Radial Shortening Osteotomy for Kienböck Disease: An Intraoperative Masterclass

Key Takeaway
This masterclass guides fellows through radial shortening osteotomy for Kienböck disease. We cover intricate lunate vascularity, ulnar variance assessment, and meticulous preoperative planning. The core focus is a real-time, step-by-step intraoperative execution, detailing incision, dissection, precise osteotomy, and hardware fixation. We emphasize critical anatomical landmarks, potential pitfalls, and advanced rehabilitation protocols to optimize patient outcomes.
Welcome, fellows, to the operating theater. Today, we are addressing a highly challenging and biomechanically complex condition: Kienböck disease, formally recognized as the avascular necrosis (AVN) of the carpal lunate. Our patient presents with a classic clinical picture: a young, active individual with chronic, debilitating dorsal wrist pain, significantly decreased grip strength, and a clear history of negative ulnar variance on standard posteroanterior radiographs. We have staged this specific presentation as Lichtman Stage IIIA, making a radial shortening osteotomy our primary, evidence-based surgical strategy. This procedure is not merely a structural alteration; it is a profound biomechanical intervention designed to unload the lunate, redistribute transcarpal forces, and ideally, facilitate spontaneous revascularization or, at the very least, halt the inexorable progression of the disease.
Comprehensive Introduction and Patho-Epidemiology
Before we make our initial incision and expose the distal radius, it is imperative that we thoroughly review the fundamental principles driving Kienböck disease. Understanding the patho-epidemiology dictates why our chosen intervention is so critical and how it alters the natural history of the wrist.
Pathogenesis of Kienbock Disease
The exact etiology of Kienböck disease remains a subject of intense academic debate, but it is universally accepted as a multifactorial process. The prevailing consensus points toward a complex interplay between vulnerable vascular anatomy, adverse biomechanical loading, and repetitive microtrauma. The lunate sits at the apex of the proximal carpal row, acting as the keystone of the wrist. When subjected to repetitive compressive and shear forces—particularly in the setting of negative ulnar variance—microfractures develop within the trabecular architecture of the bone. Unlike other bones with robust collateral circulation, the lunate struggles to heal these microfractures, leading to localized edema, increased intraosseous pressure, and subsequent venous congestion.
This venous hypertension initiates a vicious cycle. As intraosseous pressure rises, it eventually exceeds capillary perfusion pressure, leading to arterial ischemia and osteocyte death. The necrotic trabeculae lose their structural integrity, making the lunate highly susceptible to macroscopic collapse under the normal physiological loads of daily activities. Current histopathological studies suggest that the disease may stem more fundamentally from this venous outflow obstruction and intraosseous vascular congestion than from primary arterial insufficiency. This congestion, combined with stress fractures in the proximal lunate adjacent to the radial articular surface, leads to the predictable, progressive collapse we observe radiographically.
Furthermore, systemic factors and patient demographics play a crucial role. Kienböck disease disproportionately affects young adults between the ages of 20 and 40, with a higher prevalence in males, particularly those engaged in heavy manual labor or repetitive impact activities. However, it is also observed in sedentary individuals, highlighting the importance of intrinsic anatomical predispositions over purely extrinsic occupational hazards. Recognizing these demographic and biomechanical risk factors is essential for early diagnosis and timely surgical intervention before irreversible carpal collapse occurs.
Lichtman Staging and Natural History
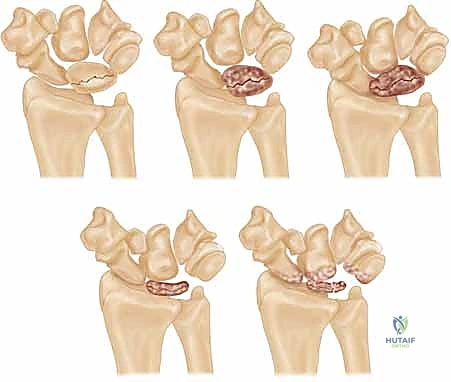
The natural history of Kienböck disease is one of progressive mechanical failure, reliably categorized by the Lichtman classification system. This staging is paramount, as it directly dictates our surgical algorithm. Stage I represents the earliest phase, where standard radiographs appear entirely normal, but magnetic resonance imaging (MRI) reveals the hallmark signs of ischemia: decreased signal intensity on T1-weighted images and variable signal on T2-weighted images, depending on the degree of reactive edema and attempted revascularization.

