Scapholunate Ligament Bone-Ligament-Bone Reconstruction: An Intraoperative Masterclass
Key Takeaway
This masterclass details bone-ligament-bone reconstruction for scapholunate ligament tears. We cover comprehensive anatomy, precise preoperative planning, and granular intraoperative steps from incision to graft fixation. Fellows will learn critical pearls, pitfalls, and post-operative management, ensuring optimal outcomes for carpal instability. This immersive guide emphasizes meticulous technique and rationale in the operating theater.
Welcome, fellows, to the operating theater. Today, we're tackling a challenging yet incredibly rewarding procedure: the Bone-Ligament-Bone (BLB) Reconstruction of the Scapholunate Ligament. This isn't just about fixing a tear; it's about restoring the intricate biomechanics of the wrist, preventing the relentless progression of degenerative arthritis, and giving our patients back their function. Let's scrub in and walk through this together.
Understanding Scapholunate Instability: The Foundation
Before we make any incision, we must have an absolute mastery of the pathology we're addressing. Scapholunate ligament tears are, unequivocally, the most common form of carpal instability. If left untreated, this injury leads to predictable and debilitating degenerative changes in the wrist, often culminating in what we call Scapholunate Advanced Collapse (SLAC wrist).
Anatomy of the Scapholunate Ligament
Let's orient ourselves. The scapholunate interosseous ligament is an intrinsic, intra-articular ligament composed of collagen fascicles, and it's truly a marvel of engineering. It has three distinct parts, each with unique biomechanical properties:
- Dorsal Portion: This is the workhorse, fellows – the strongest of the three. It's typically 2 to 3 mm thick and 3 to 5 mm long. Its collagen bundles are oriented transversely, making it supremely effective at limiting dorsal-palmar translation between the scaphoid and lunate. Crucially, its most dorsal aspect merges seamlessly with the wrist articular capsule. It can withstand over 300 Newtons (N) of tensile stress before failure.
- Volar Portion: Thinner at just 1 mm thick and 4 to 5 mm long, with obliquely oriented collagen bundles. Together with the proximal portion, it's vital for limiting dorsal-palmar rotation. It's intersected by the loose radioscapholunate ligament, also known as the ligament of Testut. Failure here occurs at around 150 N.
- Proximal (Membranous) Portion: This is the weakest and thinnest part, predominantly fibrocartilaginous and avascular. There are no neurovascular bundles within it, which unfortunately contributes to its poor healing potential. A mere 25 N of stress can cause this portion to fail.
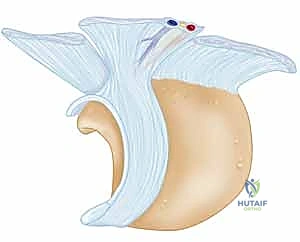
FIG 1 • The scapholunate ligament viewed from the proximal radial side with the scaphoid removed. Note the distinct dorsal, membranous, and volar components.
The lunate naturally flexes with the scaphoid and extends with the triquetrum. In a scapholunate ligament injury, this vital connection to the scaphoid is lost. The scaphoid, freed from the lunate's influence, will flex and rotate away due to its other attachments. Conversely, the lunate, now unconstrained by the scaphoid, will fall into a dorsal intercalated segment instability (DISI) pattern. Understand that for this profound rotational instability to manifest, the dorsal capsular ligaments must also be injured or significantly attenuated.
Pathogenesis and Natural History: The Unfolding Disaster
The typical mechanism of injury is a fall on an outstretched hand. Mayfield and colleagues elegantly described this as an axial load combined with excessive dorsiflexion, ulnar deviation, and midcarpal supination. This unfortunate combination forces the capitate to drive a wedge between the scaphoid (which is pushed radially and dorsally) and the lunate (which is pushed ulnarly and palmarly).
