Fingertip Amputation Reconstruction: An Intraoperative Masterclass in Soft Tissue Coverage
Key Takeaway
This masterclass guides fellows through advanced soft tissue coverage for fingertip amputations. We'll meticulously cover comprehensive surgical anatomy, critical preoperative planning, and real-time, step-by-step intraoperative execution of various flap and graft techniques. Learn to manage neurovascular risks, optimize patient outcomes, and navigate potential pitfalls with expert precision, ensuring functional and aesthetic restoration of the most sensitive area of the hand.
Introduction and Epidemiology
Fingertip amputations and associated soft tissue injuries represent the most frequently encountered upper extremity traumas evaluated in acute care and emergency settings, comprising approximately forty-five percent of all hand trauma. Anatomically, the fingertip is defined as the portion of the digit extending distal to the terminal insertion of the flexor and extensor tendons at the distal interphalangeal (DIP) joint. Serving as the primary organ of tactile gnosis, the fingertip is densely innervated and highly specialized to facilitate fine motor manipulation, pinch kinematics, and complex environmental interaction.
The pathogenesis of these traumatic injuries spans a broad spectrum of mechanisms, including sharp lacerations, high-energy crush injuries, avulsions, and localized compression trauma. The specific mechanism of injury directly dictates the macroscopic and microscopic zone of injury, the viability of the remaining soft tissue envelope, and the subsequent reconstructive algorithm. Industrial accidents, table saw injuries, and door crush mechanisms remain the most frequently reported etiologies, often presenting with concomitant osseous, neurovascular, and tendinous compromise.
Classification systems are indispensable for standardizing surgical communication, prognosticating outcomes, and guiding reconstructive options. The Tamai classification divides fingertip amputations into two distinct anatomical zones:
* Zone I: Injuries occurring distal to the lunula.
* Zone II: Injuries occurring between the distal interphalangeal joint and the lunula.
Alternatively, the Allen classification categorizes injuries based on the precise level of tissue loss:
* Type I: Involving only the volar pulp.
* Type II: Involving the nail bed and pulp, preserving the distal phalanx.
* Type III: Involving the distal phalanx and nail bed.
* Type IV: Amputation proximal to the lunula with significant distal phalanx loss.
Regardless of the classification system utilized, the overarching goals of surgical management remain consistent: preservation of functional digital length, restoration of durable and sensate soft tissue coverage, prevention of debilitating neuromas, and maintenance of interphalangeal joint mobility.
Surgical Anatomy and Biomechanics
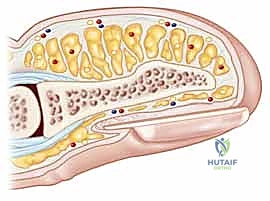
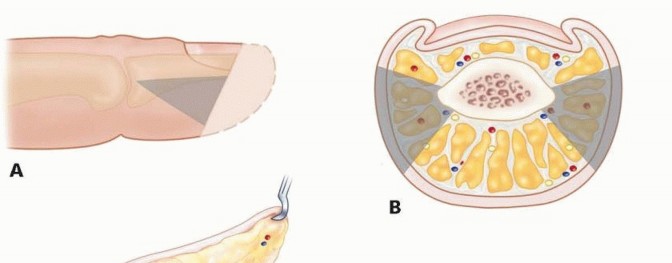
A profound understanding of fingertip anatomy is paramount for executing local flap coverage, preserving vascularity, and minimizing iatrogenic morbidity. The fingertip is a complex composite structure comprising the distal phalanx, the perionychium, the volar pulp, and a highly specialized neurovascular network.
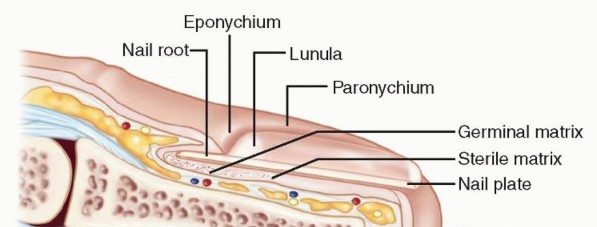
The Nail Complex
The perionychium consists of the nail bed and the surrounding paronychia. The nail bed is further subdivided into the germinal matrix (proximal) and the sterile matrix (distal). The germinal matrix is responsible for approximately ninety percent of nail plate generation, while the sterile matrix provides adherence and the remaining ten percent of vertical growth. The eponychium is the proximal skin fold overlying the nail root, and the hyponychium is the specialized keratinized tissue distal to the nail bed that acts as an immunological and physical barrier against subungual infection.

