Masterclass: Modular Radial Head Arthroplasty for Complex Elbow Trauma
Key Takeaway
This masterclass details modular radial head arthroplasty for complex elbow trauma. We cover comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution from a surgeon's perspective. Fellows will learn precise techniques for implant sizing, stem insertion, and crucial ligamentous repair, emphasizing neurovascular protection and stability assessment. Extensive pearls and pitfalls, alongside postoperative rehabilitation, ensure optimal patient outcomes for these challenging injuries.
Comprehensive Introduction and Patho-Epidemiology
Fellows, welcome to the operating theater. Today, we are undertaking a masterclass in one of the most unforgiving yet rewarding procedures in orthopedic traumatology: modular radial head arthroplasty. This intervention is a definitive cornerstone in the management of complex elbow trauma, particularly when the radial head sustains an unreconstructable fracture and concomitant ligamentous injuries critically compromise elbow stability. This procedure transcends the mere substitution of shattered bone; it is an intricate exercise in restoring the profound biomechanics, load-transfer kinematics, and stabilizing forces of the elbow and forearm axis.
To appreciate the gravity of this procedure, we must first understand the patho-epidemiology of these injuries. Radial head fractures account for approximately one-third of all adult elbow fractures. While a vast majority are low-energy, non-displaced injuries amenable to conservative management or simple open reduction and internal fixation (ORIF), high-energy trauma presents a vastly different clinical entity. Axial loading applied to a partially flexed, pronated forearm generates massive sheer and compressive forces across the radiocapitellar joint. When this force vector is combined with valgus stress and supination, it initiates a cascade of capsuloligamentous failure, often culminating in the dreaded "terrible triad" of the elbow—a constellation of a radial head fracture, coronoid fracture, and posterolateral elbow dislocation.
Historically, the orthopedic community relied heavily on radial head excision for comminuted fractures. However, longitudinal follow-up studies and advanced biomechanical analyses have unequivocally demonstrated the catastrophic long-term sequelae of this approach. Excision in the setting of ligamentous incompetence leads to proximal radial migration, profound valgus instability, altered ulnohumeral tracking, and rapid-onset post-traumatic arthropathy. The advent of metallic radial head arthroplasty revolutionized our treatment algorithm. By utilizing modern modular metallic implants, we can accurately reconstruct the radiocapitellar column, thereby restoring the critical secondary valgus and primary axial stabilizing properties of the native radial head, even in the presence of severe collateral ligament disruption.
The transition from silicone implants—which were notoriously plagued by catastrophic wear, fragmentation, and reactive silicone synovitis—to modern modular metallic designs represents a paradigm shift. Today’s modular systems, featuring interchangeable stems and heads, allow the surgeon to meticulously recreate the native articular geometry and offset. This modularity is paramount; failing to accurately reproduce the native radial head volume leads to "overstuffing" of the joint, resulting in accelerated capitellar wear, severe stiffness, and early aseptic loosening. Therefore, precision in patient selection, preoperative templating, and intraoperative execution is non-negotiable.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever handed to you, an exhaustive mastery of the regional anatomy and elbow biomechanics is mandatory. The elbow is not merely a simple hinge; it is a highly constrained, multi-axial trochoginglymoid joint that facilitates both flexion-extension and forearm pronosupination.
Osteology and Articular Geometry
The osteology of the proximal radius and its articulation is deceptively complex. The radial head is our primary anatomical focus. Contrary to simplified textbook diagrams, the radial head is not a perfect cylinder; it is distinctly elliptical. It features a concave articular dish (the fovea) that articulates with the spherical capitellum of the distal humerus, facilitating load transfer during axial compression. The peripheral articular margin of the radial head rotates smoothly within the lesser sigmoid notch of the proximal ulna during pronation and supination.
The capitellum serves as the distal humeral counter-articulation. It is a hemispherical structure located anterior and inferior to the lateral epicondyle. The articular cartilage of the capitellum is particularly vulnerable to shear forces and iatrogenic damage from improperly sized radial head implants. Distal to the radial head lies the radial neck, the precise location where our osteotomy must be performed. The medullary canal of the proximal radius exhibits significant anatomic variance in diameter, taper, and bow. This inherent variability underscores the necessity of modular implant systems, allowing independent sizing of the diaphyseal stem and the articular head to achieve a secure fit without compromising the articular tracking.
Furthermore, the radial head is not perfectly collinear with the radial shaft; it exhibits a subtle offset. The native head is typically offset laterally and anteriorly relative to the central axis of the radial neck. Modern modular implants attempt to replicate this offset, or at least accommodate it through "loose-fit" smooth stem designs that allow the implant to self-center within the radiocapitellar joint during active motion, thereby minimizing eccentric edge-loading on the capitellum.
