Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures

Introduction and Epidemiology
The distal ulna represents the critical fixed point around which the radius and the hand function. Historically, fractures of the distal ulna have been inadequately treated or entirely neglected in comparison to their larger counterpart, the radius. The distal radius routinely attracts immediate attention and aggressive surgical treatment efforts, while ulnar-sided pathology is frequently relegated to an afterthought. However, the outcomes following distal forearm fractures can be significantly improved if the fixed point—the distal ulna—is addressed surgically with the same precision and urgency as the radius.
Recent orthopedic literature has devoted increased attention to the treatment, biomechanics, and outcomes of distal ulnar fractures and their associated ligamentous injuries. The epidemiology of these fractures typically follows a bimodal distribution. High-energy trauma, such as motor vehicle collisions or sports-related injuries, predominantly affects younger male populations, often resulting in complex, comminuted, or open fractures. Conversely, low-energy trauma, specifically falls from a standing height, primarily affects the elderly female population with underlying osteopenia or osteoporosis.

Isolated ulnar shaft and distal ulnar fractures most commonly occur when the forearm is struck directly by an object, explaining the classic eponym "nightstick fracture." However, distal ulnar fractures involving the metaphysis, ulnar head, or styloid are most often due to a fall on an outstretched hand. It is a well-established biomechanical understanding that ulnar-sided injuries are more frequently caused by backward falls in which the forearm is loaded in forced supination. This specific vector loads the ulnar side of the distal forearm and wrist, resulting in distal ulnar fractures, triquetral chip fractures, and triangular fibrocartilage complex injuries. In contrast, radial-sided injuries are more often caused by forward falls, loading the radial side of the forearm in pronation and causing scaphoid fractures and distal radius fractures.

Many distal ulnar fractures, particularly those that are non-displaced, leave only marginal long-term problems. However, displaced distal ulnar malunions consistently cause distal radioulnar joint incongruency, leading to subsequent chronic instability, blocked forearm rotation, and early-onset post-traumatic arthrosis. This natural history underscores exactly why the meticulous surgical management of these deceptive fractures is paramount for restoring upper extremity kinematics.

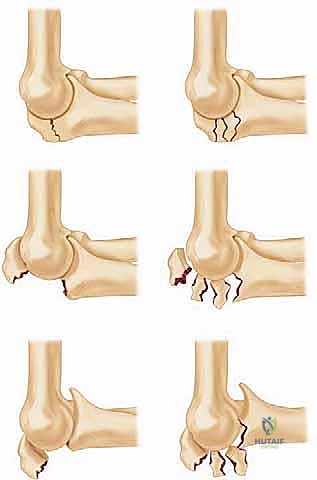
The classification of distal ulnar fractures relies heavily on the AO/OTA alphanumeric system, specifically designated as segment 2U3. Fractures are further subdivided based on their extra-articular or intra-articular nature, with specific attention paid to the involvement of the ulnar styloid, the ulnar head (articular surface), and the metaphyseal neck. Biyani and colleagues also proposed a highly useful clinical classification system that categorizes these injuries into simple styloid fractures, metaphyseal neck fractures, and complex intra-articular head fractures, which directly guides the algorithmic approach to internal fixation.

As life expectancy increases and the population remains active later in life, the incidence of distal forearm fractures is projected to rise exponentially. Consequently, orthopedic surgeons must possess a comprehensive understanding of the operative indications and advanced fixation techniques required to manage complex distal ulnar pathology. The paradigm has shifted from benign neglect to proactive stabilization, recognizing that the ulnar column is indispensable for grip strength, forearm rotation, and overall upper extremity function.

Surgical Anatomy and Biomechanics
Osteology of the Distal Ulna
The ulnar head forms the essential fixed pedestal on which the hand and radius rest. The radius rotates around the ulnar head through the distal radioulnar joint during dynamic forearm pronation and supination. The distal ulna comprises the metaphyseal neck, the articular head (seat), the ulnar styloid process, and the fovea. The fovea, located at the base of the ulnar styloid, serves as the critical insertion footprint for the deep limb of the radioulnar ligaments.