It's critical to recognize associated injuries; an ipsilateral distal radius fracture or scaphoid fracture can occur in up to 30% of these cases. An acute scapholunate injury may or may not immediately present with a DISI pattern. If surrounding ligaments (like the dorsal extrinsics) are also acutely injured, DISI can be seen early. However, even if these structures are initially intact, their attenuation over time will eventually lead to DISI. Correcting this pattern is paramount for any treatment to succeed.
The natural history of an untreated scapholunate injury is a grim progression:
- Pain and Instability: Initial symptoms.
- DISI Deformity: The lunate extends dorsally, and the scaphoid flexes volarly.
- SLAC Wrist Progression: A very specific, sequential pattern of wrist arthrosis develops:
- Stage IA: Radial styloid arthrosis, with or without scaphoid arthrosis.
- Stage IB: Radioscaphoid arthrosis.
- Stage II: Capitolunate arthrosis.
- Stage III: Pan-arthritis, sparing only the radiolunate joint in most cases.
Patient Evaluation: Unmasking the Instability
Our diagnostic journey begins long before the OR.
Patient History and Physical Findings
Patients typically present with radial-sided wrist pain, particularly with loading activities, and a subjective sense of weakness.
On physical examination, we meticulously assess:
- Observation and Palpation: Look for gross edema or any visible deformity. Palpate just distal to the tubercle of Lister for exquisite tenderness, a hallmark of scapholunate interval pathology.
- Range of Motion (ROM): Assess flexion, extension, ulnar, and radial deviation. Decreased ROM or pain at extremes of motion are common.
- Ballottement Test: Stabilize the lunate with one hand and attempt to translate the scaphoid dorsally and volarly with the other. Pain or abnormal instability is highly suggestive of a scapholunate tear.
- Watson Test (Scaphoid Shift Test): This is a cornerstone. While stabilizing the lunate and applying pressure to the scaphoid tuberosity, gently move the wrist from ulnar to radial deviation. In a normal wrist, the scaphoid flexes smoothly. In a wrist with a scapholunate tear, the proximal pole of the scaphoid will dorsally subluxate out of the scaphoid fossa, often with a palpable and sometimes audible "clunk." This clunk is indicative of instability.
- Grip Strength: Weakness is a sensitive but non-specific indicator of scapholunate disruption.
- Comprehensive Wrist Examination: Always rule out associated injuries and differential diagnoses:
- Lunatotriquetral tears: Pain with a "shuck" test of the lunate and triquetrum.
- Distal radius or scaphoid fracture: Tenderness over the distal radius or in the anatomical snuffbox.
- TFCC tears: Pain with an axial load and ulnar deviation through a flexion-extension arc.
- Masses: Carefully examine for any ganglion cysts or other masses.
- DeQuervain tenosynovitis, Dorsal wrist impaction syndrome, Midcarpal instability, Dorsal ganglion cyst, Radioscaphoid or Scaphotrapezial arthritis.
Imaging and Other Diagnostic Studies
Our diagnostic armamentarium includes:
- Plain Radiographs: Always start here.
- PA, Lateral, and Scaphoid Views: Standard series. Some advocate for a "complete" series including clenched-fist PA, radial deviation PA, and flexion/extension laterals. Compare to the contralateral wrist if possible.
- Static Instability Signs (PA view):
- Increased Scapholunate Gap: A normal interval is less than 3 mm. Greater than 3 mm is the classic Terry Thomas sign.
- Scaphoid Ring Sign: The scaphoid collapses into flexion, causing its tuberosity to project in the coronal plane, appearing as a "ring."
- Volar Lip Overlap: The volar lip of the extended lunate may overlap with the capitate.