The bony tuft of the distal phalanx must adequately support the nail bed; loss of this critical osseous support leads to a predictable downward curvature of the nail plate, clinically recognized as a hook nail deformity.
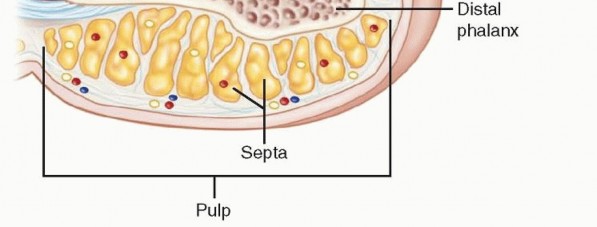
Volar Pulp Architecture
The volar pulp is uniquely designed to withstand compressive, tensile, and shear forces during pinch and grasp kinematics. It consists of dense adipose tissue compartmentalized by robust fibrous septa that anchor the volar dermis to the periosteum of the distal phalanx.

These septa prevent skin displacement during pinch maneuvers but simultaneously create closed anatomical compartments. While biomechanically advantageous, these closed spaces can rapidly sequester infection (felon) or hematoma, leading to localized microvascular compromise and subsequent tissue necrosis if not promptly decompressed.
Neurovascular Supply
Arterial inflow is provided by the proper palmar digital arteries, which bifurcate near the distal interphalangeal joint to form an arborizing anastomotic arcade within the pulp. Venous drainage is predominantly dorsal, relying on a delicate, low-pressure network of superficial veins.
Innervation is supplied by the proper palmar digital nerves, which divide into multiple terminal branches distal to the DIP joint. This dense arborization provides the fingertip with its exquisite static and moving two-point discrimination (normally 2-4 mm). High concentrations of specialized mechanoreceptors, including Pacinian corpuscles (mediating high-frequency vibration) and Meissner corpuscles (mediating light touch and low-frequency vibration), are embedded within the volar dermis.
Indications and Contraindications
The decision-making process for soft tissue coverage of fingertip amputations depends on multiple variables: the absolute size of the defect, the geometric plane of the amputation (transverse, volar oblique, dorsal oblique), the presence of exposed bone or tendon, and patient-specific factors such as age, handedness, occupational demands, and medical comorbidities (e.g., diabetes, peripheral vascular disease, smoking status).

Healing by secondary intention is an excellent, conservative option for superficial defects measuring less than 1.0 cm² without exposed bone or tendon. This method relies on wound contracture and epithelialization, often resulting in superior sensory recovery and minimal cold intolerance compared to complex flap coverage. However, when bone is exposed, or the defect exceeds 1.0 cm², surgical intervention is mandated to prevent osteitis, osteomyelitis, painful adherent scarring, and functional impairment.
| Clinical Scenario | Recommended Management Strategy | Contraindications & Considerations |
|---|---|---|
| Defect < 1 cm², no exposed bone | Healing by Secondary Intention | Exposed bone, exposed tendon, large defect size |
| Transverse or Dorsal Oblique, exposed bone | V-Y Advancement Flap (Atasoy) | Volar oblique defects, extensive volar pulp loss |
| Transverse or Lateral Oblique, exposed bone | Bilateral V-Y Flap (Kutler) | Volar oblique defects, risk of hyperesthetic midline scar |
| Volar Oblique defect, exposed bone | Cross-Finger Flap | Stiff joints, advanced age, rheumatoid arthritis, uncooperative patient |
| Distal Volar defect (Index/Middle) | Thenar Flap | Older patients (high risk of PIP joint flexion contracture) |
| Thumb Volar defect (< 1.5 - 2.0 cm) | Moberg Volar Advancement Flap | Use in lesser digits (high risk of dorsal skin necrosis) |
| Extensive tissue loss, unsalvageable | Revision Amputation / Shortening | When functional length is critical for specific occupational needs |
Pre Operative Planning and Patient Positioning
Comprehensive preoperative evaluation begins with a meticulous history and physical examination. The surgeon must document the exact mechanism of injury. Crush and avulsion injuries typically exhibit a wider zone of trauma than sharp lacerations; utilizing marginal tissue in these high-energy injuries frequently leads to delayed flap necrosis. Handedness, occupation, and the patient's capacity for postoperative compliance are critical variables in selecting the appropriate reconstructive ladder.