The stability of the distal radioulnar joint is achieved through a combination of bony congruity between the sigmoid notch of the distal radius and the ulnar head, heavily supported by the intrinsic and extrinsic radioulnar ligaments. The spheres of the two articular surfaces differ significantly in their radii of curvature, meaning the joint is not perfectly congruent. Approximately sixty percent of the joint surfaces are in contact during neutral rotation, and this contact area decreases significantly at the extremes of pronation and supination. This inherent osseous mismatch necessitates a robust soft-tissue envelope to prevent subluxation or dislocation during dynamic loading.

Ligamentous Stabilizers and the Triangular Fibrocartilage Complex
The Triangular Fibrocartilage Complex is the primary stabilizer of the distal radioulnar joint. It is a multi-component structure consisting of the articular disc, the dorsal and volar radioulnar ligaments, the meniscus homologue, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris tendon subsheath. The radioulnar ligaments are further divided into superficial and deep (ligamentum subcruentum) fibers. The deep fibers, which insert into the fovea of the ulnar head, are the true axis of rotation and the most critical components for maintaining distal radioulnar joint stability.

Avulsion fractures of the ulnar styloid base often involve the foveal attachment of the Triangular Fibrocartilage Complex, leading to profound distal radioulnar joint instability if left unaddressed. Conversely, tip fractures of the ulnar styloid typically only involve the superficial radioulnar ligaments and rarely result in clinically significant instability, provided the distal radius is anatomically reduced.

Secondary Stabilizers and Forearm Kinematics
Secondary stabilizers of the distal radioulnar joint include the pronator quadratus, the interosseous membrane (specifically the distal oblique bundle), and the extensor carpi ulnaris tendon. The extensor carpi ulnaris tendon rests within the sixth dorsal compartment, securely anchored to the ulnar head by its subsheath. During forearm rotation, the extensor carpi ulnaris acts as a dynamic stabilizer; its subsheath tension varies depending on the position of the forearm, providing a dorsal buttress against ulnar head subluxation during supination.

Biomechanically, the distal ulna is responsible for bearing approximately twenty percent of the axial load transmitted across the wrist joint in neutral ulnar variance. However, this load transmission is highly dynamic. In power grip or forced pronation, relative positive ulnar variance occurs, increasing the axial load on the ulnar head to up to forty percent. This phenomenon explains why malunions resulting in ulnar shortening or angulation drastically alter load mechanics, leading to ulnocarpal impaction syndrome and accelerated degenerative changes within the distal radioulnar joint.
The interosseous membrane plays a crucial role in longitudinal forearm stability. Central band disruptions, commonly seen in Essex-Lopresti injuries, lead to proximal migration of the radius if the radial head is fractured or resected. In the context of distal ulnar fractures, the integrity of the distal oblique bundle of the interosseous membrane is critical. When the distal ulna is fractured, the normal tension of the interosseous membrane is lost, allowing for multi-planar instability of the ulnar shaft and head.

Indications and Contraindications
The decision-making process for the surgical management of distal ulnar fractures requires a comprehensive assessment of fracture morphology, distal radioulnar joint stability, and patient-specific factors. Unlike the distal radius, where operative parameters are rigidly defined by radiographic measurements (e.g., radial height, volar tilt), the indications for the distal ulna are heavily predicated on joint congruency and the presence of concomitant injuries.

Isolated, non-displaced fractures of the ulnar neck or shaft can often be managed non-operatively with a short period of immobilization followed by functional bracing. However, when displacement occurs, the deforming forces of the pronator quadratus and the extensor carpi ulnaris frequently lead to progressive angulation and shortening. Operative intervention is mandated when acceptable alignment cannot be maintained or when the fracture directly compromises the distal radioulnar joint.