FIG 2 • A. PA radiograph demonstrating an increased scapholunate gap and a scaphoid ring sign. B. A fluoroscopic image of another example of an increased scapholunate gap. C. The contralateral wrist demonstrates a normal scapholunate interval.

FIG 2 • A. PA radiograph demonstrating an increased scapholunate gap and a scaphoid ring sign. B. A fluoroscopic image of another example of an increased scapholunate gap. C. The contralateral wrist demonstrates a normal scapholunate interval.
* Static Instability Signs (Lateral view):
* Increased Scapholunate Angle: Measured by drawing lines through the longitudinal axes of the scaphoid and lunate. Normally 30-60 degrees. An angle greater than 60 degrees indicates scaphoid flexion.
* DISI Deformity: A radiolunate angle greater than 15 degrees indicates the lunate is extended dorsally.

FIG 2 • (continued) D. A lateral radiograph demonstrating an increased scapholunate angle.
* Dynamic Instability (Stress Radiographs): Flexion/extension laterals, radial/ulnar deviation, and clenched-fist views may reveal diastasis not evident on static films.
* Chronic Injury: Look for signs of arthritis (SLAC wrist stages).

FIG 2 • (continued) E,F. Scapholunate advanced collapse (SLAC) wrist. E. Early-stage arthrosis from a chronic scapholunate ligament injury affecting the radial styloid.
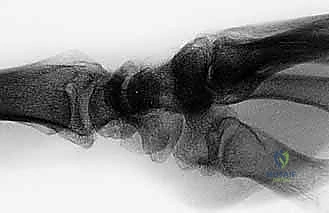
FIG 2 • (continued) F. This PA view on the right demonstrates a more advanced stage. Bone–ligament–bone reconstruction may not be the preferred choice of treatment here.

FIG 2 • (continued) F. This PA view on the right demonstrates a more advanced stage. Bone–ligament–bone reconstruction may not be the preferred choice of treatment here.
* Magnetic Resonance Imaging (MRI): Valuable for assessing acute and chronic tears, providing excellent soft tissue detail.

FIG 2 • (continued) G. MRI with a scapholunate ligament injury.
* Diagnostic Arthroscopy: This is often the gold standard. It allows direct visualization of the ligament, assessment of tissue quality, and diagnosis of concomitant injuries. Geissler et al. published a four-stage classification based on arthroscopic findings, which guides our treatment decisions.

FIG 2 • (continued) H. Arthroscopic view. Arthroscopy can easily identify scapholunate ligament tears.
Treatment Algorithm: When to Reconstruct
Our treatment strategy is dictated by the chronicity of the injury and the presence of arthrosis.
Nonoperative Management
Nonoperative management is seldom indicated for significant scapholunate injuries. Only Geissler grade 1 injuries (minor sprains) are typically treated with immobilization alone. We prefer a removable volar splint worn full-time for 4 weeks, followed by 4 weeks of splinting with removal for active range-of-motion exercises. Passive ROM and strengthening are initiated after 8 weeks.
Surgical Management: Indications for BLB Reconstruction
The decision for surgical intervention, and specifically for BLB reconstruction, is crucial.
- Acute (≤ 3-4 weeks):
- Dynamic Instability: Immobilization, arthroscopic shrinkage, percutaneous pinning, or capsulodesis.
- Static Instability: Open repair of the scapholunate interosseous ligament (if possible) is the treatment of choice. If not amenable to repair, then BLB reconstruction, tendon weave, or capsulodesis.
- Subacute (4-24 weeks): Reconstruction, tendon weave, or capsulodesis. Primary repair may still be possible if sufficient remnant ligament is available.
- Chronic (> 24 weeks):
- No Arthrosis: Reconstruction, tendon weave, or capsulodesis.
- With Arthrosis (SLAC Wrist): Salvage procedures are indicated (e.g., PRC, intercarpal arthrodesis like STT, scaphocapitate, or scapholunate-capitate arthrodesis). Crucially, repair or reconstruction of the scapholunate ligament is futile in the presence of SLAC arthrosis. These procedures will not address arthritic pain.
Advantages of Bone-Ligament-Bone Reconstruction
This technique offers several key advantages:
- More Anatomic Reconstruction: Better approximates the complex carpal kinematics compared to tendon weaves.
- Bone-to-Bone Healing: This is a significant advantage over tendon-to-bone healing, providing a robust, predictable construct.
- Local Tissue Availability: We prefer local tissue for the graft, minimizing donor site morbidity.
Preoperative Planning: Precision is Paramount
Every successful surgery begins with meticulous planning.
- Radiographic Review: Thoroughly review all plain radiographs for any evidence of arthrosis. If SLAC changes are present (Stage IB or higher), a reconstruction is contraindicated, and we pivot to a salvage procedure.
- MRI Review: Scrutinize the MRI for the extent of the scapholunate ligament tear, associated soft tissue pathology, and any other carpal injuries.
- Associated Injuries: Address any concomitant fractures or other soft tissue pathology.
- Anesthesia Consultation: Discuss regional block options (e.g., axillary block) in addition to general anesthesia for excellent postoperative pain control.
- Watson Shift Test Under Anesthesia: This is a critical step. With the patient fully relaxed, the examiner can often better appreciate the characteristic clunk of instability without the confounding factor of patient pain and guarding. This confirms the dynamic instability.
- Graft Source Decision: We prefer local tissue, specifically the capitohamate ligament, due to its proximity and the avoidance of a second operative site and its associated morbidity. While dorsal tarsometatarsal ligaments from the foot have biomechanical similarities, clinical evidence for their superiority is lacking, and they introduce a separate donor site risk.
Patient Positioning and Arthroscopy: Initial Assessment
Let's get our patient positioned.
- Supine Positioning: The patient is positioned supine on the operating table.
- Hand Table: A specialized hand table is appropriately positioned and secured.
- Tourniquet: A non-sterile tourniquet is placed on the upper arm, set to 250 mm Hg. We'll inflate this after exsanguination.
- Preparation and Draping: Standard sterile preparation and draping of the upper extremity.
- Arthroscopic Setup: The wrist is then placed in an arthroscopic tower. We use plastic hook-and-eye straps and finger traps to apply about 10 to 15 pounds of traction. This distracts the joint, allowing for optimal visualization during diagnostic arthroscopy.


