Operative Orthopaedics: Comprehensive Surgical Anatomy and Biomechanics of the Wrist
Key Takeaway
A profound understanding of wrist surgical anatomy and biomechanics is the cornerstone of operative orthopedics. This comprehensive guide details the intricate osseous architecture, capsuloligamentous stabilizers, and vascular networks of the carpus. Designed for orthopedic residents and consultants, it explores the triangular fibrocartilage complex (TFCC), intrinsic and extrinsic ligaments, and kinematic principles essential for executing precise surgical approaches and optimizing patient outcomes in complex wrist disorders.
Comprehensive Introduction and Patho-Epidemiology
The human wrist represents an evolutionary marvel, an anatomically and biomechanically sophisticated transition zone interposing the robust lever arm of the forearm and the intricate, highly prehensile terminal effector organ—the hand. Engineered to provide an extraordinary dichotomy of multi-planar mobility and rigid structural stability, the wrist facilitates spatial positioning for fine motor tasks while simultaneously withstanding and transmitting massive axial and sheer forces during power grip. For the operative orthopedic surgeon, a profound, three-dimensional understanding of this region—encompassing the distal radioulnar joint (DRUJ), the radiocarpal joint, the ulnocarpal joint, and the complex intercarpal articulations—is not merely academic; it is an absolute prerequisite for successful surgical intervention.
The patho-epidemiology of wrist disorders reflects the vulnerability of this complex kinematic chain. Distal radius fractures remain the most ubiquitous orthopedic injury encountered in clinical practice, accounting for approximately one-sixth of all fractures evaluated in emergency departments. These injuries exhibit a bimodal distribution: high-energy trauma (such as motor vehicle collisions or falls from height) predominantly afflicting young, active males, and low-energy falls from a standing height affecting the burgeoning population of osteoporotic and osteopenic postmenopausal females. Concurrently, carpal fractures, particularly of the scaphoid, represent a significant burden of injury in the young athletic demographic, carrying a notoriously high risk of nonunion and avascular necrosis due to their tenuous retrograde vascular supply.
Beyond osseous trauma, the capsuloligamentous architecture of the wrist is frequently compromised, leading to devastating patterns of carpal instability. Scapholunate (SL) ligament tears, often dismissed initially as simple sprains, are the most common cause of carpal instability and, if left untreated, inexorably progress to Scapholunate Advanced Collapse (SLAC) arthritis. Similarly, high-energy hyperextension injuries can initiate the classic perilunate cascade, resulting in catastrophic disruption of the midcarpal joint. The economic and psychosocial burden of these injuries is staggering, often resulting in prolonged absences from the workforce and permanent disability if anatomic restoration and kinematic balance are not meticulously achieved.
This masterclass synthesizes the foundational anatomical, biomechanical, and kinematic principles of the wrist. It bridges the critical gap between textbook anatomy and the practical, high-stakes realities of the operating theater. By detailing precise surgical approaches, ligamentous preservation techniques, and evidence-based postoperative protocols, this chapter serves as a definitive reference for mastering operative orthopaedics of the wrist.
Detailed Surgical Anatomy and Biomechanics
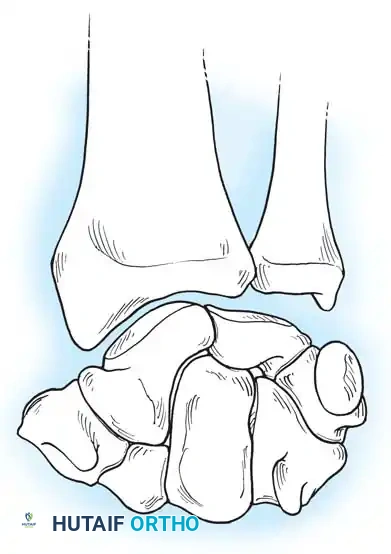
Osseous Architecture and Articulations
The osseous framework of the wrist comprises the distal radius, the distal ulna, and eight carpal bones arranged dynamically into two distinct rows. The distal radius presents a biconcave articular surface divided by a subtle sagittal ridge into the scaphoid and lunate fossae. The radial inclination averages 22 degrees, while the volar tilt averages 11 degrees; precise restoration of these parameters is the cornerstone of distal radius fracture fixation.
