Open Reduction of Supracondylar Fractures of the Humerus
Introduction and Epidemiology
Supracondylar fractures of the humerus are the most frequently encountered elbow fractures in the pediatric orthopedic population, accounting for approximately 60% to 70% of all pediatric elbow trauma. The incidence peaks between the ages of 5 and 7 years, coinciding with a period of increased ligamentous laxity and the biomechanical vulnerability of the remodeling distal humerus. In contrast, supracondylar fractures in the adult population are relatively rare, typically resulting from high-energy trauma (e.g., motor vehicle collisions, falls from height), and are frequently characterized by severe comminution, intra-articular extension, and compromised soft-tissue envelopes.
The vast majority of these injuries (approximately 95%) are extension-type fractures, classically resulting from a fall on an outstretched hand (FOOSH) with the elbow locked in hyperextension. This mechanism drives the olecranon into the olecranon fossa, utilizing it as a fulcrum to fracture the anatomically thin supracondylar region, subsequently displacing the distal fragment posteriorly. Flexion-type injuries comprise the remaining 5%, typically arising from direct trauma to the posterior aspect of the flexed elbow, driving the distal fragment anteriorly. Flexion-type fractures are notoriously unstable and carry a higher risk of ulnar nerve injury.
The modified Gartland classification system remains the universally accepted framework for categorizing pediatric extension-type supracondylar fractures and guiding treatment algorithms:
* Type I: Nondisplaced or minimally displaced (<2 mm) with an intact anterior humeral line.
* Type II: Displaced with an intact posterior cortex (hinge). The anterior humeral line passes anterior to the capitellum.
* Type III: Completely displaced with no cortical contact, characterized by severe soft tissue periosteal stripping.
* Type IV: A classification popularized by Leitch et al., describing a fracture with multidirectional instability (unstable in both flexion and extension) due to circumferential periosteal disruption. This is typically diagnosed intraoperatively.
The gold standard of treatment for displaced supracondylar fractures (Gartland Types II, III, and IV) is closed reduction and percutaneous pinning (CRPP). However, open reduction is an indispensable, albeit less frequently utilized, surgical intervention. Open reduction is strictly indicated when closed methods are inadequate, unsafe, or impossible due to severe displacement, interposition of critical soft tissues, concomitant neurovascular compromise, or the presence of an open fracture. Understanding the precise indications and executing the appropriate surgical approach is paramount for achieving anatomical osteosynthesis and preventing catastrophic complications.
Surgical Anatomy and Biomechanics
A profound mastery of the regional anatomy and biomechanics of the distal humerus is a prerequisite for safely navigating the surgical exposures required for open reduction. The supracondylar region represents a critical transitional zone where the robust, tubular diaphyseal bone flares and flattens into the medial and lateral columns of the metaphysis.
Osteology and Articular Anatomy
The distal humerus is architecturally defined by a triangular construct formed by the medial and lateral columns, which converge proximally at the supracondylar ridges and are joined distally by the articular block. The central region between the columns is remarkably thin, forming the coronoid fossa anteriorly and the olecranon fossa posteriorly. This "supracondylar thinness" is the primary anatomical stress riser responsible for the high incidence of fractures in this location. Distally, the medial column supports the trochlea (articulating with the greater sigmoid notch of the ulna), while the lateral column supports the capitellum (articulating with the radial head).
Neurovascular Anatomy
The neurovascular structures traversing the elbow joint are intimately associated with the distal humerus and are highly vulnerable to injury from initial fracture displacement, subsequent manipulation, or surgical dissection.
- Brachial Artery and Median Nerve: These critical structures course through the antecubital fossa, medial to the biceps brachii tendon and superficial to the brachialis muscle. In severe extension-type fractures, the sharp, proximal diaphyseal fragment is driven anteriorly and distally. It frequently "buttonholes" through the anterior periosteum, the brachialis muscle belly, and the anterior capsule, directly impaling or tenting the brachial artery and median nerve. The anterior interosseous nerve (AIN), a motor branch of the median nerve, is the most frequently injured neural structure in extension-type fractures.
- Ulnar Nerve: The ulnar nerve descends posterior to the medial intermuscular septum and passes through the cubital tunnel, directly posterior to the medial epicondyle. It is at significant risk during medial surgical approaches, during the placement of medial K-wires (especially if the elbow is hyperflexed, which subluxates the nerve anteriorly), and in flexion-type supracondylar fractures where the distal fragment displaces anteromedially.