FIG 3 • Arthroscopic setup. The arthroscopic tower uses plastic hook-and-eye straps and finger traps. About 10 to 15 lb of traction is used to distract the joint for the diagnostic arthroscopy.
The diagnostic wrist arthroscopy is crucial. It allows us to:
* Evaluate the true extent of the scapholunate ligament injury.
* Assess the quality of any remaining ligamentous tissue.
* Diagnose any concomitant injuries that might influence our surgical plan.
Once the diagnostic arthroscopy is completed and the decision to proceed with open reconstruction is confirmed, we will release the traction, remove the wrist from the tower, and pronate the forearm, placing the hand flat on the hand table for the open approach.
The Dorsal Wrist Approach: Gaining Exposure
Now, let's turn our attention to the operative field.
- Incision: We'll make a longitudinal incision, approximately 6 to 8 cm in length. This incision starts just ulnar to the tubercle of Lister, extending distally towards the base of the third metacarpal. This precise placement allows for excellent exposure of the dorsal wrist capsule while minimizing disruption to critical structures.

TECH FIG 1 • Approach. A. A 6 to 8-cm incision is made ulnar to the tubercle of Lister, extending distally.
> **Surgical Warning:** Be mindful of the dorsal sensory branches of the ulnar and radial nerves during your skin incision and subcutaneous dissection. Meticulous hemostasis is key to maintaining a clear field.
- Subcutaneous Dissection: Using sharp and blunt dissection, carefully elevate the skin flaps. Identify and protect any superficial veins.
- Extensor Compartment Identification and Transposition:
- Locate the third extensor compartment, which houses the Extensor Pollicis Longus (EPL) tendon.
- Incise the sheath of the third compartment longitudinally.
- Carefully elevate the EPL tendon and transpose it in a radial direction. This provides direct access to the underlying dorsal wrist capsule.

TECH FIG 1 • Approach. B. The third extensor compartment is incised and the tendon is radialized.
> **Surgical Warning:** Ensure the EPL tendon is fully mobilized and retracted without excessive tension to prevent postoperative tendinitis or rupture.
- Interval Dissection: Continue your dissection between the second and fourth extensor compartments. This interval provides a safe corridor to the dorsal capsule.
- Posterior Interosseous Nerve (PIN) Excision: At this point, we will identify and excise a segment of the posterior interosseous nerve. This denervation procedure is routinely performed to decrease residual postoperative pain from the dorsal wrist capsule. Use careful blunt dissection to isolate the nerve and resect a small segment.
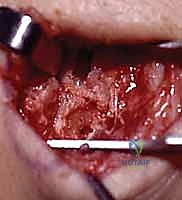
- Dorsal Wrist Capsulotomy: We'll perform a ligament-splitting dorsal wrist capsulotomy. This incision is made through the dorsal intercarpal and dorsal radiocarpal ligaments. This approach preserves the integrity of the capsule as much as possible, allowing for a more robust repair later.