The proximal carpal row consists of the scaphoid, lunate, triquetrum, and pisiform. This row functions entirely as an intercalated segment. With the exception of the flexor carpi ulnaris inserting onto the pisiform (a sesamoid bone), the proximal row has no direct tendinous insertions. Consequently, its spatial orientation and movement are dictated entirely by the mechanical forces exerted by the surrounding articular contours and its robust ligamentous tethers.
The distal carpal row includes the trapezium, trapezoid, capitate, and hamate. In stark contrast to the proximal row, these bones are tightly bound to each other via stout interosseous ligaments and to the metacarpal bases, forming a rigid functional unit that moves synchronously with the hand. The capitate serves as the keystone of this arch, and its proximal head acts as the universal center of rotation for global wrist kinematics.
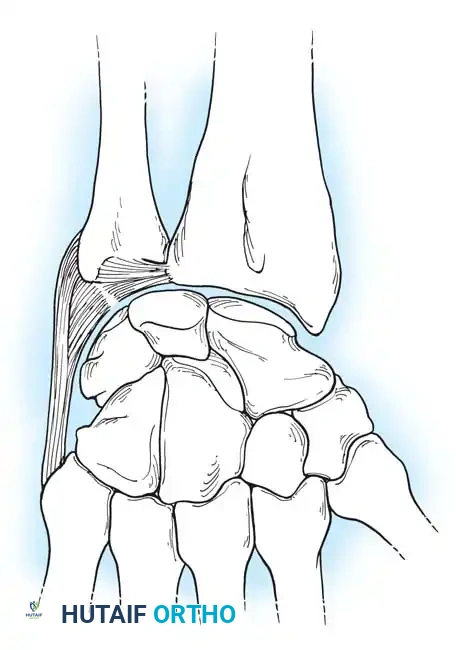
The radiocarpal joint is formed by the articulation of the distal radius with the convex proximal surfaces of the scaphoid and lunate. The triquetrum, importantly, does not articulate with the distal ulna; instead, it articulates proximally with the triangular fibrocartilage complex (TFCC). Viegas has emphasized the considerable anatomical variation found within the carpus, most notably the Type II lunate, present in up to 70% of individuals, which features an additional medial facet articulating with the proximal pole of the hamate. Recognizing this morphological variant is critical, as it alters normal wrist kinematics and predisposes patients to hamatolunate arthrosis, a frequent confounding factor in ulnar-sided wrist pain.
The Triangular Fibrocartilage Complex (TFCC)
The distal ulna articulates with the radius at the sigmoid notch, accommodating the ulnar head through approximately two-thirds of its rotational arc during pronosupination. The architecture of the sigmoid notch is highly variable, ranging from a deep "C" shape to a shallow, almost flat contour, which directly influences the inherent osseous stability of the DRUJ.
Separating the hyaline cartilage-covered ulnar head from the carpus is the TFCC, a critical chondroligamentous stabilizer first comprehensively described by Palmer and Werner. The TFCC is the primary stabilizer of the DRUJ and the ulnocarpal articulation, serving both as a ligamentous tether and a vital load-bearing shock absorber. Under normal neutral ulnar variance, the radius absorbs approximately 80% of the axial load across the wrist, while the ulna absorbs 20%. However, in states of ulnar positive variance (e.g., following a foreshortened distal radius fracture), the load transmitted through the ulnar column and TFCC increases exponentially, leading to ulnar impaction syndrome and degenerative TFCC tearing.
The TFCC is not a single structure but a multi-structural complex comprising several distinct components. The Articular Disc (TFC proper) is a biconcave fibrocartilaginous structure that absorbs axial loads; its central portion is avascular, precluding spontaneous healing of traumatic tears in this zone. The Dorsal and Volar Radioulnar Ligaments are the primary stabilizers of the DRUJ, with the deep (foveal) fibers providing the most critical isometric restraint during forearm rotation. The Meniscus Homologue is a reflection of fibrous tissue extending from the dorsal radius to the volar carpus. The complex is further reinforced by the Ulnar Collateral Ligament (UCL), the Extensor Carpi Ulnaris (ECU) Subsheath (which is intimately blended with the dorsal aspect of the TFCC), and the Ulnolunate and Ulnotriquetral Ligaments, which are volar extrinsic ligaments preventing volar subluxation of the ulnar carpus. When performing ulnar-sided surgical approaches or arthroscopy, extreme care must be taken to preserve the foveal attachments of the radioulnar ligaments; disruption here leads to profound DRUJ instability that cannot be salvaged merely by repairing the articular disc.