Ligamentous Stabilizers and The Capsular Complex
Elbow stability is a synergistic interplay between osseous congruity, dynamic muscular compression, and static capsuloligamentous tension. The Medial Collateral Ligament (MCL), specifically its anterior bundle, is the primary restraint against valgus stress. Crucially, the radial head acts as the primary secondary valgus stabilizer. In the setting of an incompetent MCL, the radial head must absorb the entirety of the valgus load. If the radial head is excised without replacement in this scenario, gross valgus instability and rapid joint subluxation are inevitable.

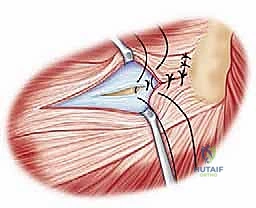
On the lateral side, the Lateral Collateral Ligament (LCL) complex is paramount for preventing varus and posterolateral rotatory instability (PLRI). This complex comprises the Radial Collateral Ligament (RCL), the Annular Ligament, and the Lateral Ulnar Collateral Ligament (LUCL). The LUCL originates from the isometric point on the lateral epicondyle and inserts onto the supinator crest of the ulna, acting as a critical sling supporting the radial head. During our surgical approach, meticulous preservation or robust anatomical repair of the LUCL is absolutely critical. Failure to restore LUCL tension will result in chronic PLRI, rendering the arthroplasty functionally useless.
Axial stability is governed by the Interosseous Membrane (IOM), particularly its central band. The IOM couples the radius and ulna, transferring approximately 80% of axial loads from the distal radius to the proximal ulna. In an Essex-Lopresti injury, massive axial energy ruptures the radial head, tears the IOM longitudinally, and disrupts the distal radioulnar joint (DRUJ). In such cases, a rigid, accurately sized radial head arthroplasty is the only mechanical block preventing the radius from migrating proximally and causing debilitating ulnocarpal impaction.
Neurovascular Topography
Navigating the lateral elbow requires profound respect for the regional neurovascular topography, most notably the Posterior Interosseous Nerve (PIN). The PIN, the deep motor branch of the radial nerve, dives beneath the arcade of Frohse to enter the supinator muscle. It wraps around the radial neck, placing it at extreme risk during lateral surgical approaches, retracter placement, and radial neck reaming.
The position of the PIN is dynamic and highly dependent on forearm rotation. Supination draws the PIN proximally and laterally, bringing it perilously close to the surgical field at the radial neck. Conversely, pronation of the forearm moves the PIN more distal and medial, safely distancing it from our operative window. Therefore, whenever dissecting distal to the annular ligament or reaming the radial canal, the forearm must be strictly maintained in pronation.
Other critical structures include the radial recurrent artery, which forms a vascular leash crossing the surgical interval. These vessels are frequently encountered during the deep dissection and require meticulous bipolar coagulation or formal ligation to prevent postoperative hemarthrosis. While the median and ulnar nerves are not directly in the lateral surgical field, a comprehensive preoperative and postoperative neurologic examination is mandatory to document any concomitant traction injuries sustained during the initial traumatic dislocation.
Exhaustive Indications and Contraindications
The decision to proceed with a modular radial head arthroplasty versus ORIF or non-operative management requires astute clinical judgment. As a rule, radial head arthroplasty is reserved for fractures that are mechanically unreconstructable, particularly when associated with complex elbow instability.
We specifically indicate radial head arthroplasty for Mason Type III (comminuted, displaced) and Type IV (associated with dislocation) fractures where the fragment count exceeds three, or where the articular cartilage is so severely impacted that a congruent joint surface cannot be restored. In these scenarios, attempted ORIF often leads to hardware failure, nonunion, or severe stiffness due to the extensive soft tissue stripping required for fixation. Arthroplasty provides immediate structural stability and allows for early, aggressive rehabilitation.
The presence of associated ligamentous injuries drastically lowers the threshold for arthroplasty. In the setting of a "terrible triad" injury, the coronoid fracture and LUCL tear render the elbow profoundly unstable. Here, the radial head prosthesis acts as the crucial anterior and valgus buttress. Similarly, in an Essex-Lopresti lesion with a disrupted IOM, the radial head must be replaced to prevent proximal radial migration; excision alone in this setting is an absolute contraindication. Furthermore, arthroplasty is highly effective in salvage scenarios, such as post-traumatic nonunions, failed ORIF with hardware cutout, or symptomatic proximal radial migration following a historical radial head excision.