TECH FIG 1 • Approach. C. A ligament-splitting incision is made in the capsule.

TECH FIG 1 • Approach. C. A ligament-splitting incision is made in the capsule.
> **Surgical Warning:** Ensure your capsulotomy provides adequate exposure to the scapholunate interval without unnecessarily traumatizing surrounding healthy capsule or underlying carpal bones.
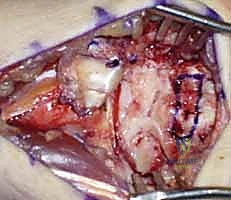
- Direct Visual Inspection: With the capsule opened, we can now directly inspect and probe the scapholunate ligament. This final intraoperative assessment helps us confirm the extent of the tear and determine if a direct primary repair is feasible (which is rare in chronic cases) or if reconstruction is indeed the best course of action.
Graft Harvesting: The Capitohamate Ligament
Our preferred graft source is the capitohamate ligament. It's local, readily available, and minimizes additional donor site morbidity.
- Localization: Using fluoroscopy, we'll confirm our position and use an 18-gauge needle to precisely identify the capitohamate ligament. This ensures we harvest the correct structure.
- Harvesting the Bone-Ligament-Bone Graft:
- We'll use a quarter-inch osteotome to carefully harvest a portion of the capitohamate ligament.
- Crucially, this harvest must include bone blocks measuring approximately 10 x 5 x 5 mm at each end of the ligament. This concept is directly analogous to the bone-patellar tendon-bone autograft used in anterior cruciate ligament reconstructions, allowing for robust bone-to-bone healing within the carpal tunnels we'll create.
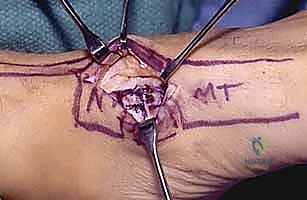
TECH FIG 2 • A. The capitohamate ligament is harvested with bone blocks (10 × 5 × 5 mm) on either end.
TECH FIG 2 • A. The capitohamate ligament is harvested with bone blocks (10 × 5 × 5 mm) on either end.