- Radial Nerve: The radial nerve courses from the posterior compartment of the arm through the lateral intermuscular septum, descending anterior to the lateral epicondyle between the brachialis and brachioradialis muscles. It is susceptible to injury during lateral surgical approaches or from the initial trauma if the distal fragment displaces posteromedially, driving the proximal fragment laterally.
Musculoskeletal and Ligamentous Anatomy
The musculature crossing the elbow joint acts as a potent deforming force post-fracture and frequently acts as an impediment to closed reduction.
* Anterior Compartment: The brachialis muscle is the primary soft-tissue structure interposed in irreducible extension-type fractures. The biceps brachii and pronator teres also exert deforming forces.
* Posterior Compartment: The triceps brachii inserts onto the olecranon; its unopposed pull exacerbates the posterior displacement and extension deformity of the distal fragment.
* Medial and Lateral Compartments: The common flexor origin (medial epicondyle) and common extensor origin (lateral epicondyle) exert rotational and coronal plane forces on the distal articular fragment.
Biomechanics of Displacement
In the classic extension-type injury, the hyperextension moment creates a tension failure of the anterior cortex and a compression failure of the posterior cortex. The periosteum, which is thick in children, typically tears anteriorly but remains intact posteriorly in Type II fractures, acting as a hinge. In Type III fractures, the periosteum is circumferentially torn. The pull of the triceps displaces the distal fragment posteriorly and proximally. Concurrently, the forearm musculature often dictates the coronal and rotational displacement, typically resulting in posteromedial displacement and internal rotation of the distal fragment.
Indications and Contraindications
The threshold for transitioning from closed reduction to open reduction must be clearly defined. Open reduction is associated with higher risks of infection, stiffness, and iatrogenic neurovascular injury; therefore, it is reserved for scenarios where closed methods have definitively failed or are contraindicated.
Indications for Open Reduction
- Irreducible Fracture: The most frequent indication. Failure to achieve an acceptable anatomical reduction after 2 to 3 gentle, systematic closed attempts dictates open intervention. Irreducibility is almost universally caused by soft tissue interposition, most commonly the brachialis muscle, anterior capsule, or, critically, the median nerve or brachial artery.
- Vascular Compromise (The Ischemic Limb): A "white, pulseless hand" (exhibiting pallor, poikilothermia, paresthesia, paralysis, and pain out of proportion) before or after reduction is an absolute surgical emergency requiring immediate open exploration of the antecubital fossa to address brachial artery entrapment, intimal tear, or transection.
- Note on the "Pink, Pulseless Hand": If the hand is well-perfused (warm, brisk capillary refill) but lacks a palpable radial pulse post-reduction, the current standard of care supports close observation rather than immediate exploration, provided the reduction is anatomical. However, any deterioration in perfusion mandates immediate surgical exploration.
- Open Fractures: All open supracondylar fractures (Gustilo-Anderson Grades I-III) require formal surgical debridement, irrigation, and open reduction with internal fixation to mitigate the risk of osteomyelitis and ensure mechanical stability.
- Evolving Compartment Syndrome: Clinical signs of compartment syndrome in the forearm require emergent volar and dorsal fasciotomies. The fracture must be simultaneously openly reduced and stabilized to prevent further soft tissue trauma.
- Delayed Presentation: Fractures presenting beyond 7 to 14 days post-injury exhibit early callus formation, contracture of the soft tissue envelope, and significant hematoma organization. Closed reduction is typically impossible, necessitating a careful open approach to clear the fracture site and mobilize the fragments.
- Associated Neurological Deficit (Specific Scenarios): While most initial nerve palsies are neurapraxias that resolve spontaneously, an open approach is indicated if a nerve deficit develops after a reduction attempt (suggesting iatrogenic entrapment) or in the setting of an open fracture.
Contraindications
- Absolute: Unstable polytrauma patients requiring life-saving interventions ("damage control" orthopedics may dictate temporary splinting or rapid external fixation rather than definitive open reduction).
- Relative: Active local soft tissue infection (cellulitis) over the planned surgical incision site. Severe medical comorbidities precluding general anesthesia.