| Indications for Radial Head Arthroplasty | Contraindications for Radial Head Arthroplasty |
|---|---|
| Unreconstructable Mason Type III/IV fractures (>3 fragments) | Active local or systemic infection |
| Fractures with associated elbow dislocation (Terrible Triad) | Skeletally immature patients (open physes) |
| Essex-Lopresti injuries (IOM tear + DRUJ disruption) | Isolated, non-displaced fractures amenable to conservative care |
| Severe comminution with known MCL or LCL disruption | Simple 2-part fractures highly amenable to stable ORIF |
| Failed prior ORIF with hardware failure or nonunion | Severe, uncorrectable proximal radial bone loss precluding stem seating |
| Symptomatic proximal migration post-prior excision | Neuropathic joint (Charcot arthropathy) |
Pre-Operative Planning, Templating, and Patient Positioning
Success in radial head arthroplasty is heavily predicated on meticulous preoperative planning. The operating room is not the environment for improvisation; you must enter with a definitive roadmap, a primary plan, and a robust salvage strategy.
Advanced Imaging and Templating
The diagnostic workup begins with high-quality orthogonal radiographs. Standard anteroposterior (AP), lateral, and oblique views of the elbow must be scrutinized. We assess the radiocapitellar line, which should intersect the capitellum in all views. Crucially, bilateral posteroanterior (PA) radiographs of the wrists in neutral rotation are mandatory to evaluate for ulnar variance. Positive ulnar variance on the injured side, especially in the presence of a comminuted radial head, is the hallmark of an Essex-Lopresti injury and dictates that the radial head must be replaced to restore axial length.




While plain films are essential, a Computed Tomography (CT) scan with 3D reconstructions is the gold standard for preoperative planning. The CT scan allows us to definitively quantify the degree of comminution, assess for subtle capitellar shear fractures, and evaluate the size of any associated coronoid fragments. This dictates whether the coronoid will require separate fixation (e.g., via a medial approach or anterior lasso technique) prior to addressing the radial head.
Digital templating is performed using radiographs of the contralateral, uninjured elbow. We template the diameter of the radial head and the width of the radial neck canal. The primary goal of templating is to avoid the most common and devastating complication of this procedure: overstuffing the radiocapitellar joint. An oversized implant acts as a cam during forearm rotation, prying the ulnohumeral joint apart, stretching the collateral ligaments, and accelerating capitellar cartilage destruction. When in doubt between two sizes, it is always safer to downsize the radial head diameter by 1-2 millimeters.
Implant Selection Strategy
The modern orthopedic armamentarium offers various modular metallic implants. The current consensus favors monopolar, modular designs. Bipolar implants, which feature an additional articulation between the head and stem, were initially designed to improve tracking; however, long-term data demonstrated unacceptable rates of dissociation, polyethylene wear, and severe osteolysis.
Regarding stem fixation, surgeons must choose between press-fit (porous-coated) and loose-fit (smooth) stems. A smooth, loose-fitting stem acts as a spacer rather than a rigidly fixed prosthesis. This intentional micromotion allows the radial head to self-center against the capitellum during the complex kinematics of pronosupination, reducing edge-loading. Conversely, a rigidly fixed, porous-coated stem requires absolutely perfect anatomical alignment; any slight malposition will result in asymmetric capitellar wear and eventual aseptic loosening of the stem due to massive sheer forces at the bone-implant interface. For acute trauma, a smooth, loose-fitting modular stem is generally preferred by most elbow specialists.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia, frequently supplemented by a regional supraclavicular or interscalene nerve block. This provides excellent intraoperative muscle relaxation—crucial for joint reduction and stability testing—and profound postoperative analgesia, facilitating early rehabilitation.
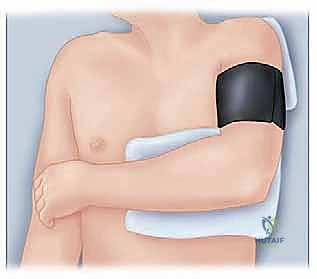
The patient is positioned supine. The injured arm is draped free and placed either on a radiolucent hand table or brought across the patient's chest. The "arm over chest" position is highly advantageous for lateral approaches, as gravity assists in opening the lateral joint space when varus stress is applied. A sterile tourniquet is applied high on the brachium. The C-arm fluoroscopy unit must be positioned to allow unobstructed AP and lateral imaging of the elbow throughout the procedure without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped and the plan finalized, we proceed to the surgical execution. Meticulous soft tissue handling and precise osseous preparation are the hallmarks of a successful arthroplasty.
