Mastering Triangular Fibrocartilage Complex (TFCC) Repair: An Intraoperative Guide

Key Takeaway
This masterclass guides fellows through the intricate world of Triangular Fibrocartilage Complex (TFCC) repair. We delve into detailed wrist anatomy, preoperative planning, and a granular, step-by-step intraoperative execution of arthroscopic and open techniques. Emphasizing critical decision-making, complication avoidance, and comprehensive rehabilitation, this session equips surgeons with the expertise to manage challenging ulnar-sided wrist pathologies effectively.
Introduction: Understanding the TFCC and Ulnar-Sided Wrist Pain
Alright, fellows, gather around. Today, we're operating on a complex case of ulnar-sided wrist pain, a common yet often misdiagnosed condition. Our focus will be the Triangular Fibrocartilage Complex, or TFCC, a critical structure that, when injured, can severely impact a patient's function and quality of life.
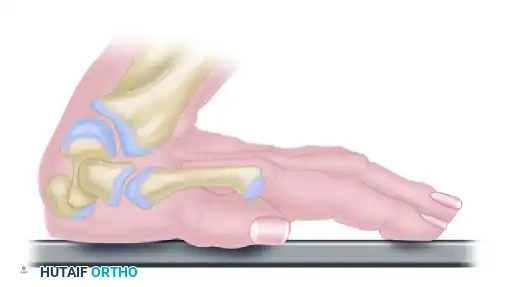
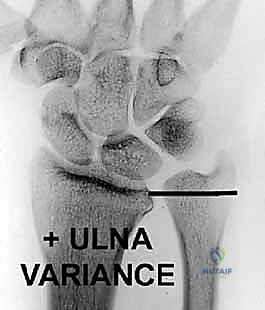
The TFCC is more than just a piece of cartilage; it's a dynamic unit. It's the primary shock absorber and stabilizer of the distal radioulnar joint (DRUJ) and the ulnar carpus. Think of it as the meniscus of the wrist. The amount of load transferred to the distal ulna varies significantly with ulnar variance. In a wrist with positive ulnar variance, where the ulna extends further distally relative to the radius, a greater axial load is transmitted, often leading to increased stress on the TFCC. Conversely, negative ulnar variance, where the ulna is shorter, reduces this load.
Forearm rotation also profoundly impacts the TFCC. As we supinate the forearm, the ulna migrates proximally, creating a relative negative ulnar variance. Pronation reverses this, causing the ulna to move distally, leading to a relative positive ulnar variance. Simultaneously, the ulnar head glides within the sigmoid notch of the radius – dorsally with pronation and volarly with supination. These intricate movements highlight the TFCC's role in extending the gliding surface of the radiocarpal joint, cushioning the ulnar carpus, and, crucially, stabilizing the DRUJ.
Disorders of the TFCC manifest as ulnar-sided wrist pain, weakness, and instability, severely affecting the patient's ability to perform daily activities. Our goal today, through precise diagnosis and meticulous surgical treatment, is to restore stability, alleviate pain, and ensure a robust functional return for our patient.
Comprehensive Surgical Anatomy of the TFCC
Let's begin with a detailed review of the anatomy, which is paramount to safe and effective TFCC surgery.
The TFCC: Structure and Attachments
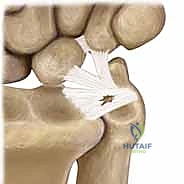
The TFCC is a cartilaginous and ligamentous structure strategically interposed between the ulnar carpus and the distal ulna. It originates distally from the sigmoid notch of the radius – a concave articular surface on the medial aspect of the distal radius – and extends to insert into the base of the ulnar styloid.
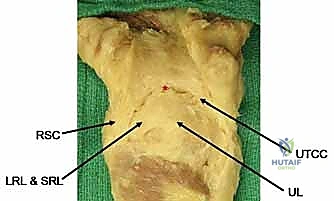
The TFCC also attaches to the ulnar carpus via the ulnocarpal ligament complex, which includes the ulnolunate, ulnotriquetral, and ulnar collateral ligaments. These ligaments are not independent structures but rather function as a cohesive unit with the TFCC itself.