Physical examination must precisely quantify the involved digits, the geometry of the amputation (transverse, volar oblique, dorsal oblique, or radial/ulnar oblique), and the integrity of the nail complex. Vascular status is assessed via capillary refill time and skin turgor; prolonged refill suggests proximal arterial injury, vasospasm, or severe crush. Neurologic assessment includes static and moving two-point discrimination in the adjacent uninjured digits to establish a baseline for postoperative comparison.

Standard orthogonal plain radiographs (posteroanterior, lateral, and oblique views) of the affected digit are mandatory. These images are utilized to assess the remaining osseous architecture, evaluate for the presence of radiopaque foreign bodies, and identify associated phalangeal fractures that may require concurrent stabilization.
Surgical procedures are typically performed in the supine position with the affected extremity extended on a radiolucent hand table. The use of a digital tourniquet (e.g., a sterile glove finger or commercial digital tourniquet) or a forearm tourniquet is essential to maintain a bloodless surgical field, facilitating precise identification of neurovascular structures under loupe magnification. Anesthesia is most commonly achieved via a digital block using a long-acting local anesthetic (e.g., bupivacaine). While traditionally taught to avoid epinephrine in the digits, the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique utilizing lidocaine with epinephrine (1:100,000) is now widely accepted and frequently utilized, provided phentolamine is available for reversal if necessary. For more complex, multi-stage regional flaps (cross-finger, thenar), a regional block or monitored anesthesia care (MAC) may be preferred.
Detailed Surgical Approach and Technique
Wound Preparation and Debridement
Regardless of the chosen reconstructive technique, meticulous surgical debridement is the foundational step. The wound must be irrigated copiously with sterile normal saline to decrease bacterial bioburden. Devitalized soft tissue, contaminated bone fragments, and non-viable nail matrix must be sharply excised back to healthy, bleeding margins.


If the distal phalanx is exposed and prominent, it should be conservatively trimmed back with a rongeur or bone cutter until healthy, bleeding cortical or cancellous bone is encountered. However, extreme caution is advised: conservative bone resection is paramount to maintain structural support for the nail bed and prevent subsequent hook nail deformity.
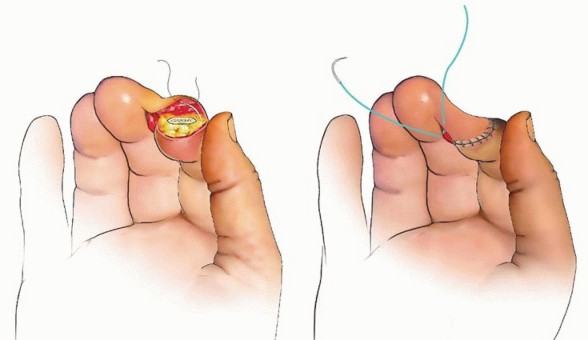
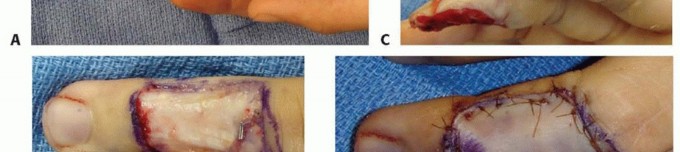
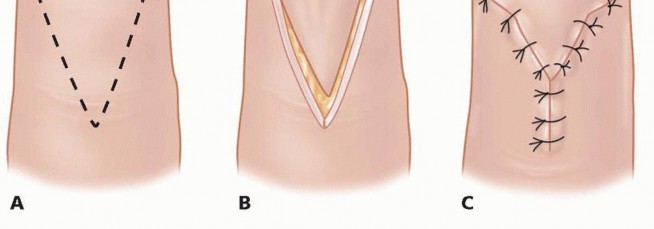
Volar V-Y Advancement Flap (Atasoy Technique)
The Atasoy V-Y advancement flap is considered the workhorse local flap for transverse and dorsal oblique fingertip amputations presenting with exposed distal phalangeal bone.


