Radial Nerve Palsy Tendon Transfers: An Intraoperative Masterclass

Key Takeaway
Welcome, fellows, to an immersive surgical masterclass on tendon transfers for radial nerve palsy. We'll meticulously restore wrist, finger, and thumb extension, covering detailed anatomy, preoperative planning, and granular intraoperative execution. Learn precise donor harvest, optimal tensioning, and crucial neurovascular protection to achieve excellent functional outcomes for our patients.
Introduction and Epidemiology
Radial nerve palsy distal to the triceps innervation profoundly alters the biomechanics of the forearm and hand, resulting in predictable and highly debilitating motor deficits. The hallmark clinical presentation—characterized by the inability to actively extend the wrist, the metacarpophalangeal (MCP) joints of the fingers, and the thumb—is classically referred to as "drop wrist." The loss of active wrist extension secondarily impairs the mechanical advantage of the digital flexors. Without stable wrist extension to provide a tenodesis effect, the flexor tendons operate at a shortened functional length, significantly reducing grip strength and overall hand dexterity. Tendon transfers remain the gold standard reconstructive strategy for restoring function in patients with irreversible radial nerve palsy, or they can be utilized as an "internal splint" during prolonged nerve recovery.
The majority of radial nerve deficits result from traumatic injuries, with idiopathic, compressive (e.g., Saturday night palsy), and neoplastic etiologies representing a smaller subset. Traumatic radial nerve injury is most frequently associated with mid-to-distal third humeral shaft fractures. The nerve is particularly vulnerable in the Holstein-Lewis fracture pattern (a spiral fracture of the distal third of the humerus), where it can be tethered or lacerated as it pierces the lateral intermuscular septum. Iatrogenic injuries sustained during surgical exploration, open reduction and internal fixation (ORIF) of the humerus, or hardware removal also account for a significant proportion of radial nerve palsies.
The natural history and management of traumatic radial nerve palsy depend heavily on the mechanism and severity of the injury (Seddon and Sunderland classifications). Neurapraxic lesions typically follow low-energy blunt trauma or transient compression and generally demonstrate spontaneous recovery within three to four months. Conversely, high-energy trauma, open fractures, or penetrating injuries are more likely to result in axonotmesis or neurotmesis, necessitating early surgical exploration and potential microsurgical repair. When primary nerve repair, autologous nerve grafting, or nerve transfers fail to yield functional reinnervation after 12 to 18 months, irreversible motor endplate degradation and muscle fibrosis occur. In these chronic scenarios, tendon transfers become the definitive and necessary reconstructive strategy to restore upper extremity biomechanics and functional independence.
Surgical Anatomy and Biomechanics
Radial Nerve Course and Innervation Sequence
A meticulous understanding of radial nerve anatomy and its highly predictable innervation sequence is paramount for differentiating isolated nerve injuries from primary myotendinous disruptions, localizing the level of the lesion, and monitoring clinical recovery. Originating from the posterior cord of the brachial plexus, the radial nerve carries fibers from the C5 through T1 nerve roots. It exits the axilla and spirals around the posterior humerus within the spiral groove (radial sulcus), descending between the medial and lateral heads of the triceps. It then pierces the lateral intermuscular septum to enter the anterior compartment of the arm.


The sequence of muscle innervation follows a strict proximal-to-distal pattern. Proximal to the elbow joint, the proper radial nerve innervates the brachioradialis (BR) and the extensor carpi radialis longus (ECRL). In a subset of patients, it also provides direct branches to the extensor carpi radialis brevis (ECRB). At the level of the radiocapitellar joint, the nerve bifurcates into the superficial sensory branch (providing sensation to the dorsal radial hand) and the deep motor branch, which continues as the posterior interosseous nerve (PIN).