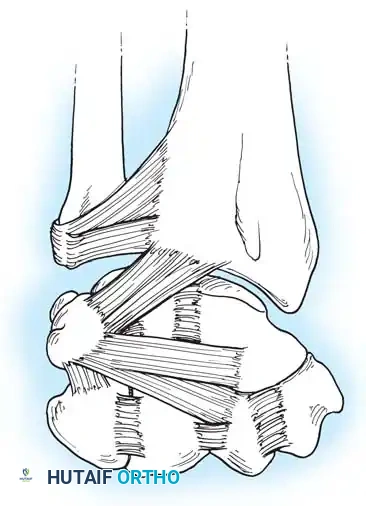
Capsuloligamentous Stabilizers
The stability of the carpus relies heavily on a complex, highly innervated network of intrinsic (interosseous) and extrinsic ligaments. The palmar (volar) ligaments are substantially thicker and mechanically stronger than their dorsal counterparts, reflecting the evolutionary need to resist the massive extension forces generated during a fall on an outstretched hand (FOOSH).
The palmar extrinsic ligaments connect the forearm to the carpus. The Radioscaphocapitate (RSC) Ligament acts as a vital sling supporting the scaphoid waist and must be meticulously repaired during volar approaches to prevent rotatory subluxation of the scaphoid. The Long Radiolunate (LRL) Ligament prevents ulnar translation of the lunate, while the Short Radiolunate (SRL) Ligament anchors the lunate to the lunate fossa. The Radioscapholunate (RSL) Ligament, historically known as the Ligament of Testut, is now understood to be primarily a neurovascular conduit rather than a true mechanical stabilizer. Crucially, the Space of Poirier is a distinct area of capsular weakness located on the palmar aspect of the midcarpal joint, between the RSC and the palmar radiolunotriquetral ligaments. It overlies the palmar surface of the lunate and represents the classic site of capsular failure and lunate extrusion in Stage IV perilunate dislocations.
The dorsal capsuloligamentous network, while thinner, is biomechanically vital for preventing dorsal intercalated segment instability (DISI) and guiding complex carpal kinematics. The Dorsal Radiocarpal (DRC) Ligament originates from the dorsal radial margin of the lunate fossa, spans the lunotriquetral joint, and inserts onto the dorsal triquetrum. Viegas and Mizuseki classified the DRC into distinct morphological types based on its thickness and insertion footprint.
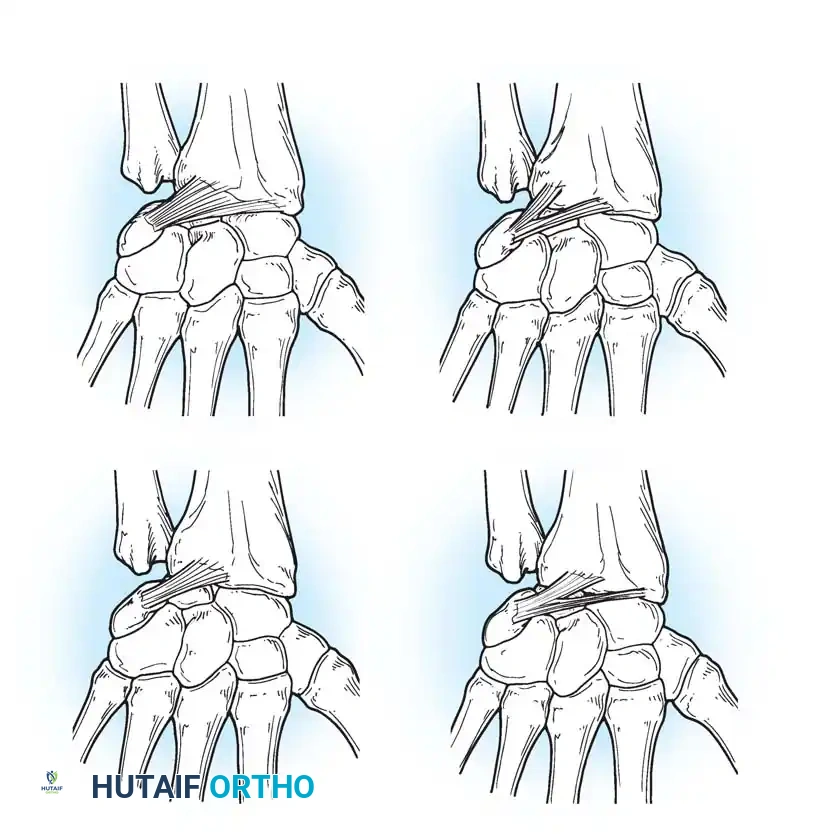
The Dorsal Intercarpal (DIC) Ligament originates from the dorsal triquetrum, courses transversely across the midcarpal joint, and inserts onto the dorsal scaphoid waist and trapezoid. Viegas verified distinct types of DIC ligaments, noting that its laminated structure allows it to change shape dynamically during wrist motion, accommodating the shifting geometry of the proximal row.