The apex of the "V" is designed precisely at or just distal to the distal interphalangeal joint crease to avoid flexion contractures. The width of the base of the flap should equal the width of the nail bed defect. Incisions are made strictly through the dermis, taking care not to violate the underlying subcutaneous fat where the neurovascular arborization resides.


The critical and most technically demanding step involves the systematic release of the fibrous septa that tether the volar skin to the periosteum of the distal phalanx. This must be performed meticulously using tenotomy scissors or a #15 scalpel blade, staying immediately adjacent to the periosteum. This deep plane of dissection avoids iatrogenic injury to the neurovascular bundles within the pulp. Once adequately mobilized, the flap is advanced distally to cover the exposed bone without tension. The distal edge is sutured to the nail bed or hyponychium, and the proximal defect is closed side-to-side in a "Y" configuration.
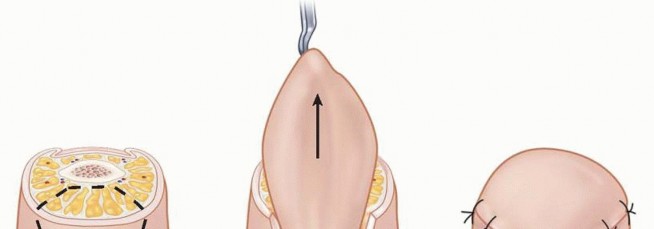
Bilateral V-Y Advancement Flap (Kutler Technique)
The Kutler flap is specifically indicated for transverse or lateral oblique amputations. It utilizes two laterally based, triangular advancement flaps rather than a single volar flap.

The apices of the triangles are positioned along the mid-lateral line of the digit, extending proximally. Similar to the Atasoy flap, initial incisions are made solely through the dermis. The deep fibrous septa are then meticulously released from the phalangeal periosteum to allow for mobilization.

Both lateral flaps are mobilized and advanced distally to meet at the midline over the exposed bone. The flaps are sutured to each other at the apex, to the nail bed dorsally, and the proximal donor sites are closed in a "Y" fashion. While effective, this technique can occasionally result in a hyperesthetic midline scar directly over the tip, making it less favorable than the Atasoy flap for patients requiring fine tactile discrimination.
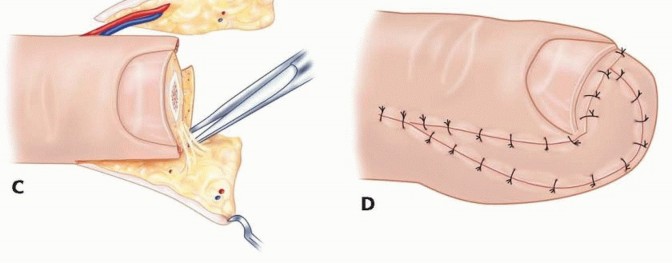
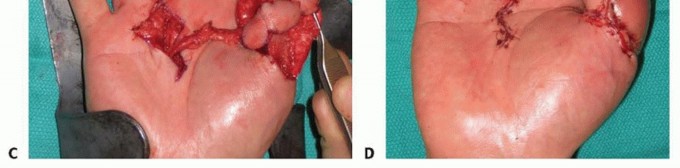
Cross Finger Flap
The cross-finger flap is a highly reliable regional flap ideal for volar oblique defects where local advancement flaps provide insufficient coverage or excessive tension. It utilizes the dorsal skin and subcutaneous tissue of an adjacent, less critical digit (typically the middle or ring finger).


