Surgical Release of the Sternocleidomastoid Muscle for Congenital Muscular Torticollis

Key Takeaway
Welcome, fellows, to an in-depth surgical masterclass on the release of the sternocleidomastoid (SCM) muscle for congenital muscular torticollis. We'll meticulously cover preoperative planning, precise patient positioning, detailed surgical anatomy including neurovascular structures, and a granular, real-time breakdown of the unipolar and bipolar release techniques. Our focus is on achieving optimal functional and cosmetic outcomes while navigating potential pitfalls.
Welcome, fellows, to the operating theater. Today, we are addressing a common yet critical pediatric orthopedic condition: congenital muscular torticollis (CMT). Our focus will be on the surgical release of the sternocleidomastoid (SCM) muscle, a procedure that, when performed meticulously, can dramatically improve a child's quality of life, restoring neck mobility and preventing long-term craniofacial asymmetry. The nuances of this operation require a profound respect for cervical anatomy, a disciplined surgical technique, and a comprehensive understanding of the underlying pathophysiology.
Comprehensive Introduction and Patho-Epidemiology
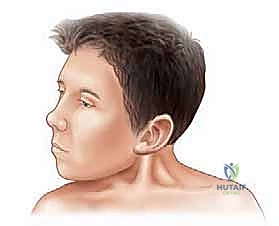
Congenital muscular torticollis is the third most common congenital musculoskeletal anomaly, superseded only by developmental dysplasia of the hip (DDH) and congenital talipes equinovarus (clubfoot). With an incidence ranging widely in the literature from 0.4% to 1.3% of live births, it is a condition every pediatric orthopedic surgeon will encounter frequently. The hallmark of the disorder is a unilateral contracture of the SCM muscle, compelling the infant’s head into characteristic lateral flexion toward the ipsilateral side and rotation toward the contralateral side.
The precise etiology of CMT remains a subject of academic debate, though it is generally accepted to be multifactorial, involving a combination of intrauterine compartment syndrome and mechanical birth trauma. The leading theory posits that intrauterine malposition—exacerbated by factors such as oligohydramnios, primiparity, and macrosomia—leads to localized ischemia of the SCM muscle. This ischemic event triggers a cascade of muscle necrosis and subsequent fibrosis. Alternatively, difficult or traumatic deliveries, particularly breech presentations or those requiring forceps, may induce a stretch injury or direct hematoma within the muscle belly. This localized trauma initiates a compartment syndrome within the investing layer of the deep cervical fascia, ultimately culminating in fibromatosis colli.
Clinically, the condition often presents within the first two to four weeks of life as a palpable, firm, non-tender "pseudotumor" located in the inferior or middle third of the SCM muscle belly. Histologically, this mass is devoid of true neoplastic cells; rather, it is composed of dense, proliferating fibroblasts and interspersed residual degenerating muscle fibers. Over the subsequent six to twelve months, this mass typically regresses, leaving behind a dense, non-yielding fibrotic band. If left untreated, the persistent mechanical tethering leads to progressive secondary deformities, including plagiocephaly (flattening of the contralateral occiput and ipsilateral frontal bossing), facial asymmetry (hemifacial hypoplasia), and eventual compensatory cervicothoracic scoliosis.

Detailed Surgical Anatomy and Biomechanics
A flawless surgical release is predicated upon an intimate, three-dimensional understanding of the cervical anatomy. The sternocleidomastoid muscle serves as a critical anatomical landmark, effectively dividing the neck into the anterior and posterior triangles. The muscle is enveloped by the superficial layer of the deep cervical fascia, which splits to enclose the muscle belly before reuniting.
Muscular Origins and Insertions
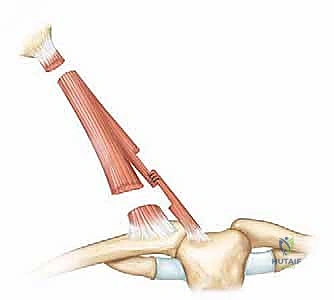
The SCM is a robust, paired, two-headed muscle. The sternal head is tendinous and rounded, originating from the anterior and superior surface of the manubrium sterni. The clavicular head is more fleshy and broad, originating from the superior surface of the medial third of the clavicle. These two heads are separated by a small triangular interval (the supraclavicular fossa) before they converge as they ascend obliquely across the neck. The muscle inserts via a strong aponeurosis into the lateral surface of the mastoid process of the temporal bone and the lateral half of the superior nuchal line of the occipital bone. Biomechanically, unilateral contraction results in ipsilateral lateral flexion and contralateral rotation of the head. Bilateral contraction acts to extend the upper cervical spine and flex the lower cervical spine, protruding the chin forward.