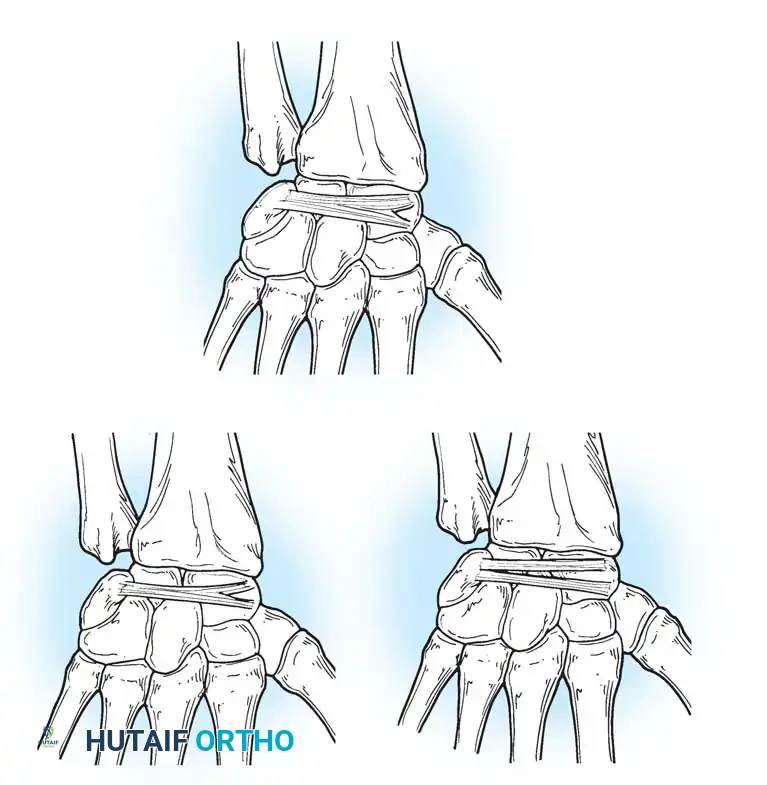
Together, the DRC and DIC form a lateral "V" shape that stabilizes the proximal row. This V-shaped configuration acts as a dynamic tension band, preventing dorsal subluxation of the carpus during wrist flexion and providing a critical checkrein against rotatory instability.
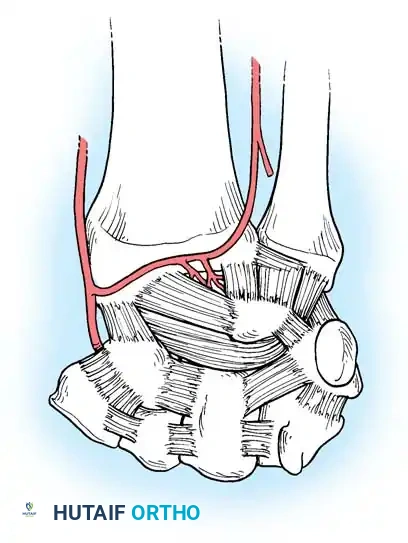
Vascular Anatomy of the Carpus
Understanding the extraosseous and intraosseous vascularity of the wrist is paramount, particularly when managing fractures of the scaphoid, lunate, and capitate, which are highly susceptible to avascular necrosis (AVN) and subsequent structural collapse. Gelberman et al. meticulously mapped the terminal branches of the radial, ulnar, and anterior interosseous arteries, demonstrating that they form three dorsal and three palmar transverse arterial arches.
