Scaphotrapezial-Trapezoid (STT) Fusion: A Comprehensive Surgical Guide
Key Takeaway
Scaphotrapezial-trapezoid (STT) fusion, or triscaphe arthrodesis, is a limited carpal fusion designed to stabilize the radial column while preserving functional wrist motion. Primary indications include isolated STT osteoarthritis and dynamic scapholunate instability. Successful outcomes rely on meticulous joint decortication, precise anatomical reduction of the scaphoid to prevent radioscaphoid impingement, and rigid Kirschner wire fixation augmented with cancellous bone graft to ensure robust union.
Comprehensive Introduction and Patho-Epidemiology
The scaphotrapezial-trapezoid (STT) fusion, originally conceptualized and popularized by H. Kirk Watson in the late twentieth century as the "triscaphe arthrodesis," remains one of the most mechanically profound limited carpal arthrodeses in the armamentarium of the orthopedic hand surgeon. The procedure is meticulously designed to surgically unite the scaphoid, trapezium, and trapezoid into a single, rigid biomechanical block. By effectively stabilizing the radial column of the carpus, the STT fusion halts the insidious progression of localized degenerative changes while preserving a highly functional arc of radiocarpal and midcarpal motion. Unlike total wrist arthrodesis, which sacrifices all radiocarpal and intercarpal kinematics for absolute pain relief, the STT fusion represents a sophisticated compromise, demanding a rigorous understanding of carpal mechanics to execute successfully.
The patho-epidemiology of STT joint dysfunction is deeply rooted in the unique mechanical stresses subjected to the radial column. Isolated STT osteoarthritis is the second most common form of degenerative joint disease in the wrist, surpassed only by trapeziometacarpal (basal joint) arthritis. It predominantly affects middle-aged to elderly females, often presenting bilaterally. The pathogenesis is typically driven by chronic, repetitive shear forces across the complex multi-planar articulation of the STT joint, exacerbated by subtle ligamentous laxity or occupational microtrauma. Over time, the articular cartilage undergoes fibrillation, fissuring, and eventual denudation, leading to subchondral sclerosis, osteophyte formation, and debilitating radial-sided wrist pain.
Furthermore, the STT fusion plays a pivotal role in the management of early-stage Scapholunate Advanced Collapse (SLAC). In the SLAC wrist, the rupture of the scapholunate interosseous ligament leads to a kinematic decoupling of the proximal carpal row. The scaphoid flexes palmarly while the lunate extends dorsally, creating a dorsal intercalated segment instability (DISI) deformity. If left untreated, this abnormal posture alters the contact mechanics between the scaphoid and the distal radius, leading to predictable, progressive arthrosis. By fusing the STT joint, the surgeon effectively locks the scaphoid to the stable distal carpal row, eliminating its pathological flexion and preventing the abnormal shear forces at the radioscaphoid articulation, provided that the articular cartilage at the scaphoid fossa remains pristine.
Despite its biomechanical elegance, triscaphe arthrodesis is notoriously technically demanding. It requires not only meticulous joint preparation to ensure a high rate of osteogenesis but also the precise spatial reduction of the scaphoid prior to fixation. Failure to anatomically position the scaphoid during the fusion process inevitably leads to disastrous kinematic consequences, including altered radiocarpal mechanics, severe dorsal impingement against the radial styloid, and accelerated adjacent-segment arthrosis. Consequently, mastery of this procedure requires an exhaustive comprehension of carpal pathoanatomy, rigorous preoperative templating, and flawless intraoperative execution.
Detailed Surgical Anatomy and Biomechanics
The scaphoid functions as a critical, dynamic tie-rod bridging the proximal and distal carpal rows. Osteologically, it is a complex, boat-shaped bone that lacks direct tendinous attachments, relying entirely on its intricate ligamentous constraints and articular morphology to govern its motion. The STT joint itself is a highly congruent, multi-planar articulation that facilitates the transmission of immense compressive and shear forces from the thumb and radial digits directly to the radiocarpal joint. The distal articular surface of the scaphoid is convex, articulating intimately with the concave proximal surfaces of both the trapezium and the trapezoid, creating a specialized joint that must accommodate both rotation and axial loading during power grip and pinch maneuvers.