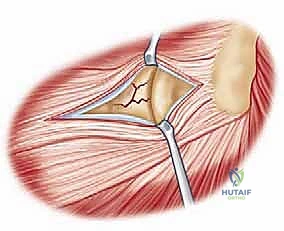
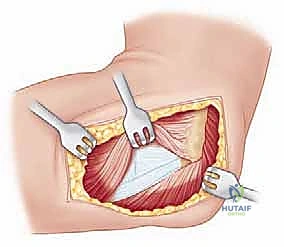
The Surgical Approach
We typically utilize a lateral approach to the elbow, choosing between the Kocher interval or the Extensor Digitorum Communis (EDC) split. The Kocher approach utilizes the internervous plane between the anconeus (radial nerve) and the Extensor Carpi Ulnaris (PIN). While it provides excellent exposure of the radial head, extending this approach too far anteriorly or distally risks violating the intact LUCL or injuring the PIN.



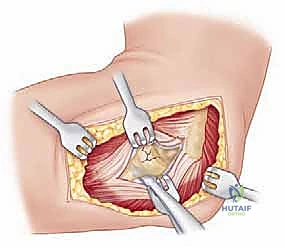
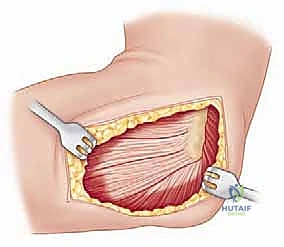
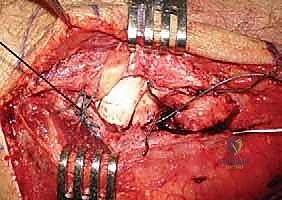
Increasingly, trauma surgeons prefer the EDC split (the Taylor and Scham approach) or the Kaplan interval (between EDC and ECRB). The EDC split provides direct, centralized access to the radiocapitellar joint. An incision is made from the lateral epicondyle extending distally toward the Lister's tubercle. The deep fascia is incised, and the EDC muscle belly is bluntly split longitudinally. This approach stays anterior to the LUCL, preserving this critical stabilizer. Upon reaching the capsule, a longitudinal arthrotomy is performed. The fracture hematoma is evacuated, and the joint is thoroughly irrigated to remove all osteochondral debris.
Radial Head Excision and Canal Preparation
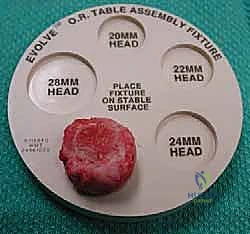
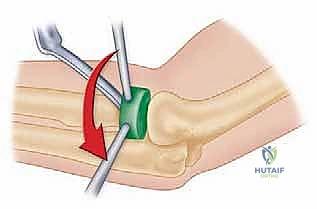
Once the joint is exposed, the comminuted radial head fragments are meticulously excised. It is imperative to preserve the annular ligament during this process. The excised fragments are transferred to the back table and reassembled like a jigsaw puzzle. This reconstructed native head is measured with calipers to determine the exact diameter and thickness required for the modular prosthesis.


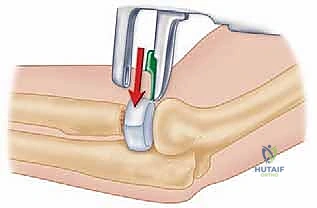
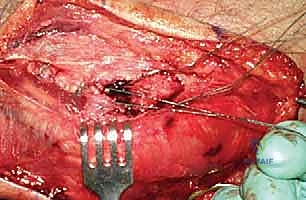
Next, the radial neck osteotomy is performed. An oscillating saw is used to create a clean, transverse cut perpendicular to the axis of the radial neck. The level of the osteotomy is dictated by the fracture pattern; we resect only as much bone as necessary to reach a stable, circumferential cortical base. Care must be taken to preserve the bicipital tuberosity to maintain supination strength.
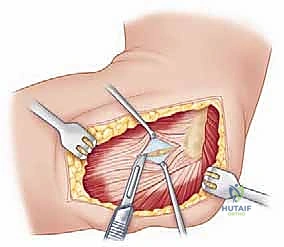
With the forearm strictly pronated to protect the PIN, the medullary canal is prepared. A starter awl is introduced into the canal, followed by sequential broaching or reaming. The canal is prepared to accommodate the selected stem size. If a loose-fit smooth stem is chosen, the canal is reamed slightly larger than the stem diameter to allow for the desired self-centering micromotion.
Implantation and Trialing
The trialing phase is arguably the most critical step of the operation. The selected trial stem and head are inserted. The elbow is reduced, and we perform a comprehensive dynamic assessment. We evaluate the radiocapitellar articulation throughout a full arc of flexion-extension and pronosupination.