The dorsal and volar radioulnar ligaments are fibrous thickenings within the substance of the peripheral TFCC. These are the primary stabilizers of the DRUJ, limiting both rotation and axial migration of the ulna relative to the radius. They are critical for maintaining the congruity and stability of the DRUJ during forearm rotation.
The central, horizontal portion of the TFCC is its thinnest part, composed of obliquely oriented collagen fibers designed to resist multidirectional stress. This structural difference is key to understanding its biomechanics and healing potential.
Vascularity and Clinical Implications
The vascularity of the TFCC is a critical anatomical consideration that dictates our treatment approach. The TFCC receives its blood supply from the ulnar artery via its radiocarpal branches, as well as the dorsal and palmar branches of the anterior interosseous artery. These vessels penetrate the TFCC in a radial fashion.
However, histologic studies demonstrate that these vessels supply only the peripheral 10% to 40% of the TFCC. The central section and its radial attachment are largely avascular. This fundamental difference in vascularity directly supports the concept that peripheral injuries, with their robust blood supply, have a much greater potential to heal if appropriately repaired. Conversely, tears of the central, avascular portion typically do not heal with suture repair and are usually best treated with debridement.
Neurovascular Risks and Muscular Intervals
When performing wrist arthroscopy or open procedures, we must be acutely aware of the surrounding neurovascular structures:
- Ulnar Nerve: Located on the ulnar side of the wrist, passing through Guyon's canal. Its dorsal sensory branch courses subcutaneously over the dorsal aspect of the ulnar wrist. Meticulous care is required, especially when creating ulnar-sided portals (e.g., 6R, 6U).
- Ulnar Artery: Accompanies the ulnar nerve through Guyon's canal.
- Dorsal Ulnar Sensory Nerve Branch: Highly susceptible to injury during portal placement, particularly the 6R and 6U portals, which can lead to painful neuromas or sensory deficits.
- Extensor Carpi Ulnaris (ECU) Tendon: This tendon runs within its own sheath in the sixth dorsal compartment, immediately adjacent to the TFCC. Its stability is crucial, and subluxation can mimic TFCC pathology. Our surgical approaches must navigate around this tendon and its sheath.
Relevant Osteology
A thorough understanding of the bony landmarks is essential:
- Distal Radius: Sigmoid notch (TFCC origin), Lister's tubercle (dorsal landmark).
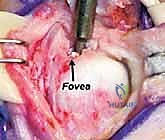
- Distal Ulna: Ulnar head (articulates with sigmoid notch), ulnar styloid (TFCC insertion, ulnocarpal ligament attachment), fovea (deep depression at the base of the styloid where the TFCC attaches).
- Carpal Bones: Lunate and triquetrum (components of the ulnar carpus, articulating with the TFCC via ulnocarpal ligaments).
Pathogenesis and Biomechanics of TFCC Injuries
TFCC injuries are broadly categorized into traumatic (Class 1) and degenerative (Class 2) lesions, as per the Palmer classification system.
Traumatic Lesions (Palmer Class 1)
These injuries typically result from:
* An extension, pronation force applied to an axially loaded wrist, often seen in a fall on an outstretched hand (FOOSH injury).
* A distraction force to the ulnar aspect of the wrist.
* A resisted torque force.
These traumatic lesions are more common in patients with ulnar-positive or neutral variance and are frequently associated with distal radius fractures. Studies have shown a high incidence of TFCC injuries coexisting with distal radial fractures, ranging from 43% to 84%.
Degenerative Lesions (Palmer Class 2)
Degeneration of the TFCC is an age-related phenomenon, typically beginning in the third decade of life and increasing in frequency and severity with age. By the fifth decade, 100% of TFCCs may appear abnormal histologically. However, it's crucial to remember that these age-related degenerative lesions are often asymptomatic. It's when a degenerative lesion becomes symptomatic, often due to a superimposed minor trauma or chronic impaction, that it requires intervention. Degenerative lesions are commonly associated with positive ulnar variance and ulnocarpal impaction syndrome.