Critical Neurovascular Relationships
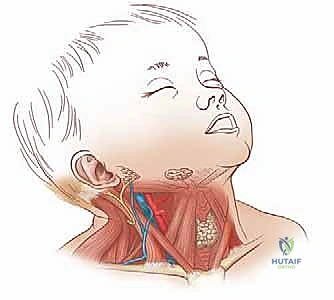
The neurovascular anatomy surrounding the SCM is unforgiving, and iatrogenic injury can be devastating. The spinal accessory nerve (Cranial Nerve XI) is the most critical structure at risk during the proximal dissection. It exits the jugular foramen, descends deep to the posterior belly of the digastric muscle, and pierces the deep surface of the SCM in its superior third to provide motor innervation. It then traverses obliquely through the muscle belly, exiting the posterior border at Erb’s point to supply the trapezius. Injury to CN XI results in profound shoulder dysfunction, characterized by a drooping shoulder, scapular winging, and weakness in shoulder abduction.
Superficially, the greater auricular nerve (derived from C2 and C3 spinal nerves) curls around the posterior border of the SCM near Erb's point and ascends vertically across the muscle to supply sensory innervation to the parotid gland region, the mastoid, and the auricle. Transection leads to distressing permanent numbness. The external jugular vein (EJV) descends vertically across the superficial surface of the SCM, deep only to the platysma. It is a major source of hemorrhage if inadvertently transected during the distal superficial dissection. Deep to the SCM lies the carotid sheath, containing the common carotid artery, internal jugular vein, and vagus nerve. The surgical plane must remain strictly within or superficial to the SCM fascial envelope to avoid catastrophic vascular injury.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be made judiciously, following a rigorous trial of conservative management. Physical therapy, consisting of dedicated, parent-assisted passive stretching (lateral bending away from the affected side and rotation toward it), is highly efficacious, yielding a success rate of over 90% when initiated before one year of age.
Operative Indications
Surgical release is strictly reserved for recalcitrant cases or late presentations. The primary indication is a persistent, clinically significant deformity (head tilt and restricted range of motion) that has failed to improve after a minimum of six months of compliant, supervised physical therapy, typically in a child who has reached one year of age. Furthermore, children presenting late (beyond 12 to 18 months of age) with established severe contractures, a palpable tight fibrous band, and a range of motion deficit exceeding 10 to 15 degrees in lateral flexion or rotation are immediate candidates for surgery. Early operative intervention in these late presenters is critical to halt the progression of facial asymmetry and plagiocephaly, which become increasingly refractory to remodeling as the child ages.
Contraindications and Differential Diagnosis
Surgery is absolutely contraindicated if the diagnosis of congenital muscular torticollis is in doubt. Torticollis is a physical sign, not a singular diagnosis, and a myriad of life-threatening or vision-threatening conditions can mimic CMT. Ophthalmologic torticollis, driven by superior oblique palsy (CN IV palsy) or strabismus, typically presents after three months of age when visual tracking matures; the head tilt is a compensatory mechanism to maintain binocular vision and resolves when the affected eye is patched. Neurologic etiologies, particularly posterior fossa tumors (e.g., medulloblastoma, ependymoma) or syringomyelia, must be excluded, especially if accompanied by atypical neurological signs, insidious onset, or pain. Orthopedic anomalies such as Klippel-Feil syndrome, atlantoaxial rotatory subluxation (AARS), or congenital cervical scoliosis contraindicate standard SCM release.