As the disease advances to Stage II, the lunate begins to exhibit increased radiodensity and sclerosis on plain radiographs. Despite these density changes, the overall anatomical shape and height of the lunate are maintained. This sclerosis represents a combination of compacted necrotic trabeculae and the apposition of new woven bone on dead trabecular cores—a frustrated attempt at creeping substitution. Stage IIIA, our patient's current stage, is characterized by structural failure. The lunate undergoes macroscopic collapse, losing its height and altering its geometry, yet the overall carpal height remains preserved, and there is no fixed scaphoid rotation or proximal migration of the capitate.
If left untreated, the condition relentlessly progresses to Stage IIIB, defined by lunate collapse accompanied by significant carpal instability. This includes a decrease in the carpal height ratio, proximal migration of the capitate into the space vacated by the collapsing lunate, and a fixed palmar flexion of the scaphoid, often visible as the "cortical ring sign" on AP radiographs. Ultimately, the altered kinematics lead to Stage IV, characterized by widespread radiocarpal and midcarpal secondary osteoarthritis. Our goal with the radial shortening osteotomy today is to intercept this natural history at Stage IIIA, preventing the catastrophic transition to Stage IIIB and Stage IV.
Detailed Surgical Anatomy and Biomechanics
To execute a precise and effective radial shortening osteotomy, a profound understanding of the lunate's precarious vascular supply and the intricate biomechanics of the radiocarpal joint is absolutely essential. We are not just cutting bone; we are manipulating a sophisticated load-bearing mechanism.
Lunate Vascular Anatomy and Vulnerability
The lunate, centrally positioned in the proximal carpal row, possesses a highly unique and unforgiving vascular anatomy. Its extraosseous blood supply is theoretically robust, fed by a rich network of branches from the radial, ulnar, and anterior interosseous arteries. These vessels converge to form intricate dorsal and volar radiocarpal plexuses. However, the intraosseous supply—the vessels that actually penetrate the bone to nourish the marrow and osteocytes—is the true Achilles' heel of the lunate. Because the lunate is almost entirely ensheathed in articular cartilage to facilitate complex multi-planar wrist motion, vessels can only enter at its non-articular dorsal and volar poles.

Anatomical injection studies have demonstrated that a significant percentage of lunates (ranging from 7% to 20%) are inherently "at risk" because large volumes of their internal trabecular bone rely on a single, dominant intraosseous vessel. Furthermore, up to 31% of lunates lack internal arterial anastomoses or branching, forming a Y-shaped or I-shaped vascular pattern. This terminal vascular distribution makes them highly susceptible to avascular necrosis if that solitary vessel is compromised by trauma, thrombosis, or increased intraosseous pressure.
This unique vascular anatomy explains why even minor, repetitive trauma or altered biomechanics can trigger catastrophic AVN. The proximal pole of the lunate, which articulates directly with the lunate fossa of the distal radius, is particularly vulnerable, as it is the furthest point from the dorsal and volar vascular entry zones. Our surgical goal with the osteotomy is to create a more favorable mechanical environment, drastically reducing the compressive and shear forces across this ischemic proximal pole, thereby allowing the tenuous vascular supply a chance to recover and initiate creeping substitution.
Ulnar Variance and Radiocarpal Biomechanics
Let us turn our attention to the distal forearm and the critical relationship between the lengths of the radius and ulna, known as ulnar variance. In a normal wrist with neutral ulnar variance, the distal articular surfaces of the radius and ulna are flush. Under these conditions, the radius bears approximately 80% of the axial load transmitted across the radiocarpal joint, while the ulna, via the triangular fibrocartilage complex (TFCC), absorbs the remaining 20%.
However, when a patient exhibits negative ulnar variance—where the ulna is anatomically shorter than the radius—this delicate load-sharing ratio is severely disrupted. Biomechanical studies have shown that even a 1 to 2 mm negative variance can shift the load distribution such that the radius bears up to 95% of the transcarpal forces. This disproportionately high load is concentrated directly across the radiolunate joint. The lunate is subjected to immense shear and compressive forces, particularly at its radial aspect, where its articulation with the rigid lunate fossa of the distal radius is far less compliant than its articulation with the thicker, shock-absorbing TFCC on the ulnar side.