Operative vs. Non-Operative Decision Matrix
| Clinical Parameter | Indication for Open Reduction (Operative) | Indication for Closed Management (CRPP or Cast) |
|---|---|---|
| Fracture Reducibility | Irreducible after 2-3 closed attempts; soft tissue interposition. | Gartland I (Cast); Gartland II, III, IV successfully reduced closed. |
| Vascular Status | White, pulseless, ischemic hand; loss of perfusion post-reduction. | Intact pulses; Pink, pulseless hand with robust capillary refill post-reduction. |
| Neurological Status | New onset deficit post-reduction (suspected entrapment). | Deficit present pre-reduction (typically neurapraxia, observe). |
| Soft Tissue Envelope | Open fractures (Gustilo I-III); impending compartment syndrome. | Closed fracture; soft compartments without severe skin tenting. |
| Timing | Delayed presentation (>7-14 days) with organized callus. | Acute presentation (<7 days). |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning minimizes intraoperative delays and reduces the risk of iatrogenic complications.
Clinical and Radiographic Assessment
- Neurovascular Mapping: A meticulous, documented neurovascular examination is the most critical pre-operative step. Assess the median nerve (AIN branch: OK sign; flexor pollicis longus and flexor digitorum profundus to the index finger), radial nerve (wrist/finger extension), and ulnar nerve (finger abduction/adduction). Document baseline vascular status (radial/ulnar pulses, capillary refill, Doppler signals if necessary).
- Radiographic Parameters: High-quality AP and true lateral radiographs are mandatory.
- Lateral View: Assess the Anterior Humeral Line (AHL). In a normal elbow, the AHL should intersect the middle third of the capitellum. Assess the "teardrop" (formed by the anterior coronoid fossa and posterior olecranon fossa); disruption indicates severe rotation or structural collapse.
- AP View: Measure Baumann's Angle (the angle between the longitudinal axis of the humeral shaft and a line drawn along the physeal line of the lateral condyle). Normal is typically 70-75 degrees. Alteration indicates coronal plane malalignment (varus/valgus).
- Advanced Imaging: CT scanning is rarely indicated for acute pediatric supracondylar fractures but is highly valuable for adult fractures, highly comminuted patterns, or evaluating complex non-unions/malunions prior to corrective osteotomy.
Patient Positioning and Setup
- Anesthesia: General anesthesia with endotracheal intubation is standard.
- Positioning: The patient is placed supine. Two primary arm positions are utilized based on surgeon preference and planned approach:
- Hand Table: The arm is extended onto a radiolucent hand table. This is excellent for anterior or lateral approaches and allows easy C-arm access.
- Chest Drape (Arm over chest): The arm is brought across the patient's chest. This is highly effective for lateral and medial approaches, allowing the surgeon to work without fighting gravity, and permits rapid, unimpeded C-arm imaging by simply rotating the C-arm over the chest.
- Tourniquet: A non-sterile tourniquet is applied high on the brachium. Exsanguination with an Esmarch bandage is performed prior to inflation. If a posterior approach is planned, a sterile tourniquet may be applied after draping to maximize the surgical field.
- Fluoroscopy: The C-arm must be positioned to allow seamless transition between AP and lateral views without compromising the sterile field.
Detailed Surgical Approach and Technique
The selection of the surgical approach is dictated by the direction of displacement, the structures requiring exploration, and the specific column requiring direct visualization.
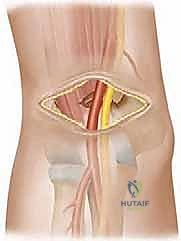
1. Anterior Approach (Modified Henry or Brachialis Split)
The anterior approach is the gold standard when vascular exploration is mandated (the ischemic limb) or when the proximal fragment has buttonholed through the brachialis, entrapping the neurovascular bundle.
- Incision: A curvilinear or S-shaped incision across the antecubital fossa, extending proximally along the medial border of the biceps and distally over the brachioradialis.
- Internervous Plane: The classic Henry approach utilizes the plane between the brachioradialis (radial nerve) and the pronator teres (median nerve). Alternatively, a direct, longitudinal split of the brachialis muscle belly can be performed, navigating between its dual innervation (musculocutaneous nerve medially, radial nerve laterally).
- Deep Dissection:
- Identify and protect the medial antebrachial cutaneous nerve.
- Locate the brachial artery and median nerve. In severely displaced fractures, these structures may be draped over the sharp metaphyseal spike of the proximal fragment.