| Clinical Scenario | Indication Status | Rationale / Required Action |
|---|---|---|
| Infant < 1 year, mild band | Contraindicated | First-line treatment is rigorous physical therapy. High spontaneous resolution rate. |
| Child > 1 year, failed 6mo PT | Indicated | Fibrotic band is established; conservative measures exhausted. Prevents facial asymmetry. |
| Late presentation (> 2 years) | Indicated | High likelihood of permanent craniofacial deformity. Often requires bipolar release or Z-plasty. |
| Torticollis with pain/fever | Contraindicated | Suspect Grisel syndrome, retropharyngeal abscess, or osteomyelitis. Requires urgent medical/ENT workup. |
| Torticollis resolving with eye patch | Contraindicated | Indicates ophthalmologic etiology (e.g., CN IV palsy). Refer to Pediatric Ophthalmology. |
| Associated neurological deficits | Contraindicated | High suspicion for posterior fossa tumor or syrinx. Urgent MRI required. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning ensures both the safety of the procedure and the adequacy of the surgical release. The preoperative clinical evaluation must document the exact degrees of restricted lateral flexion and rotation, as well as the presence and severity of facial asymmetry and plagiocephaly.
Imaging Protocols
Standardized imaging is mandatory to rule out osseous anomalies. Cervical spine radiographs, including anteroposterior (AP), lateral, and open-mouth odontoid views, are non-negotiable. These films rule out congenital fusions (Klippel-Feil), hemivertebrae, and atlantoaxial instability. In infants presenting with a palpable mass, ultrasonography is highly useful to confirm fibromatosis colli and differentiate it from branchial cleft cysts, cystic hygromas, or solid neoplasms. Furthermore, given the well-documented 8% to 20% coexistence rate of CMT with developmental dysplasia of the hip (DDH), a screening hip ultrasound (or AP pelvis radiograph in older toddlers) is a mandatory component of the preoperative workup. Magnetic Resonance Imaging (MRI) of the brain and cervical spine is reserved for patients with atypical presentations, progressive symptoms, pain, or any focal neurological deficits.
Anesthesia and Positioning
The procedure is performed under general anesthesia. Airway management can be challenging in patients with severe, fixed cervical deformities; the anesthesia team must be prepared with fiberoptic intubation capabilities. Crucially, the endotracheal tube should be secured on the unaffected side of the mouth. This seemingly minor detail prevents the tube from kinking or obstructing the surgical field during the extreme lateral flexion and rotation maneuvers required to assess the adequacy of the release intraoperatively.
The patient is placed in the supine position on the operating table. A small, firm sandbag or a rolled towel is placed transversely under the scapula and shoulder of the affected side. This elevation allows the head to gently drop back into extension, placing the SCM under maximal tension. The head is then laterally flexed toward the unaffected side and rotated toward the affected side, further bowstringing the fibrotic SCM band, making its margins prominent and easily palpable. The surgical prep must be wide—extending from the lower mandible to the nipple line, and from the anterior midline to the posterior trapezius border. Draping must be meticulous yet flexible; sterile towels should be utilized in a manner that allows the surgeon to freely manipulate the head and neck through a full, unrestricted range of motion during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical objective is a complete resection of the fibrotic tether while preserving the normal cosmetic contour of the neck and avoiding neurovascular catastrophe. While a unipolar release (distal only) may suffice for mild cases, a bipolar release (both distal and proximal) is the gold standard for moderate to severe deformities. In older children, a Z-plasty lengthening of the distal sternal head is often employed to preserve the V-neck contour.
Step 1: The Distal Incision and Superficial Dissection
We begin at the distal pole. A transverse incision, approximately 3 to 4 cm in length, is made within the Langer’s lines of the neck, situated exactly 1 to 2 cm superior to the clavicle and centered over the palpable sternal and clavicular heads of the SCM. Placing the incision directly over the clavicle is a common error that results in a hypertrophic, tethered, and highly visible scar.
Using a #15 blade, the skin and subcutaneous fat are incised. The platysma muscle, which runs longitudinally in this region, is identified and carefully divided transversely in line with the skin incision. It is imperative to identify and protect the external jugular vein, which typically runs vertically just superficial to the SCM fascia or within the lateral margin of the incision. If the EJV is in the way, it should be gently mobilized and retracted laterally; if it severely impedes the approach, it must be meticulously double-ligated and divided.

Step 2: Distal SCM Release
Once the platysma is retracted, the investing layer of the deep cervical fascia is incised, exposing the glistening, fibrotic bands of the sternal and clavicular heads. Using fine Metzenbaum scissors or a right-angle clamp, a safe plane is bluntly developed deep to the SCM but superficial to the carotid sheath. The surgeon must stay strictly within the fascial envelope of the muscle.