Operative Versus Non Operative Management Parameters
The following table delineates the established academic guidelines for selecting between operative and non-operative management of distal ulnar fractures.
| Clinical/Radiographic Parameter | Operative Indication | Non-Operative Indication |
|---|---|---|
| Fracture Displacement | > 2 mm displacement or translation | < 2 mm displacement |
| Angulation | > 10 degrees in any plane | < 10 degrees, stable on serial imaging |
| Distal Radioulnar Joint | Incongruent, subluxated, or frankly dislocated | Congruent and stable throughout ROM |
| Ulnar Styloid Involvement | Base fracture with foveal disruption and DRUJ instability | Tip fracture or base fracture with stable DRUJ |
| Articular Incongruity | > 1 mm step-off in the ulnar head articular surface | No articular step-off |
| Concomitant Injuries | Associated displaced distal radius fracture (unstable DRUJ) | Isolated injury with stable kinematics |
| Open Fractures | All open fractures require surgical debridement/fixation | N/A |
Contraindications to Surgical Intervention
Absolute contraindications to open reduction and internal fixation of the distal ulna include active, untreated local or systemic infection and severe medical comorbidities that preclude the safe administration of anesthesia. Relative contraindications encompass severe osteopenia or osteoporosis where hardware purchase is deemed impossible, though modern locked plating systems have largely mitigated this concern.

Additionally, in low-demand, non-ambulatory elderly patients, the risks of surgical intervention may outweigh the biomechanical benefits. In these specific scenarios, malunion of the distal ulna may be tolerated, provided that severe pain or skin breakdown from bony prominence does not occur. Pre-existing advanced arthrosis of the distal radioulnar joint may also alter the surgical plan; rather than attempting complex articular reconstruction, primary salvage procedures such as a Darrach or Sauve-Kapandji procedure may be indicated in the acute setting.

Pre Operative Planning and Patient Positioning
Imaging and Templating
Meticulous pre-operative planning is the cornerstone of successful distal ulnar reconstruction. Standard imaging must include true posteroanterior, lateral, and oblique radiographs of the wrist and forearm. A true lateral radiograph is critical for assessing distal radioulnar joint congruency; the volar cortices of the pisiform and the scaphoid pole should be aligned. On a true lateral, the ulnar head should sit perfectly within the sigmoid notch.
In cases of intra-articular comminution or when distal radioulnar joint subluxation is suspected but not definitively visualized on plain films, a computed tomography scan is mandatory. Axial CT cuts through the distal radioulnar joint provide unparalleled visualization of the sigmoid notch, the ulnar head, and any interposed bony fragments that may block reduction. Three-dimensional CT reconstructions are highly beneficial for conceptualizing complex, multi-fragmentary ulnar head fractures and planning specific screw trajectories.

Magnetic resonance imaging is rarely indicated in the acute fracture setting unless there is a high clinical suspicion of an isolated, complete Triangular Fibrocartilage Complex tear without an associated bony avulsion, or if a concomitant carpal ligamentous injury (e.g., scapholunate interosseous ligament tear) is suspected.

Implant templating should be performed using digital templating software. The surgeon must select an implant that provides adequate purchase in the small, often osteoporotic distal fragment. Dedicated distal ulna hook plates, 2.0 mm or 2.4 mm locking compression plates, and tension band constructs should all be available in the operating room. Intramedullary devices, such as customized ulnar nails or headless compression screws, may be considered for transverse neck fractures, though their use is less common than plate osteosynthesis.

Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating table with the affected upper extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The arm is prepped and draped in a standard sterile fashion, ensuring exposure from the fingertips to the mid-humerus to allow for full assessment of forearm rotation and elbow kinematics.