- Utilize vessel loops for gentle retraction. If the artery is thrombosed or transected, vascular surgery consultation is immediately required for thrombectomy, primary anastomosis, or reverse saphenous vein grafting.
- Extract the proximal fragment from the brachialis muscle belly.
- Reduction: With the neurovascular bundle protected, the fracture is easily visualized. Gentle longitudinal traction and direct manipulation allow for anatomical reduction.
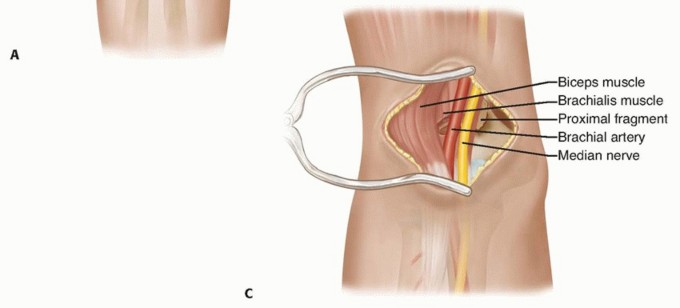
Figure: Anterior approach demonstrating the critical relationship of the brachial artery and median nerve draped over the anteriorly displaced proximal fracture fragment.
2. Lateral Approach
The lateral approach is highly versatile, carrying a lower risk of catastrophic neurovascular injury compared to the anterior or medial approaches. It is excellent for irreducible extension-type fractures with lateral column comminution.
- Incision: A longitudinal incision centered over the lateral epicondyle, extending proximally along the lateral supracondylar ridge.
- Dissection:
- Incise the fascia. The approach can be developed by elevating the brachioradialis and extensor carpi radialis longus (ECRL) anteriorly and the triceps posteriorly.
- The radial nerve must be respected. It crosses the lateral intermuscular septum approximately 10 cm proximal to the radiocapitellar joint. Dissection must remain subperiosteal to avoid injuring the nerve as it courses anteriorly.
- Clear the fracture hematoma and identify the interposing periosteum or muscle.
- Reduction and Fixation: Direct manipulation of the lateral column ensures rotational and sagittal alignment. Fixation is typically achieved with lateral divergent K-wires.
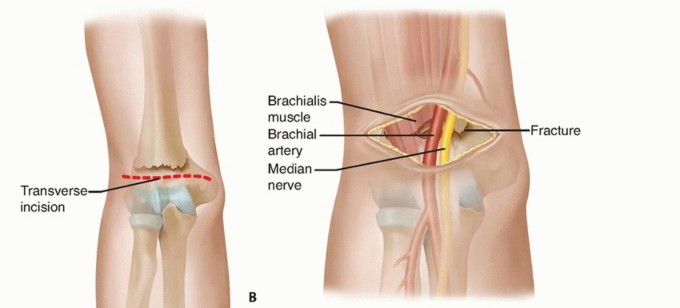
Figure: Lateral surgical approach illustrating direct visualization of the lateral column and subsequent stabilization with lateral divergent K-wires, minimizing ulnar nerve risk.
3. Medial Approach
Indicated primarily for medial column comminution, ulnar nerve exploration/decompression, or when a medial pin is strictly required for biomechanical stability but closed placement is deemed too high-risk.
- Incision: Longitudinal incision over the medial epicondyle.
- Dissection:
- The primary objective is the identification and protection of the ulnar nerve within the cubital tunnel.
- The nerve is isolated with a vessel loop. Depending on the extent of dissection required, it may be left in situ or mobilized for anterior transposition.
- The common flexor origin is elevated or split to expose the medial column.
- Fixation: Allows for direct, visually confirmed placement of a medial K-wire, completely eliminating the risk of iatrogenic ulnar nerve impalement.
4. Posterior Approach (Olecranon Osteotomy or Triceps-Sparing)
Reserved for complex, highly comminuted adult supracondylar/intercondylar fractures, or severe pediatric non-unions requiring extensive reconstructive osteosynthesis.
- Incision: A midline posterior incision curving slightly around the olecranon tip.
- Dissection (Olecranon Osteotomy):
- The ulnar nerve is definitively identified, neurolysed, and protected.
- A chevron-shaped osteotomy of the olecranon is performed (apex distal) to increase surface area for later repair and enhance rotational stability.