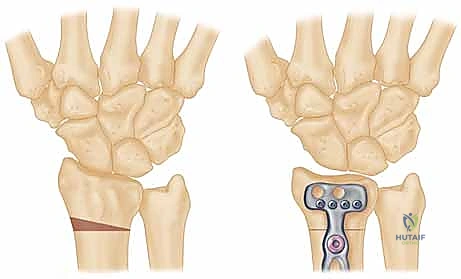
The radial shortening osteotomy directly and elegantly addresses this biomechanical imbalance. By surgically shortening the radius by a meticulously calculated 2 to 3 millimeters, we effectively "level" the joint. This intervention decreases joint compression forces at the radiolunate joint and redistributes them ulnarward to the ulnolunate joint and the TFCC. Furthermore, shortening the radius relatively lengthens the extensor and flexor musculotendinous units crossing the wrist joint. This "de-tensioning" effect further diminishes the overall static compressive forces acting on the carpus, providing a significant biological advantage over ulnar lengthening procedures, which do not offer this musculotendinous relaxation.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of success in Kienböck disease management. The radial shortening osteotomy is a powerful tool, but its application must be strictly governed by precise radiographic and clinical criteria.
Patient Selection Criteria
The ideal candidate for a radial shortening osteotomy is a patient presenting with Lichtman Stage I, II, or IIIA Kienböck disease, coupled with negative or neutral ulnar variance. In these early to intermediate stages, the lunate, while ischemic and potentially sclerotic or beginning to collapse, has not yet triggered a catastrophic breakdown of global carpal kinematics. The primary objective in these patients is joint leveling to decompress the lunate, thereby relieving pain, preserving grip strength, and halting radiographic progression.

The procedure is particularly efficacious in patients with symptomatic negative ulnar variance, as the biomechanical rationale for load shifting is most robust in this population. However, even in patients with neutral ulnar variance, a minimal shortening of 2 mm can still provide the necessary decompression through the relaxation of the crossing musculotendinous units. Age is also a consideration; the procedure is highly favored in younger, active patients (typically under 50 years of age) who place high functional demands on their wrists and require a durable, joint-preserving solution rather than a salvage arthrodesis.
The application of this technique in Lichtman Stage IIIB remains a topic of nuanced academic debate. In Stage IIIB, fixed carpal collapse and scaphoid rotation have already occurred. While some surgeons argue that the altered kinematics make joint leveling futile, a substantial body of literature suggests that radial shortening can still yield excellent pain relief and functional improvement in Stage IIIB, provided the radiocarpal and midcarpal articular cartilage remains viable. The decision here relies heavily on the surgeon's assessment of carpal reducibility and the absence of frank arthritic changes.
Absolute and Relative Contraindications
Conversely, strict adherence to contraindications prevents predictable surgical failures. The most absolute contraindication for a radial shortening osteotomy is the presence of Lichtman Stage IV Kienböck disease. Once significant secondary osteoarthritis has developed in the radiocarpal or midcarpal joints, altering the joint level will not alleviate the pain generated by the denuded articular surfaces. These patients require definitive salvage procedures, such as a proximal row carpectomy (PRC), a four-corner arthrodesis, or a total wrist fusion.