Ligamentous anatomy surrounding the STT joint is paramount to understanding its inherent stability and the consequences of its surgical obliteration. The palmar STT ligaments are robust structures that resist dorsal translation of the distal carpal row, while the dorsal STT capsule is relatively thin. More proximally, the scapholunate interosseous ligament and the extrinsic palmar radiocarpal ligaments (specifically the radioscaphocapitate ligament) dictate the resting posture of the scaphoid. During normal wrist kinematics, particularly the "dart-thrower's motion" (coupled radial deviation/extension to ulnar deviation/flexion), the scaphoid exhibits a remarkable degree of independent motion. It flexes during radial deviation to avoid impingement against the radial styloid and extends during ulnar deviation to span the carpus.
When the STT joint is surgically fused, the fundamental biomechanics of the radial column are permanently altered. The scaphoid is inextricably locked to the distal carpal row (trapezium and trapezoid), effectively eliminating its ability to flex and extend independently. Consequently, the entire newly formed triscaphe unit must move synchronously with the capitate and the rest of the distal carpal row. This kinematic shift forces the radiocarpal joint to accommodate all subsequent flexion and extension of the radial column. While this successfully unloads the midcarpal joint and stabilizes the scaphoid, it places increased mechanical demand on the radioscaphoid articulation.
The most critical biomechanical parameter during STT fusion is the sagittal alignment of the scaphoid. If the scaphoid is inadvertently fused in an excessively extended (vertical or longitudinal) position, its proximal pole will abruptly impinge against the dorsal rim of the radial styloid during active wrist extension. This dorsal impingement acts as a mechanical block, severely limiting wrist extension, causing intractable pain, and rapidly accelerating degenerative changes at the radiocarpal joint. Conversely, if the scaphoid is fused in excessive flexion, it limits wrist flexion and can lead to midcarpal impingement. Therefore, achieving an anatomical scaphoid angle—typically between 45 and 60 degrees relative to the longitudinal axis of the radius—is the absolute sine qua non of a successful STT fusion.
Exhaustive Indications and Contraindications
The decision to proceed with an STT fusion must be based on a rigorous clinical and radiographic evaluation, as the procedure is highly specific in its indications and unforgiving in the presence of contraindications. The primary indication is isolated STT osteoarthritis. Patients typically present with insidious onset, progressive radial-sided wrist pain that is profoundly exacerbated by radial deviation, power pinch, and thumb loading. Clinical examination often reveals localized tenderness directly over the STT joint, distal to the anatomic snuffbox, and a positive STT grind test. Radiographically, this presents as joint space narrowing, subchondral sclerosis, and osteophyte formation strictly limited to the articulation between the scaphoid, trapezium, and trapezoid.
Another classic indication is the early management of Scapholunate Advanced Collapse (SLAC), specifically Stage I and early Stage II. In these scenarios, the scapholunate ligament is ruptured, and the scaphoid is dynamically or statically subluxated, but the degenerative changes are strictly confined to the radial styloid or the very distal aspect of the scaphoid fossa. By fusing the STT joint, the surgeon stabilizes the scaphoid, prevents its pathological flexion, and theoretically halts the progression of the SLAC wrist. Furthermore, STT fusion is selectively utilized in Stage III Kienböck’s disease. In this application, the fusion acts as a mechanical offloading procedure; by locking the radial column, compressive forces are preferentially transmitted through the scaphoid and radius, thereby decreasing the mechanical burden on the collapsing, avascular lunate.
However, the contraindications for STT fusion are absolute and must be strictly respected to avoid catastrophic postoperative outcomes. The most critical contraindication is the presence of radioscaphoid arthritis. If there is any evidence of cartilage denudation, subchondral cyst formation, or sclerosis at the proximal pole of the scaphoid or the scaphoid fossa of the distal radius, an STT fusion will dramatically exacerbate the patient's pain. Because the fusion forces the radiocarpal joint to bear the entirety of the radial column's motion, a pre-existing arthritic radioscaphoid joint will rapidly deteriorate. In such instances, salvage procedures such as a four-corner fusion or proximal row carpectomy (PRC) are mandatory.