Biomechanical Functions Revisited
Let's reiterate the critical biomechanical roles:
1. Axial Load Transmission: The TFCC transmits approximately 20% of an axially applied load from the ulnar carpus to the distal ulna. This percentage can increase significantly with positive ulnar variance.
2. DRUJ Stabilization: It is the major stabilizer of the DRUJ, preventing excessive dorsal-volar translation and rotation of the ulna relative to the radius. The dorsal and volar radioulnar ligaments are key to this stability.
3. Ulna Stabilization: It acts as a stabilizer of the entire ulna, contributing to overall wrist and forearm stability.
Classification of TFCC Injuries (Palmer Classification)
The Palmer classification system remains the most useful for describing and guiding the treatment of TFCC injuries.
Traumatic Lesions (Class 1)
These are divided into subclasses based on the location of the tear:
* Class 1A: Central Tear. This involves a tear in the central, horizontal portion of the TFCC, typically 2 to 3 mm medial to its radial attachment. It's usually oriented from dorsal to volar. Due to the avascular nature of this central zone, these tears often don't heal and are usually debrided arthroscopically.
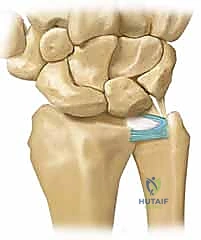
* Class 1B: Ulnar Avulsion. This is an avulsion of the peripheral aspect of the TFCC from its insertion onto the distal ulna. It can occur as a pure soft tissue avulsion or be associated with an ulnar styloid fracture. This type of injury directly disrupts the stabilizing effect on the DRUJ, leading to clinical instability. These peripheral tears are typically well-vascularized and amenable to repair.
* Class 1C: Distal Avulsion (Ulnocarpal Ligament Tear). This represents an avulsion of the TFCC's attachment to the ulnar carpus, specifically through disruption of the ulnolunate and ulnotriquetral ligaments. These lesions lead to ulnar carpal instability, often with volar translocation of the carpus.
* Class 1D: Radial Avulsion. This is a detachment of the TFCC from its insertion onto the radius at the distal sigmoid notch. It can range from an isolated disc tear to a global TFCC injury involving disruption of both dorsal and volar radioulnar ligaments, resulting in significant DRUJ instability.
Degenerative Lesions (Class 2)
These are age-related, nontraumatic lesions, typically characterized by central perforations and often associated with positive ulnar variance. The natural history is a progressive cascade of degenerative changes:
* Type 2A: TFC wear.
* Type 2B: TFC wear with chondromalacia of the lunate or distal ulna.
* Type 2C: Fibrillated central TFC lesion with perforation.
* Type 2D: Central TFC perforation with chondromalacia of the lunate and distal ulna, and a lunatotriquetral (LT) ligament tear.
* Type 2E: All of the above, plus arthritic changes of the lunate, triquetrum, and distal ulna.
Fellows, it's important to note that degenerative and traumatic lesions can coexist. A pre-existing degenerative lesion can become symptomatic following a minor traumatic event.
Patient History and Physical Findings: The Diagnostic Process
A thorough history and physical examination are the cornerstones of diagnosing TFCC injuries.
History
Patients typically present with ulnar-sided wrist pain, often accompanied by clicking, catching, or grinding sensations. The pain is frequently exacerbated by activities involving forearm rotation, gripping, or axial loading of the wrist. A history of a fall on an outstretched hand is common for traumatic injuries.
Physical Examination
- Inspection: Look for swelling over the ulnar aspect of the wrist, which might indicate inflammation. Sometimes, inflammation of the extensor carpi ulnaris (ECU) tendon sheath is also present.
- Palpation:
- Point Tenderness: Localized tenderness over the TFCC and distal ulna is a key finding. The more isolated the point of maximal tenderness, the more specific the diagnosis.
- Fovea Sign: Point tenderness directly over the ulnar TFCC origin (the depression between the ulnar styloid and the ulnar head) is highly indicative of a Type 1A or 1B TFCC injury or an ulnar extrinsic injury (Type 1C).
- Lunatotriquetral Interval: Tenderness here, combined with a positive shuck test, suggests an LT ligament tear.