The PIN passes beneath the tendinous arch of the supinator muscle—the arcade of Frohse—where it is highly susceptible to compression. Upon exiting the supinator, the PIN innervates the remaining extensor musculature in the following general anatomical order: extensor carpi radialis brevis (ECRB), extensor digitorum communis (EDC), extensor carpi ulnaris (ECU), extensor digiti minimi (EDM), abductor pollicis longus (APL), extensor pollicis longus (EPL), extensor pollicis brevis (EPB), and finally, the extensor indicis proprius (EIP). Recognizing that the motor point for each nerve branch is consistently located just proximal to the myotendinous junction is critical during both nerve exploration and donor muscle mobilization.
Biomechanics of Tendon Transfers
Successful tendon transfer surgery relies on strict adherence to established biomechanical principles (often attributed to Boyes and Brand). These principles dictate that the donor muscle must possess adequate strength, excursion (amplitude), and a straight line of pull to achieve the desired functional outcome without creating secondary biomechanical deficits.

- Supple Joints: The recipient joints must possess full, unrestricted passive range of motion prior to transfer. A tendon transfer is designed to provide dynamic motion; it cannot overcome a fixed capsular or joint contracture.
- Donor Muscle Strength: The donor muscle must be Medical Research Council (MRC) grade 5. A muscle typically loses at least one MRC grade of strength following transfer due to altered resting length and vector changes. Therefore, transferring a sub-maximal muscle (Grade 4 or less) will result in functional failure.
- Amplitude and Excursion: The excursion of the donor tendon should closely match that of the recipient. Wrist extensors require approximately 33 mm of excursion, while digital extensors require approximately 50 mm. If a donor with lesser excursion (e.g., Flexor Carpi Radialis, ~30 mm) is used for digital extension, the surgeon and patient must rely on the dynamic tenodesis effect of the wrist to achieve full digital flexion and extension.
- Synergistic Function: Transferring synergistic muscles facilitates cortical plasticity and easier postoperative motor re-education. Wrist flexors naturally contract during active digital extension to stabilize the carpus; thus, using a wrist flexor (like the FCR) to power digital extensors is a highly synergistic and intuitive transfer.
- Straight Line of Pull: The transfer route should be as direct as possible. Acute angles decrease mechanical efficiency and increase friction, which can lead to early transfer failure or attenuation.
- Expendable Donor: The loss of the donor muscle's primary function must not result in a significant functional or cosmetic deficit.