Below is a comprehensive table detailing the indications and contraindications for STT fusion, alongside the underlying clinical rationale.
| Clinical Condition | Status for STT Fusion | Clinical Rationale and Biomechanical Justification |
|---|---|---|
| Isolated STT Osteoarthritis | Primary Indication | Eliminates painful micro-motion at the arthritic STT articulation while preserving functional radiocarpal and midcarpal kinematics. |
| SLAC Wrist (Stage I / Early Stage II) | Primary Indication | Stabilizes the pathologically flexing scaphoid, correcting the DISI deformity and preventing progression of radiocarpal arthrosis, provided the scaphoid fossa is pristine. |
| Kienböck’s Disease (Stage III) | Secondary Indication | Alters load transmission across the carpus. By fusing the radial column, forces bypass the central column, mechanically unloading the fragmented lunate. |
| Midcarpal Instability (Palmar) | Selective Indication | Restores stability to the radial column in highly selected cases of dynamic midcarpal instability where conservative management has failed. |
| Radioscaphoid Arthritis (SLAC Stage III) | Absolute Contraindication | Fusing the STT joint forces all radial column motion through the radioscaphoid joint. Pre-existing arthritis here will rapidly accelerate, causing severe pain and stiffness. |
| Pancarpal Arthritis / Rheumatoid Arthritis | Absolute Contraindication | Inflammatory arthropathies involve global cartilage destruction and poor bone stock, leading to high nonunion rates and failure. Total wrist arthrodesis is preferred. |
| Severe Osteopenia / Osteoporosis | Relative Contraindication | Inadequate cancellous bone stock compromises the rigid fixation required for intercarpal arthrodesis, significantly increasing the risk of hardware failure and nonunion. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful triscaphe arthrodesis. The process begins with exhaustive radiographic imaging. Standard posteroanterior (PA), lateral, and oblique views of the wrist are mandatory. A clenched-fist PA view is particularly useful to dynamically assess scapholunate diastasis and the extent of scaphoid rotary subluxation. However, plain radiography frequently underestimates the true spatial extent of carpal arthrosis. Therefore, a high-resolution, non-contrast Computed Tomography (CT) scan with sagittal and coronal reconstructions is highly recommended. The CT scan allows the surgeon to meticulously map the precise location of subchondral cysts, evaluate the bone stock available for fixation, and definitively rule out occult degenerative changes at the radioscaphoid joint.
H. Kirk Watson outlined five foundational principles that must be meticulously templated preoperatively and strictly observed intraoperatively to achieve a successful triscaphe arthrodesis. First, careful planning using the aforementioned advanced imaging is non-negotiable. Second, the surgeon must minimize the fused joints; only the scaphoid, trapezium, and trapezoid should be included in the fusion mass to preserve maximum residual carpal motion. Third, adequate autologous cancellous bone grafting is mandatory; allograft or synthetic substitutes yield unacceptably high nonunion rates in limited carpal fusions. Fourth, the external dimensions of the fused triscaphe unit must perfectly equal the external dimensions of the same bones in their native, normal state. Over-distraction or collapse of the STT space alters the kinematics of the entire carpus. Fifth, selective pinning must be employed; fixation wires must only cross the joints intended for fusion, avoiding inadvertent tethering of the radiocarpal or trapeziometacarpal joints.
Patient positioning and anesthesia are critical for optimal surgical execution. The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) combined with intravenous sedation, though general anesthesia may be utilized based on patient preference or comorbidities. The patient is positioned supine with the operative extremity extended on a specialized, radiolucent hand table. This ensures unimpeded access for the fluoroscopy C-arm, which must be positioned to allow seamless transition between PA and lateral views without manipulating the sterile field.
A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg (or 100 mm Hg above systolic pressure) following exsanguination of the limb with an Esmarch bandage. The hand, wrist, and forearm are prepped with a chlorhexidine-based solution and draped in a standard sterile fashion. The surgeon must ensure that the thumb and fingers remain exposed to assess digital alignment and tension during the reduction and pinning phases. A sterile marking pen is used to outline the anatomic landmarks: the radial styloid, Lister’s tubercle, the base of the first metacarpal, and the anticipated course of the superficial radial nerve.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Exposure, and Joint Preparation
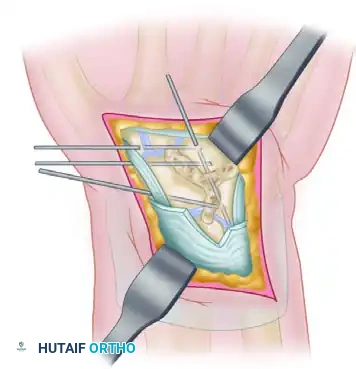
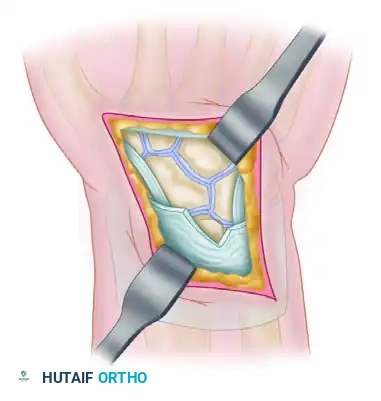
The surgical approach to the STT joint requires precise dissection to avoid iatrogenic injury to critical neurovascular structures. A transverse or slightly curved longitudinal incision is made on the dorsum of the wrist, centered directly over the STT articulation, typically just distal to the radial styloid. As the dissection proceeds through the subcutaneous tissues, the surgeon must meticulously identify and gently retract the delicate dorsal sensory branches of the superficial radial nerve, along with the accompanying dorsal venous network. The extensor retinaculum is then identified and opened longitudinally along the course of the extensor pollicis longus (EPL) tendon within the third dorsal compartment. The EPL is transposed radially to protect it and enhance exposure.