- The triceps-olecranon complex is reflected proximally, granting unparalleled 360-degree visualization of the distal humeral articular block and both columns.
- Reduction and Fixation: Allows for precise articular reduction and application of orthogonal or parallel dual-plate constructs. The osteotomy is subsequently repaired with tension band wiring or a dedicated olecranon plate.

Figure: Posterior approach utilizing an olecranon osteotomy. This provides maximum exposure of the articular surface and facilitates dual-plate osteosynthesis for complex adult distal humerus fractures.
Principles of Osteosynthesis
- Pediatric K-wire Fixation: The goal is maximum biomechanical stability with minimal iatrogenic risk.
- Lateral Divergent Pinning: Two or three 1.6 mm or 2.0 mm K-wires inserted from the lateral epicondyle, engaging the medial cortex of the proximal fragment. The pins should be maximally separated at the fracture site to optimize torsional stability. This is the preferred configuration as it avoids the ulnar nerve.
- Crossed Pinning (Medial and Lateral): Biomechanically superior in torsional rigidity but carries a well-documented risk of ulnar nerve injury (up to 4%). If a medial pin is used, it should be placed via a mini-open technique to directly protect the nerve.
- Adult Plate Fixation: Requires rigid, anatomical fixation to allow for immediate early active motion. Dual plating (medial and lateral columns) using pre-contoured anatomical locking plates is the standard of care.
Complications and Management
Open reduction, by virtue of the extensive soft tissue dissection required, inherently carries a higher complication profile than closed methods.
Specific Complications
| Complication | Pathophysiology & Incidence | Clinical Management & Salvage Strategies |
|---|---|---|
| Neurological Injury | Pre-injury: AIN (extension type), Ulnar (flexion type). Incidence: 10-20%. Iatrogenic: Ulnar nerve via medial pinning. Incidence: 1-4%. |
Pre-existing: Mostly neurapraxia. Observe for 3-4 months. Baseline EMG/NCS at 6 weeks if no clinical improvement. Iatrogenic: If recognized post-op, immediate surgical exploration, pin removal, and nerve decompression/repair are mandatory. |
| Vascular Injury & Volkmann's Ischemia | Brachial artery entrapment/laceration. Incidence: <1%. Unrecognized ischemia leads to irreversible muscle necrosis and Volkmann's ischemic contracture. | Immediate exploration for white, pulseless limbs. Fasciotomy for impending compartment syndrome. Volkmann's contracture is a devastating end-stage complication requiring complex salvage (muscle slides, tendon transfers, free functioning muscle transfers). |
| Malunion (Cubitus Varus) | "Gunstock Deformity." Incidence: 5-10%. Caused by failure to correct coronal plane rotation and medial column collapse. The distal humerus does not remodel rotational or coronal deformities. | Primarily a cosmetic deformity, but can cause tardy ulnar nerve palsy or posterolateral rotatory instability (PLRI) long-term. Corrected via a lateral closing-wedge or dome supracondylar osteotomy. |
| Stiffness / Arthrofibrosis | Higher incidence following open reduction due to capsular scarring and prolonged immobilization. | Aggressive, early active and active-assisted ROM. Avoid aggressive passive stretching (risk of heterotopic ossification). Surgical contracture release (arthrolysis) for refractory cases >6-12 months post-op. |
| Infection | Superficial or deep surgical site infection, or pin-tract infection. Incidence: 1-5%. | Pin-tract: Oral antibiotics, local care. Deep infection: Emergent surgical irrigation and debridement. Hardware is retained if stable until fracture union is achieved, then removed. |
| Nonunion | Exceedingly rare in pediatric populations (<0.1%). More common in adults with severe comminution. | Requires revision open reduction, autologous bone grafting (iliac crest), and rigid internal fixation (locking plates). |
Post Operative Rehabilitation Protocols
The rehabilitation paradigm must balance the need for fracture stability with the imperative to restore functional elbow range of motion.
Phase 1: Immobilization and Protection (Weeks 0-3/4)
- Immobilization: The arm is placed in a well-padded posterior long-arm splint or bivalved cast. The elbow is immobilized in approximately 60 to 80 degrees of flexion with the forearm in neutral rotation. Extreme flexion (>90 degrees) is avoided to prevent vascular compromise and excessive swelling.