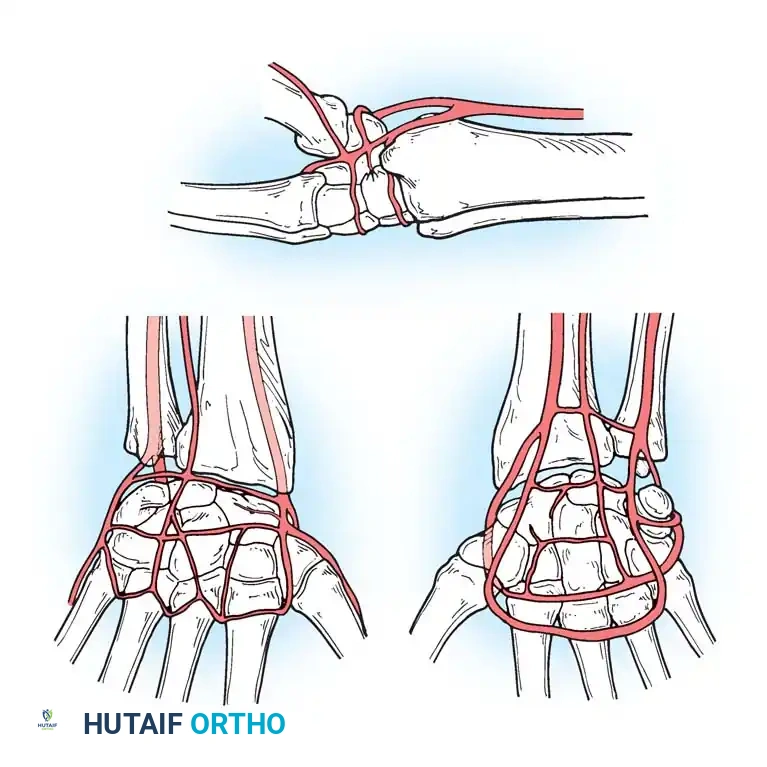
The Dorsal Arterial Arches comprise the Dorsal Radiocarpal Arch (supplying the proximal lunate and triquetrum), the Dorsal Intercarpal Arch (the largest arch, supplying the distal carpal row and providing critical anastomotic flow to the lunate and triquetrum), and the Basal Metacarpal Arch. The Palmar Arterial Arches include the Palmar Radiocarpal Arch, the highly variable Palmar Intercarpal Arch, and the deep Palmar Arch, which consistently communicates with the dorsal basal metacarpal arch.
The scaphoid represents a unique and perilous vascular watershed. It receives 70-80% of its blood supply from branches of the radial artery entering the dorsal ridge, which then perfuse the bone in a retrograde fashion toward the proximal pole. The remaining 20-30% enters volarly at the distal tubercle. Consequently, fractures at the scaphoid waist or proximal pole acutely disrupt this delicate retrograde supply, leading to notoriously high rates of nonunion and proximal pole AVN. Surgical approaches, particularly dorsal exposures for percutaneous or open screw fixation, must meticulously preserve the dorsal ridge vasculature to optimize the biological environment for osteosynthesis.
Biomechanics and Kinematics
The kinematics of the wrist are dictated entirely by the complex articular geometry and the tethering ligaments, operating without direct tendinous insertions on the proximal row. The center of rotation for global wrist motion—both flexion/extension and radial/ulnar deviation—is located within the proximal head of the capitate.
Most functional activities of daily living do not occur in pure orthogonal planes (i.e., pure flexion or pure deviation). Instead, they occur in an oblique plane known as the "dart-thrower's motion"—moving from radial extension to ulnar flexion. Biomechanical studies have demonstrated that this motion occurs primarily at the midcarpal joint, with minimal movement of the proximal carpal row (specifically the scaphoid and lunate). This physiological reality makes the dart-thrower's arc a safe and highly effective rehabilitation motion following scapholunate ligament repairs, allowing early functional movement without stressing the healing ligamentous reconstruction.