Indications and Contraindications
Tendon transfers for radial nerve palsy are definitively indicated when spontaneous nerve recovery has failed, when the time elapsed since injury exceeds the viability window of motor endplates (typically 12 to 18 months), or when massive soft tissue and nerve destruction precludes primary repair or grafting.
In select cases, early tendon transfers may be performed as an "internal splint" simultaneously with nerve repair or grafting. This provides the patient with immediate functional restoration, eliminates the need for cumbersome and often non-compliant external dynamic orthoses, and prevents flexion contractures while awaiting slow axonal regeneration (which progresses at approximately 1 mm per day).
Contraindications include severe joint arthrofibrosis, inadequate donor muscle strength, active regional infection, and poor soft tissue beds (e.g., severe scarring or skin grafting directly over the planned transfer route) that would impede tendon gliding. Patient compliance is also a paramount consideration, as the postoperative rehabilitation protocol is demanding and absolutely essential for a successful outcome.
| Parameter | Operative Indications | Non-Operative Indications and Contraindications |
|---|---|---|
| Nerve Status | Irreversible nerve injury, failed grafting, presentation >18 months post-injury, or used as an "internal splint" | Acute neurapraxia, recovering axonotmesis (advancing Tinel sign) |
| Joint Mobility | Full passive range of motion at wrist, MCP, and IP joints | Fixed joint contractures, severe arthrofibrosis |
| Donor Muscles | MRC Grade 5 strength in proposed donors (e.g., PT, FCR, FCU, FDS) | Donor strength < Grade 4, global brachial plexus injury |
| Soft Tissue Bed | Supple, well-vascularized subcutaneous tissue | Extensive scarring, active infection, inadequate soft tissue coverage |
| Patient Factors | Cooperative, capable of complex postoperative rehabilitation | Poor compliance, severe cognitive impairment, inability to participate in therapy |
Pre Operative Planning and Patient Positioning
Clinical Assessment and Diagnostics
Preoperative planning begins with a meticulous physical examination to document exact motor deficits and confirm the level of the radial nerve lesion. A high radial nerve palsy involves the loss of the BR, ECRL, and all PIN-innervated muscles. In contrast, Posterior Interosseous Nerve (PIN) syndrome spares the ECRL. Because the ECRL inserts on the base of the second metacarpal, its unopposed action in PIN syndrome results in a characteristic radial deviation during active wrist extension, alongside the loss of digital and thumb MCP extension.
Passive range of motion must be rigorously assessed. Any contractures of the wrist, metacarpophalangeal, or interphalangeal joints must be addressed preoperatively through aggressive hand therapy, dynamic splinting, or surgical release prior to considering tendon transfer. The strength of potential donor muscles—specifically the pronator teres (PT), flexor carpi radialis (FCR), flexor carpi ulnaris (FCU), flexor digitorum superficialis (FDS), and palmaris longus (PL)—must be confirmed as MRC grade 5.
Electrodiagnostic studies (Electromyography [EMG] and Nerve Conduction Velocities [NCV]) are highly valuable when the timeline of recovery is ambiguous. Fibrillation potentials and positive sharp waves indicate active, ongoing denervation. Conversely, the presence of nascent polyphasic motor unit potentials suggests early reinnervation, which may warrant further observation and delay of tendon transfer surgery.
Donor Selection and Transfer Sets
Several established transfer combinations exist, primarily differing in the choice of donor for digital extension. The selection depends on surgeon preference, available donors, and patient-specific functional demands.
- The Brand Transfer (FCR Transfer): This is currently the most widely utilized set due to its excellent functional outcomes and low donor morbidity. It involves transferring the PT to the ECRB for wrist extension, the FCR to the EDC for finger extension, and the PL to the EPL for thumb extension. Importantly, this transfer preserves the FCU, which is critical for the "dart-thrower's motion" and the powerful ulnar deviation necessary in many activities of daily living (e.g., hammering).
- The Jones Transfer (FCU Transfer): Historically popular, this utilizes the PT to the ECRB, the FCU to the EDC, and the FCR to the EPL. While the FCU provides robust excursion and strength for digital extension, sacrificing the FCU often leads to an undesirable and functionally limiting radial deviation deformity of the wrist, making this transfer less favorable in modern practice.
- The Boyes Transfer (FDS Transfer): This technique transfers the PT to the ECRB, the FDS of the middle finger to the EDC, and the FDS of the ring finger to the EPL and EIP. It avoids sacrificing any wrist flexors, preserving native wrist kinematics. However, it can lead to proximal interphalangeal (PIP) joint recurvatum, swan neck deformities, or stiffness in the donor digits, and it is technically more demanding.
Patient Positioning
The patient is positioned supine on the operating table with the affected upper extremity extended on a radiolucent hand table. A non-sterile tourniquet is applied high on the brachium. The entire upper extremity is prepped and draped in a standard sterile fashion to allow circumferential access from the elbow to the fingertips. Loupe magnification is highly recommended for meticulous tendon dissection, epitenon preservation, and weaving.
Detailed Surgical Approach and Technique
The following section details the surgical steps for the most commonly performed combination: the modified Brand transfer (Pronator Teres to Extensor Carpi Radialis Brevis, Flexor Carpi Radialis to Extensor Digitorum Communis, Palmaris Longus to Extensor Pollicis Longus).
Pronator Teres to Extensor Carpi Radialis Brevis
The restoration of strong, centralized wrist extension is the cornerstone of radial nerve palsy reconstruction. The ECRB is preferred over the ECRL as the recipient because its central insertion at the base of the third metacarpal provides pure wrist extension without the radial deviation vector associated with the ECRL.