The wrist capsule is subsequently exposed. While the standard approach enters the capsule between the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) tendons, Kleinman’s modification offers superior visualization. By entering the capsule between the first and second dorsal extensor compartments, the surgeon gains excellent, direct exposure of the adjacent surfaces of the STT joint while allowing safe, direct retraction of the radial artery. The STT joint capsule is incised, and the capsulotomy is extended proximally to explicitly expose the proximal articular surface of the scaphoid and the scaphoid fossa of the radius. This is the final, definitive intraoperative checkpoint to rule out radioscaphoid arthrosis before committing to the fusion.
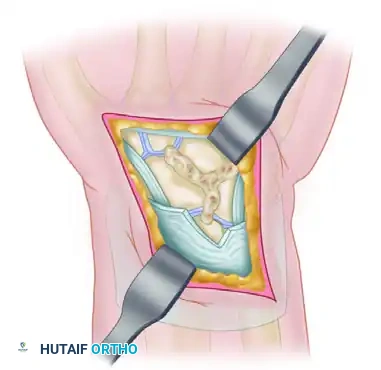
Preparation of the fusion bed is a meticulous process. Using a combination of fine rongeurs, sharp 4-mm osteotomes, and a high-speed 2.0-mm fluted burr, the surgeon removes the articular cartilage and subchondral bone from the opposing surfaces of the trapezium, trapezoid, and the distal pole of the scaphoid. Continuous chilled saline irrigation must be utilized during burring to prevent thermal necrosis of the underlying osteocytes. The decortication must proceed down to healthy, punctate bleeding cancellous bone to optimize the osteogenic potential of the fusion bed. Adhering to Kleinman’s clinical pearl, the surgeon should aim to remove only the dorsal two-thirds of the articular surfaces. Preserving the palmar one-third of the joint acts as a structural buttress, maintaining native carpal height and preventing the disastrous volar collapse of the fusion mass during compression.
Scaphoid Reduction and Bone Grafting
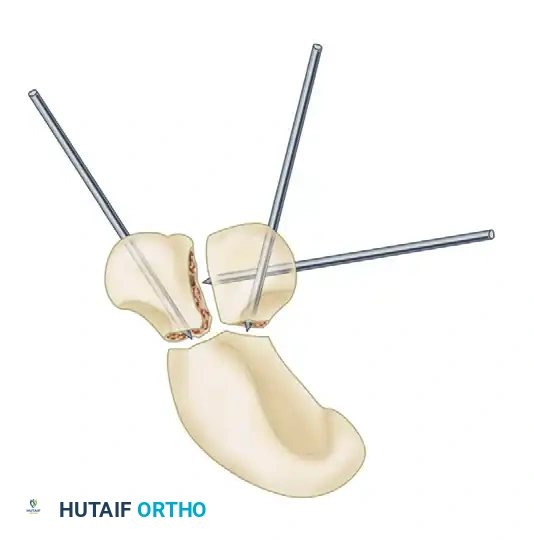
Anatomical reduction of the scaphoid is undeniably the most critical biomechanical step of the entire procedure. The scaphoid must be rotated out of its pathologically flexed posture. A robust, curved elevator or a specialized dental pick is introduced palmar to the distal neck of the rotated scaphoid. Using controlled leverage, the surgeon gently dorsiflexes the distal pole. This maneuver elevates the distal scaphoid, reducing it to its anatomical posture, and simultaneously secures the proximal pole congruently within the scaphoid fossa of the radius. The longitudinal axis of the scaphoid must be meticulously set to an angle of 45 to 60 degrees relative to the longitudinal axis of the radius. Any angle less than 30 degrees indicates excessive longitudinal (vertical) orientation, which will inevitably lead to severe radioscaphoid impingement during postoperative wrist extension.