- Triquetrum: Point tenderness may signify an avulsion fracture.
- Pisotriquetral Joint: Crepitus and pain on a shear test may indicate pisotriquetral arthritis.
- Provocative Tests:
- TFCC Compression Test: With the wrist in ulnar deviation and axially loaded, pronating and supinating the forearm will often elicit a painful response and a click, particularly with central tears or impaction.
- DRUJ Instability Assessment: This is crucial. Stabilize the distal radius with one hand and apply dorsal and volar forces to the distal ulna. Compare the motion and any subluxation with the uninjured contralateral wrist. Perform this in neutral rotation, full supination, and full pronation. Significant instability can manifest as laxity of the distal ulna with a positive "piano key" sign (the ulna springs back after being depressed) and dorsal prominence. This indicates a significant tear or detachment of the dorsal or volar radioulnar ligaments (Class 1B or 1D).
- ECU Instability Test: A click produced by ulnar deviation and supination over the ECU sheath at the distal ulna indicates ECU instability with subluxation out of its sixth extensor compartment.
- Carpal Supination Deformity: A visual ulnar prominence that can be passively corrected by applying a dorsal force to the pisiform suggests an ulnar extrinsic ligament tear (Class 1C).
- Midcarpal Instability: An audible clunk and visual subluxation of the carpus that occurs with active ulnar deviation suggests midcarpal instability.
- Neurovascular Examination: Always assess the ulnar nerve (motor and sensory), the dorsal ulnar sensory nerve branch, and the ulnar artery to rule out concomitant nerve entrapment or vascular compromise.
- Grip Strength: Use a Jamar dynamometer to objectively quantify patient effort and monitor therapeutic progress.
Surgical Warning: TFCC injuries rarely occur in isolation. Always conduct a comprehensive evaluation of all commonly injured structures on the ulnar side of the wrist to avoid missing concomitant pathologies.
Imaging and Other Diagnostic Studies
Plain Radiographs
- Views: Obtain neutral rotation posteroanterior (PA) and lateral views of the wrist. Oblique views may also be helpful.
- Assessment: These radiographs are essential to assess for fractures (e.g., ulnar styloid, triquetral avulsion), ligament instability causing carpal malalignment, and, critically, ulnar variance.
Fellows, determining ulnar variance is paramount as it directly influences treatment options, especially for degenerative lesions.
* DRUJ: Radiographs should also examine the DRUJ for signs of subluxation, arthritis, or abnormalities of the ulnar styloid, such as an acute or chronic nonunited fracture fragment.
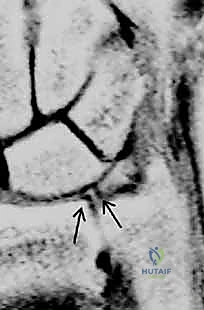
Magnetic Resonance Imaging (MRI)
- Utility: MRI is a valuable tool for diagnosing TFCC tears, particularly Class 1A (central) and 1D (radial avulsion) lesions.
- Sequences: T2-weighted images in the coronal plane offer the greatest diagnostic value. The TFCC normally exhibits a homogenous low signal intensity. Synovial fluid appears as a bright signal on T2-weighted images and will outline tears within the TFCC.
* MR Arthrography: Injecting gadolinium into the joint enhances the visualization of TFCC tears, improving sensitivity and specificity compared to conventional MRI. However, even with arthrography, negative results in a patient with strong clinical suspicion should be interpreted with caution.
* Sensitivity & Specificity: The reported sensitivity and specificity of MRI for TFCC tears vary widely in the literature (e.g., sensitivity 44-95%, specificity 75-95%). While useful, MRI findings do not always perfectly correlate with arthroscopic findings.
Wrist Arthroscopy: The Gold Standard
- Diagnostic Superiority: Wrist arthroscopy has become the criterion standard for both diagnosing and treating TFCC lesions. It offers unparalleled accuracy in determining the exact location, size, and stability of tears, and whether a flap is unstable or impinging.
- Concomitant Lesions: Arthroscopy also allows for the identification and treatment of coexisting pathologies, such as tears within the lunotriquetral interosseous ligament, ECU subsheath tears, or chondral lesions of the carpus or distal ulna.