Fluoroscopy is essential. The C-arm can be brought in parallel to the hand table or from the foot of the bed, depending on the surgeon's preference and the spatial constraints of the operating room. The monitor should be positioned directly across from the surgeon for optimal viewing without breaking the sterile field or ergonomic posture. Prior to incision, the tourniquet is inflated to the appropriate pressure (typically 250 mmHg or 100 mmHg above systolic blood pressure) following exsanguination with an Esmarch bandage.
Detailed Surgical Approach and Technique
Surgical Approach and Neurovascular Protection
The distal ulna is approached via a direct longitudinal or slightly curvilinear incision over the subcutaneous border of the ulna. The incision typically begins at the level of the ulnar styloid and extends proximally along the ulnar shaft for 5 to 8 centimeters, depending on the fracture's proximal extension.
The most critical anatomical hazard during this approach is the dorsal sensory branch of the ulnar nerve. This nerve branches from the main ulnar nerve approximately 5 to 8 centimeters proximal to the ulnar styloid, passing deep to the flexor carpi ulnaris tendon before piercing the deep fascia to become subcutaneous. It then travels distally and dorsally across the ulnar aspect of the wrist to provide sensation to the dorso-ulnar aspect of the hand and the ulnar one and a half digits.
Blunt dissection through the subcutaneous tissues is mandatory to identify and protect the dorsal sensory branch of the ulnar nerve. Once identified, the nerve should be gently mobilized and retracted with a vessel loop. Excessive traction must be avoided to prevent neurapraxia or the formation of a painful neuroma.

The deep fascial incision is made directly over the ulnar shaft, utilizing the internervous plane between the extensor carpi ulnaris (innervated by the posterior interosseous nerve) and the flexor carpi ulnaris (innervated by the ulnar nerve). The extensor carpi ulnaris tendon sheath is left intact whenever possible to maintain its role as a dynamic stabilizer of the distal radioulnar joint. Subperiosteal dissection is performed to expose the fracture site, taking care to preserve the soft tissue attachments to comminuted fragments to maintain their vascular supply.

Fracture Reduction Techniques
Anatomic reduction of the distal ulna is paramount. The reduction maneuver typically involves longitudinal traction combined with direct manipulation of the fracture fragments using dental picks, Freer elevators, or small pointed reduction forceps. In cases of metaphyseal comminution, restoring length and rotation is the primary objective. The intact radius (or the anatomically reconstructed radius, if concomitantly fractured) serves as a template for ulnar length.

Provisional fixation is achieved using 0.045-inch or 0.062-inch Kirschner wires. These wires can be placed percutaneously or through the open wound, directing them from the distal fragment into the proximal shaft. Fluoroscopic imaging in both posteroanterior and lateral planes is utilized to confirm the provisional reduction. Special attention must be paid to the congruency of the distal radioulnar joint; any residual subluxation suggests an imperfect reduction of the ulnar shaft or an unrecognized soft tissue interposition.

Implant Selection and Fixation Strategies
The choice of fixation construct is dictated by the fracture pattern and bone quality.
Distal Ulnar Metaphyseal and Neck Fractures:
For transverse, oblique, or comminuted fractures of the ulnar neck and distal shaft, plate osteosynthesis is the gold standard. A dedicated 2.0 mm or 2.4 mm distal ulna locking plate is applied to the tension surface (typically the volar-ulnar or direct ulnar aspect) of the bone. The plate must be contoured precisely to match the anatomical bow of the distal ulna to prevent secondary displacement during screw insertion.

In osteoporotic bone, locking screws are essential in the short distal fragment to prevent hardware pullout. A minimum of three bicortical screws (or their biomechanical equivalent in locking unicortical screws) should be placed in both the proximal and distal fragments.

Ulnar Head Fractures:
Intra-articular fractures of the ulnar head require meticulous articular reduction. Small articular fragments can be stabilized using headless compression screws (1.5 mm or 2.0 mm) buried beneath the cartilage surface. If the head is severely comminuted and not amenable to internal fixation, primary ulnar head arthroplasty may be considered in low-demand patients, though this is generally reserved as a salvage procedure rather than an acute intervention.

Ulnar Styloid Base Fractures:
When an ulnar styloid base fracture is accompanied by distal radioulnar joint instability, fixation is mandatory. This can be achieved using a tension band wiring technique, a dedicated styloid hook plate, or a solitary cannulated compression screw if the fragment is large enough. Tension band wiring utilizes two parallel longitudinal K-wires and a figure-of-eight
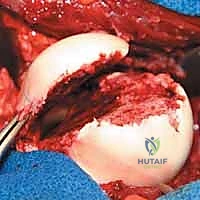
Clinical & Radiographic Imaging








You Might Also Like