The clavicular head is often broader than anticipated, sometimes extending to the middle third of the clavicle. A right-angle clamp is passed deep to the clavicular head, and the muscle is divided using electrocautery to ensure hemostasis. The sternal head is similarly isolated and divided. As the muscle is transected, the underlying deep cervical fascia will often present as a secondary tethering band; this must also be carefully divided. The surgeon should visually confirm that the carotid sheath and its contents remain undisturbed deep to the operative field.
Step 3: The Proximal Incision
Attention is then directed to the proximal insertion. A 3 cm transverse incision is made just inferior to the tip of the mastoid process, carefully hidden within the natural skin creases or the hairline. The subcutaneous tissue and platysma are divided to expose the proximal SCM, which is often a thick, tendinous band at this level.
Step 4: Proximal Release and Nerve Protection
The proximal release is fraught with danger due to the proximity of the spinal accessory nerve. The nerve typically enters the deep surface of the SCM approximately 3 to 5 cm inferior to the mastoid tip. Therefore, the proximal release must be performed as close to the mastoid insertion as anatomically possible.
The muscle is carefully mobilized. A right-angle clamp is passed deep to the tendinous insertion, staying intimately on the bone of the mastoid process. The muscle is divided completely. The surgeon must be vigilant for the greater auricular nerve, which crosses the posterior border of the SCM slightly more distally; retraction should be gentle to avoid neuropraxia.


Step 5: Intraoperative Assessment and Closure
Following the bipolar release, the anesthesiologist removes the shoulder roll. The surgeon then takes the patient's head and passively maneuvers it through a full range of motion. The goal is to achieve lateral flexion such that the ear touches the ipsilateral shoulder, and rotation such that the chin reaches the contralateral shoulder without resistance.
If restriction persists, the surgeon must systematically palpate the neck for residual tight bands. Often, the anterior border of the trapezius, the scalene fascia, or the deep cervical fascia requires additional fractional release. Once full, unrestricted motion is confirmed, the wounds are irrigated copiously. Hemostasis is achieved with bipolar cautery. The platysma is meticulously repaired with interrupted absorbable sutures (e.g., 4-0 Vicryl) to prevent a widened scar. The skin is closed with a running subcuticular suture (e.g., 5-0 Monocryl) and reinforced with Steri-Strips.
Complications, Incidence Rates, and Salvage Management
While SCM release is highly successful, the potential for complications remains significant due to the complex regional anatomy. Meticulous technique and a deep understanding of salvage pathways are essential for the operating surgeon.
The most devastating complication is iatrogenic nerve injury. Injury to the spinal accessory nerve (CN XI) occurs in less than 1% of cases but results in severe, permanent morbidity. If a CN XI transection is recognized intraoperatively, immediate primary epineural repair using 8-0 or 9-0 nylon under microscopic magnification is mandatory. If recognized postoperatively, early exploration and nerve grafting may be required. Greater auricular nerve injury is more common, leading to numbness over the ear and jaw angle; while distressing, it is generally managed expectantly, as sensory overlap often compensates over time.
Vascular injuries, particularly to the external jugular vein, can obscure the surgical field and lead to postoperative hematoma. If the EJV is torn, it must be cleanly ligated; attempting to repair it in a pediatric patient is unnecessary and risks further bleeding. Deep vascular injury to the carotid artery or internal jugular vein is exceedingly rare but represents a life-threatening emergency requiring immediate pressure, vascular surgery consultation, and potential formal neck exploration.