TECH FIG 2 • B. The bone-ligament-bone graft is ready for insertion.
> **Surgical Warning:** When harvesting the bone blocks, ensure they are of adequate size to prevent pull-out from the tunnels, but not so large that they compromise the integrity of the donor carpal bones. Maintain the ligamentous attachment to both bone blocks.
Alternative Graft Source: Dorsal Tarsometatarsal Ligament (Foot)
While we prefer local tissue, it's important to be aware of alternatives. The dorsal tarsometatarsal ligaments, specifically those between the lateral cuneiform and the third metatarsal, or between the navicular and the first cuneiform of the foot, have been shown to be geometrically and biomechanically similar to the scapholunate ligament.
If you choose this option:
- Incision: Make a longitudinal incision over the base of the third metatarsal.
- Dissection: Use sharp dissection to expose the joint.
-
Harvest: Use an osteotome to harvest the ligament with large bone blocks, similar to the capitohamate technique.
Surgical Warning: Remember, harvesting from the foot creates a second operative site, increasing the potential for morbidity (pain, infection, nerve injury, gait disturbance). We reserve this for specific situations where the capitohamate ligament is deemed unsuitable.
Scapholunate Reduction and K-wire Fixation: Restoring Alignment
Now that we have our graft, our immediate priority is to restore the anatomical alignment of the scaphoid and lunate. This is a critical step, fellows.
- Reduction Maneuver: We will use a combination of direct pressure and gentle manipulation.
- Apply pressure to the scaphoid tuberosity volarly to correct its flexion deformity.
- Simultaneously, apply pressure to the dorsal aspect of the lunate to correct its extension deformity.
- Gently push the scaphoid and lunate together to close the scapholunate interval.
- You should feel the carpal bones "seat" into a more anatomical position.
- Fluoroscopic Confirmation: Under constant fluoroscopic guidance, confirm the reduction. Look for:
- A normal scapholunate interval (less than 3 mm) on PA views.
- Correction of the scaphoid ring sign.
- Correction of the scapholunate angle (30-60 degrees) and radiolunate angle (less than 15 degrees) on lateral views.
-
K-wire Fixation: Once an optimal reduction is achieved, we will temporarily stabilize the scaphoid and lunate using K-wires.
- Typically, we'll insert two 0.045-inch or 0.062-inch K-wires.
- One K-wire will pass from the scaphoid into the lunate, traversing the reduced scapholunate interval.
- A second K-wire will pass from the lunate into the triquetrum, or from the scaphoid into the capitate, to further stabilize the carpus and maintain the reduction.
- Ensure the K-wires are placed to avoid future tunnel drilling sites and are not impinging on articular surfaces.
Surgical Warning: K-wire placement must be precise. Avoid violating the midcarpal or radiocarpal joint spaces. Confirm placement with multiple fluoroscopic views (PA, lateral, oblique) to ensure proper carpal alignment and avoid iatrogenic injury. Overtightening the reduction can lead to stiffness; aim for a stable, anatomical reduction.
Tunnel Creation and Graft Passage: The Reconstruction Itself
With the carpus stabilized, we can now prepare for graft insertion.
-
Tunnel Planning: We need to create bone tunnels in the scaphoid and lunate to accommodate the bone blocks of our graft.
- Using a small burr or a K-wire followed by a cannulated drill, create a tunnel in the scaphoid, entering dorsally and exiting volarly at the site of the original scapholunate ligament attachment.
- Similarly, create a tunnel in the lunate, entering dorsally and exiting volarly at its scapholunate attachment site.
- The tunnels should be sized to allow for a snug fit of the 10x5x5 mm bone blocks.
- Ensure the tunnels are positioned anatomically to recreate the natural course of the scapholunate ligament, particularly the strong dorsal component.
Surgical Warning: Drill under constant fluoroscopic guidance to prevent inadvertent penetration of the articular cartilage or neurovascular structures. The goal is to create tunnels that precisely mimic the anatomical footprint of the original ligament. Avoid creating tunnels that are too wide, as this will compromise bone block purchase.
-
Graft Passage:
- Carefully pass one bone block of the capitohamate graft through the tunnel in the scaphoid, ensuring the ligamentous portion spans the scapholunate interval.
- Then, pass the second bone block through the tunnel in the lunate.
- Use a suture passed through the bone block or a small clamp to guide it through the tunnels.
Surgical Warning: Avoid twisting or damaging the ligamentous portion of the graft during passage. Ensure the bone blocks are fully seated within the tunnels.
Graft Tensioning and Fixation: Achieving Stability
This is where we restore the crucial tension.
- Tensioning: With the graft in place, apply gentle but firm tension to the ligamentous portion. The goal is to recreate the normal tension of the scapholunate ligament, which helps to maintain the reduction of the scaphoid and lunate.
- While maintaining the carpal reduction with the K-wires, apply appropriate tension to the graft.
-
Fixation: Secure the bone blocks within their respective tunnels.
- Interference Screws: This is a common and effective method. Use bioabsorbable interference screws (e.g., 3.0 mm or 3.5 mm) to compress the bone blocks firmly into the tunnels.
- Suture Fixation: Alternatively, or in addition, drill small pilot holes through the carpal bones distal to the tunnels and pass strong non-absorbable sutures (e.g., FiberWire) through the bone blocks and out through these pilot holes. Tie the sutures over a cortical bridge or a small button on the dorsal aspect of the bone to secure the graft.
- Fluoroscopic Confirmation: Confirm stable fixation and maintained carpal alignment with fluoroscopy after fixation.

TECH FIG 3 • A. K-wires are used to reduce the scapholunate interval.