Positive ulnar variance represents a strong relative, and often absolute, contraindication. Performing a radial shortening in a patient who already has a long ulna will severely exacerbate the positive variance, predictably leading to iatrogenic ulnar impaction syndrome. In such cases, if joint leveling is desired, a radial wedge osteotomy to alter the radial inclination, or a direct lunate revascularization procedure combined with temporary unloading, is more appropriate. Additionally, active local or systemic infection, severe osteopenia that would compromise rigid plate fixation, and patients who are medically unfit for general or regional anesthesia are standard contraindications.
| Category | Indications for Radial Shortening | Contraindications for Radial Shortening |
|---|---|---|
| Lichtman Stage | Stage I, Stage II, Stage IIIA | Stage IV (Absolute), Stage IIIB (Relative/Controversial) |
| Ulnar Variance | Negative Variance, Neutral Variance | Positive Variance (Absolute) |
| Joint Status | Preserved radiocarpal/midcarpal cartilage | Established radiocarpal or midcarpal arthritis |
| Patient Factors | Young, active, high functional demand | Severe osteopenia, active infection, poor surgical candidate |
| Carpal Kinematics | Preserved carpal height, reducible scaphoid | Fixed, irreducible carpal collapse (Relative) |
Pre-Operative Planning, Templating, and Patient Positioning
Fellows, remember this cardinal rule: the success of a radial shortening osteotomy is forged in the preoperative planning phase, long before the pneumatic tourniquet is inflated. Precision in templating dictates precision in the operating theater.
Radiographic Evaluation and Templating
Meticulous radiographic evaluation is the foundation of our preoperative plan. We require high-quality, standardized posteroanterior (PA) and lateral radiographs of the affected wrist. The PA view must be taken with the patient's shoulder abducted to 90 degrees, the elbow flexed to 90 degrees, and the forearm in neutral rotation. This specific positioning is critical, as forearm pronation or supination artificially alters the apparent ulnar variance on the radiograph.

Once standardized images are obtained, we meticulously measure the ulnar variance. We draw a line transverse to the long axis of the radius at the level of the sclerotic subchondral bone of the lunate fossa, and a second parallel line at the distal articular surface of the ulnar head. The distance between these lines dictates our required shortening. For this patient, we have templated a precise 2.5 mm of shortening. Our goal is to achieve neutral or a maximum of 1 mm of positive ulnar variance. We must avoid the temptation to over-shorten; excessive shortening drastically alters the kinematics of the distal radioulnar joint (DRUJ) and invites debilitating ulnar impaction syndrome.

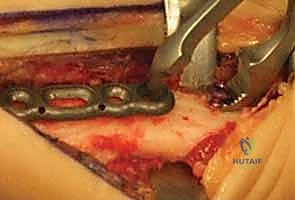
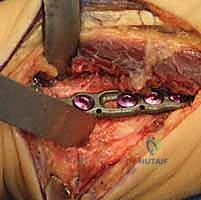
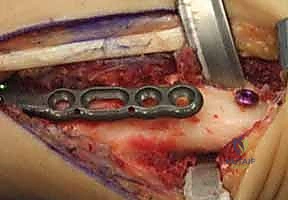
Furthermore, we must template the osteotomy site and the hardware. We typically plan the osteotomy approximately 3 to 4 centimeters proximal to the radiocarpal joint line. This location ensures we are operating in robust diaphyseal-metaphyseal cortical bone for optimal screw purchase, while remaining safely proximal to the complex capsular reflections of the DRUJ. We select our plate—typically a 6-hole or 7-hole 3.5mm dynamic compression plate (DCP) or a modern locking compression plate (LCP)—and overlay it on the digital radiographs to ensure adequate bone stock both proximally and distally.
Operating Room Setup and Anesthesia
The patient is positioned supine on the operating table, with the affected arm extended onto a specialized, radiolucent hand table. This setup is non-negotiable, as it allows for unimpeded, multi-planar fluoroscopic imaging throughout the procedure. A high-thigh pneumatic tourniquet is applied to the proximal arm. A completely bloodless field is absolutely critical for the meticulous soft tissue dissection required to identify and protect the delicate sensory nerve branches and to achieve perfect bony apposition.