Recurrence of the deformity or incomplete release occurs in 3% to 5% of cases, most frequently due to a failure to completely divide the broad clavicular head or the underlying deep cervical fascia. Recurrence requires a return to the operating room for a wider exploration, radical resection of the fibrotic scar tissue, and often a more aggressive release of surrounding fascial structures.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Spinal Accessory Nerve (CN XI) Injury | < 1% | Proximal release must be flush with the mastoid tip. Avoid deep dissection in the middle third of the SCM. | Immediate microsurgical epineural repair. Late recognition requires nerve grafting or tendon transfers (e.g., Eden-Lange procedure). |
| Greater Auricular Nerve Injury | 1 - 2% | Careful posterior border dissection. Avoid excessive traction near Erb's point. | Expectant management. Gabapentin for neuropathic pain if severe. Sensation often partially recovers. |
| External Jugular Vein Laceration | 2 - 4% | Careful superficial dissection post-platysma division. Identify and retract early. | Immediate double ligation with silk ties. Do not attempt primary repair. |
| Recurrent Deformity / Incomplete Release | 3 - 5% | Intraoperative ROM check is mandatory. Ensure deep cervical fascia and broad clavicular head are fully released. | Aggressive physical therapy. If refractory, revision surgery with radical scar excision and wide fascial release. |
| Hypertrophic Scarring / Loss of Neck Contour | 5 - 10% | Incision strictly in Langer's lines, 1-2 cm above clavicle. Consider Z-plasty in older children. | Silicone scar sheets, intralesional corticosteroid injections. Late scar revision by plastic surgery if functionally limiting. |
Phased Post-Operative Rehabilitation Protocols
The surgery itself represents only half of the therapeutic equation; an aggressive, meticulously phased postoperative rehabilitation protocol is an absolute prerequisite for maintaining the surgical correction and retraining the child's motor pathways.
Phase 1: Immediate Post-Operative Period (0 to 4 Weeks)
Immediately following surgery, the neck is placed in a soft cervical collar or, in older children with severe long-standing deformities, a custom-molded Minerva cast or a Tubular Orthosis for Torticollis (TOT) collar. The orthosis is designed to hold the head in slight overcorrection—flexed toward the unaffected side and rotated toward the affected side. During the first week, pain control is paramount to prevent muscle guarding. Gentle, active-assisted range of motion exercises are initiated once the incisions have healed, typically around post-operative day 7 to 10. Parents are instructed on proper positioning during sleep and feeding to encourage the child to look toward the newly released side.
Phase 2: Aggressive Stretching and Strengthening (4 to 12 Weeks)
At four weeks, the daytime use of the cervical orthosis is gradually weaned, though night-time wear may continue for up to three months. Formal physical therapy becomes aggressive. The therapist focuses on passive stretching to maintain the intraoperative range of motion, holding stretches for 15 to 30 seconds. Equally important is active strengthening of the contralateral SCM and the posterior cervical musculature. Because the child has spent their life compensating for the contracture, their neuromuscular control is fundamentally altered. Therapy involves visual tracking exercises, righting reflex stimulation, and prone positioning (tummy time) to build symmetrical cervical strength.
Phase 3: Long-Term Follow-Up and Remodeling (3 Months to 2 Years)
Long-term follow-up is critical. The surgeon must monitor the patient for any signs of recurrent contracture, which usually presents as a subtle loss of rotation before a visible head tilt returns. Furthermore, the remodeling of craniofacial asymmetry and plagiocephaly is monitored. In children operated on before the age of two, significant spontaneous remodeling of the skull and facial bones can be expected once the mechanical tether is removed. In older children, while the neck motion is restored, the facial asymmetry may be permanent, and expectations must be managed accordingly during preoperative counseling.
Summary of Landmark Literature and Clinical Guidelines
The management of congenital muscular torticollis has evolved significantly, guided by robust clinical literature. The landmark studies by Cheng et al. remain the cornerstone of our understanding regarding the timing of intervention. Their extensive prospective cohorts demonstrated that non-operative management with manual stretching is successful in over 90% of cases when initiated early. However, their data unequivocally showed that delaying surgery beyond one year of age in refractory cases leads to suboptimal cosmetic outcomes and a higher incidence of permanent facial asymmetry.
Furthermore, the American Academy of Pediatrics (AAP) and the Pediatric Orthopaedic Society of North America (POSNA) have established clear clinical practice guidelines emphasizing the necessity of early referral to physical therapy and the absolute requirement to rule out non-muscular causes of torticollis. The literature strongly supports the bipolar release over the unipolar release for all but the mildest deformities, as studies by Canale and others have shown a higher recurrence rate when the proximal tether is left intact. More recently, advancements in ultrasound imaging have allowed for better prognostication; infants with a larger volume of fibrotic tissue on initial ultrasound are now known to have a statistically higher likelihood of ultimately requiring surgical release.