- Monitoring: Strict neurovascular checks every 2-4 hours for the first 24-48 hours.
- Pin Care: If K-wires are left protruding, meticulous daily pin site care with chlorhexidine or saline is instituted to prevent superficial tract infections.
- Adjacent Joints: Immediate active ROM of the shoulder, wrist, and digits is encouraged to prevent dependent edema and distal stiffness.
Phase 2: Hardware Removal and Early Motion (Weeks 3-6)
- K-wire Removal: In pediatric patients, K-wires are typically removed in the outpatient clinic at 3 to 4 weeks post-operatively, contingent upon radiographic evidence of early bridging callus and clinical stability (absence of tenderness at the fracture site).
- Mobilization: Once pins are removed, the splint is discontinued, and formal physical therapy is initiated.
- ROM Exercises: Focus strictly on Active and Active-Assisted Range of Motion (AROM/AAROM).
- Critical Rule: Passive, forceful manipulation by therapists or parents is strictly contraindicated. It induces microtrauma, exacerbates inflammatory cascades, increases stiffness, and significantly elevates the risk of heterotopic ossification (myositis ossificans).
Phase 3: Strengthening and Functional Return (Weeks 6-12+)
- Strengthening: Progressive isometric and isotonic strengthening of the biceps, triceps, and forearm musculature begins once full, pain-free ROM is achieved (typically around week 6-8).
- Return to Play: Release to full, unrestricted activities, including contact sports and playground activities, is generally permitted between 10 to 12 weeks, provided there is radiographic union and symmetrical strength and ROM compared to the contralateral extremity.
- Adult Plate Fixation: In adults treated with rigid dual plating, early active motion is initiated within 3-5 days post-operatively to prevent catastrophic arthrofibrosis. Load-bearing is restricted until radiographic union is confirmed (usually 8-12 weeks).
Summary of Key Guidelines
The academic and clinical consensus regarding supracondylar humerus fractures is heavily guided by seminal literature and orthopedic societal guidelines (e.g., AAOS, POSNA).
- The Supremacy of CRPP: The paradigm shift formalized by Gartland (1959) and subsequently refined by modern techniques has established Closed Reduction and Percutaneous Pinning as the undisputed gold standard for displaced pediatric fractures. Open reduction is a salvage procedure, not a primary choice for standard Type II or III fractures.
- Pinning Configurations: Biomechanical studies, notably by Zionts et al. and clinical reviews by Skaggs et al., have demonstrated that two or three widely spaced, laterally divergent K-wires provide sufficient stability for the vast majority of fractures while completely eliminating the risk of iatrogenic ulnar nerve injury associated with crossed-pin constructs. Crossed pins are reserved for highly unstable medial columns where lateral pins fail to achieve purchase.
- The Vascular Algorithm: The management of the pulseless limb is heavily debated. The consensus, supported by Choi et al. and AAOS guidelines, dictates that a "pink, pulseless hand" post-anatomical reduction can be observed closely. However, a "white, pulseless hand" at any stage is an absolute indication for emergent anterior open exploration.
- Soft Tissue Interposition: Flynn et al. highlighted that irreducibility is almost exclusively a soft-tissue phenomenon. The brachialis muscle and the median nerve/brachial artery bundle are the most common culprits requiring an anterior or lateral open approach for extraction.
- Adult Distal Humerus Reconstructions: For adult supracondylar/intercondylar fractures, the principles established by the AO Foundation and authors like O'Driscoll mandate an olecranon osteotomy for exposure and rigid dual-plate osteosynthesis (orthogonal or parallel configurations) to permit immediate early active motion.
Clinical and Radiographic Imaging
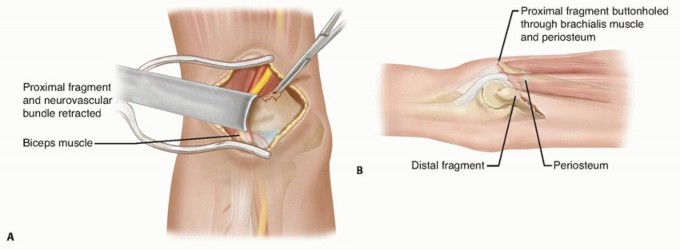
Figure: Post-operative clinical and radiographic correlation demonstrating restored alignment and healed surgical incisions following complex open reduction.
You Might Also Like