Carpal instability patterns are best understood through the lens of Mayfield, Johnson, and Kilcoyne, who described the progressive stages of perilunar instability resulting from tremendous forces of wrist hyperextension, ulnar deviation, and intercarpal supination. Stage I involves Scapholunate dissociation (SL ligament tear). If the force continues, Stage II results in capitate dislocation and disruption of the Space of Poirier. Stage III involves Lunotriquetral dissociation (LT ligament tear), effectively untethering the entire lunate. Finally, Stage IV culminates in a complete lunate dislocation, where the lunate is extruded volarly into the carpal tunnel, often causing acute median neuropathy and requiring emergent surgical reduction.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the wrist requires a nuanced synthesis of patient-specific factors, precise pathoanatomy, and a deep understanding of the natural history of the specific disorder. The following table delineates the rigorous indications and contraindications for common wrist pathologies encountered by the orthopedic surgeon.
| Pathology | Primary Surgical Indication | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Distal Radius Fracture | Volar tilt >15° dorsal, radial shortening >3mm, articular step-off >2mm, loss of radial inclination, unstable fracture patterns (e.g., volar shear/Barton's). | Active local soft tissue infection; medically unstable patient unfit for anesthesia. | Severe osteopenia/osteoporosis (may require augmented fixation); highly non-compliant patient; baseline profound dementia. |
| Scaphoid Fracture | Proximal pole fractures, displacement >1mm, intrascaphoid angle >35° (humpback deformity), delayed presentation or established non-union. | Active infection; advanced SLAC wrist arthrosis (salvage procedure indicated instead). | Tobacco abuse (significantly increases non-union risk); pediatric patients with non-displaced fractures (casting preferred). |
| Scapholunate (SL) Tear | Acute, repairable tears with dynamic or static widening (>3mm gap on clenched fist view); reducible carpal malalignment. | Established SLAC arthritis (requires salvage like PRC or 4-corner fusion); fixed, irreducible carpal deformity. | Chronic tears (>6 months) without arthritis (may require complex reconstruction rather than primary repair). |
| Perilunate Dislocation | All acute perilunate and lunate dislocations require emergent/urgent open reduction and internal fixation (ORIF) and ligamentous repair. | None in the acute setting, unless life-threatening polytrauma precludes extremity surgery. | Delayed presentation (>8 weeks) may necessitate proximal row carpectomy (PRC) or arthrodesis due to cartilage necrosis. |
| TFCC Tear (Peripheral) | Persistent ulnar-sided wrist pain >3-6 months failing conservative management; objective DRUJ instability. | Central avascular tears (require debridement, not repair); advanced ulnocarpal arthritis. | Ulnar positive variance without concurrent ulnar shortening osteotomy (USO) or wafer procedure. |
Pre-Operative Planning, Templating, and Patient Positioning
Flawless execution in the operating theater begins long before the incision is made. Pre-operative planning for wrist surgery demands high-quality, orthogonal radiographic imaging. Standard posteroanterior (PA), lateral, and oblique views are mandatory. The lateral view must be a true lateral, verified by the collinear alignment of the palmar cortices of the pisiform and the scaphoid pole; this view is critical for assessing volar tilt and identifying dorsal intercalated segment instability (DISI) or volar intercalated segment instability (VISI). Clenched fist PA views are utilized to dynamically stress the intercarpal ligaments, unmasking occult scapholunate widening (the "Terry Thomas" sign).
Advanced imaging is frequently required. High-resolution non-contrast MRI is the gold standard for evaluating the integrity of the TFCC, the SL and LT ligaments, and the vascular status of the scaphoid proximal pole. Computed Tomography (CT) with 3-dimensional reconstructions is indispensable for mapping complex intra-articular distal radius fractures, delineating die-punch fragments, and planning precise screw trajectories to avoid joint penetration.
Digital templating is a critical step, particularly for distal radius ORIF and corrective osteotomies. The surgeon must template the anticipated plate size, contour, and screw lengths, ensuring that distal locking screws will be situated subchondrally to support the articular surface without breaching the radiocarpal or DRUJ articulations.