Once the scaphoid is anatomically reduced, autologous bone graft is harvested. Given the high nonunion rates associated with limited carpal arthrodeses, dense, autologous cancellous bone is mandatory. This is most frequently obtained from the ipsilateral distal radius via a separate cortical window between the ECRL and the extensor pollicis brevis (EPB), or from the iliac crest if a larger volume is required. The harvested cancellous bone is densely packed into the decorticated STT joint spaces. The surgeon must ensure that the external dimensions of the newly grafted fusion unit perfectly match the native wrist; overstuffing the joint will cause over-distraction and alter midcarpal kinematics.
Kirschner Wire Fixation
Fixation of the triscaphe unit is typically achieved using three robust 0.045-inch or 0.062-inch Kirschner wires (K-wires). Following Watson’s highly effective recommendation, the pins are initially preset. The K-wires are passed in a retrograde fashion out through the raw, decorticated bony surfaces of the trapezium and trapezoid, exiting the dorsal skin, before the final reduction and grafting are completed.
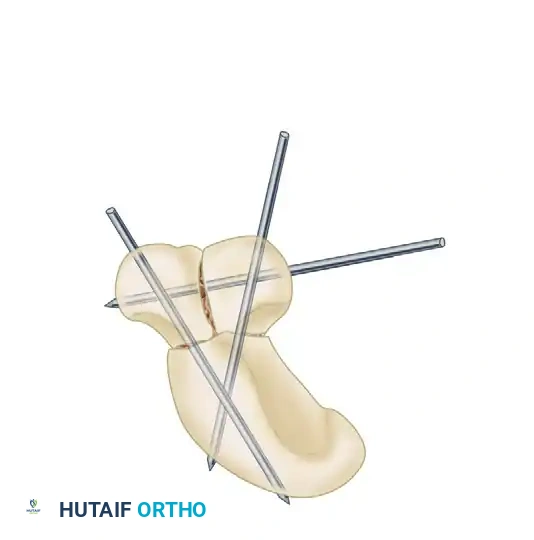
With the scaphoid held in its perfect anatomical reduction (distal pole elevated, proximal pole seated securely in the fossa), and the graft densely packed, the preset pins are driven across the fusion site in an antegrade direction. Typically, two pins are driven from the trapezoid directly into the dense bone of the scaphoid, and one pin is passed transversely across the trapezium-trapezoid articulation to lock the distal block.
Intraoperative fluoroscopy is absolutely essential at this juncture. The surgeon must obtain perfect PA and lateral views to confirm that the scaphoid angle is correct, the joint spaces are maintained, and critically, that no pins have inadvertently violated the radiocarpal or midcarpal joints. The K-wires are then cut just beneath the skin to prevent pin-tract infections while allowing for relatively easy removal in the outpatient clinic once radiographic union is achieved.
Alternative Limited Wrist Arthrodeses
While STT fusion is highly effective for specific radial column pathology, other limited intercarpal fusions are utilized depending on the precise pattern of carpal instability or degeneration. These include arthrodesis of the scaphocapitate, scaphocapitolunate, lunotriquetral, and radiolunate joints. It is imperative for the operating surgeon to note that all limited carpal fusions carry a significant complication profile, demanding exact technique.
For broader midcarpal instability or more extensive degenerative patterns that involve the capitolunate joint, a scaphocapitolunate (SCL) fusion may be indicated. The fundamental principles of joint decortication, autologous grafting, and rigid pinning remain entirely consistent with those of the STT fusion.
The approach for an SCL fusion utilizes a dorsal longitudinal or slightly oblique incision extending from the ulnar aspect of the distal radius directly to the distal pole of the scaphoid.
Deep dissection exposes the scaphocapitolunate articulation between the third and fourth dorsal extensor compartments. The capsule is typically opened in a broad, inverted-T fashion to allow visualization of all three bones simultaneously.
The articular surfaces of the scaphoid, capitate, and lunate are rigorously decorticated down to bleeding subchondral bone. The resulting voids are then densely packed with the harvested autologous cancellous bone graft to ensure a continuous osteogenic bed.