A laterally based rectangular flap is designed on the dorsum of the middle phalanx of the donor digit. The flap is elevated in the precise areolar plane between the subcutaneous tissue and the paratenon of the extensor mechanism. It is absolutely imperative to leave the paratenon intact; a denuded extensor tendon will not support the subsequent full-thickness skin graft and will lead to tendon necrosis or severe adhesions.

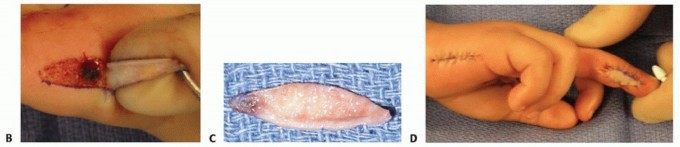
The flap is hinged laterally and sutured into the volar defect of the injured digit. A full-thickness skin graft, typically harvested from the hypothenar eminence, proximal forearm, or groin, is placed over the donor site paratenon and secured with a tie-over bolster dressing. The digits are immobilized together for two to three weeks to allow for neovascularization, after which the pedicle is divided and inset under local anesthesia.
Thenar Flap
The thenar flap is primarily indicated for significant volar oblique amputations of the index and middle fingers. It provides thick, durable, glabrous skin that closely matches the native volar pulp in both texture and resilience.


The donor site is designed on the thenar eminence, typically as a proximally based or H-shaped flap to ensure robust vascularity. The injured digit is flexed to meet the thenar eminence, ensuring the position is comfortable and the flap reaches the defect without excessive tension.
The flap is elevated, taking extreme care to avoid injury to the superficial branch of the radial nerve and the recurrent motor branch of the median nerve. The flap is sutured to the fingertip defect. The donor site can often be closed primarily or covered with a small skin graft. Division and inset are performed at two to three weeks. This flap is strictly contraindicated in older patients or those with pre-existing joint stiffness due to the high risk of permanent proximal interphalangeal (PIP) joint flexion contracture resulting from prolonged immobilization in flexion.
Moberg Volar Advancement Flap
The Moberg flap is the reconstructive procedure of choice for volar defects of the thumb measuring up to 1.5 to 2.0 centimeters. It relies on the robust, independent dorsal vascular supply of the thumb (via the princeps pollicis and dorsal arteries), making it generally unsafe for use in the lesser digits where dorsal
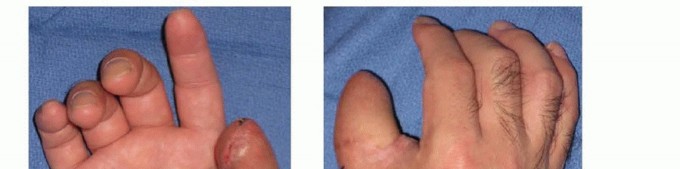
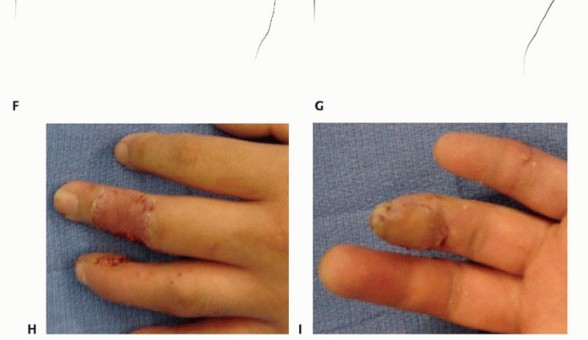
Clinical & Radiographic Imaging






You Might Also Like