TECH FIG 3 • B. Bone tunnels are created in the scaphoid and lunate to accept the bone blocks.
> **Surgical Warning:** Overtensioning can lead to stiffness,
REFERENCES
-
Berger RA. The ligaments of the wrist: a current overview of anatomy with considerations of their potential functions. Hand Clin 1997; 13:63–82.
-
Davis CA, Culp RW, Hume EL, et al. Reconstruction of the scapholunate ligament in a cadaver model using a bone-ligament-bone autograft from the foot. J Hand Surg Am 1998;23A:884–892.
-
Garcia-Elias M, Geissler WB. Carpal instability. In: Green DP, Pederson WC, Hotchkiss RN, et al, eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:535–604.
-
Geissler WB, Freeland AE, Savoie FH, et al. Intracarpal soft tissue lesions associated with an intra-articular fracture of the distal end of the radius. J Bone Joint Surg Am 1996;78A:357–365.
-
Harvey EJ. Hand-based autograft replacement of the scapholunate ligament: early outcome (meeting transcript). American Society for Surgery of the Hand. Seattle, 2000.
-
Harvey EJ, Hanel DP. Bone-ligament-bone reconstruction for scapholunate disruption. Tech Hand Upper Extr Surg 2002;6:2–5.
-
Harvey EJ, Hanel DP. Autograft replacements for the scapholunate ligament: a biomechanical comparison of hand based autografts. J Hand Surg Am 1999;24A:963–967.
-
Mayfield JK. Wrist ligamentous anatomy and pathogenesis of carpal instability. Orthop Clin 1984;15:209–216.
-
Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226–241.
-
Shin SS, Moore DC, McGovern RD, et al. Scapholunate ligament reconstruction using a bone-retinaculum-bone autograft: a biomechanic and histologic study. J Hand Surg Am 1998;23:216–221.
-
Sokolow C, Saffar P. Anatomy and histology of the scapholunate ligament. Hand Clin 2001;17:77–81.
-
Svoboda SJ, Eglseder A, Belkoff SM. Autografts from the foot for reconstruction of the scapholunate interosseous ligament. J Hand Surg Am 1995;20A:980–985.
-
Walsh JJ, Berger RA, Cooney WP. Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32–42.
-
Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9A: 358–365.
-
Watson HK, Weinzweig J, Zeppieri J. The natural progression of scaphoid instability. Hand Clin 1997;13:39–49.
-
Weiss APC. Scapholunate ligament reconstruction using a bone-retinaculum-bone autograft. J Hand Surg Am 1998;23A:205–215.
-
Wolf JM, Weiss APC. Bone-retinaculum-bone reconstruction of scapholunate ligament injuries. Orthop Clin North Am 2001;32: 241–246.
-
Lutz M, Kralinger F, Goldhahn J, et al. Dorsal scapholunate ligament reconstruction using a periosteal flap of iliac crest. Arch Orthop Trauma Surg 2004;124:197–202.
The wrist is strictly immobilized for 8 weeks. Finger and elbow range of motion is encouraged.
Pins are removed at 8 weeks and gentle active range-ofmotion exercises are started. A removable splint is still worn when not exercising for an additional 4 weeks.
Passive range of motion begins at 12 weeks, followed by strengthening.
OUTCOMES
- Patients with a partial tear or dynamic component and patients with a shorter time from injury to treatment have a better outcome.
Weiss 16 reported excellent results at a minimum of 2 years of follow-up in 13 of 14 patients with scapholunate gaps of less than 8 mm using a bone–retinaculum–bone autograft, even though it has been shown to be biomechanically weaker than the native scapholunate ligament. This may be due to graft remodeling or hypertrophy in vivo.
Lutz al 18 used a periosteal flap of iliac crest as the autograft. With an average follow-up of 29 months, they reported 6 of 11 patients to be clinically excellent or good and 5 as fair. Average radiographic parameters improved.
Hanel 5 reported that all 39 of his patients treated with the bone-ligament-bone reconstruction outlined in this chapter returned to work, but some had difficulty with return to some sports. All patients would have the surgery again as it had helped their day-to-day activities.
Although there are no long-term clinical outcome studies in the literature on bone–ligament–bone reconstruction, shortterm results are promising. A larger number of patients with a longer follow-up is required to fully recommend this technique for most scapholunate injuries.
COMPLICATIONS
- Fragmentation of the bone block intraoperatively or postoperatively
Failure of graft to incorporate if the trough made in the scaphoid or lunate is not deep enough to cause punctate bleeding for the incorporation of the graft
Pin tract infections (which are treated with oral antibiotics)
Failure to achieve normal carpal alignment