Patient positioning is standardized but requires meticulous attention to detail. The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm, typically inflated to 250 mmHg or 100 mmHg above systolic pressure after exsanguination with an Esmarch bandage. The fluoroscopy unit (C-arm) is positioned either coming in from the foot of the hand table or horizontally across the table, depending on surgeon preference, ensuring unimpeded access for dynamic intraoperative imaging. The surgeon typically sits in the axilla, providing optimal ergonomic access to both the dorsal and volar aspects of the wrist.
Step-by-Step Surgical Approach and Fixation Technique
Mastery of wrist surgery requires strict adherence to internervous planes, meticulous soft tissue handling, and the preservation of critical capsuloligamentous structures to prevent iatrogenic instability.
The Dorsal Approach to the Wrist
The dorsal approach is the workhorse exposure for open reduction internal fixation (ORIF) of dorsal shear distal radius fractures, proximal row carpectomy (PRC), four-corner arthrodesis, total wrist arthrodesis, and dorsal ganglion excision.
Step-by-Step Surgical Technique:
1. Incision and Superficial Dissection: A longitudinal incision is made centered over the Lister tubercle, extending proximally over the distal radius and distally toward the base of the third metacarpal. Full-thickness fasciocutaneous flaps are elevated to protect the delicate dorsal sensory branches of the radial nerve (radial aspect) and the dorsal branch of the ulnar nerve (ulnar aspect).
2. Extensor Retinaculum and EPL Transposition: The extensor retinaculum is identified. The third extensor compartment is opened longitudinally, and the Extensor Pollicis Longus (EPL) tendon is mobilized and transposed radially. This protects the EPL from attrition rupture against dorsal hardware.
3. Subperiosteal Elevation: The second compartment (ECRL, ECRB) and the fourth compartment (EDC, EIP) are elevated subperiosteally off the distal radius. This exposes the dorsal radiocarpal joint capsule.
4. Capsulotomy (Berger's Flap): To preserve the critical DRC and DIC ligaments, a ligament-sparing capsulotomy is mandatory. The surgeon creates a distally based, V-shaped flap (Berger's flap) that splits the difference between the fibers of the DRC and DIC ligaments.
5. Deep Exposure and Fixation: The capsular flap is reflected distally, exposing the radiocarpal and midcarpal joints. For fracture fixation, dorsal spanning or fragment-specific plates are applied. For carpal procedures, the necessary resections or fusions are performed.
6. Closure: The capsular flap is meticulously repaired with non-absorbable braided sutures to restore dorsal stability and prevent postoperative DISI. The extensor retinaculum is repaired over the tendons, but the EPL is left transposed subcutaneously to prevent friction against the retinacular repair or underlying hardware.
The Volar (Henry) Approach to the Wrist
The volar approach is the standard for ORIF of volar displaced distal radius fractures, scaphoid waist fractures, perilunate dislocations, and volar marginal lip fractures.
Step-by-Step Surgical Technique:
1. Incision and Superficial Dissection: A longitudinal incision is made over the course of the Flexor Carpi Radialis (FCR) tendon. If extending into the palm, the incision must zig-zag across the wrist creases to prevent flexion contractures. The superficial fascia is incised. The surgeon must identify and protect the palmar cutaneous branch of the median nerve (PCBMN), which lies consistently ulnar to the FCR tendon.
2. Internervous Plane: The FCR tendon sheath is incised longitudinally. The FCR tendon is retracted ulnarly, which safely pulls the median nerve away from the surgical field. The radial artery is identified and gently retracted radially.
3. Deep Dissection and PQ Elevation: This exposes the deep fascial layer covering the Flexor Pollicis Longus (FPL) and the pronator quadratus (PQ) muscle. The PQ is incised along its radial and distal borders (the classic "L" incision) and elevated ulnarly as a full-thickness muscular flap to expose the volar surface of the distal radius.
4. Capsulotomy (If Indicated): If accessing the carpus (e.g., for scaphoid ORIF or perilunate reduction), a longitudinal or T-shaped volar capsulotomy is performed. The surgeon must take extreme care to tag and repair the strong volar extrinsic ligaments (RSC, LRL) upon closure to prevent catastrophic postoperative carpal instability.