Differential Diagnosis
Before proceeding to surgery, always consider a broad differential diagnosis for ulnar-sided wrist pain:
* ECU subluxation
* Ulnar extrinsic ligament tear
* DRUJ instability (traumatic or chronic)
* Triquetral avulsion fracture
* Lunatotriquetral ligament injury
* Pisotriquetral arthritis
* Ulnar artery thrombosis
* Ulnar neuropathy at the canal of Guyon
* Dorsal ulnar sensory neuritis
* Hook of hamate fracture
* Extensor or flexor carpi ulnaris tendinopathy
Nonoperative Management
Initial management for acute TFCC injuries, especially without significant DRUJ instability or displaced fractures, is typically nonoperative.
Acute Injuries
- Immobilization: If radiographs are negative and DRUJ instability is not present, immobilize the wrist and DRUJ for 4 to 6 weeks in a cast or splint. This allows the torn edges of peripheral tears, which are well-vascularized, to heal. Even many central, avascular tears can become asymptomatic with immobilization, likely due to scar formation or a reduction in inflammation.
- Inflammation Control: A well-placed cortisone injection can help quiet ongoing synovitis.
- Rehabilitation: After immobilization, initiate a structured therapy program focusing on range-of-motion exercises, followed by gradual strengthening. Forceful grasp or torque activities should be restricted for at least 8 weeks.
- Class 1B Lesions: If a Class 1B lesion is present without an ulnar styloid fracture and the DRUJ is stable, 4 weeks of cast immobilization is often sufficient.
- Ulnar Styloid Fractures: If an ulnar styloid fracture is present, attempt closed reduction. If adequate reduction is achieved and maintained, cast immobilization is sufficient. If the styloid remains significantly displaced, open reduction and internal fixation (ORIF) may be required.
Degenerative Type 2 Lesions
The initial algorithm for degenerative type 2 tears also begins with arthroscopic debridement. If symptoms persist, further treatment may involve ulnar-
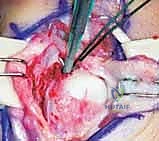
Additional Intraoperative Imaging & Surgical Steps









REFERENCES
-
Adams BD. Partial excision of the triangular fibrocartilage complex articular disk: a biomechanical study. J. Hand Surg Am 1993; 18A:334–340.
-
Bednar JM, Bos M, Giacobetti F. Comparison of the Accuracy of Clinical Exam and MRI in Diagnosing TFCC Lesions. Presented at the ASSH 52nd Annual Meeting, Sept. 11, 1997, Denver, Colorado.
-
Bednar MS, Arnoczky SP, Weiland AJ. The microvasculature of the triangular fibrocartilage complex: its clinical significance. J. Hand Surg Am 1991;16A:1101–1105.
-
Chun S, Palmer AK. The ulnar impaction syndrome: follow up of ulnar shortening osteotomy. J Hand Surg Am 1993;18A:46–53.
-
Corso SJ, Savoie FH, Geissler WB, et al. Arthroscopic repair of peripheral avulsions of the triangular fibrocartilage complex of the wrist: a multicenter study. Arthroscopy 1997;13:78–84.
-
Culp R, Osterman L, Kaufmann R. Wrist arthroscopy: operative procedures. In: Green D, Hotchkiss R, Pederson W, et al, eds. Green’s Operative Hand Surgery, 5th ed, vol.
-
Philadelphia: Elsevier, 2005.
-
Ekenstein FW, Palmer AK, Glisson RR. The load on the radius and ulna in different positions of the wrist and forearm. Acta Orthop Scand 1984;55:363–365.
-
Geissler WB, Freeland AE, Savoie FH, et al. Intracarpal soft-tissue lesions associated with an intra-articular fracture of the distal end of the radius. J Bone Joint Surg Am 1996;78A:357–365.
-
Golimbu CN, Firooznia H, Melone CP Jr, et al. Tears of the triangular fibrocartilage of the wrist: MR imaging. Radiology 1989;173: 731–733.
You Might Also Like