Anesthesia can be tailored to the patient, but a regional axillary or supraclavicular brachial plexus block, often supplemented with light general anesthesia or deep intravenous sedation, is our preferred modality. This provides excellent intraoperative muscle relaxation and superior immediate postoperative pain control. Before prepping and draping, we bring the mini C-arm into the field to confirm that we can easily obtain perfect AP and lateral views of the distal radius without moving the patient's arm excessively. Once confirmed, the arm is prepped and draped in the standard sterile fashion, ensuring full visualization from the elbow to the fingertips.
Step-by-Step Surgical Approach and Fixation Technique
Alright, fellows, let us get scrubbed in. We will proceed systematically, emphasizing anatomical awareness, absolute precision in our bone cuts, and rigid biomechanical fixation at every single step.
Incision and Superficial Dissection
"Scalpel, please." We initiate the procedure with a dorsal longitudinal incision, approximately 8 to 10 centimeters in length, centered precisely over the dorsal aspect of the distal radius. We start the incision about 5 centimeters proximal to Lister's tubercle and extend it distally toward the radiocarpal joint line. This dorsal approach provides unparalleled, direct access to the broad, flat surface of the distal radial diaphysis, which is ideal for plate application.
As we incise the skin and superficial subcutaneous tissue, we must immediately heighten our awareness of the superficial sensory branch of the radial nerve. These nerve branches are highly variable in their arborization but generally run superficially in the subcutaneous fat on the radial aspect of our incision. We utilize fine, blunt dissection techniques—using a hemostat or tenotomy scissors—to gently sweep these delicate nerve branches radially, ensuring they are thoroughly protected and retracted well out of our operative field.

Iatrogenic injury to the superficial radial nerve is the most common and arguably the most aggravating complication of this approach. A transected or aggressively stretched nerve can result in a highly symptomatic neuroma or persistent, burning dysesthesia that will completely overshadow a mechanically perfect osteotomy. Always prioritize meticulous, blunt dissection in this superficial plane. If there is any anatomical ambiguity, a sterile nerve stimulator can be utilized to confirm the identity of the neural structures before proceeding deeper.
Deep Exposure and Periosteal Elevation
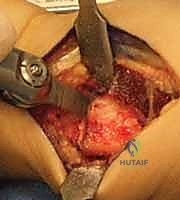
With the superficial nerves protected, we sharply incise the antebrachial fascia to reveal the extensor retinaculum and the dorsal extensor compartments. Our target interval lies between the first dorsal compartment (housing the abductor pollicis longus and extensor pollicis brevis) and the second dorsal compartment (housing the extensor carpi radialis longus and brevis). Developing this specific interval provides a direct, avascular plane down to the radial shaft, minimizing the need for excessive, traumatic retraction of the powerful wrist extensors.
Once we reach the bone, we utilize a sharp Cobb elevator to perform a meticulous subperiosteal dissection. We elevate the periosteum from the dorsal, radial, and volar aspects of the distal radius. It is crucial to expose a sufficient length of the radial diaphysis—typically 6 to 8 centimeters—to comfortably accommodate our chosen plate and allow for precise osteotomy cuts. We place blunt, self-retaining retractors (such as Gelpi or Weitlaner retractors) deep to the elevated periosteum to protect the soft tissues and extensor tendons from the oscillating saw.

We must ensure that the periosteal elevation is clean and contiguous. Preserving the integrity of the surrounding soft tissue envelope is vital for maintaining the local biological environment, which will drive rapid bone healing at the osteotomy site. We continuously irrigate the field to prevent tissue desiccation and maintain a clear view of the bare radial cortex, preparing for the critical measurement phase.
Osteotomy Execution and Radial Shortening
Now we arrive at the most critical step: determining the exact osteotomy level and executing the precise amount of shortening. Based on our preoperative templating, we require exactly 2.5 mm of shortening. We will perform a transverse osteotomy. While step-cut osteotomies offer inherent rotational stability, a transverse cut simplifies the precise calculation of shortening and allows for excellent compression when paired with a dynamic compression plate.

We begin by placing two parallel
Clinical & Radiographic Imaging Archive