5. Fixation: For distal radius fractures, a volar locking plate is applied proximal to the watershed line to prevent flexor tendon irritation. Subchondral locking screws are placed to support the articular surface.
6. Closure: The volar capsule is repaired if opened. The pronator quadratus is reapproximated to the radial border to cover the hardware and provide a dynamic soft-tissue interposition between the plate and the flexor tendons. The FCR sheath is left open to prevent postoperative tenosynovitis or stenosis.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications in wrist surgery can and do occur. The operative surgeon must be intimately familiar with the incidence, presentation, and salvage management of these adverse events.
| Complication | Estimated Incidence | Pathophysiology & Presentation | Salvage Management & Treatment |
|---|---|---|---|
| Extensor Pollicis Longus (EPL) Rupture | 1% - 5% (Post-distal radius fracture/ORIF) | Attrition rupture due to prominent dorsal screws penetrating the 3rd compartment, or ischemia from fracture hematoma. Presents as inability to retropulse the thumb. | Extensor Indicis Proprius (EIP) to EPL tendon transfer. Direct repair is rarely possible due to tendon retraction and degeneration. |
| Flexor Tendon Rupture (FPL most common) | 2% - 4% (With volar plating) | Iatrogenic injury from plate placement distal to the watershed line, causing friction during thumb flexion. | Hardware removal. Primary tendon repair if acute; staged reconstruction with silicone rod and tendon graft, or FDS transfer if chronic. |
| Complex Regional Pain Syndrome (CRPS) | 5% - 10% | Abnormal autonomic nervous system response post-trauma/surgery. Presents as severe burning pain, allodynia, swelling, and vasomotor skin changes. | Aggressive early therapy (desensitization), high-dose Vitamin C (prophylactic), Gabapentinoids, sympathetic nerve blocks. Avoid further surgery if possible. |
| Scaphoid Nonunion / AVN | 10% - 15% (Waist); up to 50% (Proximal pole) | Disruption of retrograde blood supply; inadequate rigid fixation; smoking. Presents as persistent radial-sided pain and radiographic sclerosis/cystic changes. | Vascularized bone grafting (e.g., 1,2 ICSRA graft or medial femoral condyle free flap) with rigid internal fixation. If advanced collapse (SLAC), proceed to PRC or 4-corner fusion. |
| Hardware Penetration into Joint | 3% - 7% | Unrecognized screw penetration into the radiocarpal or DRUJ joint during fixation, leading to rapid chondrolysis and arthritis. | Immediate hardware removal/exchange. Intraoperative use of dorsal tangential fluoroscopic views is critical to prevent this. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional success of any wrist surgery is inextricably linked to the execution of a rigorous, phased postoperative rehabilitation protocol. While specific timelines will inherently vary based on the procedure (e.g., rigid internal fixation allows earlier motion than soft-tissue ligamentous reconstruction), the overarching physiological principles remain constant.
Phase I (0-2 Weeks) - Protection and Edema Control:
Immediately postoperatively, the wrist is immobilized in a bulky, non-compressive dressing and a volar plaster splint to protect the surgical repair and manage the acute inflammatory phase. Digital range of motion (ROM) is initiated on postoperative day one; full composite flexion and extension of the fingers are mandatory to prevent flexor and extensor tendon adhesions and stiffness. Strict elevation above the level of the heart and compressive wraps (e.g., Coban) are utilized to aggressively manage edema, which is the primary enemy of early hand function.
Phase II (2-6 Weeks) - Early Protected Motion:
At the first postoperative visit, sutures are removed. For stable osseous fixations (e.g., a rigidly plated volar distal radius fracture), a custom thermoplastic splint is fabricated by a certified hand therapist. Active ROM exercises are initiated out of the splint. Crucially, the dart-thrower's motion (radial extension to ulnar flexion) is emphasized, as it maximizes functional midcarpal motion while minimizing stress on the proximal carpal row and healing radiocarpal ligaments. For ligament repairs (e.g., SL reconstruction) or unstable fracture patterns, rigid cast immobilization is maintained for a full 6 to 8 weeks to allow for adequate collagen cross-linking and tissue maturation.
**Phase III (6-