Rigid fixation is achieved using multiple K-wires, meticulously placed in a triangular or divergent configuration to neutralize the complex, multi-planar shear and bending forces across the scaphoid, capitate, and lunate during the healing phase.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, scaphotrapezial-trapezoid fusion is associated with a formidable complication profile. The literature consistently demonstrates that limited carpal fusions are technically unforgiving. The most frequent and challenging complication is nonunion (pseudoarthrosis). The STT joint has a relatively small cross-sectional surface area for fusion, and the scaphoid’s tenuous, retrograde intraosseous vascular supply makes it particularly susceptible to avascularity during extensive decortication. Nonunion rates in STT fusion range from 5% to 15% in major series. It is often the result of inadequate cartilage removal, failure to decorticate to bleeding bone, thermal necrosis from high-speed burring without irrigation, or the use of allograft instead of autologous cancellous bone.
Another severe complication is iatrogenic radiocarpal impingement and accelerated adjacent-segment arthrosis. This is almost exclusively an iatrogenic error resulting from malpositioning the scaphoid during fixation. If the scaphoid is pinned in a vertical (extended) position (scaphoid angle < 30 degrees), the proximal pole will mechanically abut the dorsal rim of the radius during wrist extension. This not only severely restricts range of motion but also generates immense focal contact pressures, leading to rapid, painful degeneration of the radioscaphoid joint. Furthermore, altered kinematics can lead to secondary trapeziometacarpal (basal joint) arthritis, as the fused triscaphe unit changes the load vectors acting on the base of the first metacarpal.
Hardware-related complications are also prevalent. Because STT fusions rely heavily on K-wire fixation, issues such as pin migration, superficial pin-tract infections, and hardware breakage are common. If pins are left protruding through the skin, the risk of deep infection tracking into the carpus increases significantly. Additionally, prominent dorsal pins can cause attritional wear and eventual rupture of the extensor tendons, particularly the EPL or ECRB. Complex Regional Pain Syndrome (CRPS) is a devastating, albeit less common, complication characterized by disproportionate pain, autonomic dysfunction, and severe wrist stiffness, requiring immediate, aggressive multidisciplinary intervention.
When an STT fusion fails—either due to painful nonunion or the development of severe adjacent-segment arthrosis—salvage procedures are mandatory. The specific salvage operation depends on the precise nature of the failure. If a nonunion occurs without adjacent arthrosis, a revision STT fusion with iliac crest bone grafting and rigid internal fixation (e.g., using headless compression screws instead of K-wires) may be attempted. However, if radioscaphoid or midcarpal arthritis has developed, the surgeon must abandon the limited fusion concept. Conversion to a Scaphoid Excision and Four-Corner Arthrodesis (lunate, capitate, hamate, triquetrum) or a Proximal Row Carpectomy (PRC) is required to eliminate the arthritic articulations while preserving a functional, albeit reduced, arc of motion.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion (Pseudoarthrosis) | 5% - 15% | Inadequate decortication, thermal necrosis, poor graft quality, smoking, premature pin removal. | Revision bone grafting with rigid internal fixation; conversion to Four-Corner Fusion if symptomatic. |
| Radiocarpal Impingement / Arthrosis | 10% - 20% | Scaphoid fused in excessive extension (vertical orientation); pre-existing occult radioscaphoid OA. | Proximal Row Carpectomy (PRC) or Four-Corner Fusion; radial styloidectomy for localized impingement. |
| Hardware Migration / Infection | 5% - 10% | Poor pin purchase, superficial pin placement, patient non-compliance with immobilization. | Early pin removal, oral/IV antibiotics; surgical debridement if deep joint space infection occurs. |
| Trapeziometacarpal (Basal Joint) OA | 5% - 12% | Altered load vectors on the 1st metacarpal base; over-distraction of the STT joint space. | Trapeziectomy with or without Ligament Reconstruction and Tendon Interposition (LRTI). |
| Complex Regional Pain Syndrome (CRPS) | 2% - 5% | Iatrogenic nerve traction (superficial radial nerve), tight cast application, prolonged immobilization. | Aggressive hand therapy, sympathetic nerve blocks, gabapentinoids, vitamin C prophylaxis. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following an STT fusion is a delicate, phased process that must meticulously balance the absolute mechanical requirement for rigid immobilization to achieve bony consolidation with the clinical imperative to prevent debilitating, permanent wrist stiffness. The rehabilitation timeline is heavily dependent on the surgeon's intraoperative assessment of fixation rigidity and the patient's radiographic progression of healing.
