stability, or biological failure in the watershed zone. Management of a symptomatic nonunion typically requires revision surgery. The existing hardware must be removed, the sclerotic fracture edges debrided back to bleeding bone, and the defect grafted with autogenous cancellous bone. Fixation is then revised, often utilizing a larger diameter solid screw or, if the canal is compromised, a lateral neutralization plate.
Hardware failure, specifically screw breakage, is a catastrophic complication that usually occurs prior to clinical union. It is frequently the result of utilizing a screw with an insufficient core diameter (e.g., a 4.0 mm cannulated screw in a large athlete) or allowing the patient to return to weight-bearing activities prematurely. Salvage is technically demanding. The proximal screw fragment is easily removed, but the distal fragment embedded in the diaphysis requires specialized extraction techniques, such as the use of a hollow reamer or trephine. Once removed, the nonunion must be addressed with bone grafting and robust revision fixation.
Iatrogenic lateral cortical blowout occurs when the starting point is too lateral or the screw is too long, failing to accommodate the lateral bow of the metatarsal. This complication compromises the fixation construct and can lead to persistent pain and nonunion. If recognized intraoperatively, the screw must be removed, the trajectory redirected (if possible), or the fixation strategy converted to a lateral plate. Symptomatic hardware is common due to the prominent screw head irritating the overlying skin or the peroneus brevis tendon. This can be managed with simple hardware removal once robust clinical and radiographic union is achieved, typically no earlier than 6 to 12 months postoperatively.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion / Delayed Union | 5% - 10% | Undersized screw, poor compression, smoking, premature weight-bearing. | Revision ORIF, exchange nailing to larger solid screw, autologous bone grafting. |
| Screw Breakage | 2% - 5% | Small core diameter screw, premature return to sport, persistent nonunion. | Removal of broken hardware (often requires trephine), bone grafting, revision fixation (plate or larger screw). |
| Lateral Cortical Blowout | 3% - 6% | Incorrect starting point (too lateral), failure to accommodate lateral bow, screw too long. | Intra-op: Redirect trajectory or convert to plate. Post-op: Revision if symptomatic or unstable. |
| Sural Nerve Injury | 1% - 3% | Poor soft tissue dissection, aggressive retractor placement. | Conservative management (gabapentinoids); surgical neurolysis or neurectomy for refractory neuroma. |
| Symptomatic Hardware | 10% - 20% | Prominent screw head, inadequate countersinking, thin soft tissue envelope. | Hardware removal after confirmed radiographic and clinical union (usually > 6 months). |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the ultimate success of the procedure as the surgical fixation itself. While intramedullary screw fixation provides excellent mechanical stability, the biological healing of the watershed zone remains slow. A premature return to weight-bearing or sporting activities can easily overwhelm the fixation construct, leading to hardware failure and nonunion.
Phase 1: Maximum Protection (Weeks 0-2). Immediately postoperatively, the patient is placed in a well-padded short leg splint or a rigid fracture boot. The patient is instructed to remain strictly non-weight-bearing on the operative extremity, utilizing crutches or a knee scooter. Elevation and cryotherapy are emphasized to control edema and mitigate pain. At the two-week mark, sutures are removed, and the surgical incision is inspected.
Phase 2: Progressive Loading (Weeks 2-6). If the incision is well-healed and the patient's pain is controlled, they are transitioned to a controlled ankle motion (CAM) boot. Weight-bearing status is highly dependent on the surgeon's assessment of the fixation stability and the patient's compliance. Many surgeons allow progressive partial weight-bearing in the boot during this phase, advancing to full weight-bearing as tolerated by week 6. Active range of motion exercises for the ankle and toes are initiated to prevent stiffness, but forceful inversion and eversion are strictly avoided to protect the peroneus brevis insertion.
Phase 3: Functional Restoration and Return to Play (Weeks 6-12+). At the 6-week mark, updated radiographs are obtained. If there is evidence of bridging callus and obliteration of the fracture line, the patient is transitioned out of the CAM boot into a stiff-soled athletic shoe, often with a custom orthotic or carbon fiber footplate to limit metatarsal bending moments. Formal physical therapy is intensified, focusing on peroneal strengthening, proprioception, and gait mechanics. Return to high-impact sports or cutting maneuvers is absolutely prohibited until there is unequivocal clinical (absence of pain on palpation) and radiographic evidence of complete osseous union, which typically occurs between 8 and 12 weeks, though it can take longer in some individuals.
Summary of Landmark Literature and Clinical Guidelines
The evolution of our understanding and treatment of Jones fractures is deeply rooted in landmark orthopedic literature. A thorough grasp of these historical and contemporary studies is essential for evidence-based practice.
Sir Robert Jones first described this injury in 1902 after sustaining it himself while dancing. However, it was Torg et al. (1984) who revolutionized our approach by clearly differentiating acute fractures from delayed unions and nonunions, establishing the classification system that remains the gold standard today. Torg's work highlighted the dismal healing rates of nonoperative management for delayed unions, paving the way for surgical intervention.
The shift toward primary operative fixation for acute fractures in athletes was heavily influenced by Kavanaugh et al. (1978), who demonstrated significant delays in return to sport and high nonunion rates with casting. Later, DeLee et al. (1983) popularized the use of intramedullary screw fixation, demonstrating excellent union rates and rapid return to play in competitive athletes.
More recently, biomechanical studies by Porter et al. and Hunt et al. have refined our surgical technique. They emphasized the critical importance of screw diameter and length, proving that larger diameter screws (4.5 mm to 5.5 mm) provide superior bending stiffness and pull-out strength compared to smaller screws, significantly reducing the incidence of hardware failure. Furthermore, contemporary systematic reviews and meta-analyses consistently support the superiority of intramedullary screw fixation over nonoperative management in athletic populations, citing significantly faster times to union and lower rates of refracture, solidifying this technique as the standard of care in modern orthopedic sports medicine.