An incision is made along the radial border of the mid-forearm. The superficial radial nerve is identified beneath the brachioradialis and carefully protected. The insertion of the PT is located on the lateral aspect of the middle third of the radial shaft. To maximize donor length, the PT is harvested with a generous strip of radial periosteum.

The ECRB tendon is identified and isolated from the ECRL. The PT is mobilized proximally into the forearm to ensure a straight line of pull and free excursion. A subcutaneous tunnel is created, and the PT tendon is routed superficially to the BR and ECRL, preparing it to be woven into the ECRB.

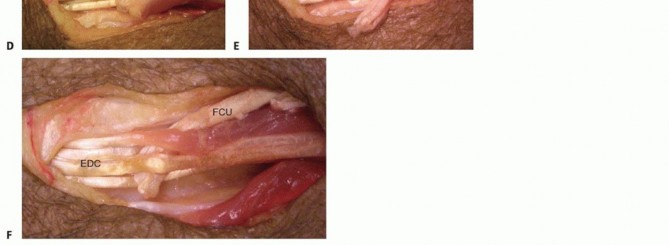
Flexor Carpi Radialis to Extensor Digitorum Communis
To restore metacarpophalangeal joint extension of the digits, the FCR is transferred to the EDC.

A transverse or longitudinal incision is made at the distal wrist crease over the FCR. The tendon is divided at its insertion on the base of the second metacarpal. A second incision is made in the mid-volar forearm to retrieve the FCR tendon proximally. The muscle belly is mobilized extensively, releasing fascial attachments to ensure adequate excursion.

A large, capacious subcutaneous tunnel is created around the radial border of the forearm, passing from volar to dorsal. The tunnel must be wide enough to accommodate the muscle belly without any mechanical tethering. The FCR tendon is passed through this tunnel to the dorsal wrist.

On the dorsal aspect, the extensor retinaculum is partially excised or longitudinally incised to expose the EDC tendons. The FCR will later be woven into all four slips of the EDC to provide synchronized digital extension.
Palmaris Longus to Extensor Pollicis Longus
Thumb extension is critical for opening the first web space to allow for grasp and pinch mechanics. The PL is an ideal donor due to its synergistic properties, expendability, and superficial location.

The EPL is identified dorsally, released from the third extensor compartment, and transposed radially out of Lister's tubercle. This transposition provides a more direct line of pull and increases its mechanical advantage for combined thumb extension and radial abduction. The PL is harvested at the wrist crease and retrieved proximally. It is then routed subcutaneously to the transposed EPL tendon.

Tendon Weaving and Tensioning Mechanics
Tensioning is arguably the most critical and technically demanding step of the procedure. Incorrect tensioning leads to immediate functional failure. Tendons are typically woven using the Pulvertaft technique, which provides superior biomechanical strength, increases the surface area for healing, and allows for early active mobilization protocols.

The Pulvertaft weave involves passing the donor tendon through the recipient tendon in a perpendicular fashion multiple times. A minimum of three passes is recommended for optimal pull-out strength. Each pass is secured with a core stitch of 3-0 or 4-0 non-absorbable braided suture (e.g., Ethibond or FiberWire), supplemented by peripheral running sutures (e.g., 4-0 Prolene) to smooth the junction, bury the tendon ends, and prevent catching during excursion.


The sequence of tensioning is paramount and must be performed in a specific order:
1. Wrist Extension (PT to ECRB): Tensioned first. The wrist is held in 30 to 40 degrees of extension with the forearm in maximum supination. The PT is pulled maximally, and the ECRB is pulled proximally to remove resting slack before the weave is secured.
2. Finger Extension (FCR to EDC): Tensioned second. The wrist is placed in neutral (0 degrees). The MCP joints are held in 0 degrees of extension, with the PIP and DIP joints allowed to flex naturally. The FCR is woven into the
Clinical & Radiographic Imaging



You Might Also Like


